
Vascular Responses following Light Therapy: A Pilot Study with Healthy Volunteers
 , ,
, ,  , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
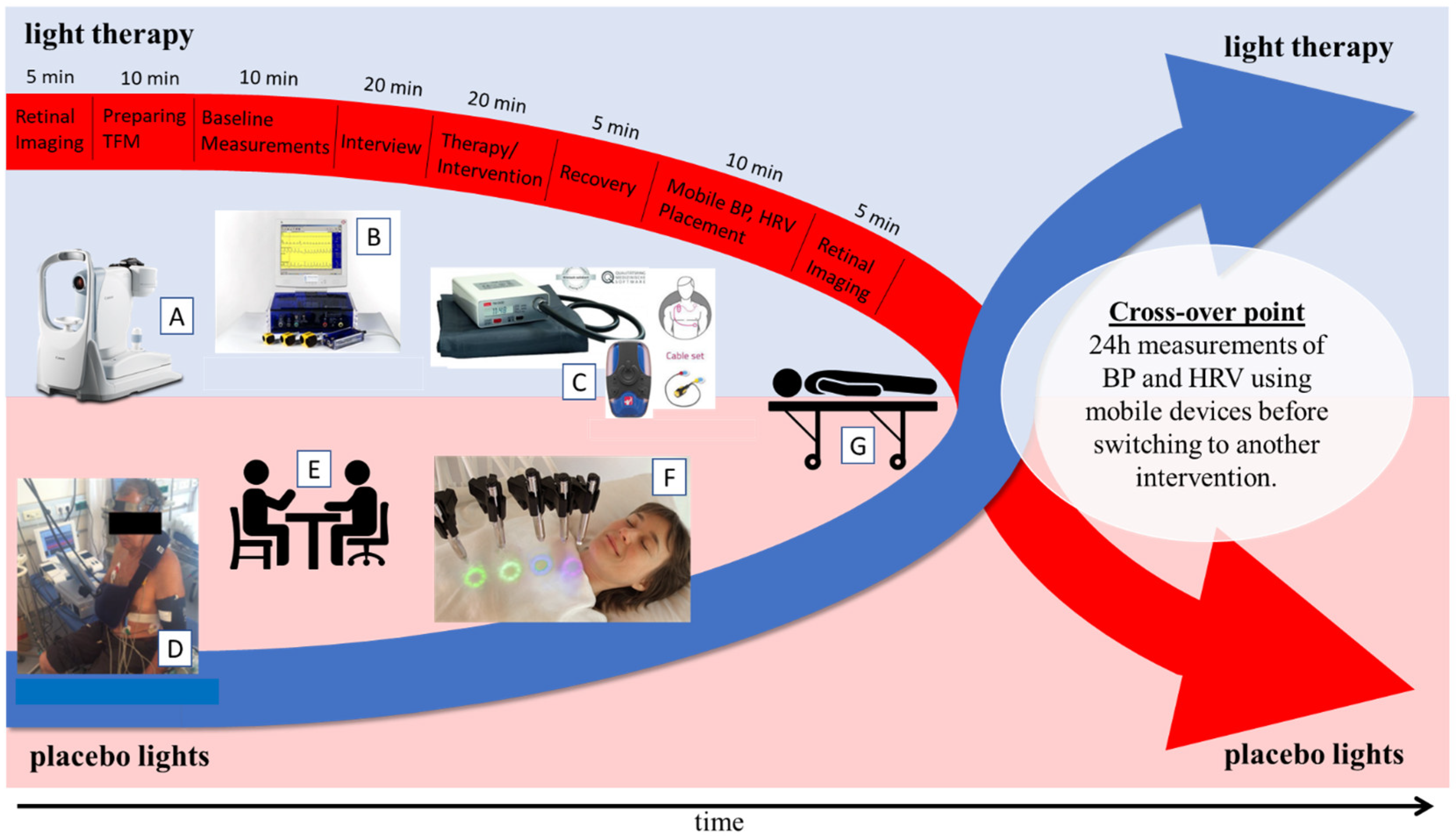
2.2. Study Design
2.3. Light Therapy Application Device
2.3.1. Light Therapy Pens
2.3.2. Placebo Light Pens
2.4. Light Therapy Protocol
2.5. Physiological Measurements
2.6. Heart Rate Variability and Blood Pressure Variability Measurements
2.7. Retinal Measurements
2.8. Statistical Analysis
3. Results
3.1. Physiological Parameters Obtained with the Task Force Monitor
3.2. Heart Rate and Blood Pressure Variability Measurements
3.3. Retinal Measurements
4. Discussion
5. Limitations
6. Conclusion and Future Directions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boutouyrie, P.; Chowienczyk, P.; Humphrey, J.D.; Mitchell, G.F. Arterial Stiffness and Cardiovascular Risk in Hypertension. Circ. Res. 2021, 128, 864–886. [Google Scholar] [CrossRef]
- Cimminiello, C.; Zambon, A.; Polo Friz, H. Hypercholesterolemia and cardiovascular risk: Advantages and limitations of current treatment options. G. Ital. Cardiol. 2016, 17, 6S-13. [Google Scholar] [CrossRef]
- Herath, P.; Wimalasekera, S.; Amarasekara, T.; Fernando, M.; Turale, S. Effect of cigarette smoking on smoking biomarkers, blood pressure and blood lipid levels among Sri Lankan male smokers. Postgrad. Med. J. 2022, 98, 848–854. [Google Scholar] [CrossRef] [PubMed]
- Tan, Y.; Cheong, M.S.; Cheang, W.S. Roles of Reactive Oxygen Species in Vascular Complications of Diabetes: Therapeutic Properties of Medicinal Plants and Food. Oxygen 2022, 2, 246–268. [Google Scholar] [CrossRef]
- Sharma, K.; Basu-Ray, I.; Sayal, N.; Vora, A.; Bammidi, S.; Tyagi, R.; Modgil, S.; Bali, P.; Kaur, P.; Goyal, A.K.; et al. Yoga as a Preventive Intervention for Cardiovascular Diseases and Associated Comorbidities: Open-Label Single Arm Study. Front. Public Health 2022, 10, 1425. [Google Scholar] [CrossRef]
- Hartley, L.; Mavrodaris, A.; Flowers, N.; Ernst, E.; Rees, K. Transcendental meditation for the primary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 2017, CD010359. [Google Scholar] [CrossRef]
- Forbes, D.; Blake, C.M.; Thiessen, E.J.; Peacock, S.; Hawranik, P. Light therapy for improving cognition, activities of daily living, sleep, challenging behaviour, and psychiatric disturbances in dementia. Cochrane Database Syst. Rev. 2014, CD003946. [Google Scholar] [CrossRef] [Green Version]
- Lindskov, F.O.; Iversen, H.K.; West, A.S. Clinical outcomes of light therapy in hospitalized patients—A systematic review. Chronobiol. Int. 2022, 39, 299–310. [Google Scholar] [CrossRef]
- Janas-Kozik, M.; Krzystanek, M.; Stachowicz, M.; Krupka-Matuszczyk, I.; Janas, A.; Rybakowski, J.K. Bright light treatment of depressive symptoms in patients with restrictive type of anorexia nervosa. J. Affect. Disord. 2011, 130, 462–465. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.; Gretz, N. Role of Visible Light on Skin Melanocytes: A Systematic Review. Photochem. Photobiol. 2021, 97, 911–915. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Song, S.; Fong, C.-C.; Tsang, C.-H.; Yang, Z.; Yang, M. cDNA microarray analysis of gene expression profiles in human fibroblast cells irradiated with red light. J. Investig. Dermatol. 2003, 120, 849–857. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Azeemi, S.T.Y.; Raza, S.M.; Yasinzai, M.; Samad, A. Effect of Different Wavelengths on Superoxide Dismutase. J. Acupunct. Meridian Stud. 2009, 2, 236–238. [Google Scholar] [CrossRef] [Green Version]
- Azeemi, S.T.Y.; Raza, S.M.; Yasinzai, M. Colors as Catalysts in Enzymatic Reactions. J. Acupunct. Meridian Stud. 2008, 1, 139–142. [Google Scholar] [CrossRef] [Green Version]
- De Chaves, M.E.A.; de Araújo, A.R.; Piancastelli, A.C.C.; Pinotti, M. Effects of low-power light therapy on wound healing: LASER x LED. An. Bras. Dermatol. 2014, 89, 616–623. [Google Scholar] [CrossRef]
- Azeemi, S.T.Y.; Mahmood, K.; Yousaf, R. Effect of Visible Range Electromagnetic Radiations (Colours) on Platelets in Thrombocytopenia in Dengue Fever. Pak. J. Med. Health Sci. 2015, 9, 462–464. [Google Scholar]
- Yousaf, R.; Azeemi, S.T.; Rashid, A. Treatment of insomnia by turquoise colour (495 nm) during pregnancy. Pak. Postgrad. Med. J. 2013, 24, 66–69. Available online: http://ppmj.org.pk/index.php/ppmj/article/view/220 (accessed on 14 July 2021).
- Azeemi, S.T.Y.; Rafiq, H.M.; Ismail, I.; Kazmi, S.R.; Azeemi, A. The mechanistic basis of chromotherapy: Current knowledge and future perspectives. Complement. Ther. Med. 2019, 46, 217–222. [Google Scholar] [CrossRef] [PubMed]
- Campbell, P.D.; Miller, A.M.; Woesner, M.E. Bright Light Therapy: Seasonal Affective Disorder and Beyond. Einstein J. Biol. Med. EJBM 2017, 32, E13–E25. Available online: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC6746555/ (accessed on 24 January 2023). [PubMed]
- Pandey, A.; Tripathi, P.; Pandey, R.; Srivatava, R.; Goswami, S. Alternative therapies useful in the management of diabetes: A systematic review. J. Pharm. Bioallied Sci. 2011, 3, 504–512. [Google Scholar] [CrossRef] [PubMed]
- Maharishi Mahesh Yogi. Available online: https://maharishilighttechnology.org/maharishi-mahesh-yogi (accessed on 12 July 2021).
- Health News: Top Stories. Available online: https://globalgoodnews.com/health-news-a.html?art=124337155712958608 (accessed on 12 July 2021).
- Travis, F.; Melzer, A.; Scharf, D. Effects of Maharishi Light Technology with Gems: A random-assignment, placebo-controlled, blinded pilot study. SAGE Open Med. 2020, 8, 2050312120918272. [Google Scholar] [CrossRef]
- Trozic, I.; Platzer, D.; Fazekas, F.; Bondarenko, A.I.; Brix, B.; Rössler, A.; Goswami, N. Postural hemodynamic parameters in older persons have a seasonal dependency. Z. Gerontol. Geriatr. 2020, 53, 145–155. [Google Scholar] [CrossRef] [Green Version]
- Lackner, H.K.; Goswami, N.; Papousek, I.; Roessler, A.; Grasser, E.K.; Montani, J.-P.; Jezova, D.; Hinghofer-Szalkay, H. Time course of cardiovascular responses induced by mental and orthostatic challenges. Int. J. Psychophysiol. 2010, 75, 48–53. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Malik, M.; Bigger, J.T.; Camm, A.J.; Kleiger, R.E.; Malliani, A.; Moss, A.J.; Schwartz, P.J. Heart rate variability: Standards of measurement, physiological interpretation, and clinical use. Eur. Heart J. 1996, 17, 354–381. [Google Scholar] [CrossRef] [Green Version]
- Cornelissen, G. Cosinor-based rhythmometry. Theor. Biol. Med. Model. 2014, 11, 16. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khan, A.; Boever, P.D.; Gerrits, N.; Akhtar, N.; Saqqur, M.; Ponirakis, G.; Gad, H.; Petropoulos, I.N.; Shuaib, A.; Faber, J.E.; et al. Retinal vessel multifractals predict pial collateral status in patients with acute ischemic stroke. PLoS ONE 2022, 17, e0267837. [Google Scholar] [CrossRef] [PubMed]
- Knudtson, M.D.; Lee, K.E.; Hubbard, L.D.; Wong, T.Y.; Klein, R.; Klein, B.E.K. Revised formulas for summarizing retinal vessel diameters. Curr. Eye Res. 2003, 27, 143–149. [Google Scholar] [CrossRef]
- Rudlof, M.E.; Šimunić, B.; Steuber, B.; Bartel, T.O.; Neshev, R.; Mächler, P.; Dorr, A.; Picha, R.; Schmid-Zalaudek, K.; Goswami, N. Effects of Meditation on Cardiovascular and Muscular Responses in Patients during Cardiac Rehabilitation: A Randomized Pilot Study. J. Clin. Med. 2022, 11, 6143. [Google Scholar] [CrossRef]
- Litscher, D.; Wang, L.; Gaischek, I.; Litscher, G. The Influence of New Colored Light Stimulation Methods on Heart Rate Variability, Temperature, and Well-Being: Results of a Pilot Study in Humans. Evid.-Based Complement. Altern. Med. ECAM 2013, 2013, 674183. [Google Scholar] [CrossRef] [Green Version]
- Yuda, E.; Ogasawara, H.; Yoshida, Y.; Hayano, J. Suppression of vagal cardiac modulation by blue light in healthy subjects. J. Physiol. Anthropol. 2016, 35, 24. [Google Scholar] [CrossRef] [Green Version]
- The Influence of Colored Light on Heart Rate Variability and Human Discomfort. Available online: https://arts.units.it/handle/11368/3015208 (accessed on 9 December 2022).
- Wong, T.Y.; Klein, R.; Sharrett, A.R.; Duncan, B.B.; Couper, D.J.; Tielsch, J.M.; Klein, B.E.K.; Hubbard, L.D. Retinal Arteriolar Narrowing and Risk of Coronary Heart Disease in Men and WomenThe Atherosclerosis Risk in Communities Study. JAMA 2002, 287, 1153–1159. [Google Scholar] [CrossRef] [Green Version]
- Wajih, N.; Alipour, E.; Rigal, F.; Zhu, J.; Perlegas, A.; Caudell, D.L.; Kim-Shapiro, D. Effects of nitrite and far-red light on coagulation. Nitric Oxide Biol. Chem. 2021, 107, 11–18. [Google Scholar] [CrossRef] [PubMed]
- Keszler, A.; Lindemer, B.; Broeckel, G.; Weihrauch, D.; Gao, Y.; Lohr, N.L. In Vivo Characterization of a Red Light-Activated Vasodilation: A Photobiomodulation Study. Front. Physiol. 2022, 13, 792. [Google Scholar] [CrossRef]
- Stern, M.; Broja, M.; Sansone, R.; Gröne, M.; Skene, S.S.; Liebmann, J.; Suschek, C.V.; Born, M.; Kelm, M.; Heiss, C. Blue light exposure decreases systolic blood pressure, arterial stiffness, and improves endothelial function in humans. Eur. J. Prev. Cardiol. 2018, 25, 1875–1883. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Marquina, N.; Oxinos, G.; Sau, A.; Ng, D. Effect of laser acupoint treatment on blood pressure and body weight—A pilot study. J. Chiropr. Med. 2008, 7, 134–139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rentz, L.E.; Bryner, R.W.; Ramadan, J.; Rezai, A.; Galster, S.M. Full-Body Photobiomodulation Therapy Is Associated with Reduced Sleep Durations and Augmented Cardiorespiratory Indicators of Recovery. Sports 2022, 10, 119. [Google Scholar] [CrossRef]
- Khattab, K.; Khattab, A.A.; Ortak, J.; Richardt, G.; Bonnemeier, H. Iyengar Yoga Increases Cardiac Parasympathetic Nervous Modulation Among Healthy Yoga Practitioners. Evid.-Based Complement. Altern. Med. ECAM 2007, 4, 511–517. [Google Scholar] [CrossRef]
- Papp, M.E.; Lindfors, P.; Storck, N.; Wändell, P.E. Increased heart rate variability but no effect on blood pressure from 8 weeks of hatha yoga—A pilot study. BMC Res. Notes 2013, 6, 59. [Google Scholar] [CrossRef] [Green Version]
- Patra, S.; Telles, S. Heart Rate Variability During Sleep Following the Practice of Cyclic Meditation and Supine Rest. Appl. Psychophysiol. Biofeedback 2010, 35, 135–140. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Langhorst, J.; Dobos, G. Are Indian yoga trials more likely to be positive than those from other countries? A systematic review of randomized controlled trials. Contemp. Clin. Trials 2015, 41, 269–272. [Google Scholar] [CrossRef]
- Cramer, H.; Lauche, R.; Haller, H.; Steckhan, N.; Michalsen, A.; Dobos, G. Effects of yoga on cardiovascular disease risk factors: A systematic review and meta-analysis. Int. J. Cardiol. 2014, 173, 170–183. [Google Scholar] [CrossRef]
- Kirkwood, G.; Rampes, H.; Tuffrey, V.; Richardson, J.; Pilkington, K. Yoga for anxiety: A systematic review of the research evidence. Br. J. Sports Med. 2005, 39, 884–891. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Males = 14 | Females = 16 | ||
|---|---|---|---|---|
| Age (years) | (46 ± 20) | 23–71 | (46 ± 17) | 24–71 |
| Height (cm) | (176.7 ± 6.2) | 166–185 | (165.8 ± 5.0) | 160–179 |
| Weight (kg) | (82.5 ± 19.5) | 56–130 | (61.1 ± 10.9) | 51–85 |
| BMI (kg/m2) | (26.5 ± 6.8) | 20–45 | (22.2 ± 3.6) | 19–32 |
| Retinal Parameter | Intervention | Before | After | F-Value, p-Value |
|---|---|---|---|---|
| CRAE (µm) | MLT | 148.9 (18.1) | 145.6 (16.3) | F(1,24) = 17.004, p < 0.001 |
| Placebo | 145.5 (18.1) | 147.5 (17.5) | ||
| CRVE (µm) | MLT | 222.7 (20.6) | 218.3 (19.8) | F(1,24) = 11.999, p = 0.002 |
| Placebo | 219.5 (22.1) | 221.9 (20.2) | ||
| AVR | MLT | 0.668 (0.047) | 0.668 (0.051) | F(1,24) = 0.069, p = 0.796 |
| Placebo | 0.663 (0.049) | 0.665 (0.053) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saloň, A.; Steuber, B.; Neshev, R.; Schmid-Zalaudek, K.; De Boever, P.; Bergmann, E.; Picha, R.; Fredriksen, P.M.; Nkeh-Chungag, B.N.; Goswami, N. Vascular Responses following Light Therapy: A Pilot Study with Healthy Volunteers. J. Clin. Med. 2023, 12, 2229. https://doi.org/10.3390/jcm12062229
Saloň A, Steuber B, Neshev R, Schmid-Zalaudek K, De Boever P, Bergmann E, Picha R, Fredriksen PM, Nkeh-Chungag BN, Goswami N. Vascular Responses following Light Therapy: A Pilot Study with Healthy Volunteers. Journal of Clinical Medicine. 2023; 12(6):2229. https://doi.org/10.3390/jcm12062229
Chicago/Turabian StyleSaloň, Adam, Bianca Steuber, Ruslan Neshev, Karin Schmid-Zalaudek, Patrick De Boever, Eva Bergmann, Rainer Picha, Per Morten Fredriksen, Benedicta Ngwechi Nkeh-Chungag, and Nandu Goswami. 2023. "Vascular Responses following Light Therapy: A Pilot Study with Healthy Volunteers" Journal of Clinical Medicine 12, no. 6: 2229. https://doi.org/10.3390/jcm12062229