
Clinical Factors Associated with Severity of Colonic Diverticular Bleeding and Impact of Bleeding Site
 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
3. Results
3.1. Background Characteristics
3.2. Data on Colonic Diverticular Bleeding
3.3. Difference between Right and Left CDB
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yamamichi, N.; Shimamoto, T.; Takahashi, Y.; Sakaguchi, Y.; Kakimoto, H.; Matsuda, R.; Kataoka, Y.; Saito, I.; Tsuji, Y.; Yakabi, S.; et al. Trend and risk factors of diverticulosis in Japan: Age, gender, and lifestyle/metabolic-related factors may cooperatively affect on the colorectal diverticula formation. PLoS ONE 2015, 10, e0123688. [Google Scholar] [CrossRef] [Green Version]
- Nagata, N.; Niikura, R.; Aoki, T.; Shimbo, T.; Itoh, T.; Goda, Y.; Suda, R.; Yano, H.; Akiyama, J.; Yanase, M.; et al. Increase in colonic diverticulosis and diverticular hemorrhage in an aging society: Lessons from a 9-year colonoscopic study of 28,192 patients in Japan. Int. J. Color. Dis. 2014, 29, 379–385. [Google Scholar] [CrossRef]
- Kinjo, K.; Matsui, T.; Hisabe, T.; Ishihara, H.; Maki, S.; Chuman, K.; Koga, A.; Ohtsu, K.; Takatsu, N.; Hirai, F.; et al. Increase in colonic diverticular hemorrhage and confounding factors. World J. Gastrointest. Pharmacol. Ther. 2016, 7, 440–446. [Google Scholar] [CrossRef] [Green Version]
- Niikura, R.; Nagata, N.; Shimbo, T.; Aoki, T.; Yamada, A.; Hirata, Y.; Sekine, K.; Okubo, H.; Watanabe, K.; Sakurai, T.; et al. Natural history of bleeding risk in colonic diverticulosis patients: A long-term colonoscopy-based cohort study. Aliment. Pharmacol. Ther. 2015, 41, 888–894. [Google Scholar] [CrossRef] [PubMed]
- Tanaka, Y.; Motomura, Y.; Akahoshi, K.; Iwao, R.; Komori, K.; Nakama, N.; Osoegawa, T.; Itaba, S.; Kubokawa, M.; Hisano, T.; et al. Predictive factors for colonic diverticular rebleeding: A retrospective analysis of the clinical and colonoscopic features of 111 patients. Gut Liver 2012, 6, 334–338. [Google Scholar] [CrossRef] [PubMed]
- Niikura, R.; Nagata, N.; Yamada, A.; Akiyama, J.; Shimbo, T.; Uemura, N. Recurrence of colonic diverticular bleeding and associated risk factors. Color. Dis. 2012, 14, 302–305. [Google Scholar] [CrossRef] [PubMed]
- Aytac, E.; Stocchi, L.; Gorgun, E.; Ozuner, G. Risk of recurrence and long-term outcomes after colonic diverticular bleeding. Int. J. Color. Dis. 2014, 29, 373–378. [Google Scholar] [CrossRef]
- Poncet, G.; Heluwaert, F.; Voirin, D.; Bonaz, B.; Faucheron, J.L. Natural history of acute colonic diverticular bleeding: A prospective study in 133 consecutive patients. Aliment. Pharmacol. Ther. 2010, 32, 466–471. [Google Scholar] [CrossRef] [Green Version]
- Okamoto, T.; Watabe, H.; Yamada, A.; Hirata, Y.; Yoshida, H.; Koike, K. The association between arteriosclerosis related diseases and diverticular bleeding. Int. J. Color. Dis. 2012, 27, 1161–1166. [Google Scholar] [CrossRef]
- Nishikawa, H.; Maruo, T.; Tsumura, T.; Sekikawa, A.; Kanesaka, T.; Osaki, Y. Risk factors associated with recurrent hemorrhage after the initial improvement of colonic diverticular bleeding. Acta Gastroenterol. Belg. 2013, 76, 20–24. [Google Scholar]
- Nagata, N.; Ishii, N.; Manabe, N.; Tomizawa, K.; Urita, Y.; Funabiki, T.; Fujimori, S.; Kaise, M. Guidelines for colonic diverticular bleeding and colonic diverticulitis: Japan Gastroenterological Association. Digestion 2019, 99 (Suppl. 1), 1–26. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L.; Orav, E.J.; Syngal, S. Early predictors of severity in acute lower intestinal tract bleeding. Arch. Intern. Med. 2003, 163, 838–843. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aoki, T.; Nagata, N.; Shimbo, T.; Niikura, R.; Sakurai, T.; Moriyasu, S.; Okubo, H.; Sekine, K.; Watanabe, K.; Yokoi, C.; et al. Development and validation of a risk scoring system for severe acute lower gastrointestinal bleeding. Clin. Gastroenterol. Hepatol. 2016, 14, 1562–1570.e2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Das, A.; Ben-Menachem, T.; Cooper, G.S.; Chak, A.; Sivak, M.V.; Gonet, J.A.; Wong, R.C. Prediction of outcome in acute lower-gastrointestinal haemorrhage based on an artificial neural network: Internal and external validation of a predictive model. Lancet 2003, 362, 1261–1266. [Google Scholar] [CrossRef]
- Peery, A.F.; Keku, T.O.; Martin, C.F.; Eluri, S.; Runge, T.; Galanko, J.A.; Sandler, R.S. Distribution and characteristics of colonic diverticular in a United States screening population. Clin. Gastroenterol. Hepatol. 2016, 14, 980–985. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nagata, N.; Niikura, R.; Shimbo, T.; Kishida, Y.; Sekine, K.; Tanaka, S.; Aoki, T.; Watanabe, K.; Akiyama, J.; Yanase, M.; et al. Alcohol and smoking affect risk of uncomplicated colonic diverticulosis in Japan. PLoS ONE 2013, 8, e81137. [Google Scholar] [CrossRef] [PubMed]
- Soh, Y.S.A.; Ooi, S.Q.D.; Chan, Y.H.; Siah, T.H.K.; Lee, S.E.; Lee, W.J.J.; Zhu, F.; Yeoh, K.G.; Gwee, K.A. Rising prevalence of colonic diverticulosis in a westernized multi-ethnic Asian community. J. Gastroenterol. Hepatol. 2021, 36, 413–420. [Google Scholar] [CrossRef] [PubMed]
- Nakaji, S.; Danjo, K.; Munakata, A.; Sugawara, K.; MacAuley, D.; Kernohan, G.; Baxter, D. Comparison of etiology of right-sided diverticula in Japan with that of left-sided diverticula in the West. Int. J. Color. Dis. 2002, 17, 365–373. [Google Scholar] [CrossRef]
- Manabe, N.; Haruma, K.; Nakajima, A.; Yamada, M.; Maruyama, Y.; Gushimiyagi, M.; Yamamoto, T. Characteristics of colonic diverticulitis and factors associated with complications: A Japanese multicenter, retrospective, cross-sectional study. Dis. Colon Rectum 2015, 58, 1174–1181. [Google Scholar] [CrossRef]
- Kinjo, K.; Matsui, T.; Hisabe, T.; Ishihara, H.; Kojima, T.; Chuman, K.; Yasukawa, S.; Beppu, T.; Koga, A.; Ishikawa, S.; et al. Risk factors for severity of colonic diverticular hemorrhage. Intest. Res. 2018, 16, 458–466. [Google Scholar] [CrossRef]
- Gilshtein, H.; Kluger, Y.; Khoury, A.; Issa, N.; Khoury, W. Massive and recurrent diverticular hemorrhage, risk factors and treatment. Int. J. Surg. 2016, 33 Pt A, 136–139. [Google Scholar] [CrossRef]
- Strate, L.L.; Saltzman, J.R.; Ookubo, R.; Mutinga, M.L.; Syngal, S. Validation of a clinical prediction rule for severe acute lower intestinal bleeding. Am. J. Gastroenterol. 2005, 100, 1821–1827. [Google Scholar] [CrossRef] [PubMed]
- García-Blázquez, V.; Vicente-Bártulos, A.; Olavarria-Delgado, A.; Plana, M.N.; Van Der Winden, D.; Zamora, J.; for the EBM-Connect Collaboration. Accuracy of CT angiography in the diagnosis of acute gastrointestinal bleeding: Systematic review and meta-analysis. Eur. Radiol. 2013, 23, 1181–1190. [Google Scholar] [CrossRef] [PubMed]
- Obana, T.; Fujita, N.; Sugita, R.; Hirasawa, D.; Sugawara, T.; Harada, Y.; Oohira, T.; Maeda, Y.; Koike, Y.; Suzuki, K.; et al. Prospective evaluation of contrast-enhanced computed tomography for the detection of colonic diverticular bleeding. Dig. Dis. Sci. 2013, 58, 1985–1990. [Google Scholar] [CrossRef] [PubMed]
- Strate, L.L.; Syngal, S. Predictors of utilization of early colonoscopy vs. radiography for severe lower intestinal bleeding. Gastrointest. Endosc. 2005, 61, 46–52. [Google Scholar] [CrossRef] [PubMed]
- Sengupta, N.; Tapper, E.B.; Feuerstein, J.D. Early versus delayed colonoscopy in hospitalized patients with lower gastrointestinal bleeding: A meta-analysis. J. Clin. Gastroenterol. 2017, 51, 352–359. [Google Scholar] [CrossRef] [PubMed]
- Kouanda, A.M.; Somsouk, M.; Sewell, J.L.; Day, L.W. Urgent colonoscopy in patients with lower gastrointestinal bleeding: A systematic review and meta-analysis. Gastrointest. Endosc. 2017, 86, 107–117. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yamagishi, T.; Kashiura, M.; Shindo, Y.; Yamanaka, K.; Tsuboi, K.; Shinhata, H. Effectiveness of endoscopic hemostasis in preventing diverticular bleeding with extravasation detected by contrast-enhanced computed tomography: A single-center retrospective cohort study. Medicine 2021, 100, e24736. [Google Scholar] [CrossRef]
- Ochi, M.; Kamoshida, T.; Hamano, Y.; Ohkawara, A.; Ohkawara, H.; Kakinoki, N.; Yamaguchi, Y.; Hirai, S.; Yanaka, A. Early colonoscopy and urgent contrast enhanced computed tomography for colonic diverticular bleeding reduces risk of rebleeding. World J. Clin. Cases 2021, 9, 2446–2457. [Google Scholar] [CrossRef]
- Witte, J.T. Band ligation for colonic bleeding: Modification of multiband ligating devices for use with a colonoscope. Gastrointest. Endosc. 2000, 52, 762–765. [Google Scholar] [CrossRef] [PubMed]
- Farrell, J.J.; Graeme-Cook, F.; Kelsey, P.B. Treatment of bleeding colonic diverticula by endoscopic band ligation: An in-vivo and ex-vivo pilot study. Endoscopy 2003, 35, 823–829. [Google Scholar] [CrossRef]
- Setoyama, T.; Ishii, N.; Fujita, Y. Enodoscopic band ligation (EBL) is superior to endoscopic clipping for the treatment of colonic diverticular hemorrhage. Surg. Endosc. 2011, 25, 3574–3578. [Google Scholar] [CrossRef] [PubMed]
- Ishii, N.; Setoyama, T.; Deshpande, G.A.; Omata, F.; Matsuda, M.; Suzuki, S.; Uemura, M.; Iizuka, Y.; Fukuda, K.; Suzuki, K.; et al. Endoscopic band ligation for colonic diverticular hemorrhage. Gastrointest. Endosc. 2012, 75, 382–387. [Google Scholar] [CrossRef] [PubMed]
- Ikeya, T.; Ishii, N.; Nakano, K.; Omata, F.; Shimamura, Y.; Ego, M.; Takagi, K.; Nakamura, K.; Fukuda, K.; Fujita, Y. Risk factors for early rebleeding after endoscopic band ligation for colonic diverticular hemorrhage. Endosc. Int. Open 2015, 03, E523–E528. [Google Scholar] [CrossRef] [Green Version]
- Shibata, S.; Shigeno, T.; Fujimori, K.; Kanai, K.; Yoshizawa, K. Colonic diverticular hemorrhage: The hood method for detecting responsible diverticula and endoscopic band ligation for hemostasis. Endoscopy 2014, 46, 66–69. [Google Scholar] [CrossRef] [PubMed]
- Akutsu, D.; Narasaka, T.; Wakayama, M.; Terasaki, M.; Kaneko, T.; Matsui, H.; Suzuki, H.; Hyodo, I.; Mizokami, Y. Endoscopic detachable snare ligation: A new treatment method for colonic diverticular hemorrhage. Endoscopy 2015, 47, 1039–1042. [Google Scholar] [CrossRef]
- Takahashi, S.; Inaba, T.; Tanaka, N. Delayed perforation after endoscopic band ligation for treatment of colonic diverticular bleeding. Dig. Endosc. 2016, 28, 484. [Google Scholar] [CrossRef] [PubMed]
- Ishii, N.; Fujita, Y. Colonic diverticulitis after endoscopic band ligation performed for colonic diverticular hemorrhage. ACG Case Rep. J. 2015, 2, 218–220. [Google Scholar] [CrossRef]
- Honda, H.; Ishii, N.; Takasu, A.; Shiratori, Y.; Omata, F. Rsik factors of early rebleeding in the endoscopic management of colonic diverticular bleeding. J. Gastroenterol. Hepatol. 2019, 34, 1784–1792. [Google Scholar] [CrossRef]
- Kawanishi, K.; Kato, J.; Kakimoto, T.; Hara, T.; Yoshida, T.; Ida, Y.; Maekita, T.; Iguchi, M.; Kitano, M. Risk of colonic diverticular rebleeding according to endoscopic appearance. Endosc. Int. Open 2018, 6, E36–E42. [Google Scholar] [CrossRef] [Green Version]
- Nagata, N.; Niikura, R.; Ishii, N.; Kaise, M.; Omata, F.; Tominaga, N.; Kitagawa, T.; Ikeya, T.; Kobayashi, K.; Furumoto, Y.; et al. Cumulative evidence for reducing recurrence of colonic diverticular bleeding using endoscopic clipping versus band ligation: Systematic review and meta-analysis. J. Gastroenterol. Hepatol. 2021, 36, 1738–1743. [Google Scholar] [CrossRef] [PubMed]
- Niikura, R.; Nagata, N.; Aoki, T.; Shimbo, T.; Tanaka, S.; Sekine, K.; Kishida, Y.; Watanabe, K.; Sakurai, T.; Yokoi, C.; et al. Predictors for identification of stigmata of recent hemorrhage on colonic diverticula in lower gastrointestinal bleeding. J. Clin. Gastroenterol. 2015, 49, e24–e30. [Google Scholar] [CrossRef] [PubMed]
- Nakano, K.; Ishii, N.; Ikeya, T.; Ego, M.; Shimamura, Y.; Takagi, K.; Nakamura, K.; Fukuda, K.; Fujita, Y. Comparison of long-term outcomes between endoscopic band ligation and endoscopic clipping for colonic diverticular hemorrhage. Endosc. Int. Open 2015, 3, E529–E533. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | |
|---|---|
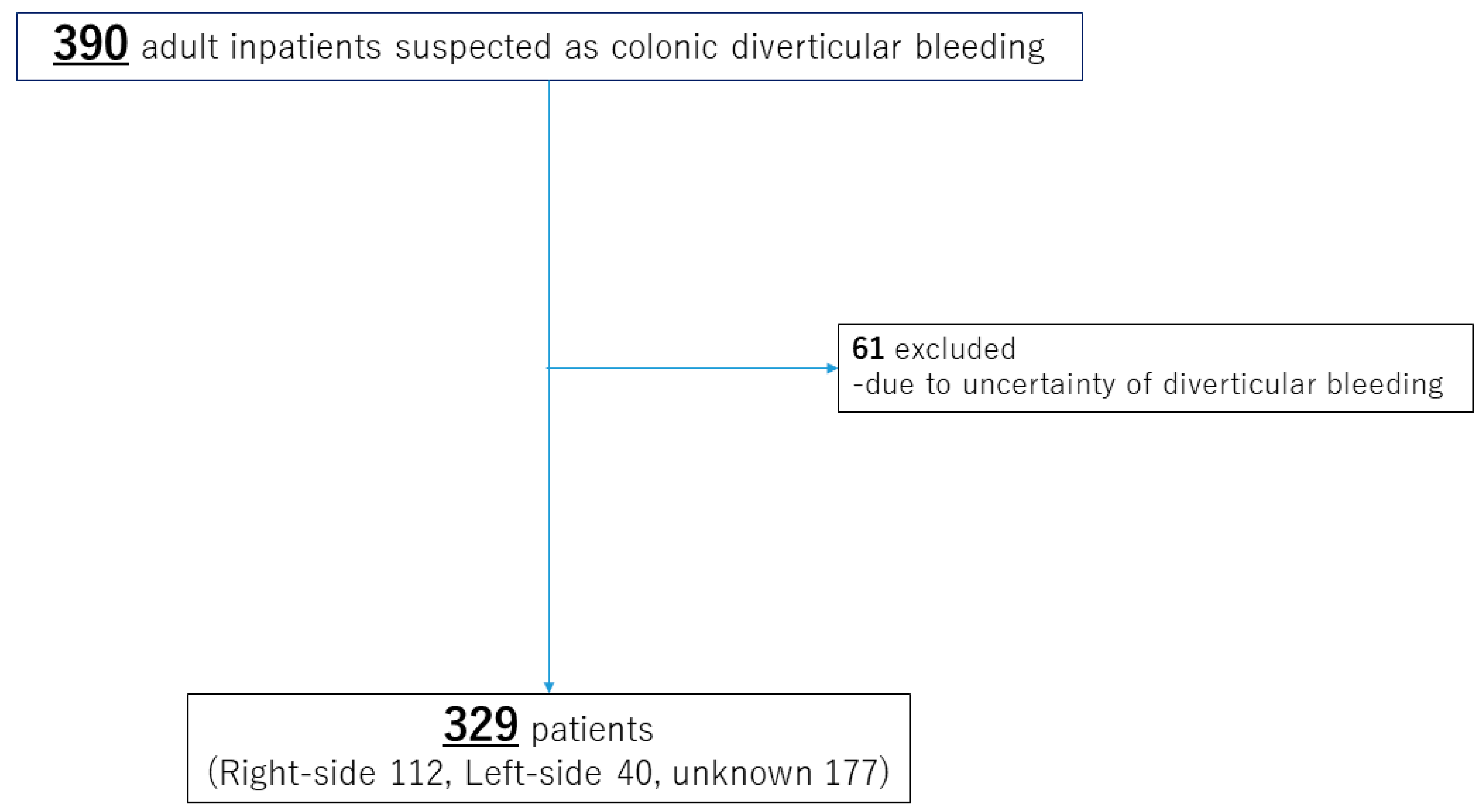
| Number of patients | 329 |
| Age (year), median (min-max) | 73 (35–98) |
| Age >= 75 years old, n (%) | 145 |
| Sex (male), n (%) | 222 (67.5) |
| Height (m), median (IQR) | 1.62 (1.53–1.68) |
| Weight (kg), median (IQR) | 59.9 (50.8–67.8) |
| Body mass index (kg/m2) > 30, n (%) | 18 (5.5) |
| Smoking, n (%) | 95 (28.9) |
| Alcohol, n (%) | 134 (40.7) |
| Comorbidities, n (%) | |
| Hypertension | 224 (68.1) |
| Dyslipidemia | 123 (37.4) |
| Diabetes mellitus | 63 (19.1) |
| Constipation | 52 (15.8) |
| Ischemic heart disease | 69 (21.0) |
| Cerebrovascular disease | 43 (13.1) |
| Chronic kidney disease | 166 (50.5) |
| Past diverticular bleeding | 148 (45.0) |
| Concomitant medicines, n (%) | |
| Antiplatelets | 143 (43.5) |
| Anticoagulants | 53 (16.1) |
| Nonsteroidal anti-inflammatory drug | 66 (20.1) |
| Diverticular bleeding | |
| Location of bleeding diverticula (right-left-unknown) | 112-40-177 |
| Hemoglobin < 10 g/dL, n (%) | 146 (44.4) |
| Heart rate/systolic blood pressure > 1, n (%) | 19 (5.8) |
| Treatment | |
| Endoscopic hemostasis | 93 (28.3) |
| Surgery | 6 (1.8) |
| Interventional radiology | 13 (4.0) |
| Blood transfusion | 157 (47.7) |
| Rebleeding | |
| Early (within 1 month) | 75 (22.8) |
| Late (within 1 year) | 62 (18.8) |
| Factors | Red Blood Cell Transfusion, n; 157 | Surgery and/or IVR, n; 19 | Rebleeding within 1 Month, n; 75 | Rebleeding within 1 Year, n; 62 |
|---|---|---|---|---|
| Older age (≥75) n; 145 | 78(54) 1.63(0.71–3.76) p = 0.25 | 6(4) 0.34(0.11–1.04) p = 0.06 | 27(19) 1.21(0.34–4.33) p = 0.77 | 33(23) 0.79(0.34–1.84) p = 0.59 |
| Hypertension, n; 224 | 115(51) 1.39(0.73–2.68) p = 0.32 | 13(6) 0.82(0.25–2.72) p = 0.75 | 57(25) 3.16(1.62–6.18) p < 0.001 | 49(22) 2.63(1.22–5.67) p = 0.01 |
| Chronic kidney diseasen; 166 | 83(50) 0.81(0.48–1.36) p = 0.42 | 9(5) 0.90(0.34–2.37) p = 0.83 | 36(22) 0.85(0.46–1.54) p = 0.58 | 43(26) 2.79(1.44–5.40) p < 0.01 |
| Past DBn; 148 | 59(40)0.66(0.42–1.06) p = 0.08 | 10(7) 1.44(0.55–3.77) p = 0.46 | 33(22) 1.070(0.62–1.84) p = 0.81 | 39(26) 2.10(1.13–3.85) p = 0.02 |
| Antiplatelets, n; 90 | 52(58) 1.05(0.42–2.64) p = 0.92 | 8(9) 2.97(0.60–14.83) p = 0.18 | 23(26) 2.00(0.74–5.38) p = 0.17 | 15(17) 0.43(0.15–1.21) p = 0.11 |
| Anticoagulants n; 53 | 34(64) 2.23(1.21–4.10) p = 0.01 | 5(9) 1.95(0.67–5.66) p = 0.22 | 16(11) 1.590(0.83–3.06) p = 0.16 | 11(21) 1.155(0.56–2.40) p = 0.70 |
| NSAIDs n; 66 | 24(36) 0.32(0.39–1.37) p = 0.73 | 1(2) 0.26(0.03–1.99) p = 0.19 | 12(18) 0.74(0.36–1.53) p = 0.42 | 16(24) 1.26(0.62–2.53) p = 0.52 |
| Confirmed DB n; 152 | 96(63) 2.88(1.77–4.69) p < 0.001 | 19(13) N/A * | 57(38) 6.19(3.34–11.48) p < 0.001 | 28(18) 1.27(0.71–2.28) p = 0.42 |
| Hb < 10 g/dL n; 146 | 102(70) 5.40(3.36–8.67) p < 0.001 | 7(5) 0.72(0.28–1.87) p = 0.50 | 35(24) 1.13(0.67–1.89) p = 0.65 | 33(23) 1.55(0.89–2.70) p = 0.12 |
| HR/sBP > 1 n; 19 | 18(95) 22.1(2.9–168.0) p < 0.01 | 19(100) N/A * | 7(37) 2.08(0.79–5.48) p = 0.14 | 1(5) 0.23(0.03–1.73) p = 0.15 |
| Characteristics | Right-Sided 112 Patients n (%) | Left-Sided 40 Patients n (%) | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|---|---|
| Red blood cell transfusion | 76 (67.9) | 20 (50.0) | 3.38 (1.36–8.38) | 0.009 |
| Invasive treatment (IVR or surgery) | 18 (16.1) | 1 (2.5) | 27.49 (3.46–218.51) | 0.002 |
| Early rebleeding (within 1 month) | 44 (39.3) | 13 (32.5) | 0.85 (0.31–2.31) | 0.747 |
| Late rebleeding (within 1 year) | 18 (16.1) | 10 (25.0) | 0.90 (0.32–2.51) | 0.843 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amano, H.; Yamamoto, T.; Ikusaka, K.; Aoki, N.; Sakurai, M.; Honda, T.; Maruyama, K.; Aoyagi, H.; Isono, A.; Abe, K.; et al. Clinical Factors Associated with Severity of Colonic Diverticular Bleeding and Impact of Bleeding Site. J. Clin. Med. 2023, 12, 1826. https://doi.org/10.3390/jcm12051826
Amano H, Yamamoto T, Ikusaka K, Aoki N, Sakurai M, Honda T, Maruyama K, Aoyagi H, Isono A, Abe K, et al. Clinical Factors Associated with Severity of Colonic Diverticular Bleeding and Impact of Bleeding Site. Journal of Clinical Medicine. 2023; 12(5):1826. https://doi.org/10.3390/jcm12051826
Chicago/Turabian StyleAmano, Hirohito, Takatsugu Yamamoto, Ken Ikusaka, Naoaki Aoki, Miyoko Sakurai, Taku Honda, Kyohei Maruyama, Hitoshi Aoyagi, Akari Isono, Koichiro Abe, and et al. 2023. "Clinical Factors Associated with Severity of Colonic Diverticular Bleeding and Impact of Bleeding Site" Journal of Clinical Medicine 12, no. 5: 1826. https://doi.org/10.3390/jcm12051826