
Understanding the Impact of COVID-19 on Chronic Lymphocytic Leukemia (CLL) Caregiving and Related Resource Needs

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Recruitment
2.2. Measures
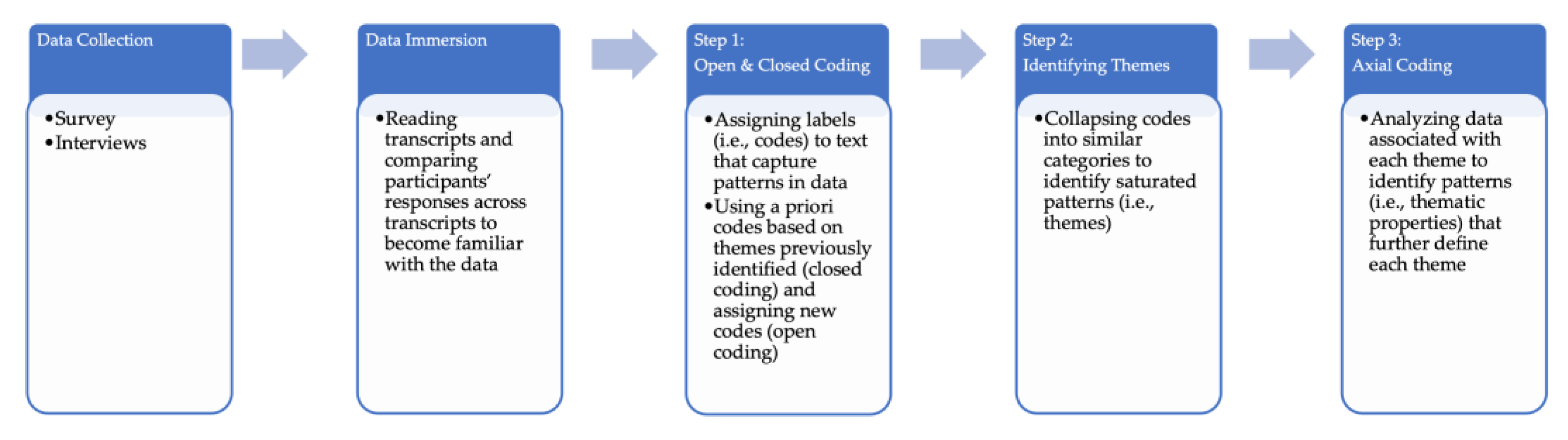
2.3. Analysis
3. Results
3.1. Survey Participants
3.2. Interview Participants
3.3. Aim 1: Challenges CLL Caregivers Encountered during the Pandemic
3.3.1. Coping with Distress
Caregivers responding to the survey (n = 223) as well as caregivers who were interviewed collectively described grappling with chronic distress. This included survey respondents caring for loved ones in watch and wait (n = 60). Caregivers wrote about living with “great fear” and “anxiety” with responses illustrating distress, focused either on a state of heightened caution to reduce risk, increased negative feelings, or COVID-19 uncertainty-related distress. Caregivers wrote about being “paranoid of bringing infection home” (Survey-91), which warranted their vigilance in maintaining heightened caution to reduce their (and their loved one’s) risk of COVID-19 infection (e.g., shopping at certain times, double masking, and wearing gloves). They wrote that “the pressure was real” and used language that captured their increased negative feelings, for example, “feeling paranoid”, “crazy”, and “nervous and anxious”. They also described distress related to uncertainty about COVID-19 risk: “More stress due to uncertainty about my husband’s safety”.(Survey-11)
Caregivers’ reports in the interview study validated this finding, illustrating the negative effect they endured: “Our lives have been sheer hell during COVID, because he’s immunocompromised” (Interview-7). Multiple caregivers expressed that coping with the pandemic (i.e., maintaining caution) was more strenuous than coping with CLL: “It’s scary. I was very, very protective about COVID because I’m thinking, ‘I don’t need you to die of COVID. We’re getting through this cancer!’” (Interview-10). They also linked their fears and heightened caution with inhibiting their mental well-being: “Quite a bit of depression on my side. I worry about her quite a bit. … I didn’t want to bring something home, and so I ended up with quite a bit of anxiety over these things and her”.(Interview-12)
How are we going to live in this world or how do we want to live in this world? How many risks? Do we want to get on a plane? … Are we going to be able to go take our trips like we would like or go to someone’s wedding like we won’t do at this point? That kind of overlays because of the fact that he’s such an at-risk individual for COVID hospitalization and death. It’s sort of like, “What do we want to do here?” The CLL seems—not to be trite—like small potatoes right now. He’s on this new drug [which] makes his white count go up for a while and then down. … It’s more like “Can you stay well through COVID? Can we still have a good life?”.(Interview-8)
I treat myself the way she wants to treat herself. That’s part of what I can do to support her. I’ll wear maybe a surgical mask, which I don’t really know if you really have to if you’re outside. But if we’re walking and we come near somebody, even if we’re outside, she’s telling me, “Put your mask on!” So, doing things like that makes her feel more confident even though I’m not really sure you need to wear a mask outside.(Interview-9)
Now that things are lifting, I’m definitely feeling much more frisky, I guess I would say, and [he’s] not at all. He really does enjoy the safety and the predictability of staying home. So how we navigate that, I think, is going to be the next issue.(Interview-2)
3.3.2. Living in Isolation
We see no one except outside, and since we live in the Midwest, the weather means that most of the year we have a social life only on Zoom. We don’t travel, go to concerts, see films in theaters, dine in restaurants, get our hair cut professionally. In fact, because the pool in our community is physically attached to a care center, we have not used the pool since the Delta surge began.(Survey-316)
These collective social losses negatively affected caregivers’ well-being: “It’s been isolating for me, because whomever I’m exposed to, she’s exposed to. I’m very social and it’s been difficult not to see my friends and family as frequently as I used to prior to the pandemic”.(Survey-411)
Because of COVID we can’t have social activities. Both she and I were in our church choir, and we can’t do that anymore. So, one of the biggest, I’d say, challenges for me is you know, a lack of social contact and we had always gone to church every Sunday and we can’t, you know. We can’t.(Interview-9)
We would go out and spend the afternoon out by our pool, have snacks and stuff and go swimming, go to the beach, go fishing. There’s just so much available at least here to keep us from completely going out of your mind.(Interview-1)
Also, unlike early in the pandemic, these caregivers now had access to rapid COVID-19 tests, which some described using to feel comfortable visiting loved ones: “We take great faith in the rapid tests. We’ve just now started going to dinner at friends’ houses and if they take a rapid, we’re good”.(Interview-10)
3.3.3. Losing In-Person Care Opportunities
Caregivers struggled with lost in-person care opportunities across the pandemic as reported in the survey study (n = 71) and interviews. While this did include some survey respondents caring for diagnosed loved ones in watch and wait, it was less prevalently reported as a challenge (n = 11). Survey respondents focused on two types of lost in-person care. They addressed both reduced in-person clinical care opportunities as well as lost in-home help. These losses were also associated with distressing language and isolation, with caregivers disclosing they felt “frustrated” and “cut off”. Caregivers were still at times unable to attend appointments either due to clinical protocols or COVID-19 exposures and infections, which could inhibit their ability to provide care: “[It’s been] extremely difficult to navigate … cannot attend appointments. [My husband] missed several biopsies etc. due to not having me attend and not understanding his treatment plans or what was expected and getting lost” (Survey-480). Caregivers also described losing in-home care help: “[COVID-19] made it difficult to get outside assistance”.(Survey-147)
As a newly diagnosed couple … it wasn’t all that easy to find resources. And it wasn’t all that easy to take it all in … It was harder to find because it all happened during COVID. And so when you look at a support group or something like that, it was all online or postponed. … You feel like you’re being barraged with all these really intense decisions, and you just don’t have the skills, the knowledge, or the ability to take it all in fast enough. It’s coming at you so quick. And the learning curve is so steep.(Interview-5)
3.3.4. Increasing Caregiving Burden
My husband contracted COVID and almost died. He was hospitalized for a month and received home health care for another month. He’s developed other problems with his heart and breathing. He currently is on long term FMLA from his job and receiving unemployment. I have to pay his insurance premiums to maintain his insurance. I’ve tried submitting these claims for reimbursement but get denied. … It’s been a huge financial burden cause it’s quite expensive. Hard on finances.(Survey-329)
Caregivers also reported instrumental care burden, which was related to their need to isolate and not receive in-person or at-home care help to reduce risk: “[COVID-19] has led to me taking on more outside tasks to minimize his exposure” (Survey-502). They juggled most if not all of the household responsibilities (e.g., keeping the house clean, outside maintenance) as well as outside tasks (e.g., grocery shopping). They wrote about solely carrying this load: “I have carried on my shoulders, the duty of protection, supplier of needed items” (Survey-507). At times, the instrumental care burden intersected with financial burden: “The sole caretaker for the entire household, while working a full-time job”.(Survey-314)
The financial blow is the bigger one for me and for both of us. … Our issues are largely around how are we going to tread water. … Normally, he would be going back to [work] but the stress, the exposure, the difficulty on the body, we’re doing everything in our power not to make him go back. … So, we’ve sold our car. … I work a side gig. And my parents—my family—has come together in tremendous ways to support us financially.(Interview-5)
I was juggling so much. I mean, it was overwhelming. It was truly overwhelming. … I don’t really want to be going out in the public and bringing something home to my immunocompromised husband. … Then it’s like, what? Do you hire somebody to come in, and then how does that get paid for? So, yeah! That’s been a big part of it, at least the stress part of it, like trying to juggle a 40-plus-hour-a-week job and then working around the appointments and having a bad night but then having to get up and get on the phone in the morning and dealing with that. Oh my gosh. It was making me crazy. It really was. … I did start seeing a therapist on the side. I did that for myself once a week for I don’t know how many weeks I did that—for months, actually.(Interview-1)
3.3.5. Realizing the Vaccine May Not Work or Didn’t Work for Their Loved One with CLL
Although not reported in the survey, caregivers who were interviewed also described an experience after the vaccine was deployed during the pandemic that was specific to CLL patients—facing that the vaccine did not protect their spouses from COVID-19. They characterized this experience in two parts. They initially held an immense sense of hope and excitement about the vaccine: “We thought that was going to change everything” (Interview-2). Caregivers even described how they personally made strong commitments to the vaccine, which included traveling long distances to receive it and making lifestyle changes to enhance efficacy: “My husband lost 65 pounds on purpose the first year, because I said, ‘You have to get in shape for the vaccine. The chance of you responding to these vaccines is not high, but it’s really even lower if you’re overweight’” (Inteview-7). Once their spouse was vaccinated, caregivers shared their shock and devastation when then learned their spouse did not develop an immune response. They recalled feeling “a real shock”: “We were so excited to go and get the shot and then he was so crestfallen to learn that he had produced no antibodies”.(Interview-8)
3.3.6. Feeling Cautiously Hopeful about EVUSHELD
He got the monoclonal antibodies just a few weeks ago. That’s like gold. It’s hard to get it. You can’t find it anywhere and he had to be invited, but luckily, they did. I guess his hematologist put a message through and he was invited to get that. So, he just did now, but it’s not a silver bullet. It’s a little bit of a breather. So, we don’t have to maybe be quite as worried. Again, not a silver bullet that you just go out and go—okay! Now, we can go out and do all this stuff.(Interview-1)
We’re a little gun-shy because we thought as you said once the vaccines came out we’d be good. We’d all be good to go and then Omicron came. And I mean Shanghai is closed down. It’s crazy the stuff that still goes on.(Interview-2)
3.3.7. Dealing with Unsupportive or Skeptical Individuals
She used to go walking with some friends of hers just as a little exercise walk, a little socialization. And they didn’t understand. … that she would have to wear a mask if she’s close to them or she’d want to walk six feet away from them. And they didn’t say anything negative but she just got the feeling that, “Oh, they really don’t want to walk with me anymore”.(Interview-9)
We both still wear our masks when we go into a store, and sometimes people are quite rude about things. I had a man come up to us in this store, and he says “I don’t know why you both have a mask on, they’re not doing any good”. He was with his wife, and he was going around harassing people, and I said “Does your wife have cancer? Or hopefully she doesn’t. But my wife has cancer, and we just can’t take a chance on things”. It’s kind of disturbing when people don’t really understand things because they don’t have a problem, and, to me, that’s kind of rude of people. I mean, nobody understands things until it happens to them.(Interivew-12)
Among his family, there were a lot of anti-vaxxers, and even a couple of folks who lean a little bit too QAnon into the “plandemic”. And so that was a huge issue. It’s like, wait a minute, you expect us to come to all these family events. You’re going to hold them indoors. You’re going to shove 12 people in the tiniest room in the house, where you’re then going to serve birthday cake with candles on top, have the birthday person blow on the cake, and then serve it to my husband with the immunocompromised [system] … Check, please. I mean, I couldn’t get out of the house fast enough. I was aghast.(Interview-5)
This lack of support and understanding impacted their ability to socialize, and when it involved loved ones, unsupportive behavior or skepticism contributed to tension and pain: “They’re anti-vax and they’re anti-mask and you know, it’s kind of hard. They won’t do anything to be accommodating to my wife. And so that really hurts”.(Interview-9)
3.4. Aim 2: COVID-19 Resources Caregivers Needed or Wanted during the Pandemic
4. Discussion
4.1. Reducing Caregivers’ Distress/Burden by Attending to Their Risk Information Needs
4.2. Addressing Divergent Risk Perceptions by Providing Interactive Information Tools
4.3. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Chronic Lymphocytic Leukemia (CLL). Available online: https://www.cancer.org/cancer/chronic-lymphocytic-leukemia.html (accessed on 14 January 2023).
- Scarfò, L.; Ferreri, A.J.M.; Ghia, P. Chronic Lymphocytic Leukaemia. Crit. Rev. Oncol. Hematol. 2016, 104, 169–182. [Google Scholar] [CrossRef]
- Gentry, E.; Passwater, C.; Barkett, N.L. Physical, Psychological, Social, and Spiritual Well-Being of Patients with Chronic Lymphocytic Leukemia and Their Caregivers: A Scoping Review. J. Oncol. Navig. Surviv. 2021, 12, 182–191. [Google Scholar]
- Berterö, C.; Eriksson, B.-E.; Ek, A.-C. Explaining Different Profiles in Quality of Life Experiences in Acute and Chronic Leukemia. Cancer Nurs. 1997, 20, 100. [Google Scholar] [CrossRef]
- Berterö, C.; Eriksson, B.-E.; Ek, A.-C. A Substantive Theory of Quality of Life of Adults with Chronic Leukaemia. Int. J. Nurs. Stud. 1997, 34, 9–16. [Google Scholar] [CrossRef] [PubMed]
- Pailler, M.E.; Johnson, T.M.; Kuszczak, S.; Attwood, K.M.; Zevon, M.A.; Griffiths, E.; Thompson, J.; Wang, E.S.; Wetzler, M. Adjustment to Acute Leukemia: The Impact of Social Support and Marital Satisfaction on Distress and Quality of Life Among Newly Diagnosed Patients and Their Caregivers. J. Clin. Psychol. Med. Settings 2016, 23, 298–309. [Google Scholar] [CrossRef] [PubMed]
- Hunt, G.; Longacre, M.; Kent, E.; Weber-Raley, L. Cancer Caregiving in the US: An Intense, Episodic, and Challenging Care Experience; National Alliance for Caregiving: Washington, DC, USA, 2016. [Google Scholar]
- Yu, H.; Zhang, H.; Yang, J.; Liu, C.; Lu, C.; Yang, H.; Huang, W.; Zhou, J.; Fu, W.; Shi, L.; et al. Health Utility Scores of Family Caregivers for Leukemia Patients Measured by EQ-5D-3L: A Cross-Sectional Survey in China. BMC Cancer 2018, 18, 950. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eichhorst, B.; Hallek, M.; Goede, V. Management of Unfit Elderly Patients with Chronic Lymphocytic Leukemia. Eur. J. Intern. Med. 2018, 58, 7–13. [Google Scholar] [CrossRef]
- Goyal, N.G.; Maddocks, K.J.; Johnson, A.J.; Byrd, J.C.; Westbrook, T.D.; Andersen, B.L. Cancer-Specific Stress and Trajectories of Psychological and Physical Functioning in Patients With Relapsed/Refractory Chronic Lymphocytic Leukemia. Ann. Behav. Med. 2018, 52, 287–298. [Google Scholar] [CrossRef]
- Vijenthira, A.; Gong, I.Y.; Fox, T.A.; Booth, S.; Cook, G.; Fattizzo, B.; Martín-Moro, F.; Razanamahery, J.; Riches, J.C.; Zwicker, J.; et al. Outcomes of Patients with Hematologic Malignancies and COVID-19: A Systematic Review and Meta-Analysis of 3377 Patients. Blood 2020, 136, 2881–2892. [Google Scholar] [CrossRef]
- Andersen, M.A.; Niemann, C.U.; Rostgaard, K.; Dalby, T.; Sørrig, R.; Weinberger, D.M.; Hjalgrim, H.; Harboe, Z.B. Differences and Temporal Changes in Risk of Invasive Pneumococcal Disease in Adults with Hematological Malignancies: Results from a Nationwide 16-Year Cohort Study. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2021, 72, 463–471. [Google Scholar] [CrossRef]
- Arellano-Llamas, A.A.; Vela-Ojeda, J.; Hernandez-Caballero, A. Chronic Lymphocytic Leukemia in the SARS-CoV-2 Pandemic. Curr. Oncol. Rep. 2022, 24, 209–213. [Google Scholar] [CrossRef]
- Kochneva, O.L.; Kislova, M.; Zhelnova, E.I.; Petrenko, A.A.; Baryakh, E.A.; Yatskov, K.V.; Dmitrieva, E.A.; Misurina, E.N.; Nikitin, K.E.; Vasilieva, E.J.; et al. COVID-19 in Patients with Chronic Lymphocytic Leukemia: A Moscow Observational Study. Leuk. Lymphoma 2022, 63, 1607–1616. [Google Scholar] [CrossRef] [PubMed]
- Kent, E.E.; Ornstein, K.A.; Dionne-Odom, J.N. The Family Caregiving Crisis Meets an Actual Pandemic. J. Pain Symptom Manage. 2020, 60, e66–e69. [Google Scholar] [CrossRef]
- Whitaker, J.A.; Parikh, S.A.; Shanafelt, T.D.; Kay, N.E.; Kennedy, R.B.; Grill, D.E.; Goergen, K.M.; Call, T.G.; Kendarian, S.S.; Ding, W.; et al. The Humoral Immune Response to High-Dose Influenza Vaccine in Persons with Monoclonal B-Cell Lymphocytosis (MBL) and Chronic Lymphocytic Leukemia (CLL). Vaccine 2021, 39, 1122–1130. [Google Scholar] [CrossRef]
- Greenberger, L.M.; Saltzman, L.A.; Senefeld, J.W.; Johnson, P.W.; DeGennaro, L.J.; Nichols, G.L. Antibody Response to SARS-CoV-2 Vaccines in Patients with Hematologic Malignancies. Cancer Cell 2021, 39, 1031–1033. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, L.C.; Thakkar, A.; Campbell, S.T.; Forest, S.K.; Pradhan, K.; Gonzalez-Lugo, J.D.; Quinn, R.; Bhagat, T.D.; Choudhary, G.S.; McCort, M.; et al. Efficacy of Booster Doses in Augmenting Waning Immune Responses to COVID-19 Vaccine in Patients with Cancer. Cancer Cell 2022, 40, 3–5. [Google Scholar] [CrossRef]
- Morawska, M. Reasons and Consequences of COVID-19 Vaccine Failure in Patients with Chronic Lymphocytic Leukemia. Eur. J. Haematol. 2022, 108, 91–98. [Google Scholar] [CrossRef]
- Rodríguez-Mora, S.; Corona, M.; Torres, M.; Casado-Fernández, G.; García-Pérez, J.; Ramos-Martín, F.; Vigón, L.; Manzanares, M.; Mateos, E.; Martín-Moro, F.; et al. Early Cellular and Humoral Responses Developed in Oncohematological Patients after Vaccination with One Dose against COVID-19. J. Clin. Med. 2022, 11, 2803. [Google Scholar] [CrossRef] [PubMed]
- Rosa, W.E.; Ferrell, B.R.; Applebaum, A.J. The Alleviation of Suffering during the COVID-19 Pandemic. Palliat. Support. Care 2020, 18, 376–378. [Google Scholar] [CrossRef] [PubMed]
- Fisher, C.L.; Wright, K.B.; Hampton, C.N.; Vasquez, T.S.; Kastrinos, A.; Applebaum, A.J.; Sae-Hau, M.; Weiss, E.S.; Lincoln, G.; Bylund, C.L. Blood Cancer Caregiving during COVID-19: Understanding Caregivers’ Needs. Transl. Behav. Med. 2021, 11, 1187–1197. [Google Scholar] [CrossRef] [PubMed]
- Park, Y.M.; Kearney, G.D.; Wall, B.; Jones, K.; Howard, R.J.; Hylock, R.H. COVID-19 Deaths in the United States: Shifts in Hot Spots over the Three Phases of the Pandemic and the Spatiotemporally Varying Impact of Pandemic Vulnerability. Int. J. Environ. Res. Public. Health 2021, 18, 8987. [Google Scholar] [CrossRef]
- Glaser, B.G.; Strauss, A.L. The Constant Comparative Method of Qualitative Analysis. In The Discovery of Grounded Theory: Strategies for Qualitative Research; Aldine Transaction: New Brunswick, NJ, USA, 1967; pp. 101–117. ISBN 978-0-202-30260-7. [Google Scholar]
- Strauss, A.L.; Corbin, J.M. Basics of Qualitative Research: Techniques and Procedures for Developing Grounded Theory; Sage: Thousand Oaks, CA, USA, 1998. [Google Scholar]
- Daly, K. Qualitative Methods for Family Studies & Human Development; SAGE Publications Inc.: Thousand Oaks, CA, USA, 2007. [Google Scholar]
- Owen, W.F. Interpretive Themes in Relational Communication. Q. J. Speech 1984, 70, 274–287. [Google Scholar] [CrossRef]
- Hennink, M.; Kaiser, B.N. Sample Sizes for Saturation in Qualitative Research: A Systematic Review of Empirical Tests. Soc. Sci. Med. 2022, 292, 114523. [Google Scholar] [CrossRef] [PubMed]
- Morse, J.M.; Barrett, M.; Mayan, M.; Olson, K.; Spiers, J. Verification Strategies for Establishing Reliability and Validity in Qualitative Research. Int. J. Qual. Methods 2002, 1, 13–22. [Google Scholar] [CrossRef]
- Sandelowski, M.; Leeman, J. Writing Usable Qualitative Health Research Findings. Qual. Health Res. 2012, 22, 1404–1413. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lloyd-Evans, B.; Giacco, D.; Forsyth, R.; Nebo, C.; Mann, F.; Johnson, S. Social Isolation in Mental Health: A Conceptual and Methodological Review. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1451–1461. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bevans, M.F.; Sternberg, E.M. Caregiving Burden, Stress, and Health Effects Among Family Caregivers of Adult Cancer Patients. JAMA 2012, 307, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Khalaila, R.; Cohen, M. Emotional Suppression, Caregiving Burden, Mastery, Coping Strategies and Mental Health in Spousal Caregivers. Aging Ment. Health 2016, 20, 908–917. [Google Scholar] [CrossRef] [PubMed]
- Campbell-Salome, G.; Fisher, C.L.; Wright, K.B.; Lincoln, G.; Applebaum, A.J.; Sae-Hau, M.; Weiss, E.S.; Bylund, C.L. Impact of the Family Communication Environment on Burden and Clinical Communication in Blood Cancer Caregiving. Psychooncology 2022, 31, 1212–1220. [Google Scholar] [CrossRef]
- Bevan, J.; Murphy, M.; Lannutti, P.; Slatcher, R.; Balzarini, R. A Descriptive Literature Review of Early Research on COVID-19 and Close Relationships. J. Soc. Pers. Relat. 2023, 40, 201–253. [Google Scholar] [CrossRef]
- Hernandez, R.A.; Colaner, C. “This Is Not the Hill to Die on. Even If We Literally Could Die on This Hill”: Examining Communication Ecologies of Uncertainty and Family Communication About COVID-19. Am. Behav. Sci. 2021, 65, 956–975. [Google Scholar] [CrossRef]
- Morrissey, B.; Biwa, V.; Johnson, A.J. Arguing about Social Distancing and Family Relationships. In Proceedings of the Family Communication Association for the National Communication Association’s Annual Meeting, Seattle, WA, USA, 18–21 November 2021. [Google Scholar]


{kind=link}
| CLL Caregivers Struggled with These Challenges | Characterized by |
|---|---|
| [since the pandemic began] | |
| Coping with distress |
|
| Living in isolation |
|
| Losing in-person care opportunities |
|
| Increasing caregiving burden |
|
| [after the vaccine was deployed] | |
| Realizing the vaccine may not work or didn’t work for their loved one with CLL |
|
| Feeling cautiously hopeful about EVUSHELD |
|
| Dealing with unsupportive or Skeptical individuals |
|
| Resource Need | Description | Caregiver Responses |
|---|---|---|
| COVID-19 Risk Information (n = 83) | Expert information addressing COVID-19 risk with targeted information specific to CLL patients: how the virus will affect them, what to do if they test positive, treatment options, antigen tests to take, and resources to share with family to explain their risk. | Specific info on how COVID impacts the CLL patient—are they even more susceptible now to even the simplest bacterial infection from a cut or scratch, or from any virus they might encounter. |
| Something in print to show family and friends WHY we are not meeting up with them and having them over. They don’t understand. | ||
| Vaccination Information/Access (n = 60) | Information about the vaccine: efficacy, medicines that might affect efficacy, how much immunity someone with CLL has, eligibility for CLL patients, treatment options when vaccines is ineffective, and when to receive the vaccine after immunotherapy. | Vaccine effectiveness for the different types of CLL and medications. |
| Safety/Precaution Information Including Equipment Access (n = 50) | Information about and access to cautionary measures (safety recommendations for patients with CLL): guidance regarding disinfecting surfaces, how to safely interact with immunocompromised people, access to masks and sanitizers, and websites indicating where to get equipment. | More what to do not to do to be safe. Kind of had to figure out initially on our own that vaccinations were not going to be effective for my wife based on medication Ibrutinib she was taking. |
| Objective, Reliable, Frequent/Ongoing Information (n = 35) | Desire for constant flow of information from objective, reliable, truthful, and less politicized and scientific sources to stay current. | I recently just discovered that CLL patients were eligible for a second booster. I’m frustrated because I’m very informed otherwise. This information fell through the cracks. |
| Information/Access to Monoclonal Infusions (n = 24) | Information on monoclonal antibody treatment: types of infusion (e.g., EVUSHELD and Remdesivir), where to find it, and how to access monoclonal infusions. | Wish he could have had monoclonal antibodies but these were not available at this time. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bagautdinova, D.; Bacharz, K.C.; Bylund, C.L.; Sae-Hau, M.; Weiss, E.S.; Rajotte, M.; Lincoln, G.; Vasquez, T.S.; Parker, N.D.; Wright, K.B.; et al. Understanding the Impact of COVID-19 on Chronic Lymphocytic Leukemia (CLL) Caregiving and Related Resource Needs. J. Clin. Med. 2023, 12, 1648. https://doi.org/10.3390/jcm12041648
Bagautdinova D, Bacharz KC, Bylund CL, Sae-Hau M, Weiss ES, Rajotte M, Lincoln G, Vasquez TS, Parker ND, Wright KB, et al. Understanding the Impact of COVID-19 on Chronic Lymphocytic Leukemia (CLL) Caregiving and Related Resource Needs. Journal of Clinical Medicine. 2023; 12(4):1648. https://doi.org/10.3390/jcm12041648
Chicago/Turabian StyleBagautdinova, Diliara, Kelsey C. Bacharz, Carma L. Bylund, Maria Sae-Hau, Elisa S. Weiss, Michelle Rajotte, Greg Lincoln, Taylor S. Vasquez, Naomi D. Parker, Kevin B. Wright, and et al. 2023. "Understanding the Impact of COVID-19 on Chronic Lymphocytic Leukemia (CLL) Caregiving and Related Resource Needs" Journal of Clinical Medicine 12, no. 4: 1648. https://doi.org/10.3390/jcm12041648