
Norepinephrine May Exacerbate Septic Acute Kidney Injury: A Narrative Review
 , , , ,
, , , , 
Abstract
:1. Plain Language Summary
2. Key Points
- Septic-AKI (S-AKI) is clinically distinct from AKI without sepsis.
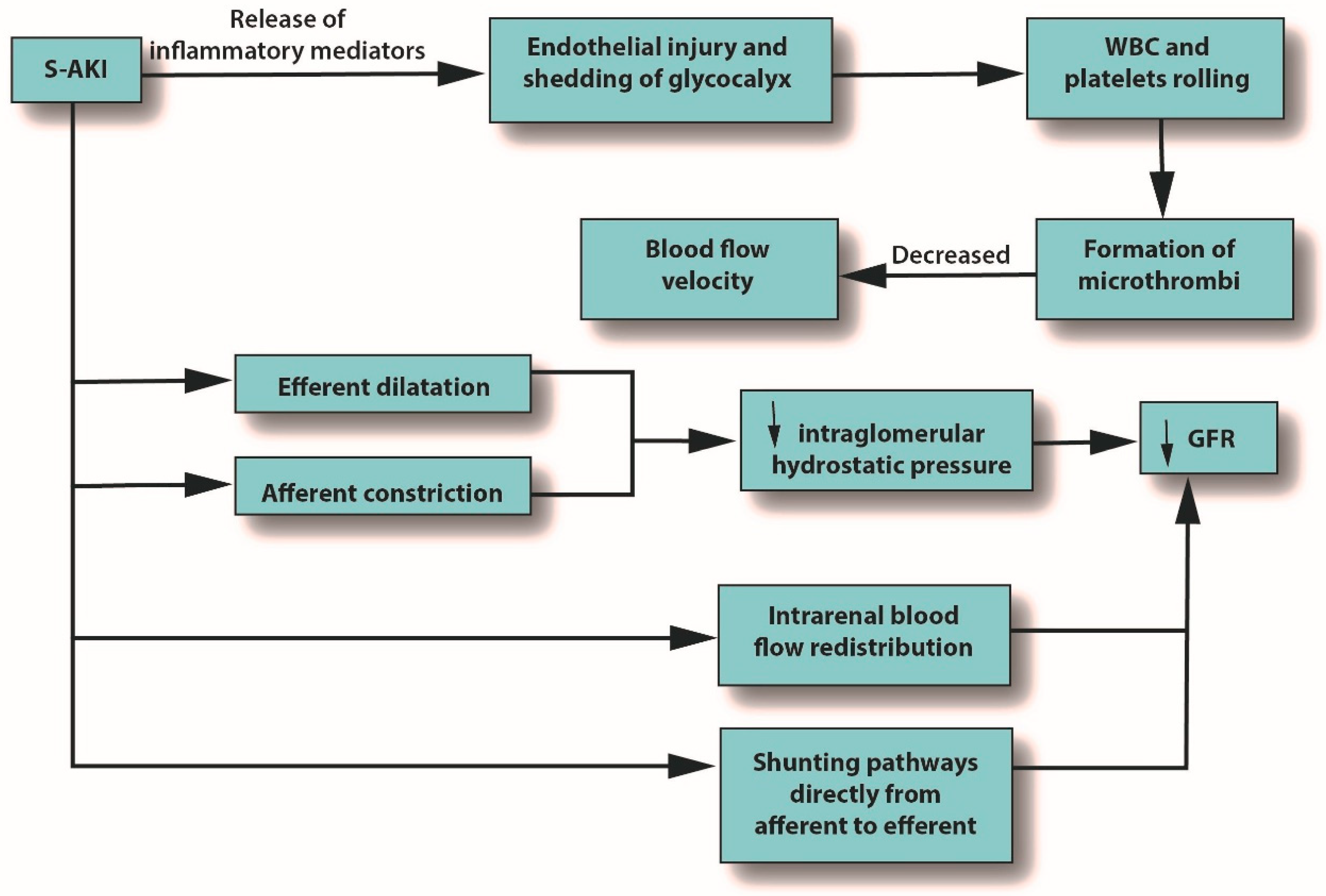
- Microcirculatory abnormalities can occur in S-AKI due to endothelial injury and shedding of the glycocalyx, which can result in reduced blood flow velocity.
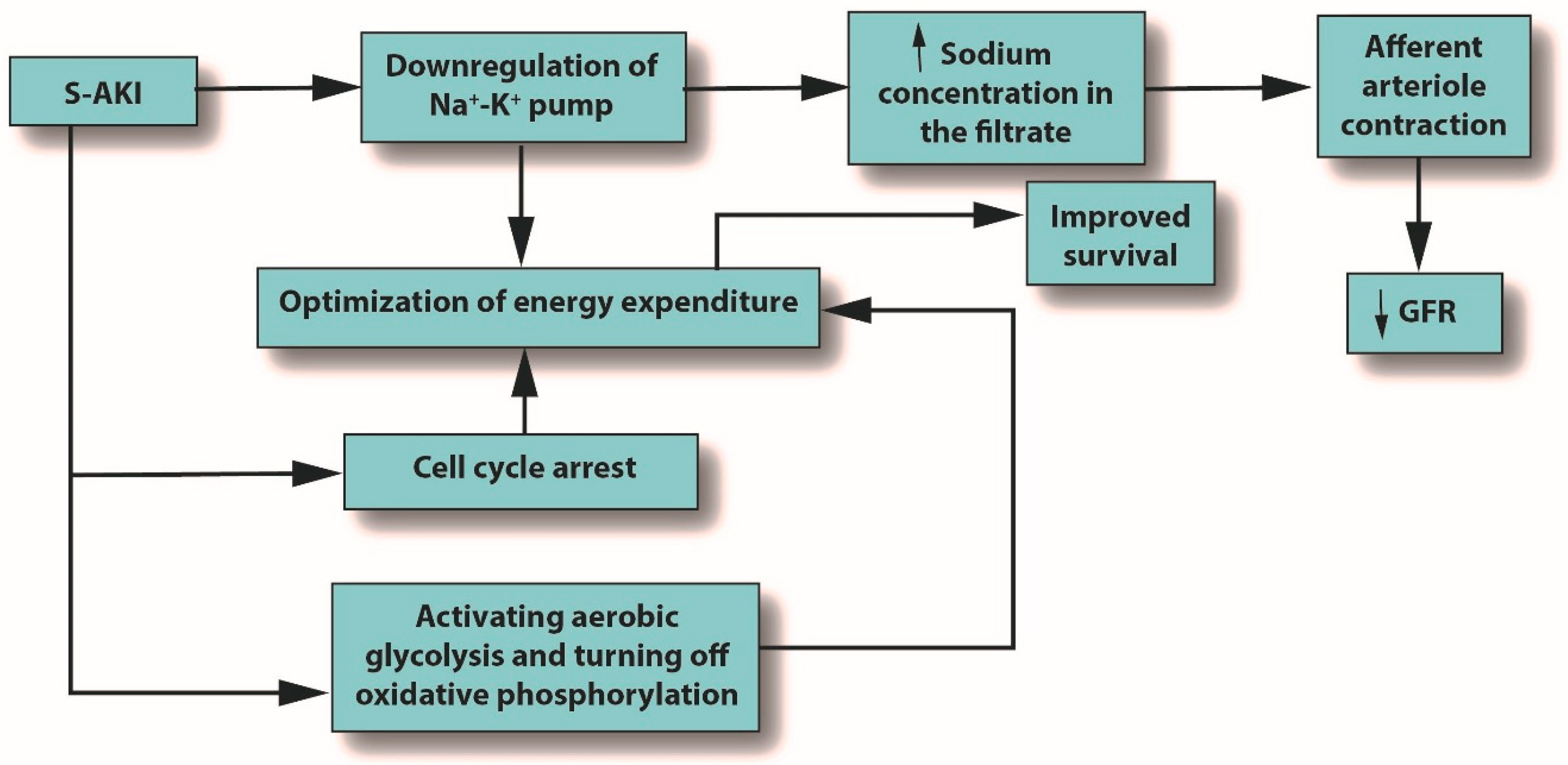
- Norepinephrine is recommended as the first-line treatment for S-AKI. It increases the glomerular filtration rate, increases sodium filtration and reabsorption, boosts renal blood flow, and has no effect on urine flow or renal vascular resistance. However, norepinephrine can reduce medullary tissue oxygen by half.
- Although 20% of cardiac output is delivered to the renal system, the renal medulla is vulnerable to hypoxia, likely due to vascular congestion.
- In head-to-head clinical studies of norepinephrine vs. vasopressin, there was no clear superiority for norepinephrine, and in some studies, vasopressin had lower mortality. In meta-analyses, vasopressin did not confer a clear-cut mortality benefit over standard care.
3. Introduction
4. Methods
5. Results
5.1. Diagnostic Challenges in S-AKI
5.2. Managing S-AKI
5.3. The Pathophysiology of S-AKI
5.4. Septic Shock
5.5. Norepinephrine in S-AKI
6. Discussion
7. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Singer, M.; Deutschman, C.S.; Seymour, C.W.; Shankar-Hari, M.; Annane, D.; Bauer, M.; Bellomo, R.; Bernard, G.R.; Chiche, J.-D.; Coopersmith, C.M.; et al. The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 801–810. [Google Scholar] [PubMed]
- van der Poll, T.; Shankar-Hari, M.; Wiersinga, W.J. The immunology of sepsis. Immunity 2021, 54, 2450–2464. [Google Scholar] [CrossRef] [PubMed]
- Rudd, K.E.; Johnson, S.C.; Agesa, K.M.; Shackelford, K.A.; Tsoi, D.; Kievlan, D.R.; Colombara, D.V.; Ikuta, K.S.; Kissoon, N.; Finfer, S.; et al. Global, regional, and national sepsis incidence and mortality, 1990–2017: Analysis for the Global Burden of Disease Study. Lancet 2020, 395, 200–211. [Google Scholar] [CrossRef] [PubMed]
- Fleischmann-Struzek, C.; Goldfarb, D.M.; Schlattmann, P.; Schlapbach, L.J.; Reinhart, K.; Kissoon, N. The global burden of paediatric and neonatal sepsis: A systematic review. Lancet Respir. Med. 2018, 6, 223–230. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Phillips, G.S.; Levy, M.L.; Seymour, C.W.; Liu, V.X.; Deutschman, C.S.; Angus, D.C.; Rubenfeld, G.D.; Singer, M. Developing a New Definition and Assessing New Clinical Criteria for Septic Shock: For the Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA 2016, 315, 775–787. [Google Scholar]
- Cecconi, M.; Evans, L.; Levy, M.; Rhodes, A. Sepsis and septic shock. Lancet 2018, 392, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Peerapornratana, S.; Manrique-Caballero, C.L.; Gómez, H.; Kellum, J.A. Acute kidney injury from sepsis: Current concepts, epidemiology, pathophysiology, prevention and treatment. Kidney Int. 2019, 96, 1083–1099. [Google Scholar] [CrossRef]
- Bagshaw, S.M.; Lapinsky, S.; Dial, S.; Arabi, Y.; Dodek, P.; Wood, G.; Ellis, P.; Guzman, J.; Marshall, J.; Parrillo, J.E.; et al. Acute kidney injury in septic shock: Clinical outcomes and impact of duration of hypo-tension prior to initiation of antimicrobial therapy. Intensive Care Med. 2009, 35, 871–881. [Google Scholar] [CrossRef]
- Bouchard, J.; Acharya, A.; Cerda, J.; Maccariello, E.R.; Madarasu, R.C.; Tolwani, A.J.; Liang, X.; Fu, P.; Liu, Z.-H.; Mehta, R.L. A Prospective International Multicenter Study of AKI in the Intensive Care Unit. Clin. J. Am. Soc. Nephrol. 2015, 10, 1324–1331. [Google Scholar] [CrossRef]
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensive Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef]
- Tain, Y.-L.; Liu, C.-L.; Kuo, H.-C.; Hsu, C.-N. Kidney Function Trajectory within Six Months after Acute Kidney Injury Inpatient Care and Subsequent Adverse Kidney Outcomes: A Retrospective Cohort Study. J. Pers. Med. 2022, 12, 1606. [Google Scholar] [CrossRef] [PubMed]
- Liu, J.; Xie, H.; Ye, Z.; Li, F.; Wang, L. Rates, predictors, and mortality of sepsis-associated acute kidney injury: A systematic re-view and meta-analysis. BMC Nephrol. 2020, 21, 318. [Google Scholar]
- Ma, S.; Evans, R.G.; Iguchi, N.; Tare, M.; Parkington, H.C.; Bellomo, R.; May, C.N.; Lankadeva, Y.R. Sepsis-induced acute kidney injury: A disease of the microcirculation. Microcirculation 2019, 26, e12483. [Google Scholar] [CrossRef] [PubMed]
- Lankadeva, Y.R.; Okazaki, N.; Evans, R.G.; Bellomo, R.; May, C.N. Renal Medullary Hypoxia: A New Therapeutic Target for Sep-tic Acute Kidney Injury? Semin. Nephrol. 2019, 39, 543–553. [Google Scholar] [PubMed]
- Pourmand, A.; Pyle, M.; Yamane, D.; Sumon, K.; Frasure, S.E. The utility of point-of-care ultrasound in the assessment of volume status in acute and critically ill patients. World J. Emerg. Med. 2019, 10, 232–238. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Rhodes, A.; Annane, D.; Gerlach, H.; Opal, S.M.; Sevransky, J.E.; Sprung, C.L.; Douglas, I.S.; Jaeschke, R.; et al. Surviving sepsis campaign: International guidelines for management of severe sepsis and septic shock: 2012. Crit. Care Med. 2013, 41, 580–637. [Google Scholar]
- Landry, D.W.; Levin, H.R.; Gallant, E.M.; Ashton, R.C.; Seo, S.; D’Alessandro, D.; Oz, M.C.; Oliver, J.A. Vasopressin Deficiency Contributes to the Vasodilation of Septic Shock. Circulation 1997, 95, 1122–1125. [Google Scholar] [CrossRef]
- Huang, H.; Wu, C.; Shen, Q.; Xu, H.; Fang, Y.; Mao, W. The effect of early vasopressin use on patients with septic shock: A systematic review and meta-analysis. Am. J. Emerg. Med. 2021, 48, 203–208. [Google Scholar]
- Landoni, G.; Bove, T.; Székely, A.; Comis, M.; Rodseth, R.N.; Pasero, D.; Ponschab, M.; Mucchetti, M.; Azzolini, M.L.; Caramelli, F.; et al. Reducing Mortality in Acute Kidney Injury Patients: Systematic Review and International Web-Based Survey. J. Cardiothorac. Vasc. Anesth. 2013, 27, 1384–1398. [Google Scholar] [CrossRef]
- Mouncey, P.R.; Richards-Belle, A.; Thomas, K.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Camsooksai, J.; Darnell, R.; Gordon, A.C.; Henry, D.; et al. Reduced exposure to vasopressors through permissive hypotension to reduce mortality in critically ill people aged 65 and over: The 65 RCT. Health Technol. Assess. 2021, 25, 1–90. [Google Scholar]
- Nagendran, M.; Russell, J.A.; Walley, K.R.; Brett, S.J.; Perkins, G.D.; Hajjar, L.; Mason, A.J.; Ashby, D.; Gordon, A.C. Vasopressin in septic shock: An individual patient data meta-analysis of randomised controlled trials. Intensive Care Med. 2019, 45, 844–855. [Google Scholar]
- Chousterman, B.G.; Swirski, F.K.; Weber, G.F. Cytokine storm and sepsis disease pathogenesis. Semin. Immunopathol. 2017, 39, 517–528. [Google Scholar] [CrossRef]
- Alobaidi, R.; Basu, R.K.; Goldstein, S.L.; Bagshaw, S.M. Sepsis-associated acute kidney injury. Semin. Nephrol. 2015, 35, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Mayr, F.B.; Yende, S.; Angus, D.C. Epidemiology of severe sepsis. Virulence 2014, 5, 4–11. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J.; Cristofaro, P.; Carlet, J.; Opal, S. New method of classifying infections in critically ill patients. Crit. Care Med. 2004, 32, 1510–1526. [Google Scholar] [CrossRef] [PubMed]
- Rangel-Frausto, M.S. The epidemiology of bacterial sepsis. Infect. Dis. Clin. N. Am. 1999, 13, 299–312. [Google Scholar] [CrossRef]
- Bassetti, M.; Vena, A.; Giacobbe, D.R.; Castaldo, N. Management of Infections Caused by Multidrug-resistant Gram-negative Pathogens: Recent Advances and Future Directions. Arch. Med. Res. 2021, 52, 817–827. [Google Scholar] [CrossRef] [PubMed]
- Kingren, M.S.; Starr, M.E.; Saito, H. Divergent Sepsis Pathophysiology in Older Adults. Antioxid. Redox Signal. 2021, 35, 1358–1375. [Google Scholar] [CrossRef] [PubMed]
- Melzer, M.; Welch, C. Does the presence of a urinary catheter predict severe sepsis in a bacteraemic cohort? J. Hosp. Infect. 2017, 95, 376–382. [Google Scholar] [CrossRef]
- Gudiol, C.; Albasanz-Puig, A.; Cuervo, G.; Carratalà, J. Understanding and Managing Sepsis in Patients with Cancer in the Era of Antimicrobial Resistance. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- Tongyoo, S.; Permpikul, C.; Mongkolpun, W.; Vattanavanit, V.; Udompanturak, S.; Kocak, M.; Meduri, G.U. Hydrocortisone treatment in early sepsis-associated acute respiratory distress syndrome: Results of a randomized controlled trial. Crit. Care 2016, 20, 329. [Google Scholar] [PubMed]
- Iba, T.; Levy, J.H. Sepsis-induced Coagulopathy and Disseminated Intravascular Coagulation. Anesthesiology 2020, 132, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Brück, E.; Schandl, A.; Bottai, M.; Sackey, P. The impact of sepsis, delirium, and psychological distress on self-rated cognitive function in ICU survivors—A prospective cohort study. J. Intensive Care 2018, 6, 1–8. [Google Scholar]
- Nandagopal, N.; Reddy, P.K.; Ranganathan, L.; Ramakrishnan, N.; Annigeri, R.; Venkataraman, R. Comparison of Epidemiology and Outcomes of Acute Kidney Injury in Critically Ill Patients with and without Sepsis. Indian J. Crit. Care Med. 2020, 24, 258–262. [Google Scholar]
- Bellomo, R.; Ronco, C.; Kellum, J.A.; Mehta, R.L.; Palevsky, P. Acute renal failure—Definition, outcome measures, animal models, fluid therapy and information technology needs: The Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit. Care 2004, 8, R204–R212. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A.; Acute Kidney Injury Network. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef]
- Xie, Y.; Huang, P.; Zhang, J.; Tian, R.; Jin, W.; Xie, H.; Du, J.; Zhou, Z.; Wang, R. Biomarkers for the diagnosis of sepsis-associated acute kidney injury: Systematic review and meta-analysis. Ann. Palliat. Med. 2021, 10, 4159–4173. [Google Scholar] [CrossRef] [PubMed]
- Khwaja, A. KDIGO Clinical Practice Guidelines for Acute Kidney Injury. Nephron Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Vijay, P.; Lal, B.B.; Sood, V.; Khanna, R.; Alam, S. Cystatin C: Best biomarker for acute kidney injury and estimation of glomerular filtration rate in childhood cirrhosis. Eur. J. Pediatr. 2021, 180, 3287–3295. [Google Scholar] [CrossRef]
- Oh, D.-J. A long journey for acute kidney injury biomarkers. Ren. Fail. 2020, 42, 154–165. [Google Scholar] [CrossRef]
- Gavelli, F.; Castello, L.M.; Avanzi, G.C. Management of sepsis and septic shock in the emergency department. Intern. Emerg. Med. 2021, 16, 1649–1661. [Google Scholar] [CrossRef]
- Bonventre, J.V. Kidney Injury Molecule-1 (KIM-1): A specific and sensitive biomarker of kidney injury. Scand. J. Clin. Lab. Investig. 2008, 68, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Changan, W.; Liu, J.; Liang, B.; Wang, X.; Wang, C. Clinical significance of novel biomarker NGAL in early diagnosis of acute renal injury. Exp. Ther. Med. 2017, 14, 5017–5021. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Yang, X.; Shu, H.; Yu, Y.; Pan, S.; Xu, J.; Shang, Y. Bioinformatic analysis identifies potential biomarkers and therapeutic targets of septic-shock-associated acute kidney injury. Hereditas 2021, 158, 13. [Google Scholar]
- Hjortrup, P.B.; The CLASSIC Trial Group; Haase, N.; Bundgaard, H.; Thomsen, S.L.; Winding, R.; Pettilä, V.; Aaen, A.; Lodahl, D.; Berthelsen, R.E.; et al. Restricting volumes of resuscitation fluid in adults with septic shock after initial management: The CLASSIC randomised, parallel-group, multicentre feasibility trial. Intensive Care Med. 2016, 42, 1695–1705. [Google Scholar] [CrossRef]
- Watson, X.; Cecconi, M. Liberal or restrictive dilemma—That’s a CLASSIC! Ann. Transl. Med. 2017, 5 (Suppl. S1), S7. [Google Scholar] [CrossRef] [PubMed]
- Bouchard, J.; Soroko, S.B.; Chertow, G.M.; Himmelfarb, J.; Ikizler, T.A.; Paganini, E.P.; Mehta, R.L. Fluid accumulation, survival and recovery of kidney function in critically ill pa-tients with acute kidney injury. Kidney Int. 2009, 76, 422–427. [Google Scholar]
- Evans, L.; Rhodes, A.; Alhazzani, W.; Antonelli, M.; Coopersmith, C.M.; French, C.; Machado, F.R.; Mcintyre, L.; Ostermann, M.; Prescott, H.C.; et al. Surviving sepsis campaign: International guidelines for management of sepsis and septic shock 2021. Intensive Care Med. 2021, 47, 1181–1247. [Google Scholar] [CrossRef]
- Jozwiakì, M.; Hamzaoui, O.; Monnet, X.; Teboul, J.-L. Fluid resuscitation during early sepsis: A need for individualization. Minerva Anestesiol. 2018, 84, 987–992. [Google Scholar] [CrossRef]
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Levy, M.M.; Evans, L.E.; Rhodes, A. The Surviving Sepsis Campaign Bundle: 2018 update. Intensive Care Med. 2018, 44, 925–928. [Google Scholar] [CrossRef] [PubMed]
- Barbar, S.D.; Binquet, C.; Monchi, M.; Bruyère, R.; Quenot, J.-P. Impact on mortality of the timing of renal replacement therapy in patients with severe acute kidney injury in septic shock: The IDEAL-ICU study (initiation of dialysis early versus delayed in the intensive care unit): Study protocol for a randomized controlled trial. Trials 2014, 15, 270. [Google Scholar] [CrossRef]
- Shah, S.R.; Tunio, S.A.; Arshad, M.H.; Moazzam, Z.; Noorani, K.; Feroze, A.M.; Shafquat, M.; Hussain, H.S.; Jeoffrey, S.A. Acute Kidney Injury Recognition and Management: A Review of the Literature and Current Evidence. Glob. J. Health Sci. 2015, 8, 120–124. [Google Scholar] [CrossRef]
- Macedo, E.; Mehta, R.L. Prerenal failure: From old concepts to new paradigms. Curr. Opin. Crit. Care 2009, 15, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Makris, K.; Spanou, L. Acute Kidney Injury: Definition, Pathophysiology and Clinical Phenotypes. Clin. Biochem. Rev. 2016, 37, 85–98. [Google Scholar]
- Mårtensson, J.; Bellomo, R. Pathophysiology of Septic Acute Kidney Injury. Contrib. Nephrol. 2016, 187, 36–46. [Google Scholar] [PubMed]
- Bellomo, R.; Wan, L.; Langenberg, C.; May, C. Septic Acute Kidney Injury: New Concepts. Nephron Exp. Nephrol. 2008, 109, e95–e100. [Google Scholar] [CrossRef]
- Bouglé, A.; Duranteau, J. Pathophysiology of Sepsis-Induced Acute Kidney Injury: The Role of Global Renal Blood Flow and Renal Vascular Resistance. Contrib. Nephrol. 2011, 174, 89–97. [Google Scholar] [CrossRef]
- Amarante-Mendes, G.P.; Adjemian, S.; Branco, L.M.; Zanetti, L.C.; Weinlich, R.; Bortoluci, K.R. Pattern Recognition Receptors and the Host Cell Death Molecular Machinery. Front. Immunol. 2018, 9, 2379. [Google Scholar] [CrossRef]
- McKernan, D.P. Pattern recognition receptors as potential drug targets in inflammatory disorders. Adv. Protein Chem. Struct. Biol. 2020, 119, 65–109. [Google Scholar] [CrossRef]
- Chen, F.; Zou, L.; Williams, B.; Chao, W. Targeting Toll-Like Receptors in Sepsis: From Bench to Clinical Trials. Antioxid. Redox Signal 2021, 35, 1324–1339. [Google Scholar] [CrossRef] [PubMed]
- Kumar, V. Toll-like receptors in sepsis-associated cytokine storm and their endogenous negative regulators as future immunomodulatory targets. Int. Immunopharmacol. 2020, 89 Pt B, 107087. [Google Scholar]
- Zeng, C.; Chen, Q.; Zhang, K.; Chen, Q.; Song, S.; Fang, X. Hepatic hepcidin protects against polymicrobial sepsis in mice by regu-lating host iron status. Anesthesiology 2015, 122, 374–386. [Google Scholar] [PubMed]
- Qiu, Z.-L.; Yan, B.-Q.; Zhao, R.; Xu, D.-W.; Shen, K.; Deng, X.-Q.; Lu, S.-Q. Combination of hepcidin with neutrophil gelatinase-associated lipocalin for prediction of the development of sepsis-induced acute kidney injury. Clin. Chim. Acta 2021, 523, 38–44. [Google Scholar] [CrossRef] [PubMed]
- Scindia, Y.; Wlazlo, E.; Leeds, J.; Loi, V.; Ledesma, J.; Cechova, S.; Ghias, E.; Swaminathan, S. Protective Role of Hepcidin in Polymicrobial Sepsis and Acute Kidney Injury. Front. Pharmacol. 2019, 10, 615. [Google Scholar] [CrossRef]
- Frische, S. Glomerular filtration rate in early diabetes: Ongoing discussions of causes and mechanisms. J. Nephrol. 2011, 24, 537–540. [Google Scholar] [CrossRef]
- Stockand, J.D.; Sansom, S.C. Regulation of filtration rate by glomerular mesangial cells in health and diabetic renal disease. Am. J. Kidney Dis. 1997, 29, 971–981. [Google Scholar] [CrossRef]
- Jani, A.; Martin, S.L.; Jain, S.; Keys, D.; Edelstein, C.L. Renal adaptation during hibernation. Am. J. Physiol. Physiol. 2013, 305, F1521–F1532. [Google Scholar] [CrossRef]
- Ratigan, E.D.; McKay, D.B. Exploring principles of hibernation for organ preservation. Transplant. Rev. 2016, 30, 13–19. [Google Scholar] [CrossRef]
- Castillo, J.P.; Rui, H.; Basilio, D.; Das, A.; Roux, B.; Latorre, R.; Bezanilla, F.; Holmgren, M. Mechanism of potassium ion uptake by the Na+/K+-ATPase. Nat. Commun. 2015, 6, 7622. [Google Scholar] [CrossRef]
- Bell, P.D.; Lapointe, J.Y.; Peti-Peterdi, J. Macula Densa Cell Signaling. Annu. Rev. Physiol. 2003, 65, 481–500. [Google Scholar] [CrossRef] [PubMed]
- Inscho, E.W.; Imig, J.D.; Cook, A.K. Afferent and Efferent Arteriolar Vasoconstriction to Angiotensin II and Norepinephrine In-volves Release of Ca2+ from Intracellular Stores. Hypertension 1997, 29, 222–227. [Google Scholar] [PubMed] [Green Version]
- Jamshidi, P.; Najafi, F.; Mostafaei, S.; Shakiba, E.; Pasdar, Y.; Hamzeh, B.; Moradinazar, M. Investigating associated factors with glomerular filtration rate: Structural equation modeling. BMC Nephrol. 2020, 21, 30. [Google Scholar] [CrossRef]
- Annane, D.; Bellissant, E.; Cavaillon, J.M. Septic shock. Lancet 2005, 365, 63–78. [Google Scholar] [PubMed]
- Schefold, J.C.; Hasper, D.; Volk, H.D.; Reinke, P. Sepsis: Time has come to focus on the later stages. Med. Hypotheses 2008, 71, 203–208. [Google Scholar] [CrossRef]
- Atzori, M.; Cuevas-Olguin, R.; Esquivel-Rendon, E.; Garcia-Oscos, F.; Salgado-Delgado, R.C.; Saderi, N.; Miranda-Morales, M.; Treviño, M.; Pineda, J.C.; Salgado, H. Locus Ceruleus Norepinephrine Release: A Central Regulator of CNS Spatio-Temporal Activation? Front. Synaptic Neurosci. 2016, 8, 25. [Google Scholar] [CrossRef]
- Finnell, J.E.; Moffitt, C.M.; Hesser, L.A.; Harrington, E.; Melson, M.N.; Wood, C.S.; Wood, S.K. The contribution of the locus coeruleus-norepinephrine system in the emergence of defeat-induced inflammatory priming. Brain Behav. Immun. 2019, 79, 102–113. [Google Scholar] [CrossRef]
- Stolk, R.F.; Van Der Pasch, E.; Naumann, F.; Schouwstra, J.; Bressers, S.; Van Herwaarden, A.E.; Gerretsen, J.; Schambergen, R.; Ruth, M.M.; Van Der Hoeven, J.G.; et al. Norepinephrine Dysregulates the Immune Response and Compromises Host Defense during Sepsis. Am. J. Respir. Crit. Care Med. 2020, 202, 830–842. [Google Scholar] [CrossRef]
- Dellinger, R.P.; Levy, M.M.; Carlet, J.M.; Bion, J.; Parker, M.M.; Jaeschke, R.; Reinhart, K.; Angus, D.C.; Brun-Buisson, C.; Beale, R.; et al. Surviving Sepsis Campaign: International guidelines for management of severe sepsis and septic shock: 2008. Crit. Care Med. 2008, 36, 296–327. [Google Scholar] [CrossRef]
- Magoon, R.; Kaushal, B.; Das, D.; Jangid, S.K. Norepinephrine in Sepsis: Looking beyond Vasoconstriction! Indian J. Crit. Care Med. 2019, 23, 544. [Google Scholar]
- Skytte Larsson, J.; Bragadottir, G.; Redfors, B.; Ricksten, S.E. Renal effects of norepinephrine-induced variations in mean arterial pressure after liver transplantation: A randomized cross-over trial. Acta Anaesthesiol. Scand. 2018, 62, 1229–1236. [Google Scholar] [CrossRef]
- Lankadeva, Y.R.; Kosaka, J.; Evans, R.G.; Bailey, S.R.; Bellomo, R.; May, C.N. Intrarenal and urinary oxygenation during norepi-nephrine resuscitation in ovine septic acute kidney injury. Kidney Int. 2016, 90, 100–108. [Google Scholar]
- Keir, I.; Kellum, J.A. Acute kidney injury in severe sepsis: Pathophysiology, diagnosis, and treatment recommendations. J. Veter Emerg. Crit. Care 2015, 25, 200–209. [Google Scholar] [CrossRef]
- Bellomo, R.; Kellum, J.A.; Ronco, C.; Wald, R.; Martensson, J.; Maiden, M.; Bagshaw, S.M.; Glassford, N.J.; Lankadeva, Y.; Vaara, S.T.; et al. Acute kidney injury in sepsis. Intensive Care Med. 2017, 43, 816–828. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Post, E.H.; Kellum, J.A.; Bellomo, R.; Vincent, J.-L. Renal perfusion in sepsis: From macro- to microcirculation. Kidney Int. 2017, 91, 45–60. [Google Scholar] [CrossRef]
- Ray, S.C.; Mason, J.; O’Connor, P.M. Ischemic Renal Injury: Can Renal Anatomy and Associated Vascular Congestion Explain Why the Medulla and Not the Cortex Is Where the Trouble Starts? Semin. Nephrol. 2019, 39, 520–529. [Google Scholar] [CrossRef]
- Wang, J.; Shi, M.; Huang, L.; Li, Q.; Meng, S.; Xu, J.; Xue, M.; Xie, J.; Liu, S.; Huang, Y. Addition of terlipressin to norepinephrine in septic shock and effect of renal perfusion: A pilot study. Ren. Fail. 2022, 44, 1207–1215. [Google Scholar] [CrossRef]
- Ince, C. Hemodynamic coherence and the rationale for monitoring the microcirculation. Crit. Care 2015, 19 (Suppl. S3), S8. [Google Scholar] [CrossRef]
- Demiselle, J.; Fage, N.; Radermacher, P.; Asfar, P. Vasopressin and its analogues in shock states: A review. Ann. Intensive Care 2020, 10, 9. [Google Scholar] [CrossRef]
- Wong, F.; Pappas, S.C.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N. Engl. J. Med. 2021, 384, 818–828. [Google Scholar] [CrossRef]
- Arora, V.; Maiwall, R.; Rajan, V.; Jindal, A.; Shasthry, S.M.; Kumar, G.; Jain, P.; Sarin, S.K. Terlipressin Is Superior to Noradrenaline in the Management of Acute Kidney Injury in Acute on Chronic Liver Failure. Hepatology 2020, 71, 600–610. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Jiang, Z.; Ying, J.; Han, Y.; Chen, Z. Optimal blood pressure decreases acute kidney injury after gastrointestinal surgery in elderly hypertensive patients: A randomized study: Optimal blood pressure reduces acute kidney injury. J. Clin. Anesth. 2017, 43, 77–83. [Google Scholar] [PubMed]
- Lamontagne, F.; Richards-Belle, A.; Thomas, K.; Harrison, D.A.; Sadique, M.Z.; Grieve, R.D.; Camsooksai, J.; Darnell, R.; Gordon, A.C.; Henry, D.; et al. Effect of Reduced Exposure to Vasopressors on 90-Day Mortality in Older Critically Ill Patients With Vasodilatory Hypotension: A Randomized Clinical Trial. JAMA 2020, 323, 938–949. [Google Scholar] [PubMed]
- Atan, R.; Peck, L.; Prowle, J.; Licari, E.; Eastwood, G.M.; Storr, M.; Goehl, H.; Bellomo, R. A Double-Blind Randomized Controlled Trial of High Cutoff Versus Standard Hemofiltra-tion in Critically Ill Patients with Acute Kidney Injury. Crit. Care Med. 2018, 46, e988–e994. [Google Scholar] [CrossRef] [PubMed]
- Azau, A.; Markowicz, P.; Corbeau, J.; Cottineau, C.; Moreau, X.; Baufreton, C.; Beydon, L. Increasing mean arterial pressure during cardiac surgery does not reduce the rate of postoperative acute kidney injury. Perfusion 2014, 29, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Russell, J.A.; Walley, K.R.; Singer, J.; Ayers, D.; Storms, M.M.; Holmes, C.L.; Hébert, P.C.; Cooper, D.J.; Mehta, S.; et al. The effects of vasopressin on acute kidney injury in septic shock. Intensive Care Med. 2010, 36, 83–91. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.A.; Walley, K.R.; Singer, J.; Gordon, A.C.; Hébert, P.C.; Cooper, D.J.; Holmes, C.L.; Mehta, S.; Granton, J.T.; Storms, M.M.; et al. Vasopressin versus Norepinephrine Infusion in Patients with Septic Shock. N. Engl. J. Med. 2008, 358, 877–887. [Google Scholar] [CrossRef]
- Zarjou, A.; Agarwal, A. Sepsis and Acute Kidney Injury. J. Am. Soc. Nephrol. 2011, 22, 999. [Google Scholar]
- Puntillo, F.; Giglio, M.; Pasqualucci, A.; Brienza, N.; Paladini, A.; Varrassi, G. Vasopressor-Sparing Action of Methylene Blue in Severe Sepsis and Shock: A Narrative Review. Adv. Ther. 2020, 37, 3692–3706. [Google Scholar] [CrossRef]
- Pasqualucci, A.; Puntillo, F.; Varrassi, G. Comments on: Methylene blue? Therapeutic alternative in the management of septic shock refractory to norepinephrine. Signa Vitae. 2021, 17, 219–220. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Studies and Patients | Agents | Findings | Safety | Comments |
|---|---|---|---|---|
| Huang 2021 [18] 5 studies 788 patients | Vasopressin infusion within 6 h of developing septic shock vs. standard care | Short-term mortality was similar between groups | Similar rates of new-onset arrhythmias | No difference between groups in ICU length of stay |
| Landoni 2013 [19] 18 interventions | Observational of 18 different interventions | Reduced mortality; vasopressin in septic shock, terlipressin for hepatorenal syndrome type 1 | 15/18 interventions reduced mortality | |
| Mouncey 2021 [20] 65 CCUs 2463 patients ≥ 65 years | Vasopressin vs. standard care | Vasopressin did not reduce 90-day mortality over standard care | Not blinded | |
| Nagendrahn 2019 [21] 4 studies 1453 patients | Vasopressin vs. standard care | No effect on 28-day mortality Reduced need for RRT | Appears safe |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Al-Husinat, L.; Alsabbah, A.; Hmaid, A.A.; Athamneh, R.; Adwan, M.; Hourani, M.N.; Almakhadmeh, S.; Modanat, Z.J.A.; Ismail, M.I.A.; Varrassi, G. Norepinephrine May Exacerbate Septic Acute Kidney Injury: A Narrative Review. J. Clin. Med. 2023, 12, 1373. https://doi.org/10.3390/jcm12041373
Al-Husinat L, Alsabbah A, Hmaid AA, Athamneh R, Adwan M, Hourani MN, Almakhadmeh S, Modanat ZJA, Ismail MIA, Varrassi G. Norepinephrine May Exacerbate Septic Acute Kidney Injury: A Narrative Review. Journal of Clinical Medicine. 2023; 12(4):1373. https://doi.org/10.3390/jcm12041373
Chicago/Turabian StyleAl-Husinat, Lou’i, Alameen Alsabbah, Amer Abu Hmaid, Razan Athamneh, Majd Adwan, Mohammad N. Hourani, Seif Almakhadmeh, Zaid Jehad Al Modanat, Mohammed I. A Ismail, and Giustino Varrassi. 2023. "Norepinephrine May Exacerbate Septic Acute Kidney Injury: A Narrative Review" Journal of Clinical Medicine 12, no. 4: 1373. https://doi.org/10.3390/jcm12041373