
The Combined Effect of Polygenic Risk Score and Prostate Health Index in Chinese Men Undergoing Prostate Biopsy
 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
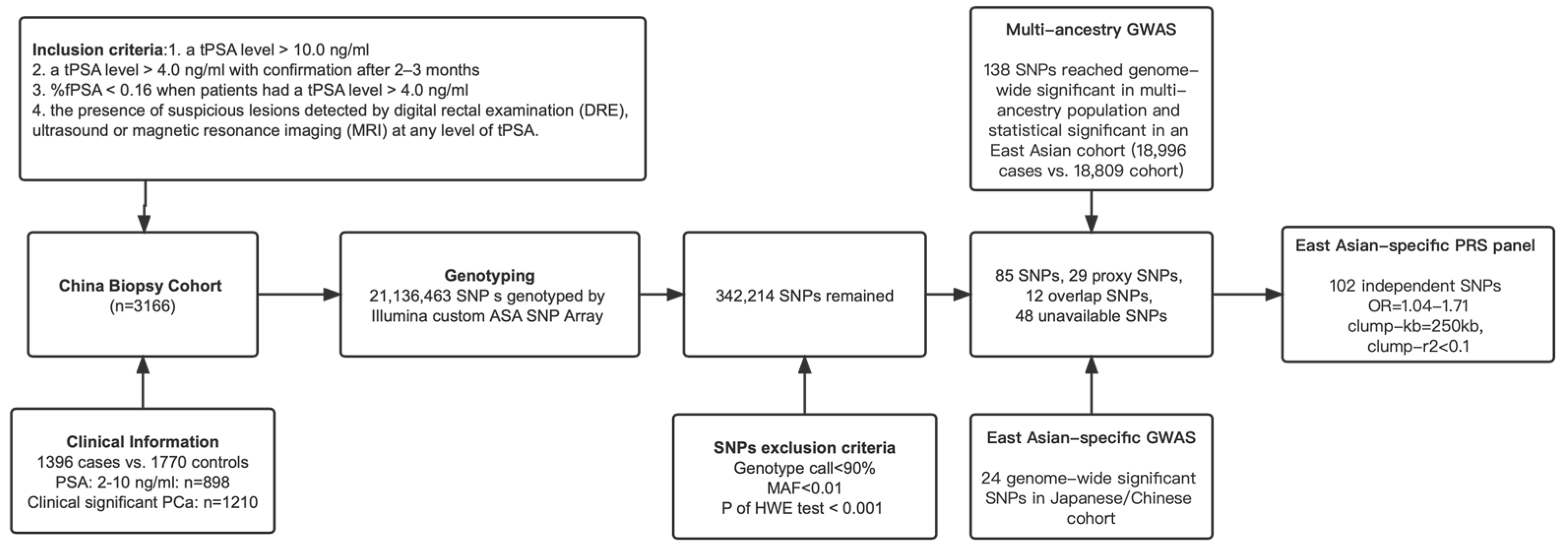
2.1. Study Population
2.2. Genotyping and PRS Calculation
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, Y.; Mo, M.; Wei, Y.; Wu, J.; Pan, J.; Freedland, S.J.; Zheng, Y.; Ye, D. Epidemiology and genomics of prostate cancer in Asian men. Nat. Rev. Urol. 2021, 18, 282–301. [Google Scholar] [CrossRef]
- Hugosson, J.; Carlsson, S.; Aus, G.; Bergdahl, S.; Khatami, A.; Lodding, P.; Pihl, C.-G.; Stranne, J.; Holmberg, E.; Lilja, H. Mortality results from the Göteborg randomised population-based prostate-cancer screening trial. Lancet Oncol. 2010, 11, 725–732. [Google Scholar] [CrossRef]
- Frånlund, M.; Månsson, M.; Godtman, R.A.; Aus, G.; Holmberg, E.; Kollberg, K.S.; Lodding, P.; Pihl, C.-G.; Stranne, J.; Lilja, H.; et al. Results from 22 years of Followup in the Göteborg Randomized Population-Based Prostate Cancer Screening Trial. J. Urol. 2022, 208, 292–300. [Google Scholar] [CrossRef]
- Song, S.H.; Byun, S.S. Polygenic risk score for genetic evaluation of prostate cancer risk in Asian populations: A narrative review. Investig. Clin. Urol. 2021, 62, 256–266. [Google Scholar] [CrossRef]
- NCCN. NCCN Guidelines Prostate Cancer, NCCN Clinical Practice Guidelines in Oncology. Prostate Cancer. Version 4.2022. Available online: http://www.nccn.org/professionals/physician_gls/f_guidelines (accessed on 1 September 2022).
- Byrne, L.; Toland, A.E. Polygenic Risk Scores in Prostate Cancer Risk Assessment and Screening. Urol. Clin. N. Am. 2021, 48, 387–399. [Google Scholar]
- Ruan, X.; Huang, D.; Huang, J.; Xu, D.; Na, R. Application of European-specific polygenic risk scores for predicting prostate cancer risk in different ancestry populations. Prostate 2022, 83, 30–38. [Google Scholar] [CrossRef]
- Akamatsu, S.; Terada, N.; Takata, R.; Kinoshita, H.; Shimatani, K.; Momozawa, Y.; Yamamoto, M.; Tada, H.; Kawamorita, N.; Narita, S.; et al. Clinical Utility of Germline Genetic Testing in Japanese Men Undergoing Prostate Biopsy. JNCI Cancer Spectr. 2022, 6, pkac001. [Google Scholar] [CrossRef]
- Jiang, H.; Liu, F.; Wang, Z.; Na, R.; Zhang, L.; Wu, Y.; Zheng, J.; Lin, X.; Jiang, D.; Sun, J.; et al. Prediction of prostate cancer from prostate biopsy in Chinese men using a genetic score derived from 24 prostate cancer risk-associated SNPs. Prostate 2013, 73, 1651–1659. [Google Scholar] [CrossRef]
- Na, R.; Ye, D.; Qi, J.; Liu, F.; Helfand, B.T.; Brendler, C.B.; Conran, C.A.; Packiam, V.; Gong, J.; Wu, Y.; et al. Prostate health index significantly reduced unnecessary prostate biopsies in patients with PSA 2–10 ng/mL and PSA > 10 ng/mL: Results from a Multicenter Study in China. Prostate 2017, 77, 1221–1229. [Google Scholar] [CrossRef]
- Hessels, D.; Schalken, J.A. The use of PCA3 in the diagnosis of prostate cancer. Nat. Rev. Urol. 2009, 6, 255–261. [Google Scholar] [CrossRef]
- Stabile, A.; Giganti, F.; Rosenkrantz, A.B.; Taneja, S.S.; Villeirs, G.; Gill, I.S.; Allen, C.; Emberton, M.; Moore, C.M.; Kasivisvanathan, V. Multiparametric MRI for prostate cancer diagnosis: Current status and future directions. Nat. Rev. Urol. 2020, 17, 41–61. [Google Scholar] [CrossRef] [PubMed]
- Seibert, T.M.; Fan, C.C.; Wang, Y.; Zuber, V.; Karunamuni, R.; Parsons, J.K.; Eeles, R.A.; Easton, D.F.; Kote-Jarai, Z.; Al Olama, A.A.; et al. Polygenic hazard score to guide screening for aggressive prostate cancer: Development and validation in large scale cohorts. BMJ 2018, 360, j5757. [Google Scholar] [CrossRef]
- Li-Sheng Chen, S.; Ching-Yuan Fann, J.; Sipeky, C.; Yang, T.-K.; Yueh-Hsia Chiu, S.; Ming-Fang Yen, A.; Laitinen, V.; Tammela, T.L.J.; Stenman, U.-H.; Auvinen, A.; et al. Risk Prediction of Prostate Cancer with Single Nucleotide Polymorphisms and Prostate Specific Antigen. J. Urol. 2019, 201, 486–495. [Google Scholar] [CrossRef] [PubMed]
- Sipeky, C.; Talala, K.M.; Tammela, T.L.J.; Taari, K.; Auvinen, A.; Schleutker, J. Prostate cancer risk prediction using a polygenic risk score. Sci. Rep. 2020, 10, 17075. [Google Scholar] [CrossRef] [PubMed]
- Pashayan, N.; Pharoah, P.D.; Schleutker, J.; Talala, K.; Tammela, T.L.; Määttänen, L.; Harrington, P.; Tyrer, J.; Eeles, R.; Duffy, S.W.; et al. Reducing overdiagnosis by polygenic risk-stratified screening: Findings from the Finnish section of the ERSPC. Br. J. Cancer 2015, 113, 1086–1093. [Google Scholar] [CrossRef]
- Ren, S.; Xu, J.; Zhou, T.; Jiang, H.; Chen, H.; Liu, F.; Na, R.; Zhang, L.; Wu, Y.; Sun, J.; et al. Plateau effect of prostate cancer risk-associated SNPs in discriminating prostate biopsy outcomes. Prostate 2013, 73, 1824–1835. [Google Scholar] [CrossRef] [PubMed]
- Huang, D.; Ruan, X.; Wu, Y.; Lin, X.; Huang, J.; Ye, D.; Gao, Y.; Ding, Q.; Xu, D.; Na, R. Genetic polymorphisms at 19q13.33 are associated with [−2]proPSA (p2PSA) levels and provide additional predictive value to prostate health index for prostate cancer. Prostate 2021, 81, 971–982. [Google Scholar] [CrossRef]
- Loeb, S.; Sanda, M.G.; Broyles, D.L.; Shin, S.S.; Bangma, C.H.; Wei, J.T.; Partin, A.W.; Klee, G.G.; Slawin, K.M.; Marks, L.S.; et al. The prostate health index selectively identifies clinically significant prostate cancer. J. Urol. 2015, 193, 1163–1169. [Google Scholar] [CrossRef]
- Beckman Coulter. Beckman Coulter Access Hybritech P2psa Instructions for Use. Beckman Coulter (The United States). 2017. Available online: https://www.beckmancoulter.com/products/immunoassay/phi (accessed on 1 September 2022).
- Das, S.; Forer, L.; Schönherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-Generation Genotype Imputation Service and Methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar]
- Galinsky, K.J.; Bhatia, G.; Loh, P.-R.; Georgiev, S.; Mukherjee, S.; Patterson, N.J.; Price, A.L. Fast Principal-Component Analysis Reveals Convergent Evolution of ADH1B in Europe and East Asia. Am. J. Hum. Genet. 2016, 98, 456–472. [Google Scholar] [CrossRef]
- Vickers, A.J.; Elkin, E.B. Decision curve analysis: A novel method for evaluating prediction models. Med. Decis. Mak. 2006, 26, 565–574. [Google Scholar] [CrossRef] [PubMed]
- Jewell, E.S.; Maile, M.D.; Engoren, M.; Elliott, M. Net Reclassification Improvement. Anesth. Analg. 2016, 122, 818–824. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Catalona, W.J.; Partin, A.W.; Sanda, M.G.; Wei, J.T.; Klee, G.G.; Bangma, C.H.; Slawin, K.M.; Marks, L.S.; Loeb, S.; Broyles, D.L.; et al. A multicenter study of [−2]pro-prostate specific antigen combined with prostate specific antigen and free prostate specific antigen for prostate cancer detection in the 2.0 to 10.0 ng/mL prostate specific antigen range. J. Urol. 2011, 185, 1650–1655. [Google Scholar] [CrossRef] [PubMed] [Green Version]



{kind=link}
{kind=link}
| Characteristics | All | Biopsy Positive | Biopsy Negative |
|---|---|---|---|
| Participants, no. (%) | 3166 | 1396 (44.1) | 1770 (55.9) |
| Age, years, median (IQR) | 68 (62–74) | 71 (65–77) | 66 (60–72) |
| Family history of PCa, no. (%) | 116 (3.7) | 62 (4.4) | 54 (3.1) |
| Prostate volume, mL, median (IQR) | 44.13 (32.47–61.44) | 38.00 (28.27–52.11) | 49.45 (37.05–67.00) |
| Hematological tumor markers: | |||
| Total PSA at biopsy, median (IQR) | 13.02 (7.76–26.07) | 22.58 (11.43–72.89) | 9.73 (6.47–15.49) |
| Free/total PSA at biopsy, median (IQR) | 0.14 (0.09–0.19) | 0.12 (0.08–0.15) | 0.16 (0.11–0.22) |
| [−2]proPSA at biopsy, median (IQR) | 22.14 (12.74–53.08) | 48.26 (21.33–223.52) | 15.91 (10.31–24.94) |
| phi at biopsy, median (IQR) | 47.39 (28.86–104.96) | 102.37 (55.09–244.50) | 33.08 (23.79–47.79) |
| Total PSA = 2–10 ng/mL, No. (%) | 898 (36.1) | 224 (20.3) | 671 (48.3) |
| Total PSA = 2–20 ng/mL, No. (%) | 1622 (51.2) | 505 (36.2) | 1117 (63.1) |
| Pathological results: | |||
| Gleason score 6, No. (%) | 276 (8.7) | 276 (19.8) | 0 |
| Gleason score ≥ 7, No. (%) | 1120 (35.4) | 1120 (80.2) | 0 |
| PRS Quintiles or Covariates 1 | PRS Threshold | PCa Proportion, % | Unadjusted | Adjusted for Age, Family History, 10 PCs | Adjusted for Age, Family History, PSA, %fPSA, 10 PCs | |||
|---|---|---|---|---|---|---|---|---|
| OR (95%CI) | p-Value | OR (95%CI) | p-Value | OR (95%CI) | p-Value | |||
| 0–20th | <5.10 | 25.3 | 1.00 | Ref. | 1.00 | Ref. | 1.00 | Ref. |
| 20–40th | 5.10–5.32 | 37.8 | 1.79 (1.41–2.28) | <0.001 | 1.86 (1.34–2.56) | <0.001 | 1.40 (1.04–1.90) | 0.027 |
| 40–60th | 5.32–5.50 | 42.0 | 2.14 (1.69–2.72) | <0.001 | 2.07 (1.50–2.84) | <0.001 | 1.82 (1.31–2.51) | <0.001 |
| 60–80th | 5.50–5.71 | 52.6 | 3.28 (2.59–4.16) | <0.001 | 3.26 (2.36–4.48) | <0.001 | 2.41 (1.75–3.32) | <0.001 |
| 80–100th | >5.71 | 62.8 | 4.99 (3.92–6.34) | <0.001 | 5.06 (3.68–6.97) | <0.001 | 3.63 (2.61–5.00) | <0.001 |
| Age | - | - | 1.07 (1.06–1.08) | <0.001 | 1.07 (1.06–1.08) | <0.001 | 1.07 (1.06–1.08) | <0.001 |
| FH 2 | - | - | 1.60 (1.00–2.55) | 0.048 | 1.84 (1.04–3.25) | 0.036 | 1.80 (0.97–3.25) | 0.259 |
| PV | - | - | 0.05 (0.03–0.09) | <0.001 | - | - | 0.01 (0.01–0.02) | <0.001 |
| tPSA | - | - | 8.45 (6.77–10.55) | <0.001 | - | - | 8.76 (6.55–11.82) | <0.001 |
| %fPSA | - | - | 0.12 (0.09–0.18) | <0.001 | - | - | 0.46 (0.30–0.72) | <0.001 |
| phi 3 | - | - | 51.66 (36.80–72.53) | <0.001 | - | - | 38.47 (27.11–54.05) | <0.001 |
| Clinical Risk Model * | AUC | 95% CI | P for AUC Comparison |
|---|---|---|---|
| FH-mediated model | 0.656 | 0.636–0.680 | Ref. |
| FH-mediated model + PRS | 0.718 | 0.696–0.741 | 3.62 × 10−10 |
| PSA-mediated model | 0.840 | 0.818–0.863 | Ref. |
| PSA-mediated model + PRS | 0.852 | 0.831–0.874 | 3.42 × 10−3 |
| phi-mediated model | 0.899 | 0.881–0.916 | Ref. |
| phi-mediated model + PRS | 0.904 | 0.887–0.921 | 0.02 |
| Clinical Risk Model | All Individuals | Early Onset (Age ≤ 55 Year) | Late Onset (Age > 55 Year) | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Individuals Reclassified (%) | NRI (%) | Individuals Reclassified (%) | NRI (%) | Individuals Reclassified (%) | NRI (%) | |||||||
| Up | Down | Value | 95%CI | Up | Down | Value | 95%CI | Up | Down | Value | 95%CI | |
| FH-mediated model | ||||||||||||
| Cases | 38.0 | 24.1 | 13.9 | 8.6–19.2 | 50.0 | 23.5 | 26.5 | −8.7~61.7 | 37.7 | 24.1 | 13.6 | 8.2–19.0 |
| Non-cases | 23.3 | 37.0 | 13.7 | 9.0–18.4 | 22.7 | 41.1 | 18.4 | 2.7–34.1 | 23.4 | 36.6 | 13.2 | 8.2–18.2 |
| All | - | - | 27.6 | 22.1–33.1 | - | - | 44.9 | 13.6–76.2 | - | - | 26.8 | 21.1–32.4 |
| PSA-mediated model | ||||||||||||
| Cases | 24.1 | 16.0 | 8.1 | 2.8–13.4 | 35.3 | 14.7 | 20.6 | −14.5~55.7 | 23.9 | 16.5 | 7.4 | 2.0–12.8 |
| Non-cases | 17.0 | 22.7 | 5.7 | 1.0–10.4 | 12.9 | 22.7 | 10.2 | −5.5~25.9 | 18.2 | 22.8 | 4.6 | −0.4~9.6 |
| All | - | - | 13.8 | 3.9–24.6 | - | - | 30.8 | 4.9–55.9 | - | - | 12.0 | 7.5–16.7 |
| phi-mediated model | ||||||||||||
| Cases | 22.6 | 17.4 | 5.2 | 0.1~10.5 | 35.3 | 14.7 | 20.6 | −14.5~55.7 | 22.4 | 17.9 | 4.5 | −0.9~9.9 |
| Non-cases | 18.1 | 21.5 | 3.4 | −1.3~8.1 | 13.5 | 22.1 | 8.6 | −7.1~24.3 | 19.0 | 21.8 | 2.8 | −2.2~7.8 |
| All | - | - | 8.6 | 4.2–13.0 | - | - | 29.2 | 3.7–54.7 | - | - | 7.3 | 2.7–11.9 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruan, X.; Huang, D.; Huang, J.; Huang, J.; Zhan, Y.; Wu, Y.; Ding, Q.; Xu, D.; Jiang, H.; Xue, W.; et al. The Combined Effect of Polygenic Risk Score and Prostate Health Index in Chinese Men Undergoing Prostate Biopsy. J. Clin. Med. 2023, 12, 1343. https://doi.org/10.3390/jcm12041343
Ruan X, Huang D, Huang J, Huang J, Zhan Y, Wu Y, Ding Q, Xu D, Jiang H, Xue W, et al. The Combined Effect of Polygenic Risk Score and Prostate Health Index in Chinese Men Undergoing Prostate Biopsy. Journal of Clinical Medicine. 2023; 12(4):1343. https://doi.org/10.3390/jcm12041343
Chicago/Turabian StyleRuan, Xiaohao, Da Huang, Jingyi Huang, Jinlun Huang, Yongle Zhan, Yishuo Wu, Qiang Ding, Danfeng Xu, Haowen Jiang, Wei Xue, and et al. 2023. "The Combined Effect of Polygenic Risk Score and Prostate Health Index in Chinese Men Undergoing Prostate Biopsy" Journal of Clinical Medicine 12, no. 4: 1343. https://doi.org/10.3390/jcm12041343