
Primary Stereotactic Radiosurgery Provides Favorable Tumor Control for Intraventricular Meningioma: A Retrospective Analysis


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Data Collection
2.2. SRS Procedure
2.3. Follow-Up and Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient and Tumor Characteristics
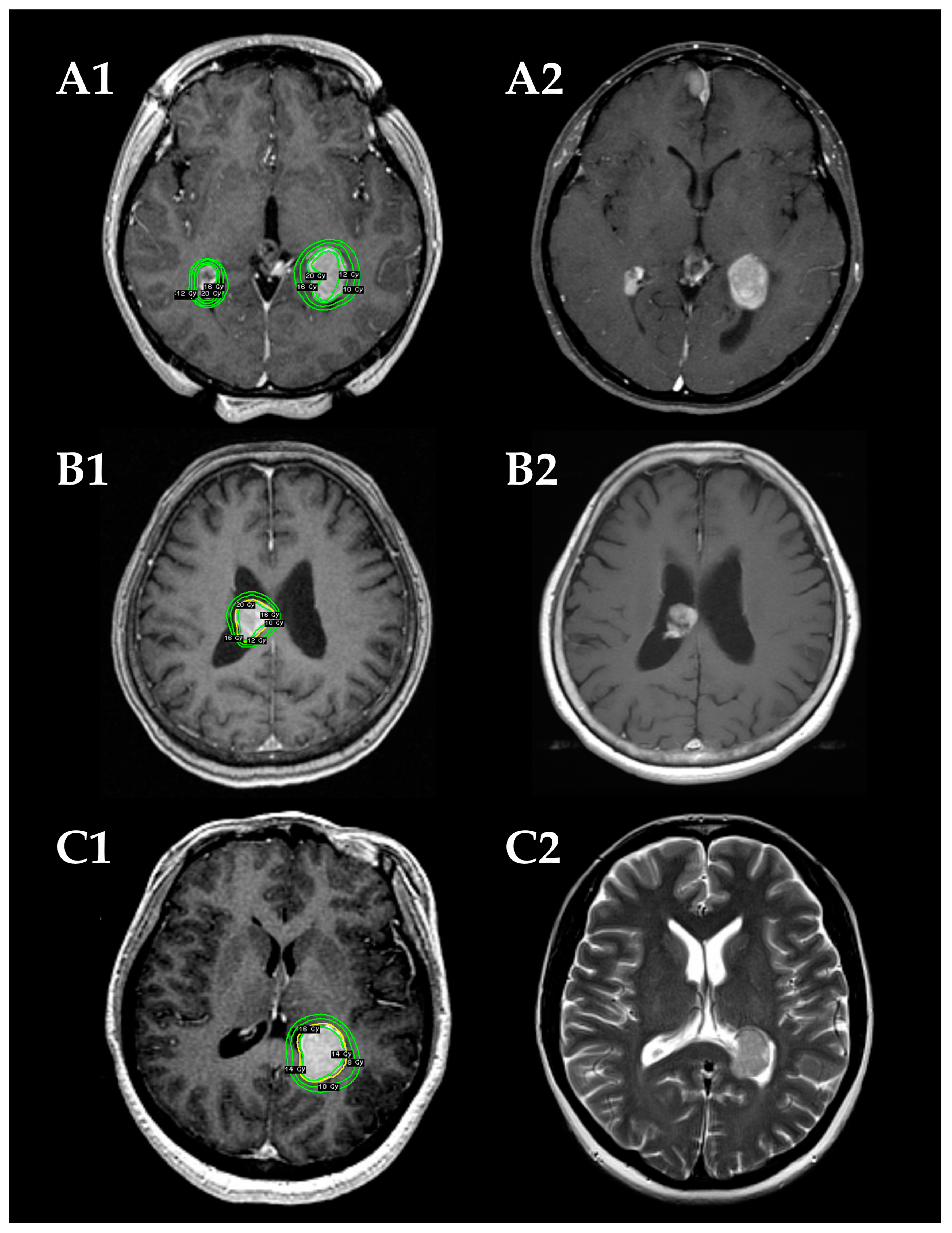
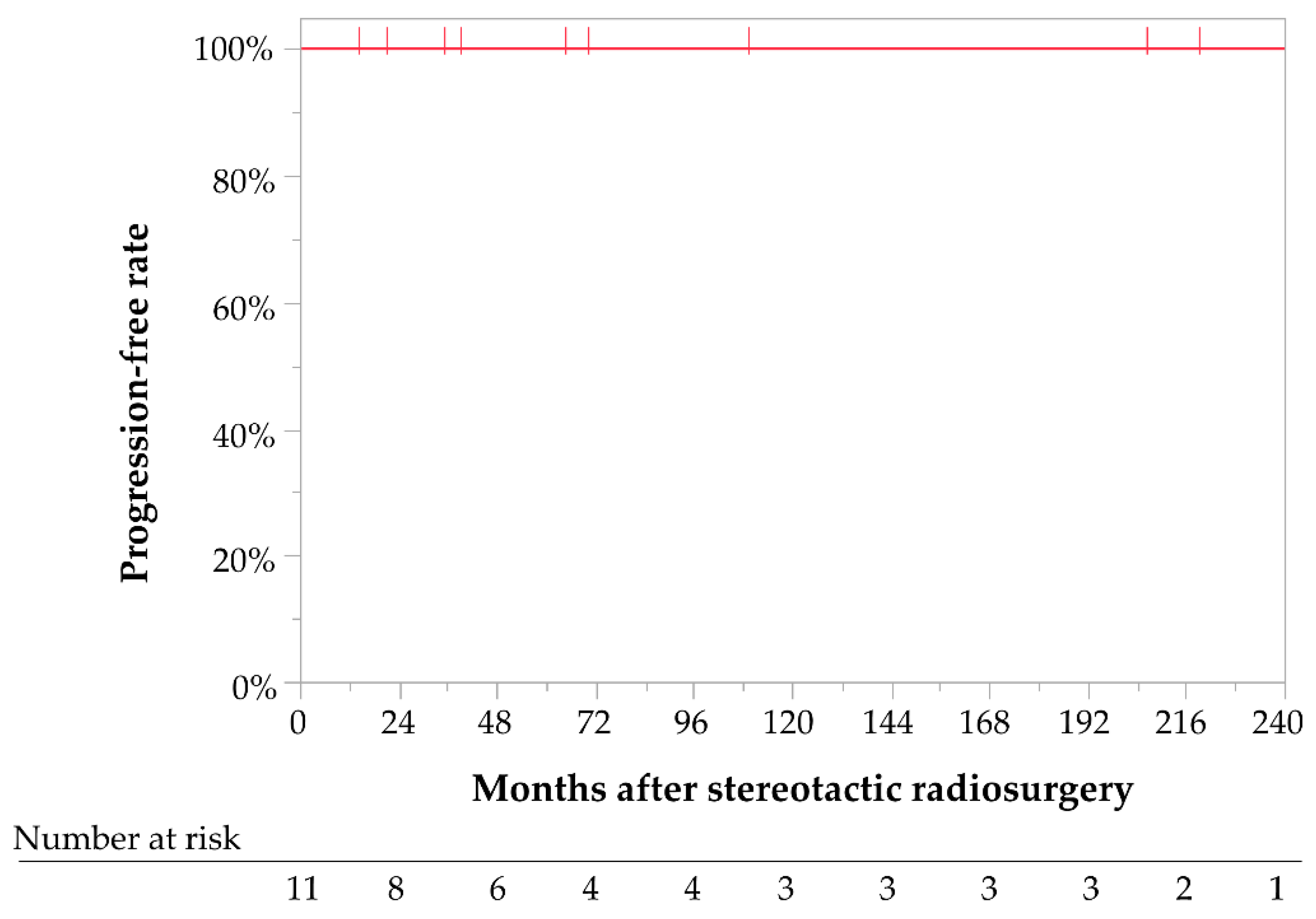
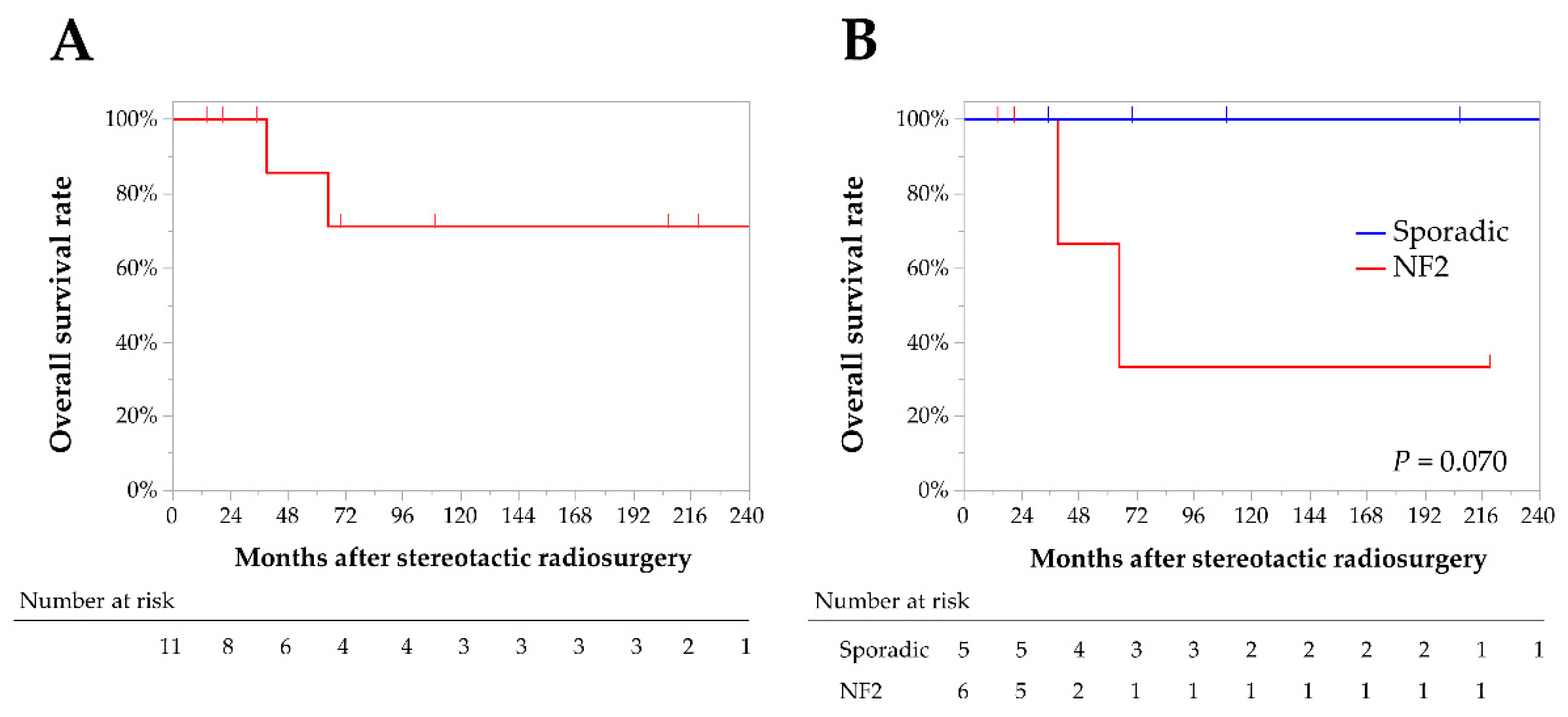
3.2. Tumor Control
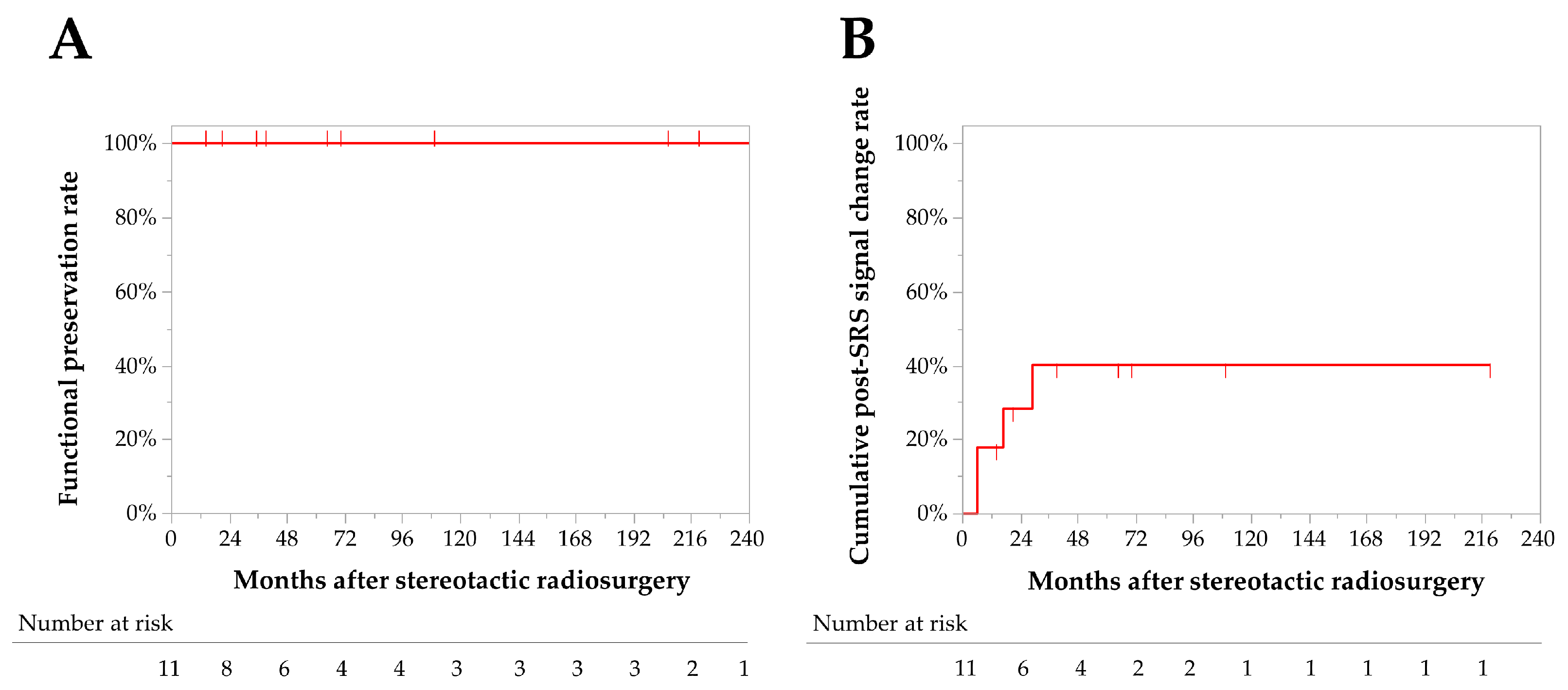
3.3. Adverse Radiation Events (AREs)
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ragel, B.T.; Jensen, R.L.; Couldwell, W.T. Inflammatory response and meningioma tumorigenesis and the effect of cyclooxygenase-2 inhibitors. Neurosurg. Focus 2007, 23, E7. [Google Scholar] [CrossRef]
- Riemenschneider, M.J.; Perry, A.; Reifenberger, G. Histological classification and molecular genetics of meningiomas. Lancet Neurol. 2006, 5, 1045–1054. [Google Scholar] [CrossRef]
- Nakamura, M.; Roser, F.; Bundschuh, O.; Vorkapic, P.; Samii, M. Intraventricular meningiomas: A review of 16 cases with reference to the literature. Surg. Neurol. 2003, 59, 490–503. [Google Scholar] [CrossRef]
- Pereira, B.J.A.; de Almeida, A.N.; Paiva, W.S.; de Aguiar, P.H.P.; Teixeira, M.J.; Marie, S.K.N. Natural history of intraventricular meningiomas: Systematic review. Neurosurg. Rev. 2020, 43, 513–523. [Google Scholar] [CrossRef]
- Bhatoe, H.S.; Singh, P.; Dutta, V. Intraventricular meningiomas: A clinicopathological study and review. Neurosurg. Focus 2006, 20, E9. [Google Scholar] [CrossRef]
- Liu, M.; Wei, Y.; Liu, Y.; Zhu, S.; Li, X. Intraventricular meninigiomas: A report of 25 cases. Neurosurg. Rev. 2006, 29, 36–40. [Google Scholar] [CrossRef]
- Odegaard, K.M.; Helseth, E.; Meling, T.R. Intraventricular meningiomas: A consecutive series of 22 patients and literature review. Neurosurg. Rev. 2013, 36, 57–64. [Google Scholar] [CrossRef]
- Li, P.; Diao, X.; Bi, Z.; Hao, S.; Ren, X.; Zhang, J.; Xing, J. Third ventricular meningiomas. J. Clin. Neurosci. 2015, 22, 1776–1784. [Google Scholar] [CrossRef]
- Li, Z.; Li, H.; Jiao, Y.; Ma, J.; Wang, S.; Cao, Y.; Zhao, J. Clinical features and long-term outcomes of pediatric intraventricular meningiomas: Data from a single neurosurgical center. Neurosurg. Rev. 2018, 41, 525–530. [Google Scholar] [CrossRef]
- Luo, W.; Xu, Y.; Yang, J.; Liu, Z.; Liu, H. Fourth Ventricular Meningiomas. World Neurosurg. 2019, 127, e1201–e1209. [Google Scholar] [CrossRef]
- Ma, J.; Cheng, L.; Wang, G.; Lin, S. Surgical management of meningioma of the trigone area of the lateral ventricle. World Neurosurg. 2014, 82, 757–769. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Lv, L.; Hu, Y.; Yin, S.; Zhou, P.; Jiang, S. Clinical features, surgical management, and long-term prognosis of intraventricular meningiomas: A large series of 89 patients at a single institution. Medicine 2019, 98, e15334. [Google Scholar] [CrossRef] [PubMed]
- Lin, M.; Bakhsheshian, J.; Strickland, B.; Rennert, R.C.; Chu, R.M.; Chaichana, K.L.; Zada, G. Exoscopic resection of atrial intraventricular meningiomas using a navigation-assisted channel-based trans-sulcal approach: Case series and literature review. J. Clin. Neurosci. 2020, 71, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Jamshidi, A.O.; Beer-Furlan, A.; Hardesty, D.A.; Ditzel Filho, L.F.S.; Prevedello, L.M.; Prevedello, D.M. Management of large intraventricular meningiomas with minimally invasive port technique: A three-case series. Neurosurg. Rev. 2021, 44, 2369–2377. [Google Scholar] [CrossRef]
- Shin, M.; Kurita, H.; Sasaki, T.; Kawamoto, S.; Tago, M.; Kawahara, N.; Morita, A.; Ueki, K.; Kirino, T. Analysis of treatment outcome after stereotactic radiosurgery for cavernous sinus meningiomas. J. Neurosurg. 2001, 95, 435–439. [Google Scholar] [CrossRef] [PubMed]
- Shinya, Y.; Hasegawa, H.; Shin, M.; Sugiyama, T.; Kawashima, M.; Takahashi, W.; Iwasaki, S.; Kashio, A.; Nakatomi, H.; Saito, N. Long-Term Outcomes of Stereotactic Radiosurgery for Vestibular Schwannoma Associated with Neurofibromatosis Type 2 in Comparison to Sporadic Schwannoma. Cancers 2019, 11, 1498. [Google Scholar] [CrossRef] [Green Version]
- Wen, P.Y.; Macdonald, D.R.; Reardon, D.A.; Cloughesy, T.F.; Sorensen, A.G.; Galanis, E.; Degroot, J.; Wick, W.; Gilbert, M.R.; Lassman, A.B.; et al. Updated response assessment criteria for high-grade gliomas: Response assessment in neuro-oncology working group. J. Clin. Oncol. 2010, 28, 1963–1972. [Google Scholar] [CrossRef]
- Huang, R.Y.; Bi, W.L.; Weller, M.; Kaley, T.; Blakeley, J.; Dunn, I.; Galanis, E.; Preusser, M.; McDermott, M.; Rogers, L.; et al. Proposed response assessment and endpoints for meningioma clinical trials: Report from the Response Assessment in Neuro-Oncology Working Group. Neuro-Oncology 2019, 21, 26–36. [Google Scholar] [CrossRef] [Green Version]
- Bertalanffy, A.; Roessler, K.; Koperek, O.; Gelpi, E.; Prayer, D.; Neuner, M.; Knosp, E. Intraventricular meningiomas: A report of 16 cases. Neurosurg. Rev. 2006, 29, 30–35. [Google Scholar] [CrossRef]
- Menon, G.; Nair, S.; Sudhir, J.; Rao, R.; Easwer, H.V.; Krishnakumar, K. Meningiomas of the lateral ventricle—A report of 15 cases. Br. J. Neurosurg. 2009, 23, 297–303. [Google Scholar] [CrossRef]
- Cabezudo, J.M.; Vaquero, J.; Garcia-de-Sola, R.; Areitio, E.; Bravo, G. Meningioma of the anterior part of the third ventricle. Acta Neurochir. 1981, 56, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Karki, P.; Yonezawa, H.; Bohara, M.; Oyoshi, T.; Hirano, H.; Moinuddin, F.M.; Hiraki, T.; Yoshioka, T.; Arita, K. Third ventricular atypical meningioma which recurred with further malignant progression. Brain Tumor Pathol. 2015, 32, 56–60. [Google Scholar] [CrossRef]
- Lozier, A.P.; Bruce, J.N. Meningiomas of the velum interpositum: Surgical considerations. Neurosurg. Focus 2003, 15, E11. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wajima, D.; Iida, J.; Nishi, N. Third ventricular meningioma--case report. Neurol. Med. Chir. 2011, 51, 75–78. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, B.Y.; Yin, B.; Li, Y.X.; Wu, J.S.; Chen, H.; Wang, X.Q.; Geng, D.Y. Neuroradiological findings and clinical features of fourth-ventricular meningioma: A study of 10 cases. Clin. Radiol. 2012, 67, 455–460. [Google Scholar] [CrossRef] [PubMed]
- Daza-Ovalle, A.; Bin-Alamer, O.; Flickinger, J.; Niranjan, A.; Lunsford, L.D. Outcomes after gamma knife radiosurgery for intraventricular meningiomas. J. Neurooncol. 2022, 160, 23–31. [Google Scholar] [CrossRef]
- Kim, I.Y.; Kondziolka, D.; Niranjan, A.; Flickinger, J.C.; Lunsford, L.D. Gamma knife radiosurgery for intraventricular meningiomas. Acta Neurochir. 2009, 151, 447. [Google Scholar] [CrossRef]
- Mindermann, T.; Heckl, S.; Mack, A. High incidence of transient perifocal edema following upfront radiosurgery for intraventricular meningiomas. Acta Neurochir. 2020, 162, 2177–2182. [Google Scholar] [CrossRef]
- Nundkumar, N.; Guthikonda, M.; Mittal, S. Peritumoral edema following Gamma Knife radiosurgery as the primary treatment for intraventricular meningiomas. J. Clin. Neurosci. 2013, 20, 616–618. [Google Scholar] [CrossRef]
- Samanci, Y.; Oktug, D.; Yilmaz, M.; Sengoz, M.; Peker, S. Efficacy of gamma knife radiosurgery in the treatment of intraventricular meningiomas. J. Clin. Neurosci. 2020, 80, 38–42. [Google Scholar] [CrossRef]
- Sheehan, J.; Pikis, S.; Islim, A.I.; Chen, C.J.; Bunevicius, A.; Peker, S.; Samanci, Y.; Nabeel, A.M.; Reda, W.A.; Tawadros, S.R.; et al. An international multicenter matched cohort analysis of incidental meningioma progression during active surveillance or after stereotactic radiosurgery: The IMPASSE study. Neuro-Oncology 2022, 24, 116–124. [Google Scholar] [CrossRef] [PubMed]
- Forde, C.; King, A.T.; Rutherford, S.A.; Hammerbeck-Ward, C.; Lloyd, S.K.; Freeman, S.R.; Pathmanaban, O.N.; Stapleton, E.; Thomas, O.M.; Laitt, R.D.; et al. Disease course of neurofibromatosis type 2: A 30-year follow-up study of 353 patients seen at a single institution. Neuro-Oncology 2021, 23, 1113–1124. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, T.; Chung, L.K.; Sheppard, J.P.; Bhatt, N.S.; Chen, C.H.J.; Lagman, C.; Kaprealian, T.; Lee, P.; Nghiemphu, P.L.; Yang, I. Surgery versus stereotactic radiosurgery for the treatment of multiple meningiomas in neurofibromatosis type 2: Illustrative case and systematic review. Neurosurg. Rev. 2019, 42, 85–96. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Fresnedo, A.; Domingo, R.A.; Sanchez-Garavito, J.E.; Perez-Vega, C.; Akinduro, O.O.; Jentoft, M.E.; Vora, S.A.; Brown, P.D.; Porter, A.B.; Bendok, B.R.; et al. The impact of multiple lesions on progression-free survival of meningiomas: A 10-year multicenter experience. J. Neurosurg. 2021, 137, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Milano, M.T.; Sharma, M.; Soltys, S.G.; Sahgal, A.; Usuki, K.Y.; Saenz, J.M.; Grimm, J.; El Naqa, I. Radiation-Induced Edema After Single-Fraction or Multifraction Stereotactic Radiosurgery for Meningioma: A Critical Review. Int. J. Radiat. Oncol. Biol. Phys. 2018, 101, 344–357. [Google Scholar] [CrossRef] [Green Version]
- Novotny, J., Jr.; Kollova, A.; Liscak, R. Prediction of intracranial edema after radiosurgery of meningiomas. J. Neurosurg. 2006, 105, 120–126. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | |
|---|---|
| Median (Range) | Tumors (n = 12) |
| Follow-up period, months | 52 (3–353) |
| Age at SRS, years | 45 (13–80) |
| Maximum diameter, mm | 24 (17–33) |
| Target volume, mL | 4.9 (1.2–9.8) |
| Marginal dose, Gy | 16 (9–18) |
| Central dose, Gy | 34 (24–45) |
| Number of isocenters | 10 (3–37) |
| Volume of normal brain tissue exposed to ≥12 Gy (V12), mL | 1.7 (1.2–2.5) |
| n (%) | Patients (n = 11) |
| Male sex | 5 (45) |
| Prior surgery for IVMs | 0 (0) |
| Multiple meningiomas | 6 (55) |
| NF2 | 5 (45) |
| n (%) | Tumors (n = 12) |
| Brain edema before SRS | 3 (25) |
| Tumor location | |
| 9 (75) |
| 2 (17) |
| 1 (8) |
| No. | Age/Sex | Location | Tumor Features | Prior Surgery | Tumor Volume | Marginal Dose | Central Dose | Follow-Up | Tumor Size at the Last F/U | ARE | Patients’ Status at the Last F/U |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | 22/F | Trigone | Sporadic | None | 7.4 mL | 9 Gy | 45 Gy | 353 months | Shrinkage | Signal change (asymptomatic) | Alive |
| 2 | 52/F | Trigone | Sporadic | None | 1.8 mL | 18 Gy | 45 Gy | 206 months | Shrinkage | Signal change (asymptomatic) | Alive |
| 3 | 13/M | Body of the LV | NF2 | None | 2.9 mL | 16 Gy | 40 Gy | 14 months | Shrinkage | None | Alive |
| 4 | 46/F | Trigone | Sporadic | None | 7.5 mL | 18 Gy | 36 Gy | 70 months | Shrinkage | None | Alive |
| 5 | 44/M | Third ventricle | NF2 | None | 2.5 mL | 15.5 Gy | 24 Gy | 219 months | Shrinkage | None | Alive |
| 6 | 33/M | Trigone | NF2 | None | 9.8 mL | 14 Gy | 28 Gy | 65 months | Unchanged | None | Died of progression of an unrelated tumor |
| 7 | 31/F | Trigone | NF2 | None | 5.5 mL | 16 Gy | 32 Gy | 21 months | Unchanged | Signal change (headache) | Alive |
| 8 | 31/F | Trigone | NF2 | None | 1.2 mL | 16 Gy | 32 Gy | 21 months | Unchanged | None | Alive |
| 9 | 80/F | Body of the LV | Sporadic | None | 4.3 mL | 16 Gy | 40 Gy | 109 months | Shrinkage | None | Alive |
| 10 | 67/M | Trigone | NF2 | None | 9.0 mL | 14 Gy | 35 Gy | 39 months | Unchanged | None | Died of progression of an unrelated tumor |
| 11 | 50/F | Trigone | Sporadic | None | 8.3 mL | 14 Gy | 28 Gy | 35 months | Shrinkage | Signal change (asymptomatic) | Alive |
| 12 | 63/M | Trigone | Sporadic | None | 4.0 mL | 14 Gy | 28 Gy | 3 months | Unchanged | None | Alive |
| Variables | HR (95% CI) | p-Value |
|---|---|---|
| Patient age (continuous) | 0.98 (0.92–1.03) | 0.478 |
| Patient age ≥ 45 (vs. <45) | 1.10 (0.15–7.79) | 0.927 |
| Maximum diameter, mm (continuous) | 0.99 (0.79–1.22) | 0.961 |
| Maximum diameter ≥ 25 mm (vs. <25) | 2.34 (0.24–22.80) | 0.464 |
| Tumor volume, mL (continuous) | 1.09 (0.79–1.64) | 0.600 |
| Tumor volume ≥ 8 mL (vs. <8) | 1.48 (0.21–10.63) | 0.697 |
| Marginal dose, Gy (continuous) | 0.91 (0.66–1.36) | 0.605 |
| Marginal dose ≥ 16 Gy (vs. <16 Gy) | 1.08 (0.15–7.92) | 0.939 |
| Central dose, Gy (continuous) | 0.05 (0.91–1.25) | 0.470 |
| Central dose ≥ 33 Gy (vs. <33 Gy) | 0.68 (0.09–4.85) | 0.697 |
| Number of isocenters (continuous) | 1.01 (0.76–1.33) | 0.962 |
| Number of isocenters ≥ 7 (vs. <7) | 0.77 (0.11–5.55) | 0.794 |
| V12, mL (continuous) | 1.44 (0.02–71.90) | 0.847 |
| V12 ≥ 2.0 mL (vs. <2.0 mL) | 1.67 (0.10–26.65) | 0.718 |
| Brain edema before SRS (vs. without edema) | 2.56 (0.36–18.25) | 0.349 |
| NF2-related (vs. sporadic) | 0.30 (0.03–2.92) | 0.302 |
| Authors | Number of Tumors | Median Age, Years (Range) | Male (%) | NF2 (%) | Location (%) | Prior Resection (%) | Median Tumor Volume, mL (Range) | Median Margin Dose, Gy (Range) | Median Follow-Up Months (Range) | Tumor Control Rate (%) | Post-SRS Signal Change (Symptomatic) (%) | Post-SRS Hydrocephalus (%) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Kim et al., 2009 [27] | 9 | 51 (14–81) | 67 | 0 | Trigone 89 Third ventricle 11 | 44 | 3.9 (0.8–11.8) | 16 (14–25) | 64 (7–161) | 67 | 0 | 0 |
| Nundkumar et al., 2013 [29] | 2 | 50 (49–50) | 0 | NA | Trigone 100 | 0 | 3.3 (2.2–4.4) | 18 (18–18) | 12 (8–17) | 100 | 100 (100) | 0 |
| Mindermann et al., 2020 [28] | 5 | 63 (50–81) | 0 | NA | Trigone 100 | 0 | 4.7 (2.5–14.1) | 13.5 (12–15) | 81 (19–240) | 100 | 80 (40) | 0 |
| Samanci et al., 2020 [30] | 6 | 41 (30–71) | 50 | 17 | Trigone 100 | 17 | 5.5 (1.2–9.2) | 12 (11–13) | 74 (24–139) | 100 | 17 (17) | 0 |
| Daza-Ovalle et al., 2022 [26] | 20 | 53 (14–84) | 63 | 0 | Trigone 90 Third ventricle 5 Fourth ventricle 5 | 30 | 4.8 (0.8–17) | 14 (12–25) | 63 (6–322) | 85 | 35 (15) | 0 |
| Present study 2022 | 12 | 45 (13–80) | 45 | 50 | Trigone 75 Body of lateral ventricle 17 Third ventricle 8 | 0 | 4.9 (1.2–9.8) | 16 (9–18) | 52 (3–353) | 100 | 33 (8) | 0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Umekawa, M.; Shinya, Y.; Hasegawa, H.; Katano, A.; Saito, N. Primary Stereotactic Radiosurgery Provides Favorable Tumor Control for Intraventricular Meningioma: A Retrospective Analysis. J. Clin. Med. 2023, 12, 1068. https://doi.org/10.3390/jcm12031068
Umekawa M, Shinya Y, Hasegawa H, Katano A, Saito N. Primary Stereotactic Radiosurgery Provides Favorable Tumor Control for Intraventricular Meningioma: A Retrospective Analysis. Journal of Clinical Medicine. 2023; 12(3):1068. https://doi.org/10.3390/jcm12031068
Chicago/Turabian StyleUmekawa, Motoyuki, Yuki Shinya, Hirotaka Hasegawa, Atsuto Katano, and Nobuhito Saito. 2023. "Primary Stereotactic Radiosurgery Provides Favorable Tumor Control for Intraventricular Meningioma: A Retrospective Analysis" Journal of Clinical Medicine 12, no. 3: 1068. https://doi.org/10.3390/jcm12031068