
Plasma Level of Pyrophosphate Is Low in Pseudoxanthoma Elasticum Owing to Mutations in the ABCC6 Gene, but It Does Not Correlate with ABCC6 Genotype

Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Genotyping
2.3. Blood Collection and PPi Analysis
2.4. Arterial Phenotypes
2.4.1. Arterial Calcification
2.4.2. Ankle-Brachial Index
2.5. Ophthalmological Phenotypes
2.5.1. Length of Angioid Streaks
2.5.2. Macular Phenotype
2.6. In Vivo Expression of ABCC6 Protein in Mouse Hepatocytes
2.7. Statistical Analysis
3. Results
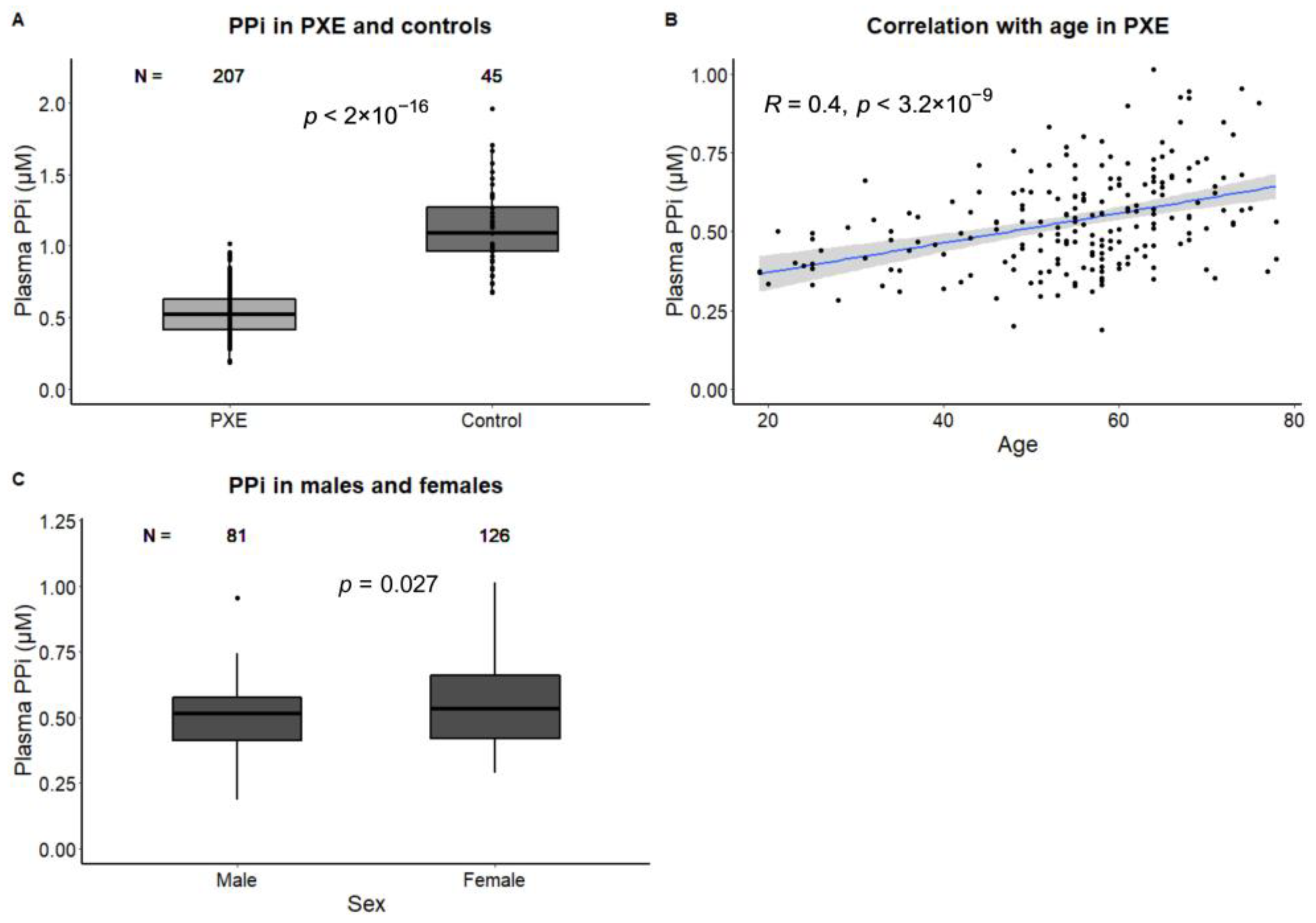
3.1. Determinants of PPi in PXE
3.2. Association of PPi and Arterial Calcification and Function
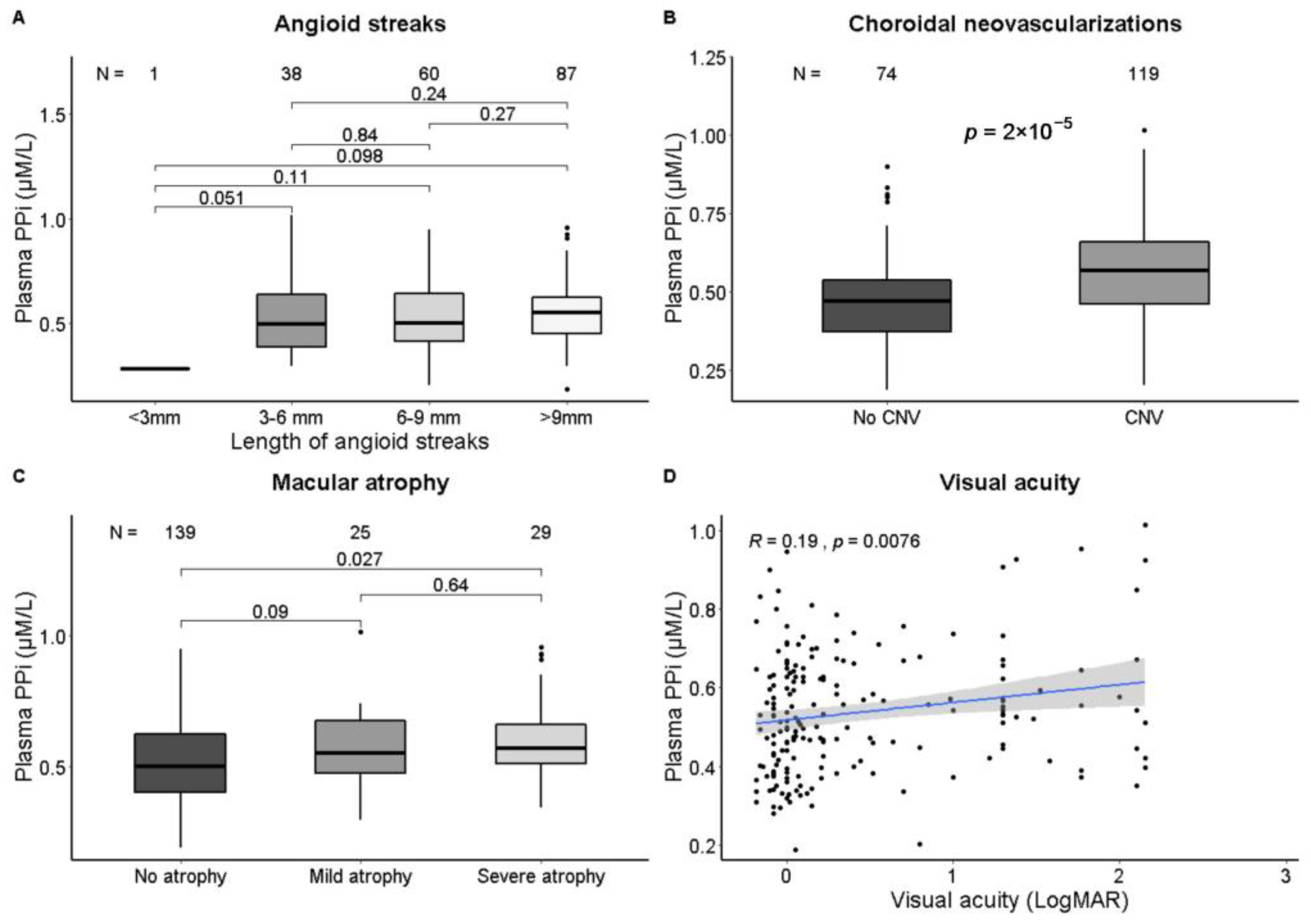
3.3. Association of PPi and Ophthalmological Phenotypes
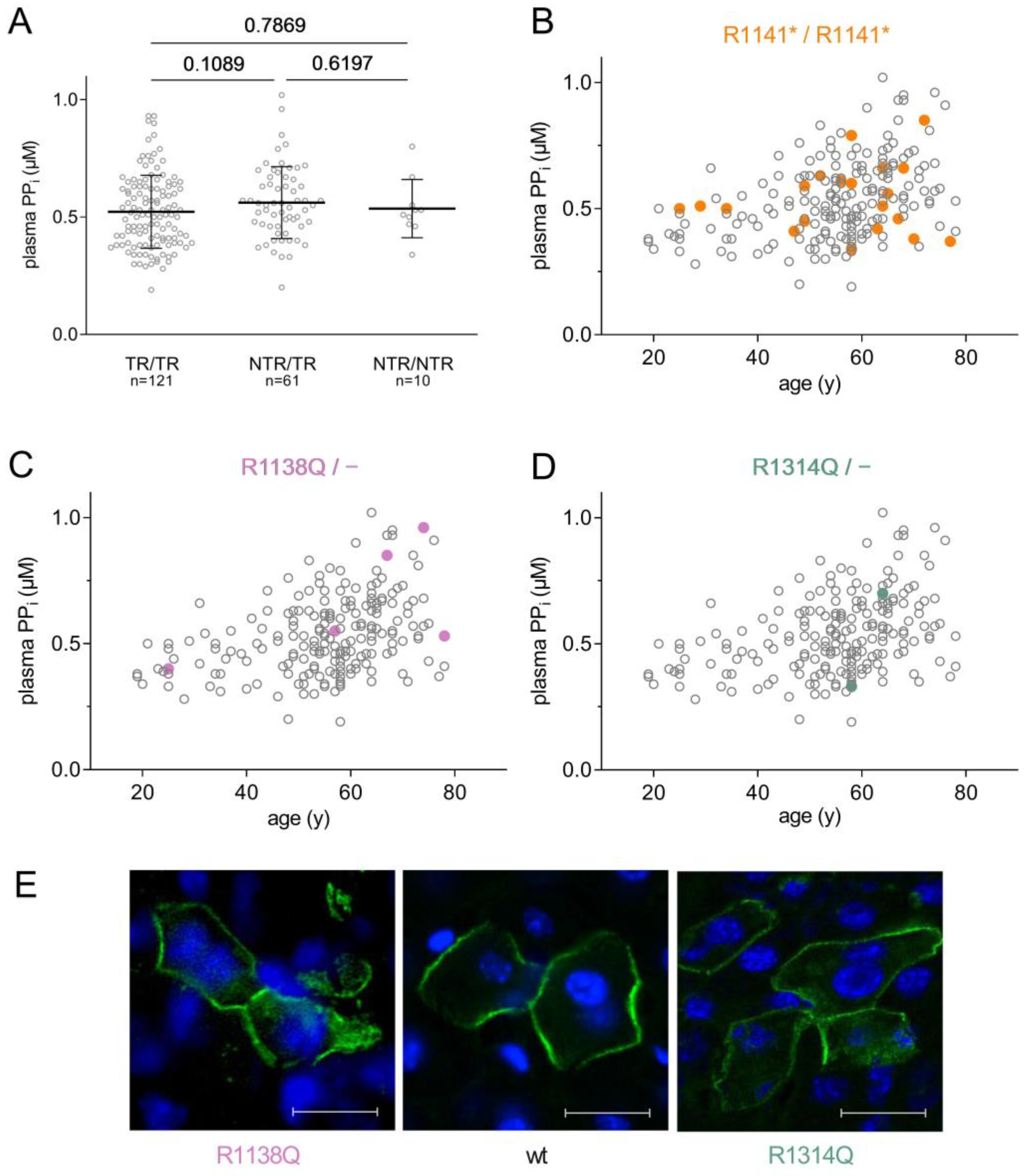
3.4. Association of PPi and ABCC6 Genotype
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Evrard, S.; Delanaye, P.; Kamel, S.; Cristol, J.-P.; Cavalier, E.; SFBC/SN Joined Working Group on Vascular Calcifications. Vascular Calcification: From Pathophysiology to Biomarkers. Clin. Chim. Acta 2015, 438, 401–414. [Google Scholar] [CrossRef] [PubMed]
- Jansen, R.S.; Duijst, S.; Mahakena, S.; Sommer, D.; Szeri, F.; Váradi, A.; Plomp, A.; Bergen, A.A.; Oude Elferink, R.P.J.; Borst, P.; et al. ABCC6-Mediated ATP Secretion by the Liver Is the Main Source of the Mineralization Inhibitor Inorganic Pyrophosphate in the Systemic Circulation-Brief Report. Arterioscler. Thromb. Vasc. Biol. 2014, 34, 1985–1989. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borst, P.; Váradi, A.; van de Wetering, K. PXE, a Mysterious Inborn Error Clarified. Trends Biochem. Sci. 2019, 44, 125–140. [Google Scholar] [CrossRef] [PubMed]
- Plomp, A.S.; Toonstra, J.; Bergen, A.A.B.; van Dijk, M.R.; de Jong, P.T.V.M. Proposal for Updating the Pseudoxanthoma Elasticum Classification System and a Review of the Clinical Findings. Am. J. Med. Genet. A 2010, 152A, 1049–1058. [Google Scholar] [CrossRef]
- Risseeuw, S.; Ossewaarde-van Norel, J.; van Buchem, C.; Spiering, W.; Imhof, S.M.; van Leeuwen, R. The Extent of Angioid Streaks Correlates With Macular Degeneration in Pseudoxanthoma Elasticum. Am. J. Ophthalmol. 2020, 220, 82–90. [Google Scholar] [CrossRef]
- Kranenburg, G.; de Jong, P.A.; Mali, W.P.; Attrach, M.; Visseren, F.L.J.; Spiering, W. Prevalence and Severity of Arterial Calcifications in Pseudoxanthoma Elasticum (PXE) Compared to Hospital Controls. Novel Insights into the Vascular Phenotype of PXE. Atherosclerosis 2017, 256, 7–14. [Google Scholar] [CrossRef]
- Leftheriotis, G.; Kauffenstein, G.; Hamel, J.F.; Abraham, P.; Le Saux, O.; Willoteaux, S.; Henrion, D.; Martin, L. The Contribution of Arterial Calcification to Peripheral Arterial Disease in Pseudoxanthoma Elasticum. PLoS ONE 2014, 9, e96003. [Google Scholar] [CrossRef] [Green Version]
- Orriss, I.R.; Arnett, T.R.; Russell, R.G.G. Pyrophosphate: A Key Inhibitor of Mineralisation. Curr. Opin. Pharmacol. 2016, 28, 57–68. [Google Scholar] [CrossRef] [Green Version]
- Pomozi, V.; Brampton, C.; Fülöp, K.; Chen, L.-H.; Apana, A.; Li, Q.; Uitto, J.; Le Saux, O.; Váradi, A. Analysis of Pseudoxanthoma Elasticum-Causing Missense Mutants of ABCC6 in Vivo; Pharmacological Correction of the Mislocalized Proteins. J. Investig. Dermatol. 2014, 134, 946–953. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Plomp, A.; Gorgels, T.; Brink, J.T.; Loves, W.; Mannens, M.; de Jong, P.T.V.M.; Bergen, A.A.B. Efficient Molecular Diagnostic Strategy for ABCC6 in Pseudoxanthoma Elasticum. Genet. Test. 2004, 8, 292–300. [Google Scholar] [CrossRef]
- Nykamp, K.; Anderson, M.; Powers, M.; Garcia, J.; Herrera, B.; Ho, Y.-Y.; Kobayashi, Y.; Patil, N.; Thusberg, J.; Westbrook, M.; et al. Sherloc: A Comprehensive Refinement of the ACMG-AMP Variant Classification Criteria. Genet. Med. 2017, 19, 1105–1117. [Google Scholar] [CrossRef] [Green Version]
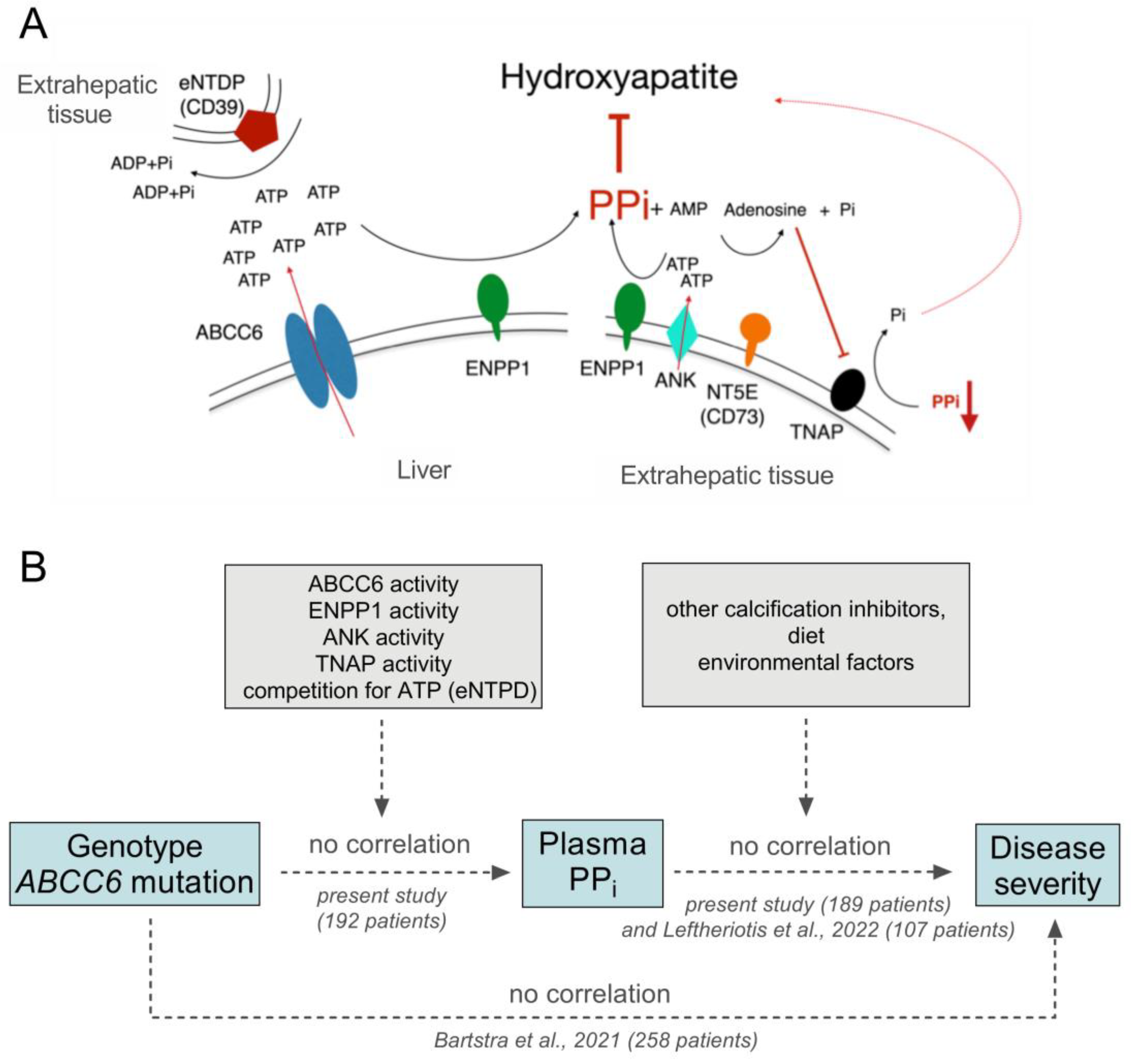
- Bartstra, J.W.; Risseeuw, S.; de Jong, P.A.; van Os, B.; Kalsbeek, L.; Mol, C.; Baas, A.F.; Verschuere, S.; Vanakker, O.; Florijn, R.J.; et al. Genotype-Phenotype Correlation in Pseudoxanthoma Elasticum. Atherosclerosis 2021, 324, 18–26. [Google Scholar] [CrossRef]
- Gräni, C.; Vontobel, J.; Benz, D.C.; Bacanovic, S.; Giannopoulos, A.A.; Messerli, M.; Grossmann, M.; Gebhard, C.; Pazhenkottil, A.P.; Gaemperli, O.; et al. Ultra-Low-Dose Coronary Artery Calcium Scoring Using Novel Scoring Thresholds for Low Tube Voltage Protocols-a Pilot Study. Eur. Heart J. Cardiovasc. Imaging 2018, 19, 1362–1371. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Willemink, M.J.; Vliegenthart, R.; Takx, R.A.P.; Leiner, T.; Budde, R.P.J.; Bleys, R.L.A.W.; Das, M.; Wildberger, J.E.; Prokop, M.; Buls, N.; et al. Coronary Artery Calcification Scoring with State-of-the-Art CT Scanners from Different Vendors Has Substantial Effect on Risk Classification. Radiology 2014, 273, 695–702. [Google Scholar] [CrossRef] [PubMed]
- Chassaing, N.; Martin, L.; Mazereeuw, J.; Barrié, L.; Nizard, S.; Bonafé, J.-L.; Calvas, P.; Hovnanian, A. Novel ABCC6 Mutations in Pseudoxanthoma Elasticum. J. Investig. Dermatol. 2004, 122, 608–613. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shi, Y.; Terry, S.F.; Terry, P.F.; Bercovitch, L.G.; Gerard, G.F. Development of a Rapid, Reliable Genetic Test for Pseudoxanthoma Elasticum. J. Mol. Diagn. 2007, 9, 105–112. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pfendner, E.G.; Vanakker, O.M.; Terry, S.F.; Vourthis, S.; McAndrew, P.E.; McClain, M.R.; Fratta, S.; Marais, A.; Hariri, S.; Coucke, P.J.; et al. Mutation Detection in the ABCC6 Gene and Genotype–Phenotype Analysis in a Large International Case Series Affected by Pseudoxanthoma Elasticum. J. Med. Genet. 2007, 44, 621–628. [Google Scholar] [CrossRef] [Green Version]
- Hu, X.; Peek, R.; Plomp, A.; Brink, J.T.; Scheffer, G.; van Soest, S.; Leys, A.; de Jong, P.T.V.M.; Bergen, A.A.B. Analysis of the Frequent R1141X Mutation in the ABCC6 Gene in Pseudoxanthoma Elasticum. Investig. Ophthalmol. Vis. Sci. 2003, 44, 1824–1829. [Google Scholar] [CrossRef] [Green Version]
- Pomozi, V.; Le Saux, O.; Brampton, C.; Apana, A.; Iliás, A.; Szeri, F.; Martin, L.; Monostory, K.; Paku, S.; Sarkadi, B.; et al. ABCC6 Is a Basolateral Plasma Membrane Protein. Circ. Res. 2013, 112, e148–e151. [Google Scholar] [CrossRef] [Green Version]
- Leftheriotis, G.; Navasiolava, N.; Clotaire, L.; Duranton, C.; Le Saux, O.; Bendahhou, S.; Laurain, A.; Rubera, I.; Martin, L. Relationships between Plasma Pyrophosphate, Vascular Calcification and Clinical Severity in Patients Affected by Pseudoxanthoma Elasticum. J. Clin. Med. 2022, 11, 2588. [Google Scholar] [CrossRef]
- Kozák, E.; Fülöp, K.; Tőkési, N.; Rao, N.; Li, Q.; Terry, S.F.; Uitto, J.; Zhang, X.; Becker, C.; Váradi, A.; et al. Oral Supplementation of Inorganic Pyrophosphate in Pseudoxanthoma Elasticum. Exp. Dermatol. 2021, 31, 14498. [Google Scholar] [CrossRef] [PubMed]
- Dedinszki, D.; Szeri, F.; Kozák, E.; Pomozi, V.; Tőkési, N.; Mezei, T.R.; Merczel, K.; Letavernier, E.; Tang, E.; Le Saux, O.; et al. Oral Administration of Pyrophosphate Inhibits Connective Tissue Calcification. EMBO Mol. Med. 2017, 9, 1463–1470. [Google Scholar] [CrossRef] [PubMed]
- Plomp, A.S.; Bergen, A.A.B.; Florijn, R.J.; Terry, S.F.; Toonstra, J.; van Dijk, M.R.; de Jong, P.T.V.M. Pseudoxanthoma Elasticum: Wide Phenotypic Variation in Homozygotes and No Signs in Heterozygotes for the c.3775delT Mutation in ABCC6. Genet. Med. 2009, 11, 852–858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ralph, D.; Nitschke, Y.; Levine, M.A.; Caffet, M.; Wurst, T.; Saeidian, A.H.; Youssefian, L.; Vahidnezhad, H.; Terry, S.F.; Rutsch, F.; et al. ENPP1 Variants in Patients with GACI and PXE Expand the Clinical and Genetic Heterogeneity of Heritable Disorders of Ectopic Calcification. PLoS Genet. 2022, 18, e1010192. [Google Scholar] [CrossRef] [PubMed]
- de Boussac, H.; Ratajewski, M.; Sachrajda, I.; Köblös, G.; Tordai, A.; Pulaski, L.; Buday, L.; Váradi, A.; Arányi, T. The ERK1/2-Hepatocyte Nuclear Factor 4alpha Axis Regulates Human ABCC6 Gene Expression in Hepatocytes. J. Biol. Chem. 2010, 285, 22800–22808. [Google Scholar] [CrossRef] [Green Version]
- Abruzzese, V.; Matera, I.; Martinelli, F.; Carmosino, M.; Koshal, P.; Milella, L.; Bisaccia, F.; Ostuni, A. Effect of Quercetin on ABCC6 Transporter: Implication in HepG2 Migration. Int. J. Mol. Sci. 2021, 22, 3871. [Google Scholar] [CrossRef] [PubMed]
- Szeri, F.; Lundkvist, S.; Donnelly, S.; Engelke, U.F.H.; Rhee, K.; Williams, C.J.; Sundberg, J.P.; Wevers, R.A.; Tomlinson, R.E.; Jansen, R.S.; et al. The Membrane Protein ANKH Is Crucial for Bone Mechanical Performance by Mediating Cellular Export of Citrate and ATP. PLoS Genet. 2020, 16, e1008884. [Google Scholar] [CrossRef]
- Villa-Bellosta, R. ATP-Based Therapy Prevents Vascular Calcification and Extends Longevity in a Mouse Model of Hutchinson-Gilford Progeria Syndrome. Proc. Natl. Acad. Sci. USA 2019, 116, 23698–23704. [Google Scholar] [CrossRef] [PubMed]
- Jahnen-Dechent, W.; Schinke, T.; Trindl, A.; Müller-Esterl, W.; Sablitzky, F.; Kaiser, S.; Blessing, M. Cloning and Targeted Deletion of the Mouse Fetuin Gene. J. Biol. Chem. 1997, 272, 31496–31503. [Google Scholar] [CrossRef] [Green Version]
- Zhao, J.; Kingman, J.; Sundberg, J.P.; Uitto, J.; Li, Q. Plasma PPi Deficiency Is the Major, but Not the Exclusive, Cause of Ectopic Mineralization in an Abcc6-/-Mouse Model of PXE. J. Investig. Dermatol. 2017, 137, 2336–2343. [Google Scholar] [CrossRef]
- Li, Q.; Huang, J.; Pinkerton, A.B.; Millan, J.L.; van Zelst, B.D.; Levine, M.A.; Sundberg, J.P.; Uitto, J. Inhibition of Tissue-Nonspecific Alkaline Phosphatase Attenuates Ectopic Mineralization in the Abcc6-/- Mouse Model of PXE but Not in the Enpp1 Mutant Mouse Models of GACI. J. Investig. Dermatol. 2019, 139, 360–368. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Albright, R.A.; Stabach, P.; Cao, W.; Kavanagh, D.; Mullen, I.; Braddock, A.A.; Covo, M.S.; Tehan, M.; Yang, G.; Cheng, Z.; et al. ENPP1-Fc Prevents Mortality and Vascular Calcifications in Rodent Model of Generalized Arterial Calcification of Infancy. Nat. Commun. 2015, 6, 10006. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jacobs, I.J.; Cheng, Z.; Ralph, D.; O’Brien, K.; Flaman, L.; Howe, J.; Thompson, D.; Uitto, J.; Li, Q.; Sabbagh, Y. INZ-701, a Recombinant ENPP1 Enzyme, Prevents Ectopic Calcification in an Abcc6-/- Mouse Model of Pseudoxanthoma Elasticum. Exp. Dermatol. 2022, 31, 1095–1101. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, S.G.; Ferreira, C.R.; MacFarlane, E.G.; Riddle, R.C.; Tomlinson, R.E.; Chew, E.Y.; Martin, L.; Ma, C.-T.; Sergienko, E.; Pinkerton, A.B.; et al. Ectopic Calcification in Pseudoxanthoma Elasticum Responds to Inhibition of Tissue-Nonspecific Alkaline Phosphatase. Sci. Transl. Med. 2017, 9, eaal1669. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kranenburg, G.; de Jong, P.A.; Bartstra, J.W.; Lagerweij, S.J.; Lam, M.G.; Ossewaarde-van Norel, J.; Risseeuw, S.; van Leeuwen, R.; Imhof, S.M.; Verhaar, H.J.; et al. Etidronate for Prevention of Ectopic Mineralization in Patients With Pseudoxanthoma Elasticum. J. Am. Coll. Cardiol. 2018, 71, 1117–1126. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | PXE (n = 207) | Controls (n = 45) | p-Value |
|---|---|---|---|
| Age, years | 55 ± 13 | 53 ± 16 | 0.21 |
| Sex, female | 126 (61%) | 19 (42%) | 0.02 |
| PPi, µM | 0.53 ± 0.15 | 1.13 ± 0.29 | <0.01 |
| Genotype | n = 192 | ||
| Two truncating, n (%) | 116 (56%) | ||
| Mixed, n (%) | 71 (34%) | ||
| Two non-truncating, n (%) | 14 (7%) | ||
| Arterial calcification | n = 189 | ||
| Peripheral, mass score | 589 (82–1932) | ||
| Total body, mass score | 1518 (186–4178) | ||
| Arterial functioning | n = 207 | ||
| Ankle brachial index | 0.89 (0.63–1.04) | ||
| Peripheral arterial disease, n (%) | 108 (52%) | ||
| Fontaine classification | |||
| No peripheral arterial disease, n (%) | 98 (47%) | ||
| Asymptomatic, n (%) | 67 (32%) | ||
| Symptomatic, n (%) | 42 (20%) | ||
| Ophthalmology | n = 193 | ||
| Length of angioid streaks | |||
| <3 mm from optic disc | 1 (0.5%) | ||
| 3–6 mm from optic disc | 38 (20%) | ||
| 6–9 mm from optic disc | 60 (32%) | ||
| >9 mm from optic disc | 87 (47%) | ||
| Choroidal neovascularization, n (%) | 119 (62%) | ||
| Macular atrophy, n (%) | |||
| Mild | 25 (13%) | ||
| Severe | 29 (15%) | ||
| Visual acuity, LogMar | 0.10 (0.00–0.70) |
| Variable | Age and Sex Adjusted β (95% Confidence Interval) |
|---|---|
| Arterial calcification mass | |
| Peripheral arteries | 0.00 (−0.02;0.02) |
| Total body | 0.01 (−0.02;0.04) |
| Arterial functioning | |
| Ankle brachial index | 0.02 (−0.06;0.09) |
| Peripheral arterial disease | 0.02 (−0.02;0.06) |
| Fontaine classification | 0.00 (−0.03;0.03) |
| Ophthalmology | |
| Angioid streaks | 0.01 (−0.02;0.03) |
| Choroidal neovascularization | 0.06 (0.01;0.11) * |
| Macular atrophy | 0.01 (−0.02;0.04) |
| Visual acuity | −0.00 (−0.04;0.03) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kozák, E.; Bartstra, J.W.; de Jong, P.A.; Mali, W.P.T.M.; Fülöp, K.; Tőkési, N.; Pomozi, V.; Risseeuw, S.; Norel, J.O.-v.; van Leeuwen, R.; et al. Plasma Level of Pyrophosphate Is Low in Pseudoxanthoma Elasticum Owing to Mutations in the ABCC6 Gene, but It Does Not Correlate with ABCC6 Genotype. J. Clin. Med. 2023, 12, 1047. https://doi.org/10.3390/jcm12031047
Kozák E, Bartstra JW, de Jong PA, Mali WPTM, Fülöp K, Tőkési N, Pomozi V, Risseeuw S, Norel JO-v, van Leeuwen R, et al. Plasma Level of Pyrophosphate Is Low in Pseudoxanthoma Elasticum Owing to Mutations in the ABCC6 Gene, but It Does Not Correlate with ABCC6 Genotype. Journal of Clinical Medicine. 2023; 12(3):1047. https://doi.org/10.3390/jcm12031047
Chicago/Turabian StyleKozák, Eszter, Jonas W. Bartstra, Pim A. de Jong, Willem P. T. M. Mali, Krisztina Fülöp, Natália Tőkési, Viola Pomozi, Sara Risseeuw, Jeannette Ossewaarde-van Norel, Redmer van Leeuwen, and et al. 2023. "Plasma Level of Pyrophosphate Is Low in Pseudoxanthoma Elasticum Owing to Mutations in the ABCC6 Gene, but It Does Not Correlate with ABCC6 Genotype" Journal of Clinical Medicine 12, no. 3: 1047. https://doi.org/10.3390/jcm12031047