
Time Trends in Clinical Characteristics and Hospital Outcomes of Hospitalizations for Lung Transplantation in COPD Patients in Spain from 2016 to 2020—Impact of the COVID-19 Pandemic
 , ,
, ,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Data Source
2.2. Study Population and Study Variables
2.3. Statistical Analysis
2.4. Ethics Statement
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sheshadri, A.; Sacks, N.C.; Healey, B.; Cyr, P.; Boerner, G.; Huang, H.J. The healthcare resource utilization and costs of chronic lung allograft dysfunction following lung transplantation in patients with commercial insurance in the United States. J. Med. Econ. 2022, 25, 650–659. [Google Scholar] [CrossRef] [PubMed]
- Yeo, H.J.; Oh, D.K.; Yu, W.S.; Choi, S.M.; Jeon, K.; Ha, M.; Lee, J.G.; Cho, W.H.; Kim, Y.T. Outcomes of Patients on the Lung Transplantation Waitlist in Korea: A Korean Network for Organ Sharing Data Analysis. J. Korean Med. Sci. 2022, 37, e294. [Google Scholar] [CrossRef]
- Arjuna, A.; Olson, M.T.; Walia, R. Current trends in candidate selection, contraindications, and indications for lung transplantation. J. Thorac. Dis. 2021, 13, 6514–6527. [Google Scholar] [CrossRef] [PubMed]
- Adegunsoye, A.; Strek, M.E.; Garrity, E.; Guzy, R.; Bag, R. Comprehensive Care of the Lung Transplant Patient. Chest 2017, 152, 150–164. [Google Scholar] [CrossRef]
- Nęcki, M.; Pandel, A.; Urlik, M.; Antończyk, R.; Latos, M.; Gawęda, M.; Stącel, T.; Wajda-Pokrontka, M.; Zawadzki, F.; Okienica, M.; et al. The Impact of Airway Complications on Survival Among Lung Transplant Recipients. Transplant. Proc. 2020, 52, 2173–2177. [Google Scholar] [CrossRef] [PubMed]
- Chambers, D.C.; Perch, M.; Zuckermann, A.; Cherikh, W.S.; Harhay, M.O.; Hayes, D., Jr.; Hsich, E.; Khush, K.K.; Potena, L.; Sadavarte, A.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-eighth adult lung transplantation report—2021; Focus on recipient characteristics. J. Heart Lung Transplant. 2021, 40, 1060–1072. [Google Scholar] [CrossRef]
- Hume, E.; Ward, L.; Wilkinson, M.; Manifield, J.; Clark, S.; Vogiatzis, I. Exercise training for lung transplant candidates and recipients: A systematic review. Eur. Respir. Rev. 2020, 29, 200053. [Google Scholar] [CrossRef]
- Timofte, I.; Wijesinha, M.; Vesselinov, R.; Kim, J.; Reed, R.; Sanchez, P.G.; Ladikos, N.; Pham, S.; Kon, Z.; Rajagopal, K.; et al. Survival benefit of lung transplantation compared with medical management and pulmonary rehabilitation for patients with end-stage COPD. ERJ Open Res. 2020, 6, 00177-2019. [Google Scholar] [CrossRef]
- Hull, T.D.; Leya, G.A.; Axtell, A.L.; Moonsamy, P.; Osho, A.; Chang, D.C.; Sundt, T.M.; Villavicencio, M.A. Lung transplantation for chronic obstructive pulmonary disease: A call to modify the lung allocation score to decrease waitlist mortality. J. Thorac. Cardiovasc. Surg. 2022, 164, 1222–1233.e11. [Google Scholar] [CrossRef]
- Schaffer, J.M.; Singh, S.K.; Reitz, B.A.; Zamanian, R.T.; Mallidi, H.R. Single- vs double-lung transplantation in patients with chronic obstructive pulmonary disease and idiopathic pulmonary fibrosis since the implementation of lung allocation based on medical need. JAMA 2015, 313, 936–948. [Google Scholar] [CrossRef]
- Todd, J.L.; Palmer, S.M. Lung transplantation in advanced COPD: Is it worth it? Semin. Respir. Crit. Care Med. 2010, 31, 365–372. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chan, E.G.; Chan, P.G.; Harano, T.; Ryan, J.P.; Morrell, M.R.; Sanchez, P.G. Trends in Lung Transplantation Practices Across the United States During the COVID-19 Pandemic. Transplantation 2021, 105, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Coll, E.; Santos, F.; Ussetti, P.; Canela, M.; Borro, J.M.; De La Torre, M.; Varela, A.; Zurbano, F.; Mons, R.; Morales, P.; et al. The Spanish Lung Transplant Registry: First report of results (2006-2010). Arch. Bronconeumol. 2013, 49, 70–78. [Google Scholar] [CrossRef]
- de Miguel-Díez, J.; López-de-Andres, A.; Hernández-Barrera, V.; de Miguel-Yanes, J.M.; Méndez-Bailón, M.; Jiménez-García, R. Trends and hospital outcomes of lung transplantation among patients with and without chronic obstructive pulmonary disease in Spain: A national population-based study (2001-2015). Int. J. Chron. Obstruct. Pulmon. Dis. 2019, 14, 729–737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Domínguez-Gil, B.; Coll, E.; Fernández-Ruiz, M.; Corral, E.; Del Río, F.; Zaragoza, R.; Rubio, J.J.; Hernández, D. COVID-19 in Spain: Transplantation in the midst of the pandemic. Am. J. Transplant. 2020, 20, 2593–2598. [Google Scholar] [CrossRef] [PubMed]
- Hardman, G.; Sutcliffe, R.; Hogg, R.; Mumford, L.; Grocott, L.; Mead-Regan, S.J.; Nuttall, J.; Dunn, S.; Seeley, P.; Clark, S.; et al. The impact of the SARS-CoV-2 pandemic and COVID-19 on lung transplantation in the UK: Lessons learned from the first wave. Clin. Transplant. 2021, 35, e14210. [Google Scholar] [CrossRef] [PubMed]
- Hallett, A.; Motter, J.D.; Frey, A.; Higgins, R.S.; Bush, E.L.; Snyder, J.; Garonzik-Wang, J.M.; Segev, D.L.; Massie, A.B. Trends in Heart and Lung Transplantation in the United States Across the COVID-19 Pandemic. Transplant. Direct. 2021, 7, e759. [Google Scholar] [CrossRef] [PubMed]
- Benvenuto, L.; Snyder, M.E.; Aversa, M.; Patel, S.; Costa, J.; Shah, L.; Robbins, H.; D’Ovidio, F.; Sonett, J.; Stanifer, B.P.; et al. Geographic Differences in Lung Transplant Volume and Donor Availability During the COVID-19 Pandemic. Transplantation 2021, 105, 861–866. [Google Scholar] [CrossRef]
- Ministerio de Sanidad, Servicios Sociales e Igualdad. Real Decreto 69/2015, de 6 de febrero, por el que se regula el Registro de Actividad de Atención Sanitaria Especializada. (Spanish National Hospital Discharge Database). BOE 2015, 35, 10789–10809. Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/docs/BOE_RD_69_2015_RAE_CMBD.pdf (accessed on 12 November 2022).
- Sundararajan, V.; Henderson, T.; Perry, C.; Muggivan, A.; Quan, H.; Ghali, W.A. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J. Clin. Epidemiol. 2004, 57, 1288–1294. [Google Scholar] [CrossRef]
- Quan, H.; Sundararajan, V.; Halfon, P.; Fong, A.; Burnand, B.; Luthi, J.C.; Saunders, L.D.; Beck, C.A.; Feasby, T.E.; Ghali, W.A. Coding algorithms for defining comorbidities in ICD-9-CM and ICD-10 administrative data. Med. Care 2005, 43, 1130–1139. [Google Scholar] [CrossRef] [PubMed]
- Ministerio de Sanidad, Consumo y Bienestar Social. Solicitud de Extracción de Datos—Extraction Request (Spanish National Hospital Discharge Database). Available online: https://www.mscbs.gob.es/estadEstudios/estadisticas/estadisticas/estMinisterio/SolicitudCMBDdocs/2018_Formulario_Peticion_Datos_RAE_CMBD.pdf (accessed on 12 November 2022).
- Leard, L.E.; Holm, A.M.; Valapour, M.; Glanville, A.R.; Attawar, S.; Aversa, M.; Campos, S.V.; Christon, L.M.; Cypel, M.; Dellgren, G.; et al. Consensus document for the selection of lung transplant candidates: An update from the International Society for Heart and Lung Transplantation. J. Heart Lung Transplant. 2021, 40, 1349–1379. [Google Scholar] [CrossRef] [PubMed]
- Barrecheguren, M.; Sáez-Giménez, B. Lung Transplantation in the COVID Era: Impact and New Paradigms. Arch. Bronconeumol. 2021, 57, 19–20. [Google Scholar] [CrossRef]
- Domínguez-Gil, B.; Coll, E.; Ferrer-Fàbrega, J.; Briceño, J.; Ríos, A. Dramatic impact of the COVID-19 outbreak on donation and transplantation activities in Spain. Cir. Esp. 2020, 98, 412–414. [Google Scholar] [CrossRef]
- Aubert, O.; Yoo, D.; Zielinski, D.; Cozzi, E.; Cardillo, M.; Dürr, M.; Domínguez-Gil, B.; Coll, E.; Da Silva, M.I.; Sallinen, V.; et al. COVID-19 pandemic and worldwide organ transplantation: A population-based study. Lancet Public Health 2021, 6, e709–e719. [Google Scholar] [CrossRef]
- Coiffard, B.; Lepper, P.M.; Prud’Homme, E.; Daviet, F.; Cassir, N.; Wilkens, H.; Hraiech, S.; Langer, F.; Thomas, P.A.; Reynaud-Gaubert, M.; et al. Management of lung transplantation in the COVID-19 era-An international survey. Am. J. Transplant. 2021, 21, 1586–1596. [Google Scholar] [CrossRef] [PubMed]
- Levine, S.M.; Anzueto, A.; Peters, J.I.; Cronin, T.; Sako, E.Y.; Jenkinson, S.G.; Bryan, C.L. Medium term functional results of single-lung transplantation for endstage obstructive lung disease. Am. J. Respir. Crit. Care Med. 1994, 150, 398–402. [Google Scholar] [CrossRef]
- Chambers, D.C.; Cherikh, W.S.; Goldfarb, S.B.; Hayes, D., Jr.; Kucheryavaya, A.Y.; Toll, A.E.; Khush, K.K.; Levvey, B.J.; Meiser, B.; Rossano, J.W.; et al. The International Thoracic Organ Transplant Registry of the International Society for Heart and Lung Transplantation: Thirty-fifth adult lung and heart-lung transplant report-2018; Focus theme: Multiorgan Transplantation. J. Heart Lung Transplant. 2018, 37, 1169–1183. [Google Scholar] [CrossRef]
- Singhal, A.; Reed, R.M. Pitfalls of single lung transplantation (SLT) for chronic obstructive pulmonary disease. BMJ Case Rep. 2014, 2014, bcr2014204355. [Google Scholar] [CrossRef] [Green Version]
- Yu, H.; Bian, T.; Yu, Z.; Wei, Y.; Xu, J.; Zhu, J.; Zhang, W. Bilateral Lung Transplantation Provides Better Long-term Survival and Pulmonary Function Than Single Lung Transplantation: A Systematic Review and Meta-analysis. Transplantation 2019, 103, 2634–2644. [Google Scholar] [CrossRef]
- Van Raemdonck, D.; Ceulemans, L.J.; Vos, R.; Verleden, G.M. Commentary: How best to dance tango in lung transplantation for chronic obstructive pulmonary disease? J. Thorac. Cardiovasc. Surg. 2022, 164, 1234–1235. [Google Scholar] [CrossRef] [PubMed]
- Banga, A.; Mohanka, M.; Mullins, J.; Bollineni, S.; Kaza, V.; Ring, S.; Bajona, P.; Peltz, M.; Wait, M.; Torres, F. Hospital length of stay after lung transplantation: Independent predictors and association with early and late survival. J. Heart Lung Transplant. 2017, 36, 289–296. [Google Scholar] [CrossRef] [PubMed]
- Rello, J.; Bello, I.; de Vicente, R.; Hermira Anchuelo, A.; Ballesteros, M.Á.; Iranzo, R.; Rellán, L.; Riera, J.; Robles, J.C.; EMPRET Study investigators. Risk Factors for Mortality in 272 Patients With Lung Transplant: A Multicenter Analysis of 7 Intensive Care Units. Arch. Bronconeumol. 2017, 53, 421–426. [Google Scholar] [CrossRef]
- Registro Español de Trasplante Pulmonar. Resultados 2001–2020. Available online: http://www.ont.es/infesp/Documents/MEMORIA%20ANUAL%20RETP%202001-2020.pdf (accessed on 12 November 2022).
- Xiao, H.; Campbell, E.S.; Song, K.S. A trend analysis of organ transplantation among ethnic groups. J. Natl. Med. Assoc. 2002, 94, 15–20, Erratum in J. Natl. Med. Assoc. 2002, 94, 659–660. [Google Scholar]
- López-de-Andrés, A.; de Miguel-Yanes, J.M.; Hernández-Barrera, V.; Méndez-Bailón, M.; González-Pascual, M.; de Miguel-Díez, J.; Salinero-Fort, M.A.; Pérez-Farinós, N.; Jiménez-Trujillo, I.; Jiménez-García, R. Renal transplant among type 1 and type 2 diabetes patients in Spain: A population-based study from 2002 to 2013. Eur. J. Intern. Med. 2017, 37, 64–68. [Google Scholar] [CrossRef] [PubMed]
- Fabbian, F.; Verzola, A.; Napoli, N.; De Giorgi, A.; Comai, G.; La Manna, G.; Gallerani, M.; Manfredini, R.; A Rodríguez-Borrego, M.; López-Soto, P.J. Impact of hospital admissions subsequent to renal transplantation on Italian regional resources: A retrospective study in the Italian region of Emilia-Romagna. Minerva Urol. Nefrol. 2019, 71, 612–618. [Google Scholar] [CrossRef]
- Godown, J.; Hall, M.; Thompson, B.; Thurm, C.; Jabs, K.; Gillis, L.A.; Hafberg, E.T.; Alexopoulos, S.; Karp, S.J.; Soslow, J.H. Expanding analytic possibilities in pediatric solid organ transplantation through linkage of administrative and clinical registry databases. Pediatr. Transplant. 2019, 23, e13379. [Google Scholar] [CrossRef]
- Hosseini-Moghaddam, S.M.; Ouédraogo, A.; Naylor, K.L.; Bota, S.E.; Husain, S.; Nash, D.M.; Paterson, J.M. Incidence and outcomes of invasive fungal infection among solid organ transplant recipients: A population-based cohort study. Transpl. Infect. Dis. 2020, 22, e13250. [Google Scholar] [CrossRef]
- Isath, A.; Rao, S.D.; Siroky, G.P.; Padmanabhan, D.; Bandyopadhyay, D.; Krittanawong, C.; Mohammed, S.; Chahal, C.A.A.; Perimbeti, S.; Mehta, D.; et al. Trends, Prevalence, and Outcomes of Sudden Cardiac Arrest Post Cardiac Transplant: A Nationwide 16-Year Study. Curr. Probl. Cardiol. 2022, 47, 100901. [Google Scholar] [CrossRef] [PubMed]
- Isath, A.; Sherif, A.A.; Siroky, G.P.; Bandyopadhyay, D.; Rao, S.D.; Krittanawong, C.; Padmanabhan, D.; Perimbeti, S.; Garg, V.P.; Chahal, A.A.; et al. Trends, Burden, and Impact of Arrhythmias on Cardiac Transplant Recipients: A 16-year Nationwide Study. Curr. Probl. Cardiol. 2022, 48, 101504. [Google Scholar] [CrossRef]
- Gomez, D.; Acuna, S.A.; Joseph Kim, S.; Nantais, J.; Santiago, R.; Calzavara, A.; Saskin, R.M.; Baxter, N.N.M. Incidence and Mortality of Emergency General Surgery Conditions Among Solid Organ Transplant Recipients in Ontario, Canada: A Population-based Analysis. Transplantation 2022, 4299. [Google Scholar] [CrossRef] [PubMed]
- Patel, S.B.; Webber, Z.; Strah, D.D.; Hellinger, R.D.; Yrun-Duffy, M.; Kowalek, K.A.; Seckeler, M.D. Acute Hospital Outcomes for Renal Transplantation in Patients With Moderate or Severe Congenital Heart Disease. Am. J. Cardiol. 2023, 186, 87–90. [Google Scholar] [CrossRef] [PubMed]
- Fielding-Singh, V.; Grogan, T.R.; Neelankavil, J.P. Accuracy of administrative database estimates of national surgical volume: Solid organ transplantation in the National Inpatient Sample. Clin. Transplant. 2021, 35, e14441. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| 2016 | 2017 | 2018 | 2019 | 2020 | TOTAL | p-Value Trend | ||
|---|---|---|---|---|---|---|---|---|
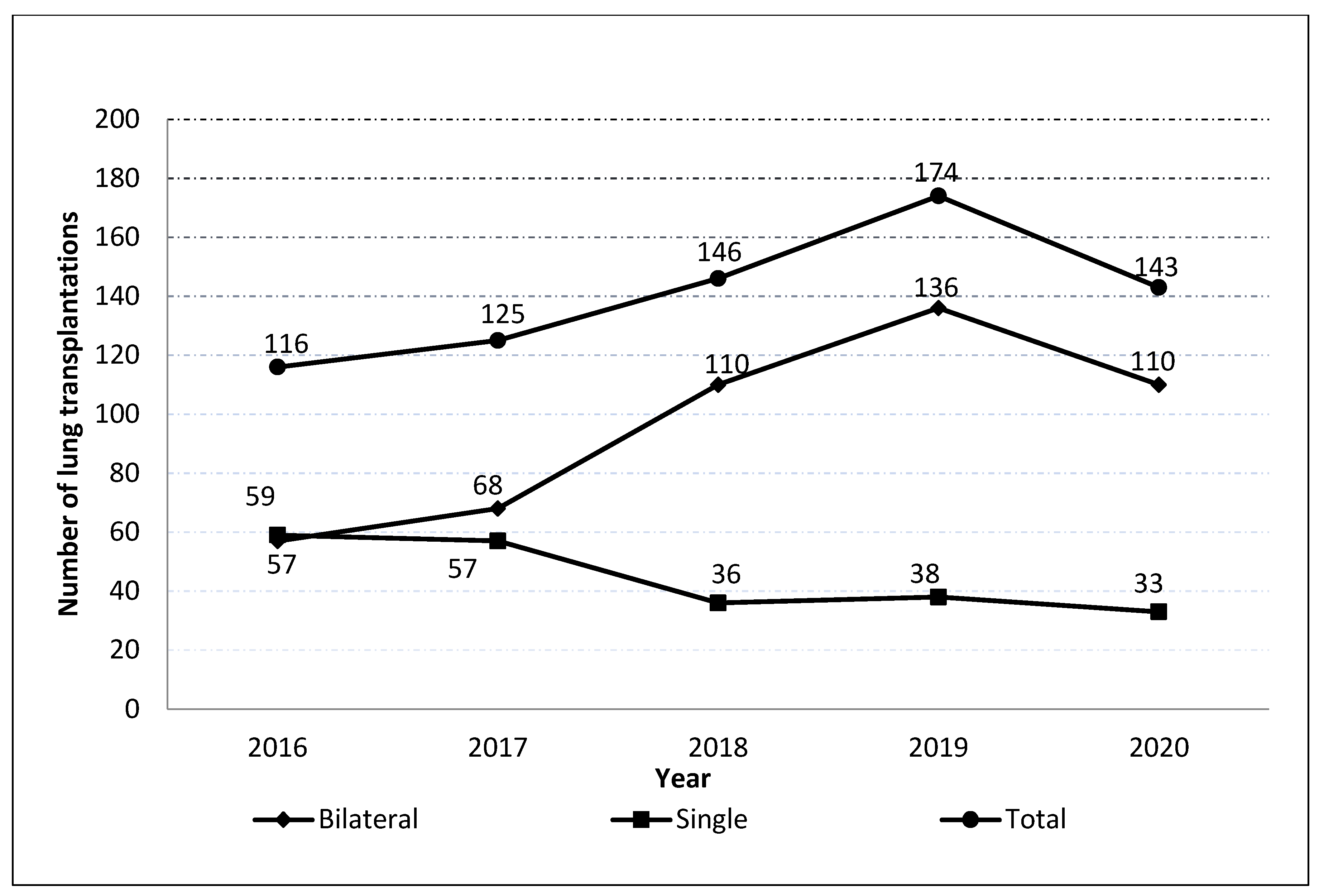
| Number of transplantations | 116 | 125 | 146 | 174 | 143 | 704 | ||
| Type, n (%) | Single | 59 (50.86) | 57 (45.6) | 36 (24.66) | 38 (21.84) | 33 (23.08) | 223 (31.68) | <0.001 |
| Bilateral | 57 (49.14) | 68 (54.4) | 110 (75.34) | 136 (78.16) | 110 (76.92) | 481 (68.32) | ||
| Men, n (%) | 84 (72.41) | 95 (76) | 98 (67.12) | 117 (67.24) | 91 (63.64) | 485 (68.89) | 0.207 | |
| Age, mean (SD) | 57.28 (7.73) | 58.55 (5.98) | 57.59 (7.7) | 58.16 (8) | 58.68 (8.73) | 58.07 (7.73) | 0.533 | |
| Age groups, n (%) | <40 years | 5 (4.31) | 2 (1.6) | 5 (3.42) | 7 (4.02) | 2 (1.4) | 21 (2.98) | 0.414 |
| 40–49 years, | 6 (5.17) | 6 (4.8) | 15 (10.27) | 13 (7.47) | 12 (8.39) | 52 (7.39) | ||
| 50–59 years | 52 (44.83) | 52 (41.6) | 54 (36.99) | 61 (35.06) | 47 (32.87) | 266 (37.78) | ||
| ≥60 years, | 53 (45.69) | 65 (52) | 72 (49.32) | 93 (53.45) | 82 (57.34) | 365 (51.85) | ||
| CCI, mean (SD) | 0.28(0.54) | 0.31 (0.56) | 0.34 (0.58) | 0.48 (0.69) | 0.36 (0.62) | 0.36 (0.61) | 0.056 | |
| CCI, n (%) | 0 | 88 (75.86) | 92 (73.6) | 104 (71.23) | 107 (61.49) | 101 (70.63) | 492 (69.89) | 0.067 |
| ≥1 | 28 (24.14) | 33 (26.4) | 42 (28.77) | 67 (38.51) | 42 (29.37) | 212 (30.11) | ||
| LOHS, median (IQR) | 32.5 (20) | 33 (24) | 34 (31) | 34 (20) | 30 (18) | 33 (21) | 0.782 | |
| IHM, n (%) | 11 (9.48) | 10 (8) | 17 (11.64) | 17 (9.77) | 15 (10.49) | 70 (9.94) | 0.897 | |
| 2016 | 2017 | 2018 | 2019 | 2020 | TOTAL | p-Value Trend | |
|---|---|---|---|---|---|---|---|
| Myocardial infarction, n (%) | 2 (1.72) | 2 (1.6) | 2 (1.37) | 6 (3.45) | 3 (2.1) | 15 (2.13) | 0.715 |
| Congestive heart failure, n (%) | 5 (4.31) | 6 (4.8) | 6 (4.11) | 12 (6.9) | 2 (1.4) | 31 (4.4) | 0.221 |
| Peripheral vascular disease, n (%) | 0 (0) | 1 (0.8) | 4 (2.74) | 5 (2.87) | 6 (4.2) | 16 (2.27) | 0.151 |
| Cerebrovascular disease, n (%) | 2 (1.72) | 5 (4) | 6 (4.11) | 2 (1.15) | 6 (4.2) | 21 (2.98) | 0.346 |
| Dementia, n (%) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | NA |
| Rheumatoid disease, n (%) | 1 (0.86) | 5 (4) | 2 (1.37) | 2 (1.15) | 3 (2.1) | 13 (1.85) | 0.340 |
| Peptic ulcer disease, n (%) | 1 (0.86) | 2 (1.6) | 2 (1.37) | 1 (0.57) | 1 (0.7) | 7 (0.99) | 0.889 |
| Mild, moderate or severe liver disease, n (%) | 5 (4.31) | 4 (3.2) | 10 (6.85) | 26 (14.94) | 16 (11.19) | 61 (8.66) | 0.001 |
| Diabetes and diabetes with complications, n (%) | 9 (7.76) | 12 (9.6) | 13 (8.9) | 16 (9.2) | 9 (6.29) | 59 (8.38) | 0.859 |
| Hemiplegia or paraplegia, n (%) | 1 (0.86) | 0 (0) | 0 (0) | 2 (1.15) | 2 (1.4) | 5 (0.71) | 0.491 |
| Renal disease, n (%) | 4 (3.45) | 2 (1.6) | 1 (0.68) | 4 (2.3) | 2 (1.4) | 13 (1.85) | 0.537 |
| Cancer and metastatic solid tumor, n (%) | 3 (2.59) | 0 (0) | 2 (1.37) | 7 (4.02) | 2 (1.4) | 14 (1.99) | 0.137 |
| AIDS/HIV, n (%) | 0 (0) | 0 (0) | 1 (0.68) | 0 (0) | 0 (0) | 1 (0.14) | 0.430 |
| Pulmonary hypertension, n (%) | 16 (13.79) | 23 (18.4) | 24 (16.44) | 27 (15.52) | 28 (19.58) | 118 (16.76) | 0.737 |
| Hemodialysis, n (%) | 5 (4.31) | 9 (7.2) | 8 (5.48) | 10 (5.75) | 11 (7.69) | 43 (6.11) | 0.794 |
| Extracorporeal membrane oxygenation, n (%) | 12 (10.34) | 12 (9.6) | 20 (13.7) | 38 (21.84) | 33 (23.08) | 115 (16.34) | 0.002 |
| Tracheostomy, n (%) | 22 (18.97) | 24 (19.2) | 33 (22.6) | 33 (18.97) | 20 (13.99) | 132 (18.75) | 0.466 |
| 2016 | 2017 | 2018 | 2019 | 2020 | TOTAL | p-Value Trend | |
|---|---|---|---|---|---|---|---|
| Lung transplant rejection, n (%) | 21 (18.1) | 18 (14.4) | 44 (30.14) | 61 (35.06) | 26 (18.18) | 170 (24.15) | <0.001 |
| Lung transplant failure, n (%) | 5 (4.31) | 9 (7.2) | 17 (11.64) | 14 (8.05) | 8 (5.59) | 53 (7.53) | 0.189 |
| Lung transplant infection, n (%) | 11 (9.48) | 14 (11.2) | 24 (16.44) | 21 (12.07) | 24 (16.78) | 94 (13.35) | 0.297 |
| Other complications of lung transplant, n (%) | 13 (11.21) | 9 (7.2) | 22 (15.07) | 22 (12.64) | 14 (9.79) | 80 (11.36) | 0.311 |
| Unspecified complication of lung transplant, n (%) | 6 (5.17) | 15 (12) | 4 (2.74) | 0 (0) | 3 (2.1) | 28 (3.98) | <0.001 |
| Any complication of lung transplant, n (%) | 44 (37.93) | 53 (42.4) | 83 (56.85) | 95 (54.6) | 59 (41.26) | 334 (47.44) | 0.002 |
| Pneumonia, n (%) | 5 (4.31) | 6 (4.8) | 13 (8.9) | 13 (7.47) | 8 (5.59) | 45 (6.39) | 0.493 |
| Ventilator associated Pneumonia, n (%) | 2 (1.72) | 1 (0.8) | 2 (1.37) | 2 (1.15) | 2 (1.4) | 9 (1.28) | 0.977 |
| Staphylococcus bacteremia, n (%) | 7 (6.03) | 17 (13.6) | 19 (13.01) | 17 (9.77) | 16 (11.19) | 76 (10.8) | 0.318 |
| Streptococcus bacteremia, n (%) | 2 (1.72) | 2 (1.6) | 2 (1.37) | 0 (0) | 1 (0.7) | 7 (0.99) | 0.529 |
| Gram-negative bacteremia, n (%) | 4 (3.45) | 11 (8.8) | 12 (8.22) | 16 (9.2) | 6 (4.2) | 49 (6.96) | 0.181 |
| Fungemia, n (%) | 2 (1.72) | 2 (1.6) | 3 (2.05) | 1 (0.57) | 2 (1.4) | 10 (1.42) | 0.842 |
| Pseudomonas aeruginosa, n (%) | 9 (7.76) | 7 (5.6) | 12 (8.22) | 5 (2.87) | 12 (8.39) | 45 (6.39) | 0.210 |
| Aspergillus, n (%) | 6 (5.17) | 1 (0.8) | 8 (5.48) | 12 (6.9) | 7 (4.9) | 34 (4.83) | 0.185 |
| Candidiasis, n (%) | 0 (0) | 2 (1.6) | 1 (0.68) | 0 (0) | 2 (1.4) | 5 (0.71) | 0.350 |
| Cytomegalovirus b, n (%) | 0 (0) | 5 (4) | 7 (4.79) | 10 (5.75) | 8 (5.59) | 30 (4.26) | 0.144 |
| 2016 | 2017 | 2018 | 2019 | 2020 | TOTAL | p-Value Trend | ||
|---|---|---|---|---|---|---|---|---|
| Type, n (%) | Single | 5 (8.47) | 2 (3.51) | 6 (16.67) | 3 (7.89) | 8 (24.24) | 24 (10.76) | 0.028 |
| Bilateral | 6 (10.53) | 8 (11.76) | 11 (10) | 14 (10.29) | 7 (6.36) | 46 (9.56) | 0.303 | |
| Sex, n (%) | Men | 7 (8.33) | 6 (6.32) | 10 (10.2) | 8 (6.84) | 12 (13.19) | 43 (8.87) | 0.305 |
| Women | 4 (12.5) | 4 (13.33) | 7 (14.58) | 9 (15.79) | 3 (5.77) | 27 (12.33) | 0.426 | |
| Age, mean (SD) | 58.82 (11.89) | 59.2 (2.39) | 56.71 (9.38) | 56.18 (15.55) | 59.53 (4.6) | 57.87 (10.2) | 0.86 | |
| Age groups, n (%) | <40 years | 1 (20) | 0 (0) | 1 (20) | 2 (28.57) | 0 (0) | 4 (19.05) | 0.936 |
| 40–49 years | 0 (0) | 0 (0) | 2 (13.33) | 1 (7.69) | 0 (0) | 3 (5.77) | 0.964 | |
| 50–59 years | 1 (1.92) | 4 (7.69) | 5 (9.26) | 5 (8.2) | 6 (12.77) | 21 (7.89) | 0.073 | |
| ≥60 years | 9 (16.98) | 6 (9.23) | 9 (12.5) | 9 (9.68) | 9 (10.98) | 42 (11.51) | 0.407 | |
| CCI, mean (SD) | 0.27 (0.47) | 0.5 (0.71) | 0.82 (0.73) | 0.41 (0.62) | 0.53 (0.74) | 0.53 (0.68) | 0.958 | |
| CCI, n (%) | 0 | 8 (9.09) | 6 (6.52) | 6 (5.77) | 11 (10.28) | 9 (8.91) | 40 (8.13) | 0.664 |
| ≥1 | 3 (10.71) | 4 (12.12) | 11 (26.19) | 6 (8.96) | 6 (14.29) | 30 (14.15) | 0.907 | |
| Any complication of lung transplant, n (%) | Yes | 7 (15.91) | 5 (9.43) | 11 (13.25) | 10 (10.53) | 12 (20.34) | 45 (13.47) | 0.506 |
| No | 4 (5.56) | 5 (6.94) | 6 (9.52) | 7 (8.86) | 3 (3.57) | 25 (6.76) | 0.764 | |
| OR (CI 95%) | ||
|---|---|---|
| Sex | Men | 1 |
| Female | 1.59 (0.93–2.72) | |
| Age groups, years | <40 | 1 |
| 40–49 | 0.2 (0.04–1.01) | |
| 50–59 | 0.35 (0.11–1.18) | |
| ≥60 | 0.56 (0.17–1.8) | |
| CCI index | 0 | 1 |
| ≥1 | 1.82 (1.08–3.05) | |
| Any complication of lung transplant | No | 1 |
| Yes | 2.14 (1.27–3.6) | |
| Year | 1.01 (0.83–1.22) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Miguel-Diez, J.; Jimenez-Garcia, R.; Hernández-Barrera, V.; Carabantes-Alarcon, D.; Zamorano-Leon, J.J.; Cuadrado-Corrales, N.; Omaña-Palanco, R.; González-Barcala, F.J.; Lopez-de-Andres, A. Time Trends in Clinical Characteristics and Hospital Outcomes of Hospitalizations for Lung Transplantation in COPD Patients in Spain from 2016 to 2020—Impact of the COVID-19 Pandemic. J. Clin. Med. 2023, 12, 963. https://doi.org/10.3390/jcm12030963
De Miguel-Diez J, Jimenez-Garcia R, Hernández-Barrera V, Carabantes-Alarcon D, Zamorano-Leon JJ, Cuadrado-Corrales N, Omaña-Palanco R, González-Barcala FJ, Lopez-de-Andres A. Time Trends in Clinical Characteristics and Hospital Outcomes of Hospitalizations for Lung Transplantation in COPD Patients in Spain from 2016 to 2020—Impact of the COVID-19 Pandemic. Journal of Clinical Medicine. 2023; 12(3):963. https://doi.org/10.3390/jcm12030963
Chicago/Turabian StyleDe Miguel-Diez, Javier, Rodrigo Jimenez-Garcia, Valentin Hernández-Barrera, David Carabantes-Alarcon, Jose J. Zamorano-Leon, Natividad Cuadrado-Corrales, Ricardo Omaña-Palanco, Francisco Javier González-Barcala, and Ana Lopez-de-Andres. 2023. "Time Trends in Clinical Characteristics and Hospital Outcomes of Hospitalizations for Lung Transplantation in COPD Patients in Spain from 2016 to 2020—Impact of the COVID-19 Pandemic" Journal of Clinical Medicine 12, no. 3: 963. https://doi.org/10.3390/jcm12030963