
Association of Shunt Size and Long-Term Clinical Outcomes in Patients with Cryptogenic Ischemic Stroke and Patent Foramen Ovale on Medical Management
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Methods
2.1. Data Collection
2.2. TCD Protocol
2.3. Grading of Shunt Sizes
2.4. Clinical Outcomes
2.5. Statistical Analysis
2.6. Statement of Ethics
3. Results
3.1. Large vs. Small Shunt: Baseline Patient Characteristics
3.2. Large vs. Small Shunt: Primary and Secondary Outcomes
3.3. Predictors of Recurrent Stroke
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Yaghi, S.; Bernstein, R.A.; Passman, R.; Okin, P.M.; Furie, K.L. Cryptogenic Stroke. Circul. Res. 2017, 120, 527–540. [Google Scholar] [CrossRef] [PubMed]
- Belkin, R.N.; Kisslo, J. Atrial septal aneurysm: Recognition and clinical relevance. Am. Heart J. 1990, 120, 948–957. [Google Scholar] [CrossRef] [PubMed]
- Hara, H.; Virmani, R.; Ladich, E.; Mackey-Bojack, S.; Titus, J.; Reisman, M.; Gray, W.; Nakamura, M.; Mooney, M.; Poulose, A.; et al. Patent foramen ovale: Current pathology, pathophysiology, and clinical status. J. Am. Coll. Cardiol. 2005, 46, 1768–1776. [Google Scholar] [CrossRef] [Green Version]
- Lechat, P.; Mas, J.L.; Lascault, G.; Loron, P.; Theard, M.; Klimczac, M.; Drobinski, G.; Thomas, D.; Grosgogeat, Y. Prevalence of patent foramen ovale in patients with stroke. N. Engl. J. Med. 1988, 318, 1148–1152. [Google Scholar] [CrossRef]
- Koutroulou, I.; Tsivgoulis, G.; Tsalikakis, D.; Karacostas, D.; Grigoriadis, N.; Karapanayiotides, T. Epidemiology of Patent Foramen Ovale in General Population and in Stroke Patients: A Narrative Review. Front. Neurol. 2020, 11, 281. [Google Scholar] [CrossRef]
- Koutroulou, I.; Tsivgoulis, G.; Karacostas, D.; Ikonomidis, I.; Grigoriadis, N.; Karapanayiotides, T. Prevalence of patent foramen ovale in the Greek population is high and impacts on the interpretation of the risk of paradoxical embolism (RoPE) score. Ther. Adv. Neurol. Disord. 2020, 13, 1756286420964673. [Google Scholar] [CrossRef] [PubMed]
- Dia, A.; Cifu, A.S.; Shah, A.P. Management of Patients with a Patent Foramen Ovale With History of Stroke or TIA. JAMA 2021, 325, 81–82. [Google Scholar] [CrossRef] [PubMed]
- Mas, J.L.; Derumeaux, G.; Guillon, B.; Massardier, E.; Hosseini, H.; Mechtouff, L.; Arquizan, C.; Bejot, Y.; Vuillier, F.; Detante, O.; et al. Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke. N. Engl. J. Med. 2017, 377, 1011–1021. [Google Scholar] [CrossRef]
- Sondergaard, L.; Kasner, S.E.; Rhodes, J.F.; Andersen, G.; Iversen, H.K.; Nielsen-Kudsk, J.E.; Settergren, M.; Sjostrand, C.; Roine, R.O.; Hildick-Smith, D.; et al. Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke. N. Engl. J. Med. 2017, 377, 1033–1042. [Google Scholar] [CrossRef] [PubMed]
- Furlan, A.J.; Reisman, M.; Massaro, J.; Mauri, L.; Adams, H.; Albers, G.W.; Felberg, R.; Herrmann, H.; Kar, S.; Landzberg, M.; et al. Closure or Medical Therapy for Cryptogenic Stroke with Patent Foramen Ovale. N. Engl. J. Med. 2012, 366, 991–999. [Google Scholar] [CrossRef] [Green Version]
- Meier, B.; Kalesan, B.; Mattle, H.P.; Khattab, A.A.; Hildick-Smith, D.; Dudek, D.; Andersen, G.; Ibrahim, R.; Schuler, G.; Walton, A.S.; et al. Percutaneous Closure of Patent Foramen Ovale in Cryptogenic Embolism. N. Engl. J. Med. 2013, 368, 1083–1091. [Google Scholar] [CrossRef] [Green Version]
- Ioannidis, S.G.; Mitsias, P.D. Patent Foramen Ovale in Cryptogenic Ischemic Stroke: Direct Cause, Risk Factor, or Incidental Finding? Front. Neurol. 2020, 11, 567. [Google Scholar] [CrossRef] [PubMed]
- De Castro, S.; Cartoni, D.; Fiorelli, M.; Rasura, M.; Anzini, A.; Zanette, E.M.; Beccia, M.; Colonnese, C.; Fedele, F.; Fieschi, C.; et al. Morphological and Functional Characteristics of Patent Foramen Ovale and Their Embolic Implications. Stroke 2000, 31, 2407–2413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tanzi, A.; Onorato, E.; Casilli, F.; Anzola, G.P. Is the search for right-to-left shunt still worthwhile? Acta Neurol. Scand. 2016, 133, 281–288. [Google Scholar] [CrossRef]
- Wessler, B.S.; Kent, D.M.; Thaler, D.E.; Ruthazer, R.; Lutz, J.S.; Serena, J. The RoPE Score and Right-to-Left Shunt Severity by Transcranial Doppler in the CODICIA Study. Cerebrovasc. Dis. 2015, 40, 52–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, D.M.; Ruthazer, R.; Weimar, C.; Mas, J.L.; Serena, J.; Homma, S.; Di Angelantonio, E.; Di Tullio, M.R.; Lutz, J.S.; Elkind, M.S.; et al. An index to identify stroke-related vs incidental patent foramen ovale in cryptogenic stroke. Neurology 2013, 81, 619–625. [Google Scholar] [CrossRef] [Green Version]
- Homma, S.; Sacco, R.L.; Di Tullio, M.R.; Sciacca, R.R.; Mohr, J.P. Effect of Medical Treatment in Stroke Patients With Patent Foramen Ovale. Circulation 2002, 105, 2625–2631. [Google Scholar] [CrossRef]
- Mas, J.L.; Arquizan, C.; Lamy, C.; Zuber, M.; Cabanes, L.; Derumeaux, G.; Coste, J.; Patent Foramen, O.; Atrial Septal Aneurysm Study Group. Recurrent cerebrovascular events associated with patent foramen ovale, atrial septal aneurysm, or both. N. Engl. J. Med. 2001, 345, 1740–1746. [Google Scholar] [CrossRef]
- Palazzo, P.; Ingrand, P.; Agius, P.; Belhadj Chaidi, R.; Neau, J.P. Transcranial Doppler to detect right-to-left shunt in cryptogenic acute ischemic stroke. Brain Behav. 2019, 9, e01091. [Google Scholar] [CrossRef]
- Komar, M.; Olszowska, M.; Przewlocki, T.; Podolec, J.; Stepniewski, J.; Sobien, B.; Badacz, R.; Kablak-Ziembicka, A.; Tomkiewicz-Pajak, L.; Podolec, P. Transcranial Doppler ultrasonography should it be the first choice for persistent foramen ovale screening? Cardiovasc. Ultrasound 2014, 12, 16. [Google Scholar] [CrossRef] [Green Version]
- Adams, H.P., Jr.; Bendixen, B.H.; Kappelle, L.J.; Biller, J.; Love, B.B.; Gordon, D.L.; Marsh, E.E., 3rd. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke 1993, 24, 35–41. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kleindorfer, D.O.; Towfighi, A.; Chaturvedi, S.; Cockroft, K.M.; Gutierrez, J.; Lombardi-Hill, D.; Kamel, H.; Kernan, W.N.; Kittner, S.J.; Leira, E.C.; et al. 2021 Guideline for the Prevention of Stroke in Patients With Stroke and Transient Ischemic Attack: A Guideline From the American Heart Association/American Stroke Association. Stroke 2021, 52, e364–e467. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Ren, Q.; Song, Y.; He, M.; Zeng, Y.; Liu, Z.; Xu, J. Prognostic role of neutrophil-lymphocyte ratio in patients with acute ischemic stroke. Medicine 2017, 96, e8624. [Google Scholar] [CrossRef] [PubMed]
- Alakbarzade, V.; Taylor, A.; Scully, M.; Simister, R.; Chandratheva, A. Utility of current thrombophilia screening in young patients with stroke and TIA. Stroke Vasc. Neurol. 2018, 3, 231–236. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wilson, W.A.; Gharavi, A.E.; Koike, T.; Lockshin, M.D.; Branch, D.W.; Piette, J.C.; Brey, R.; Derksen, R.; Harris, E.N.; Hughes, G.R.; et al. International consensus statement on preliminary classification criteria for definite antiphospholipid syndrome: Report of an international workshop. Arthritis Rheum. 1999, 42, 1309–1311. [Google Scholar] [CrossRef]
- Yaghi, S.; Moon, Y.P.; Mora-McLaughlin, C.; Willey, J.Z.; Cheung, K.; Di Tullio, M.R.; Homma, S.; Kamel, H.; Sacco, R.L.; Elkind, M.S. Left atrial enlargement and stroke recurrence: The Northern Manhattan Stroke Study. Stroke 2015, 46, 1488–1493. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kamran, S.; Singh, R.; Akhtar, N.; George, P.; Salam, A.; Babu, B.; Own, A.; Hamid, T.; Perkins, J.D. Left Heart Factors in Embolic Stroke of Undetermined Source in a Multiethnic Asian and North African Cohort. J. Am. Heart Assoc. 2020, 9, e016534. [Google Scholar] [CrossRef]
- Devereux, R.B.; Alonso, D.R.; Lutas, E.M.; Gottlieb, G.J.; Campo, E.; Sachs, I.; Reichek, N. Echocardiographic assessment of left ventricular hypertrophy: Comparison to necropsy findings. Am. J. Cardiol. 1986, 57, 450–458. [Google Scholar] [CrossRef]
- Thaler, D.E.; Di Angelantonio, E.; Di Tullio, M.R.; Donovan, J.S.; Griffith, J.; Homma, S.; Jaigobin, C.; Mas, J.L.; Mattle, H.P.; Michel, P.; et al. The risk of paradoxical embolism (RoPE) study: Initial description of the completed database. Int. J. Stroke 2013, 8, 612–619. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Conte, M.; Riegler, L.; Scarafile, R.; Cocchia, R.; Pezzullo, E.; Cavallaro, M.; Di Maio, M.; Natale, F.; Santoro, G.; et al. Transcranial Doppler Ultrasound: Incremental Diagnostic Role in Cryptogenic Stroke Part II. J. Cardiovasc. Echogr. 2016, 26, 71–77. [Google Scholar] [CrossRef] [Green Version]
- Sharma, A.K.; Bathala, L.; Batra, A.; Mehndiratta, M.M.; Sharma, V.K. Transcranial Doppler: Techniques and advanced applications: Part 2. Ann. Indian Acad. Neurol. 2016, 19, 102–107. [Google Scholar] [CrossRef]
- Lao, A.Y.; Sharma, V.K.; Tsivgoulis, G.; Frey, J.L.; Malkoff, M.D.; Navarro, J.C.; Alexandrov, A.V. Detection of right-to-left shunts: Comparison between the International Consensus and Spencer Logarithmic Scale criteria. J. Neuroimaging 2008, 18, 402–406. [Google Scholar] [CrossRef]
- Spencer, M.P.; Moehring, M.A.; Jesurum, J.; Gray, W.A.; Olsen, J.V.; Reisman, M. Power m-mode transcranial Doppler for diagnosis of patent foramen ovale and assessing transcatheter closure. J. Neuroimaging 2004, 14, 342–349. [Google Scholar] [CrossRef] [PubMed]
- Calkins, H.; Brugada, J.; Packer, D.L.; Cappato, R.; Chen, S.-A.; Crijns, H.J.G.; Damiano, R.J., Jr.; Davies, D.W.; Haines, D.E.; Haissaguerre, M.; et al. HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: Recommendations for Personnel, Policy, Procedures and Follow-Up: A report of the Heart Rhythm Society (HRS) Task Force on Catheter and Surgical Ablation of Atrial Fibrillation. Developed in partnership with the European Heart Rhythm Association (EHRA) and the European Cardiac Arrhythmia Society (ECAS); in collaboration with the American College of Cardiology (ACC), American Heart Association (AHA), and the Society of Thoracic Surgeons (STS). Endorsed and Approved by the governing bodies of the American College of Cardiology, the American Heart Association, the European Cardiac Arrhythmia Society, the European Heart Rhythm Association, the Society of Thoracic Surgeons, and the Heart Rhythm Society. Heart Rhythm 2007, 4, 816–861. [Google Scholar] [CrossRef] [PubMed]
- Turc, G.; Calvet, D.; Guerin, P.; Sroussi, M.; Chatellier, G.; Mas, J.L.; Investigators, C. Closure, Anticoagulation, or Antiplatelet Therapy for Cryptogenic Stroke With Patent Foramen Ovale: Systematic Review of Randomized Trials, Sequential Meta-Analysis, and New Insights From the CLOSE Study. J. Am. Heart Assoc. 2018, 7. [Google Scholar] [CrossRef] [Green Version]
- Lee, P.H.; Song, J.K.; Kim, J.S.; Heo, R.; Lee, S.; Kim, D.H.; Song, J.M.; Kang, D.H.; Kwon, S.U.; Kang, D.W.; et al. Cryptogenic Stroke and High-Risk Patent Foramen Ovale: The DEFENSE-PFO Trial. J. Am. Coll. Cardiol. 2018, 71, 2335–2342. [Google Scholar] [CrossRef]
- Mir, H.; Siemieniuk, R.A.C.; Ge, L.C.; Foroutan, F.; Fralick, M.; Syed, T.; Lopes, L.C.; Kuijpers, T.; Mas, J.-L.; Vandvik, P.O.; et al. Patent foramen ovale closure, antiplatelet therapy or anticoagulation in patients with patent foramen ovale and cryptogenic stroke: A systematic review and network meta-analysis incorporating complementary external evidence. BMJ Open 2018, 8, e023761. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stafford, M.B.; Bagley, J.E.; DiGiacinto, D. Comparison of Transthoracic Echocardiography, Transesophageal Echocardiography, and Transcranial Doppler in the Detection of Patent Foramen Ovale as the Etiology for Cryptogenic Stroke. J. Diagn. Med. Sonogr. 2018, 35, 127–133. [Google Scholar] [CrossRef]
- Mojadidi, M.K.; Mahmoud, A.N.; Elgendy, I.Y.; Agarwal, N.; Tobis, J.M. Transesophageal Echocardiography for the Detection of Patent Foramen Ovale. J. Am. Soc. Echocardiogr. 2017, 30, 933–934. [Google Scholar] [CrossRef] [Green Version]
- Mojadidi, M.K.; Bogush, N.; Caceres, J.D.; Msaouel, P.; Tobis, J.M. Diagnostic accuracy of transesophageal echocardiogram for the detection of patent foramen ovale: A meta-analysis. Echocardiography 2014, 31, 752–758. [Google Scholar] [CrossRef]
- Nygren, A.T.; Jogestrand, T. Detection of patent foramen ovale by transcranial Doppler and carotid duplex ultrasonography: A comparison with transoesophageal echocardiography. Clin. Physiol. 1998, 18, 327–330. [Google Scholar] [CrossRef]
- Van, H.; Poommipanit, P.; Shalaby, M.; Gevorgyan, R.; Tseng, C.H.; Tobis, J. Sensitivity of transcranial Doppler versus intracardiac echocardiography in the detection of right-to-left shunt. JACC Cardiovasc. Imaging 2010, 3, 343–348. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Messé, S.R.; Gronseth, G.S.; Kent, D.M.; Kizer, J.R.; Homma, S.; Rosterman, L.; Carroll, J.D.; Ishida, K.; Sangha, N.; Kasner, S.E. Practice advisory update summary: Patent foramen ovale and secondary stroke prevention. Rep. Guidel. Subcomm. Am. Acad. Neurol. 2020, 94, 876–885. [Google Scholar] [CrossRef]
- Katsanos, A.H.; Spence, J.D.; Bogiatzi, C.; Parissis, J.; Giannopoulos, S.; Frogoudaki, A.; Safouris, A.; Voumvourakis, K.; Tsivgoulis, G. Recurrent stroke and patent foramen ovale: A systematic review and meta-analysis. Stroke 2014, 45, 3352–3359. [Google Scholar] [CrossRef] [Green Version]
- Souteyrand, G.; Motreff, P.; Lusson, J.R.; Rodriguez, R.; Geoffroy, E.; Dauphin, C.; Boire, J.Y.; Lamaison, D.; Cassagnes, J. Comparison of transthoracic echocardiography using second harmonic imaging, transcranial Doppler and transesophageal echocardiography for the detection of patent foramen ovale in stroke patients. Eur. J. Echocardiogr. 2006, 7, 147–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kent, D.M.; Saver, J.L.; Ruthazer, R.; Furlan, A.J.; Reisman, M.; Carroll, J.D.; Smalling, R.W.; Juni, P.; Mattle, H.P.; Meier, B.; et al. Risk of Paradoxical Embolism (RoPE)-Estimated Attributable Fraction Correlates With the Benefit of Patent Foramen Ovale Closure: An Analysis of 3 Trials. Stroke 2020, 51, 3119–3123. [Google Scholar] [CrossRef]
- Morais, L.A.; Sousa, L.d.; Fiarresga, A.; Martins, J.D.; Timóteo, A.T.; Monteiro, A.V.; Soares, C.; Agapito, A.; Pinto, F.; Ferreira, R.C. RoPE Score as a Predictor of Recurrent Ischemic Events After Percutaneous Patent Foramen Ovale Closure. Int. Heart J. 2018, 59, 1327–1332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Xu, Y.; Zhao, L.; Zhang, L.; Han, Y.; Wang, P.; Yu, S. Left Atrial Enlargement and the Risk of Stroke: A Meta-Analysis of Prospective Cohort Studies. Front. Neurol. 2020, 11, 26. [Google Scholar] [CrossRef] [PubMed]
- Rigatelli, G.; Zuin, M.; Adami, A.; Aggio, S.; Lanza, D.; d’Elia, K.; Braggion, G.; Russo, M.; Mazza, A.; Roncon, L. Left atrial enlargement as a maker of significant high-risk patent foramen ovale. Int. J. Cardiovasc. Imaging 2019, 35, 2049–2056. [Google Scholar] [CrossRef]
- Lee, M.J.; Park, S.-J.; Yoon, C.H.; Hwang, J.-W.; Ryoo, S.; Kim, S.J.; Kim, G.-M.; Chung, C.-S.; Lee, K.H.; Bang, O.Y. Association of Left Atrial Enlargement with Cortical Infarction in Subjects with Patent Foramen Ovale. J. Stroke 2016, 18, 304–311. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez, C.J.; Homma, S.; Sacco, R.L.; Di Tullio, M.R.; Sciacca, R.R.; Mohr, J.P.; Investigators, P. Race-ethnic differences in patent foramen ovale, atrial septal aneurysm, and right atrial anatomy among ischemic stroke patients. Stroke 2003, 34, 2097–2102. [Google Scholar] [CrossRef] [PubMed]
- Di Tullio, M.R.; Sacco, R.L.; Sciacca, R.R.; Jin, Z.; Homma, S. Patent Foramen Ovale and the Risk of Ischemic Stroke in a Multiethnic Population. J. Am. Coll. Cardiol. 2007, 49, 797–802. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; Dweck, M.R.; Holte, E.; Fontes-Carvalho, R.; Cameli, M.; Aboumarie, H.S.; Diener, H.C.; Haugaa, K.H. EACVI survey on the management of patients with patent foramen ovale and cryptogenic stroke. Eur. Heart J.—Cardiovasc. Imaging 2020, 22, 135–141. [Google Scholar] [CrossRef] [PubMed]



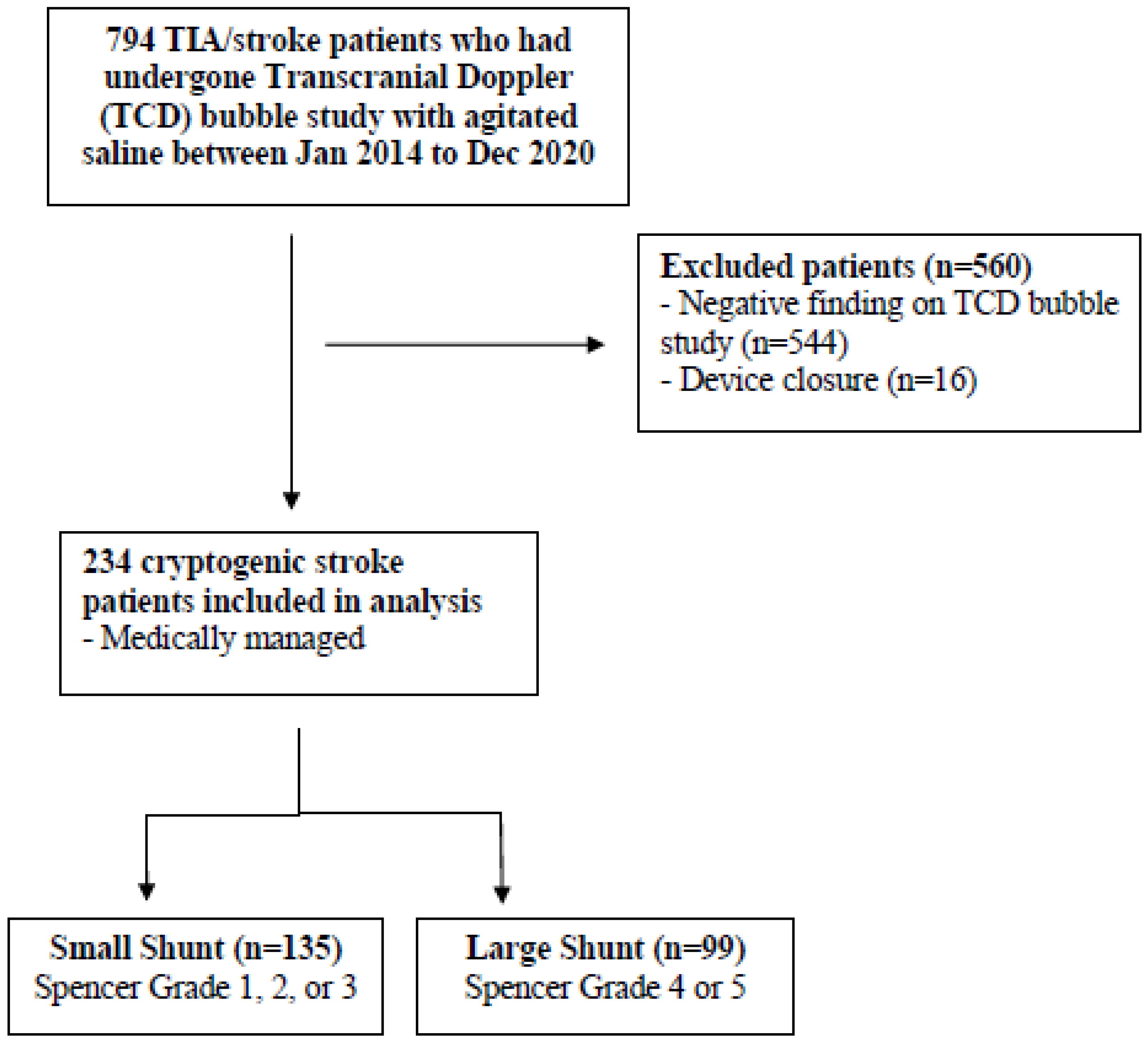{kind=link}
{kind=link}
| Small Shunt (Spencer Grade 1–3) n = 135 | Large Shunt (Spencer Grade 4–5) n = 99 | p-Value | |
|---|---|---|---|
| Patient characteristics | |||
| Age (years) of stroke, mean (SD) | 50.2 (12.6) | 51.0 (13.9) | 0.665 |
| Female, % (n) | 31.1 (42) | 31.3 (31) | 0.974 |
| Race, % (n) | 0.385 | ||
| Chinese | 62.2 (84) | 45.5 (45) | |
| Malay | 8.9 (12) | 6.1 (6) | |
| Indian | 11.1 (15) | 24.2 (24) | |
| Others | 17.8 (24) | 24.2 (24) | |
| Co-morbidities | |||
| Hypertension, % (n) | 36.3 (49) | 28.3 (28) | 0.197 |
| Diabetes mellitus, % (n) | 15.6 (21) | 13.1 (13) | 0.603 |
| Dyslipidaemia, % (n) | 19.3 (26) | 27.3 (27) | 0.148 |
| Ischaemic heart disease, % (n) | 3.7 (5) | 6.1 (6) | 0.400 |
| Smoking, % (n) | 7.4 (10) | 14.1 (14) | 0.093 |
| Previous stroke/TIA, % (n) | 10.4 (14) | 9.1 (9) | 0.745 |
| Chronic kidney disease, % (n) | 1.5 (2) | 1.0 (1) | 0.751 |
| Previous venous thromboembolism, % (n) | 1.5 (2) | 1.0 (1) | 0.751 |
| Presence of thrombophilia, % (n) | 13.1 (53/61) | 18.5 (10/54) | 0.452 |
| Stroke characteristics | |||
| NIHSS on arrival, median (IQR) | 6 (1.8–12.5) | 8 (0.0–16.3) | 0.871 |
| Tissue plasminogen activator, % (n) | 11.9 (16) | 12.1 (12) | 0.950 |
| Endovascular thrombectomy, % (n) | 6.7 (9) | 6.1 (6) | 0.852 |
| Bilateral infarcts, % (n) | 10.4 (14) | 12.1 (12) | 0.674 |
| Infarct involving cortex, % (n) | 44.4 (60) | 54.5 (54) | 0.127 |
| Large vessel occlusion, % (n) | 14.8 (20) | 17.1 (17) | 0.625 |
| Antithrombotic regime | |||
| Single antiplatelet treatment, % (n) | 60.7 (82) | 52.5 (52) | 0.453 |
| Dual antiplatelet treatment, % (n) | 24.4 (33) | 30.3 (30) | 0.289 |
| Anticoagulation, % (n) | |||
| DOACs | 7.4 (10) | 6.1 (6) | 0.959 |
| Vitamin K antagonist | 5.2 (7) | 5.1 (5) | 1.000 |
| Overall | 12.6 (17) | 11.1 (11) | 0.986 |
| Transthoracic echocardiogram (TTE) | |||
| PFO visualized on TTE, % (n) | 3.0 (4) | 5.1 (5) | 0.412 |
| Atrial septal aneurysm, % (n) | 0.07 (1) | 0.1 (1) | 0.825 |
| LVEF < 50%, % (n) | 3.0 (4) | 7.1 (7) | 0.211 |
| Dilated left atrial size ≥ 40 mm, % (n) | 19.3 (26) | 24.2 (24) | 0.420 |
| Others | |||
| Implantable Loop Recorder implantation, % (n) | 8.1 (11) | 2.0 (2) | 0.043 |
| RoPE Score, median (IQR) | 6 (4–7) | 6 (5–7) | 0.734 |
| Outcomes | Small Shunt (Spencer Grade 1–3) n = 135 | Large Shunt (Spencer Grade 4–5) n = 99 | p-Value |
|---|---|---|---|
| No. of days since follow-up, median (IQR) | 301 (143–903) | 400 (146–872) | 0.200 |
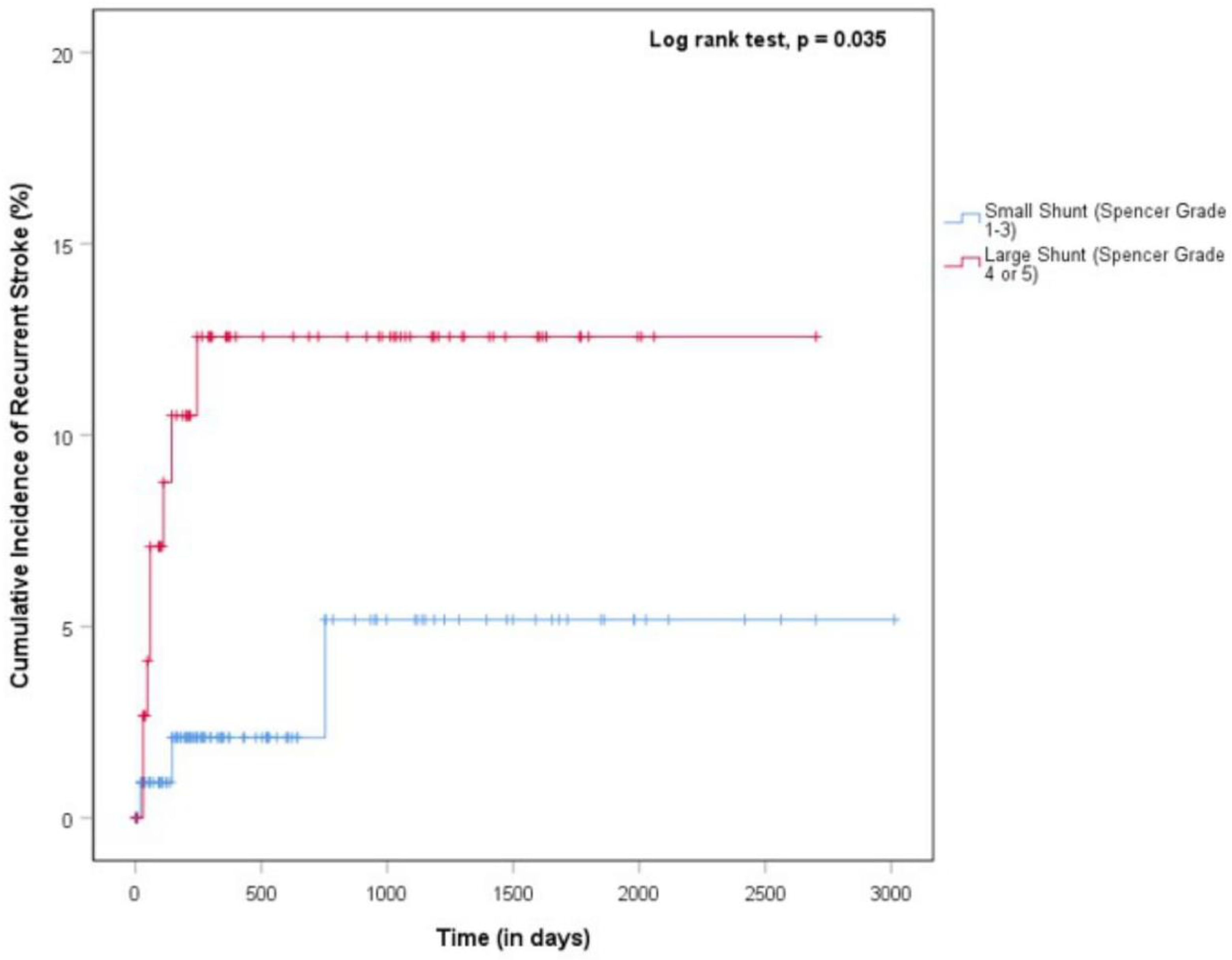
| Recurrent ischemic stroke, % (n) | 2.2 (3) | 8.1 (8) | 0.036 |
| Mortality, % (n) | 3.0 (4) | 0.0 (0) | 0.140 |
| New atrial fibrillation detected, % (n) | 1.5 (2) | 1.0 (1) | 0.751 |
| Variables | No Recurrent Stroke n = 223 | Recurrent Stroke n = 11 | p-Value |
|---|---|---|---|
| Patient characteristics | |||
| Age (years) of stroke, mean (SD) | 50.4 (13.3) | 52.3 (11.6) | 0.651 |
| Female, % (n) | 31.4 (70) | 27.3 (3) | 0.774 |
| Race, % (n) | 0.006 | ||
| Chinese | 56.1 (125) | 36.4 (4) | |
| Malay | 8.1 (18) | 0.0 (0) | |
| Indian | 11.1 (33) | 54.5 (6) | |
| Others | 21.1 (47) | 9.1 (1) | |
| Large shunt (Spencer grade 4–5), % (n) | 40.8 (91) | 72.7 (8) | 0.036 |
| Co-morbidities | |||
| Hypertension, % (n) | 32.7 (73) | 36.4 (4) | 0.803 |
| Diabetes mellitus, % (n) | 14.3 (32) | 18.2 (2) | 0.725 |
| Dyslipidaemia, % (n) | 22.4 (50) | 27.3 (3) | 0.707 |
| Ischaemic heart disease, % (n) | 4.9 (11) | 0.0 (0) | 0.451 |
| Smoking, % (n) | 9.9 (22) | 18.2 (2) | 0.375 |
| Previous stroke/TIA, % (n) | 9.9 (22) | 9.1 (1) | 0.933 |
| Chronic kidney disease, % (n) | 1.3 (3) | 0.0 (0) | 1.00 |
| Previous venous thromboembolism, % (n) | 1.3 (3) | (0) | 1.00 |
| Presence of thrombophilia, % (n) | 16.2 (18/111) | 0.0 (0/4) | 1.00 |
| Initial stroke characteristics | |||
| Bilateral infarcts, % (n) | 11.2 (25) | 9.1 (1) | 0.827 |
| Infarct involving cortex, % (n) | 49.3 (110) | 36.4 (4) | 0.401 |
| Large vessel occlusion | 15.8 (33) | 36.4 (4) | 0.056 |
| Imaging studies | |||
| Patent foramen ovale detected on transthoracic echocardiography, % (n) | 4.6 (9) | 0.0 (0) | 0.467 |
| Atrial septal aneurysm, % (n) | 1.0 (2) | 0.0 (0) | 0.748 |
| LVEF < 50%, % (n) | 4.0 (9) | 18.2 (2) | 0.088 |
| Dilated left atrial size ≥ 40 mm, % (n) | 21.5 (48) | 18.2 (2) | 0.792 |
| Others | |||
| Implantable Loop Recorder implantation, % (n) | 5.4 (12) | 9.1 (1) | 0.600 |
| ROPE score, median (IQR) | 6 (5–7) | 5 (4–7) | 0.448 |
| New atrial fibrillation detected | 1.3 (3) | 0.0 (0) | 0.699 |
| Variable | Adjusted Odds Ratio (95% CI) | p-Value |
|---|---|---|
| Large shunt (Spencer grade 4–5) | 4.09 (1.04–16.0) | 0.043 |
| RoPE score | 0.869 (0.615–1.23) | 0.428 |
| LA diameter > 40 mm | 0.667 (0.134–3.31) | 0.620 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lim, I.C.Z.Y.; Teo, Y.H.; Fang, J.T.; Teo, Y.N.; Ho, J.S.Y.; Lee, Y.Q.; Chen, X.; Ong, K.H.-X.; Leow, A.S.T.; Ho, A.F.-W.; et al. Association of Shunt Size and Long-Term Clinical Outcomes in Patients with Cryptogenic Ischemic Stroke and Patent Foramen Ovale on Medical Management. J. Clin. Med. 2023, 12, 941. https://doi.org/10.3390/jcm12030941
Lim ICZY, Teo YH, Fang JT, Teo YN, Ho JSY, Lee YQ, Chen X, Ong KH-X, Leow AST, Ho AF-W, et al. Association of Shunt Size and Long-Term Clinical Outcomes in Patients with Cryptogenic Ischemic Stroke and Patent Foramen Ovale on Medical Management. Journal of Clinical Medicine. 2023; 12(3):941. https://doi.org/10.3390/jcm12030941
Chicago/Turabian StyleLim, Isis Claire Z. Y., Yao Hao Teo, Jun Tao Fang, Yao Neng Teo, Jamie S. Y. Ho, Yong Qin Lee, Xintong Chen, Kathleen Hui-Xin Ong, Aloysius S. T. Leow, Andrew Fu-Wah Ho, and et al. 2023. "Association of Shunt Size and Long-Term Clinical Outcomes in Patients with Cryptogenic Ischemic Stroke and Patent Foramen Ovale on Medical Management" Journal of Clinical Medicine 12, no. 3: 941. https://doi.org/10.3390/jcm12030941