
Suprapapillary Biliary Stents Have Longer Patency Times than Transpapillary Stents—A Systematic Review and Meta-Analysis
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy and Eligibility Criteria
2.2. Selection Strategy and Data Extraction
2.3. Risk of Bias Assessment and Certainty of Evidence
2.4. Statistical Analysis
3. Results
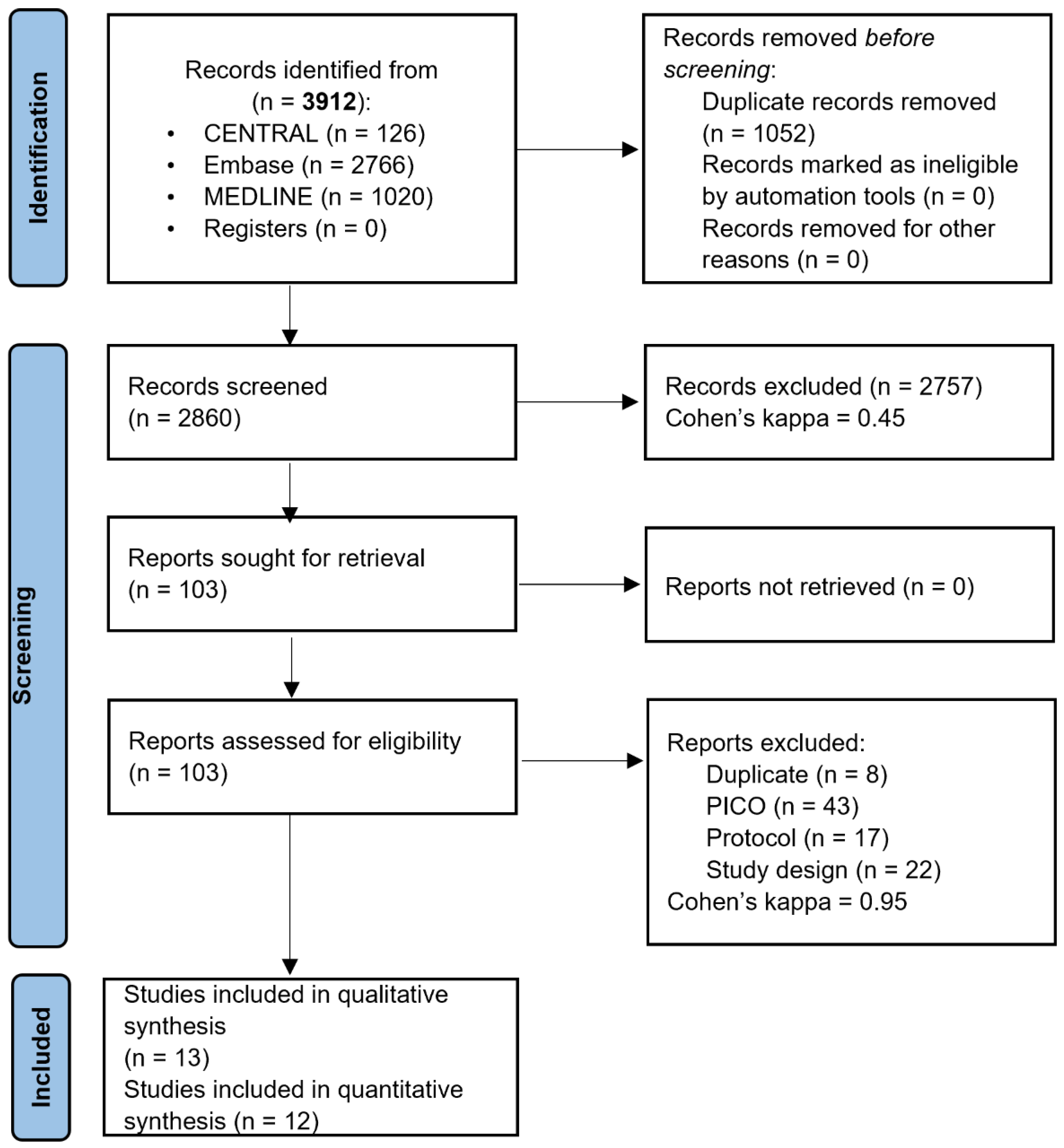
3.1. Systematic Search and Selection
3.2. Description of the Selected Studies
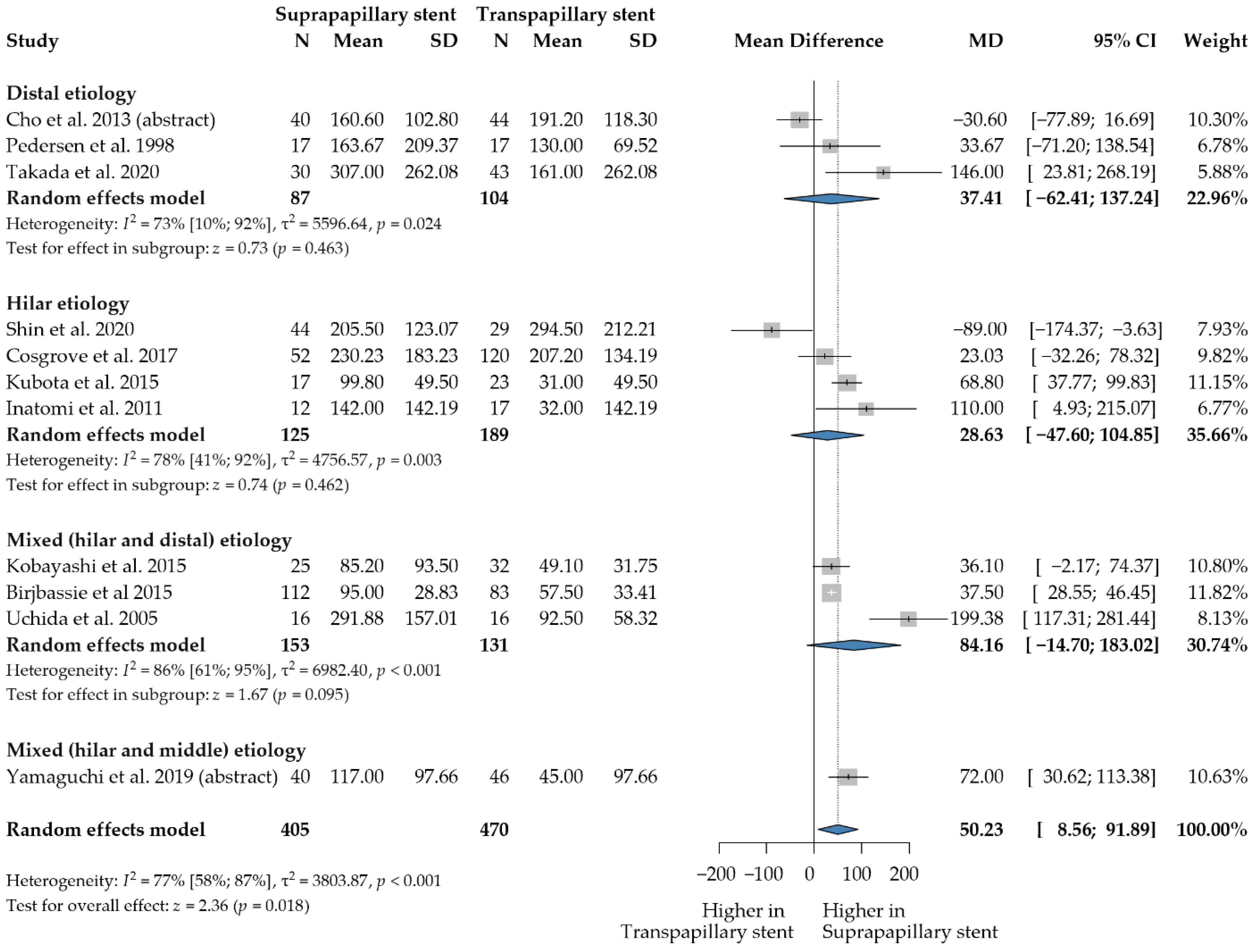
3.3. Stent Patency
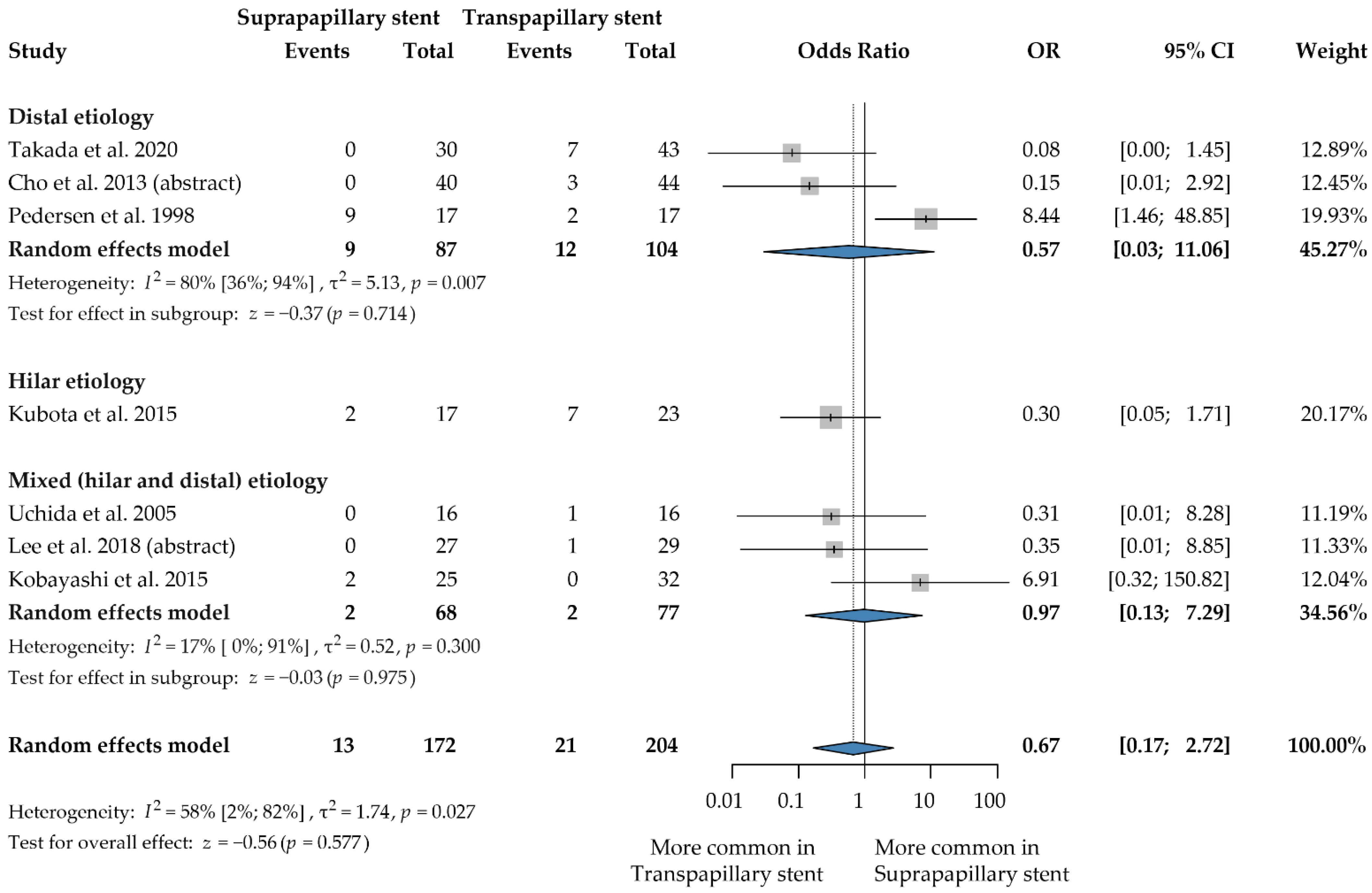
3.4. Stent Migration
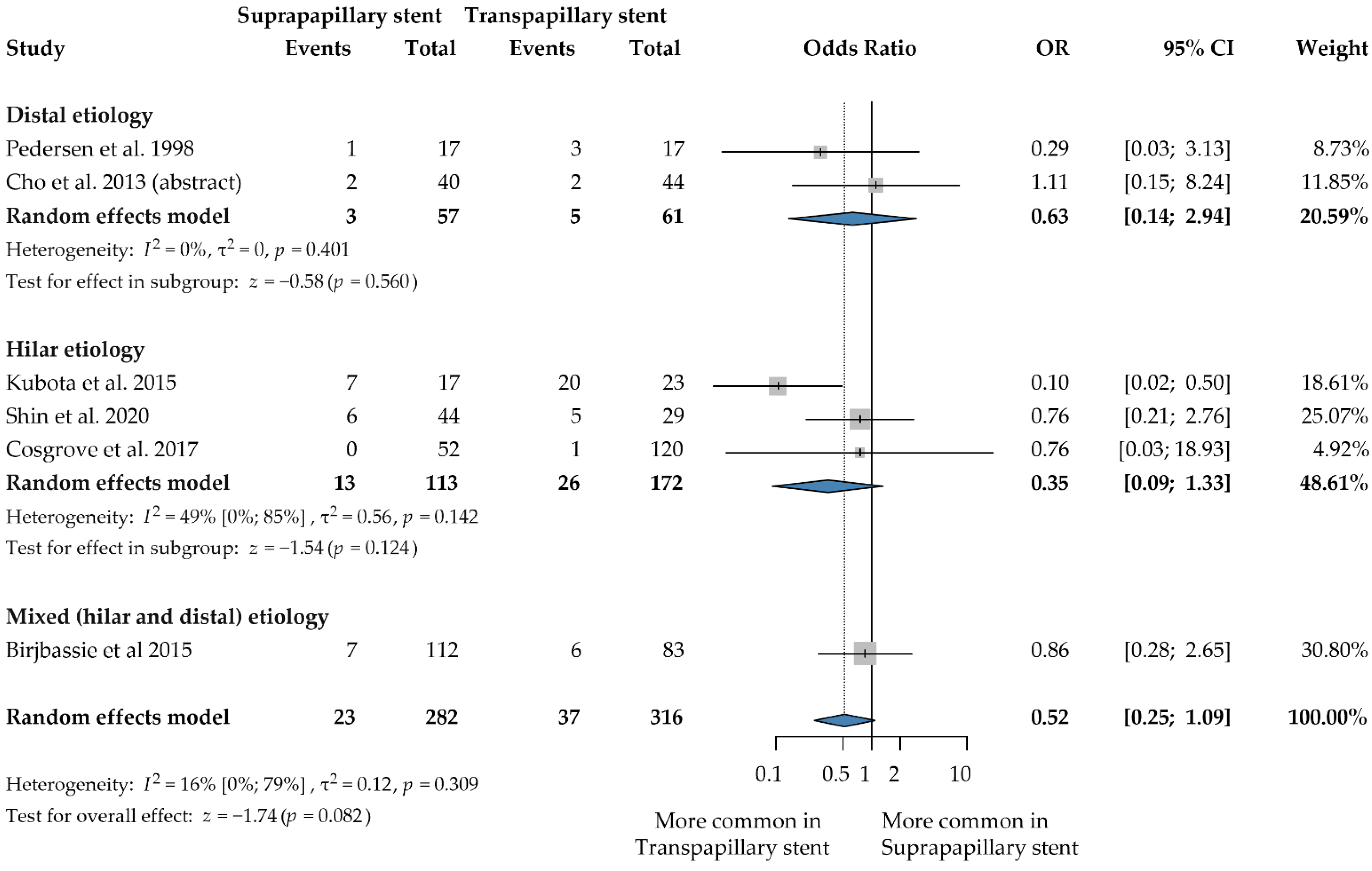
3.5. Cholangitis
3.6. Pancreatitis
3.7. Cholecystitis
3.8. Other Complications
3.9. Risk of Bias Assessment
3.10. Publication Bias
3.11. Certainty of Evidence
4. Discussion
4.1. Stent Patency
4.2. Stent Migration
4.3. Cholangitis
4.4. Pancreatitis
4.5. Strengths and Limitations
4.6. Implication for Practice
4.7. Implications for Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
Abbreviations
| CI | Confidence interval |
| ERCP | Endoscopic retrograde cholangiopancreatography |
| IQR | Interquartile ranges |
| OR | Odds ratio |
| RCT | Randomized controlled trial |
| SO | Sphincter of Oddi |
| SPS | Suprapapillary stent |
| SEMS | Self-expandable metallic stent |
| TPS | Transpapillary stent |
| WMD | Weighted mean difference |
References
- Khan, M.A.; Baron, T.H.; Kamal, F.; Ali, B.; Nollan, R.; Ismail, M.K.; Tombazzi, C.; Artifon, E.L.; Repici, A.; Khashab, M.A. Efficacy of self-expandable metal stents in management of benign biliary strictures and comparison with multiple plastic stents: A meta-analysis. Endoscopy 2017, 49, 682–694. [Google Scholar] [CrossRef] [PubMed]
- Almadi, M.A.; Barkun, A.; Martel, M. Plastic vs. Self-Expandable Metal Stents for Palliation in Malignant Biliary Obstruction: A Series of Meta-Analyses. Am. J. Gastroenterol. 2017, 112, 260–273. [Google Scholar] [CrossRef] [PubMed]
- Takada, R.; Ikezawa, K.; Kiyota, R.; Imai, T.; Abe, Y.; Fukutake, N.; Ashida, R.; Nawa, T.; Tabuchi, T.; Katayama, K.; et al. Self-expandable metallic stent placement above the papilla without endoscopic sphincterotomy in patients with distal malignant biliary obstruction. Endosc. Int. Open 2020, 8, e753–e760. [Google Scholar] [CrossRef] [PubMed]
- Kikuyama, M.; Shirane, N.; Kawaguchi, S.; Terada, S.; Mukai, T.; Sugimoto, K. New 14-mm diameter Niti-S biliary uncovered metal stent for unresectable distal biliary malignant obstruction. World J. Gastrointest. Endosc. 2018, 10, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Dowidar, N.; Kolmos, H.J.; Matzen, P. Experimental clogging of biliary endoprostheses. Role of bacteria, endoprosthesis material, and design. Scand. J. Gastroenterol. 1992, 27, 77–80. [Google Scholar] [CrossRef]
- Leung, J.W.; Del Favero, G.; Cotton, P.B. Endoscopic biliary prostheses: A comparison of materials. Gastrointest. Endosc. 1985, 31, 93–95. [Google Scholar] [CrossRef]
- van Berkel, A.M.; van Marle, J.; Groen, A.K.; Bruno, M.J. Mechanisms of biliary stent clogging: Confocal laser scanning and scanning electron microscopy. Endoscopy 2005, 37, 729–734. [Google Scholar] [CrossRef]
- Uchida, N.; Tsutsui, K.; Ezaki, T.; Fukuma, H.; Kamata, H.; Kobara, H.; Matsuoka, H.; Kinekawa, F.; Aritomo, Y.; Yokoyama, F.; et al. Estimation of the stent placement above the intact sphincter of Oddi against malignant bile duct obstruction. J. Gastroenterol. 2005, 40, 291–296. [Google Scholar] [CrossRef]
- Kuwatani, M.; Kawakubo, K.; Sakamoto, N. Possible reasons for the regrettable results of patency of an inside stent in endoscopic transpapillary biliary stenting. Dig. Endosc. 2021, 34, 334–344. [Google Scholar] [CrossRef]
- Jang, S.; Stevens, T.; Parsi, M.; Lopez, R.; Zuccaro, G.; Dumot, J.; Vargo, J.J. Association of covered metallic stents with cholecystitis and stent migration in malignant biliary stricture. Gastrointest. Endosc. 2018, 87, 1061–1070. [Google Scholar] [CrossRef]
- Mergener, K.; Baillie, J. Retrieval of distally migrated, impacted biliary endoprostheses using a novel guidewire/basket "lasso" technique. Gastrointest. Endosc. 1999, 50, 93–95. [Google Scholar] [CrossRef]
- Pedersen, F.M.; Lassen, A.T.; Schaffalitzky de Muckadell, O.B. Randomized trial of stent placed above and across the sphincter of Oddi in malignant bile duct obstruction. Gastrointest. Endosc. 1998, 48, 574–579. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.; Hernán, M.A.; Reeves, B.C.; Savović, J.; Berkman, N.D.; Viswanathan, M.; Henry, D.; Altman, D.G.; Ansari, M.T.; Boutron, I.; et al. ROBINS-I: A tool for assessing risk of bias in non-randomised studies of interventions. BMJ 2016, 355, i4919. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [Green Version]
- McGuinness, L.A.; Higgins, J.P.T. Risk-of-bias VISualization (robvis): An R package and Shiny web app for visualizing risk-of-bias assessments. Res. Synth. Methods 2020, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Schünemann, H.B.J.; Guyatt, G.; Oxman, A. (Eds.) GRADE Handbook for Grading Quality of Evidence and Strength of Recommendations; Updated October 2013; The GRADE Working Group: Philadelphia, PA, USA, 2013; Available online: guidelinedevelopment.org/handbook (accessed on 7 June 2022).
- GRADEpro GDT: GRADEpro Guideline Development Tool; Developed by Evidence Prime, Inc.; McMaster University: Hamilton, ON, Canada, 2020; Available online: gradepro.org (accessed on 7 June 2022).
- Higgins, J.P.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2; Cochrane: Rockville, MA, USA, 2021; Available online: www.training.cochrane.org/handbook (accessed on 15 December 2022).
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Viechtbauer, W. Bias and Efficiency of Meta-Analytic Variance Estimators in the Random-Effects Model. J. Educ. Behav. Stat. 2005, 30, 261–293. [Google Scholar] [CrossRef]
- Brijbassie, A. Transpapillary vs. intraductal fully covered selfexpanding metal stent placement for malignant and benign biliary disease: Does it make a difference? J. Interv. Gastroenterol. 2015, 5, 64. [Google Scholar] [CrossRef]
- Cosgrove, N.; Siddiqui, A.A.; Adler, D.G.; Shahid, H.; Sarkar, A.; Sharma, A.; Kowalski, T.E.; Loren, D.; Warndorf, M.; Chennat, J.; et al. A Comparison of Bilateral Side-by-Side Metal Stents Deployed Above and Across the Sphincter of Oddi in the Management of Malignant Hilar Biliary Obstruction. J. Clin. Gastroenterol. 2017, 51, 528–533. [Google Scholar] [CrossRef]
- Inatomi, O.; Bamba, S.; Shioya, M.; Mochizuki, Y.; Ban, H.; Tsujikawa, T.; Saito, Y.; Andoh, A.; Fujiyama, Y. Threaded biliary inside stents are a safe and effective therapeutic option in cases of malignant hilar obstruction. BMC Gastroenterol. 2013, 13, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kobayashi, N.; Watanabe, S.; Hosono, K.; Kubota, K.; Nakajima, A.; Kaneko, T.; Sugimori, K.; Tokuhisa, M.; Goto, A.; Mori, R.; et al. Endoscopic inside stent placement is suitable as a bridging treatment for preoperative biliary tract cancer. BMC Gastroenterol. 2015, 15, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kubota, K.; Hasegawa, S.; Iwasaki, A.; Sato, T.; Fujita, Y.; Hosono, K.; Nakajima, A.; Mori, R.; Matsuyama, R.; Endo, I. Stent placement above the sphincter of Oddi permits implementation of neoadjuvant chemotherapy in patients with initially unresectable Klatskin tumor. Endosc. Int. Open 2016, 4, E427–E433. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, J.; Park, J.S.; Jeong, S.; Lee, D.H. Comparison of the Clinical Outcomes of Suprapapillary and Transpapillary Stent Insertion in Unresectable Cholangiocarcinoma with Biliary Obstruction. Dig. Dis. Sci. 2020, 65, 1231–1238. [Google Scholar] [CrossRef] [PubMed]
- Cho, J.N.; Han, J.; Kim, H.G.; Shin, I.H.; Park, S.H.; Moon, J.H.; Kim, J.H.; Lee, D.H.; Maetani, I.; Maguchi, H.; et al. Prospective randomized trial comparing covered metal stent placed above and across the sphincter of oddi in malignant biliary obstruction. Gastrointest. Endosc. 2013, 77, AB139–AB140. [Google Scholar] [CrossRef]
- Lee, H.W.; Moon, J.H.; Choi, H.J.; Lee, Y.N.; Lee, T.H.; Choi, M.H.; Cha, S.W.; Cho, Y.D.; Park, S.H. Modified Fully Covered Self-Expandable Metal Stent Versus Plastic Stent For Preoperative Biliary Drainage In Patients With Resectable Malignant Biliary Obstruction. Endoscopy 2018, 50, 44–45. [Google Scholar] [CrossRef]
- Taniguchi, Y. Intraductal vs. transpapillary fully covered metal stent placement for malignant biliary strictures. Gastrointest. Endosc. 2020, 91, 949–956. [Google Scholar] [CrossRef]
- Yamaguchi, A.; Moriuchi, R.; Wada, K.; Tao, K.; Konishi, H.; Miura, R.; Tamaru, Y.; Kusunoki, R.; Kuwai, T.; Kouno, H.; et al. Intraductal Plastic Stent Placement is an Effective Therapy for Unresectable Malignant Hilar Biliary Obstruction. J. Gastroenterol. Hepatol. 2019, 34, 175. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Isayama, H.; Nakai, Y.; Kogure, H.; Yamamoto, N.; Koike, K. Biliary self-expandable metallic stent for unresectable malignant distal biliary obstruction: Which is better: Covered or uncovered? Dig. Endosc. 2013, 25 (Suppl. S2), 71–74. [Google Scholar] [CrossRef]
- Obermeier, A.; Würstle, S.; Tübel, J.; Stolte, P.; Feihl, S.; Lipovcic, N.; Lanzinger, S.; Mühlhofer, H.; Weber, A.; Schmid, R.M.; et al. Novel antimicrobial coatings based on polylactide for plastic biliary stents to prevent post-endoscopic retrograde cholangiography cholangitis. J. Antimicrob. Chemother. 2019, 74, 1911–1920. [Google Scholar] [CrossRef] [PubMed]
- Hamada, T.; Nakai, Y.; Isayama, H.; Koike, K. Antireflux metal stent for biliary obstruction: Any benefits? Dig. Endosc. 2021, 33, 310–320. [Google Scholar] [CrossRef] [PubMed]
- Knyrim, K.; Wagner, H.J.; Pausch, J.; Vakil, N. A prospective, randomized, controlled trial of metal stents for malignant obstruction of the common bile duct. Endoscopy 1993, 25, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Ridtitid, W.; Rerknimitr, R.; Janchai, A.; Kongkam, P.; Treeprasertsuk, S.; Kullavanijaya, P. Outcome of second interventions for occluded metallic stents in patients with malignant biliary obstruction. Surg. Endosc. 2010, 24, 2216–2220. [Google Scholar] [CrossRef] [PubMed]
- Matsushita, M.; Hajiro, K.; Takakuwa, H.; Nishio, A. Are biliary stents placed above the sphincter of oddi really ineffective? Gastrointest. Endosc. 2000, 51, 116–117. [Google Scholar] [CrossRef] [PubMed]
- Tringali, A.; Hassan, C.; Rota, M.; Rossi, M.; Mutignani, M.; Aabakken, L. Covered vs. uncovered self-expandable metal stents for malignant distal biliary strictures: A systematic review and meta-analysis. Endoscopy 2018, 50, 631–641. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, T.; Fujioka, S.; Yanagisawa, S.; Yanaga, K.; Kakutani, H.; Tajiri, H.; Urashima, M. Placement of a metallic stent across the main duodenal papilla may predispose to cholangitis. Gastrointest. Endosc. 2006, 63, 792–796. [Google Scholar] [CrossRef]
- Zhou, H.; Li, L.; Zhu, F.; Luo, S.-Z.; Cai, X.-B.; Wan, X.-J. Endoscopic sphincterotomy associated cholangitis in patients receiving proximal biliary self-expanding metal stents. Hepatobiliary Pancreat. Dis. Int. 2012, 11, 643–649. [Google Scholar] [CrossRef]
- Sofi, A.A.; Nawras, A.; Alaradi, O.H.; Alastal, Y.; Khan, M.A.; Lee, W.M. Does endoscopic sphincterotomy reduce the risk of post-endoscopic retrograde cholangiopancreatography pancreatitis after biliary stenting? A systematic review and meta-analysis. Dig. Endosc. 2016, 28, 394–404. [Google Scholar] [CrossRef]
- Coté, G.A.; Kumar, N.; Ansstas, M.; Edmundowicz, S.A.; Jonnalagadda, S.; Mullady, D.K.; Azar, R.R. Risk of post-ERCP pancreatitis with placement of self-expandable metallic stents. Gastrointest. Endosc. 2010, 72, 748–754. [Google Scholar] [CrossRef]
- Okano, N.; Igarashi, Y.; Kishimoto, Y.; Mimura, T.; Ito, K. Necessity for endoscopic sphincterotomy for biliary stenting in cases of malignant biliary obstruction. Dig. Endosc. 2013, 25 (Suppl. S2), 122–125. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year, Country, Number of Centers | Study Design | Time of Enrollment | N0 of Patients (Age, N0 of Females) | Indication(s) for Stent Placement | Exclusion Criteria | Stent Type (TPS vs. SPS) | EST (TPS, SPS) | Outcome(s) |
|---|---|---|---|---|---|---|---|---|
| Brijbassie et al. 2015 [2], USA, 1 center | Retrospective case series | 2006–2009 | 195 patients (mean age 67.1 ± 12.2 years, 75) | Benign and malignant biliary strictures | N/A | metal (FCSEMS) vs. metal (FCSEMS) | yes, partial | Stent patency, post-ERCP cholangitis |
| Cho et al. 2013 [3] (abstract), Japan, 6 centers | Prospective, randomized trial | 2010–2012 | 84 patients (mean age 72 ± 12.5, N/A) | Unresectable malignant biliary obstruction | Ampullary cancer, Klatskin tumor, combined intrahepatic bile duct cancer, hemobilia, previous history of biliary drainage | metal (CSEMS) vs. metal (CSEMS) | yes, no | Stent patency, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis, other procedure-related complications: bleeding or cholecystitis |
| Cosgrove et al. 2017 [4], USA, 3 centers | Retrospective cohort | 2007–2013 | 172 patients (mean age 66.5 ± 14.18, 66) | Unresectable malignant hilar biliary strictures of any etiology | Curative surgical resection | bilateral metal (SEMS) vs. bilateral metal (SEMS) | yes, based on the endoscopist decision (108, 5) | Stent patency, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis, other procedure-related complications: bleeding or perforation |
| Inatomi et al. 2011 [5], Japan, 1 center | Retrospective cohort | 2007–2011 | 42 patients (67.5 ± 12.2 years, 20) | Unresectable malignant hilar biliary obstruction | N/A | plastic + metal (uncovered) vs. plastic (threaded) | only in metal stents | Stent patency, stent migration, other procedure-related complications: bleeding or perforation |
| Kobayashi et al. 2015 [6], Japan, 1 center | Retrospective cohort | 2006–2011 | 57 patients (median age 71 (56–86), 12) | Primary biliary duct cancer | Percutaneous transhepatic biliary, pancreatic cancer, ampullary cancer, and intra hepatic cancer | plastic vs. plastic | yes (3,3) | Stent patency, stent occlusion, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis, other procedure-related complications: bleeding, biliary and pancreatic fistula, or liver abscess |
| Kubota et al. 2015 [7], Japan, 1 center | Retrospective cohort | 2012–2015 | 40 patients (mean age 70, 13) | Primary biliary duct cancer | Gallbladder cancer, intrahepatic cholangiocarcinoma, and biliary cancer arising from pancreatic head lesions and metastatic Klatskin tumors | plastic vs. threaded plastic | yes (multiple TPS) | Stent patency, stent occlusion, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis |
| Lee et al. 2018 (abstract) [8], N/A | Retrospective cohort | 2015–2017 | 56 (N/A, N/A) | obstructive jaundice due to resectable extrahepatic malignant biliary obstruction | N/A | plastic vs. metal (FCSEMS) | N/A | Stent occlusion, stent migration |
| Pedersen et al. 1998 [9], Denmark, 1 center | Prospective, randomized trial | 1992–1996 | 34 patients (median age 73.5 (IQR: 67–80), 21) | Malignant biliary obstruction | Curable lesion was suspected or if liver metastases were present at the time of the ERCP | plastic vs. plastic | No | Stent patency, stent occlusion, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis, other procedure-related complications: bleeding, cholecystitis, or perforation |
| Shin et al. 2020 [10], Korea and Japan, 1 center | Retrospective cohort | 2005–2015 | 73 patients (median age 75 (49–90), 36) | Hilar cholangiocarcinoma | Previous history of SEMS treatment, CCC involving the duodenum, prior history of gastrointestinal surgery, failure of endoscopic SEMS insertion, or SEMS insertion by a modality other than endoscopy | metal (SEMS) vs. metal (SEMS) | Yes (all) | Stent patency, stent occlusion, post-ERCP cholangitis, post-ERCP pancreatitis, procedure-related complications: cholecystitis |
| Takada et al. 2020 [11], Japan, 1 center | Retrospective cohort | 2014–2016 | 73 patients (median age 69 (52–86), 38) | Unresectable distal malignant biliary obstruction | Duodenal stents or they underwent concurrent placement of plastic stents and SEMS | metal (SEMS: covered+ uncovered) vs. metal (SEMS: covered + uncovered) | yes (12,10) | Stent patency, stent occlusion, stent migration, other procedure-related complications: cholecystitis, liver abscess, or liver hematoma |
| Taniguchi et al. 2020 (abstract) [12], Japan, 1 center | Retrospective cohort | 2016–2019 | 96 patients (N/A, N/A) | Nonhilar, extrahepatic, malignant biliary stricture | N/A | metal (covered) vs. metal (covered) | N/A | Stent patency, stent occlusion |
| Uchida et al. 2005 [13], Japan, 1 center | Prospective, non-randomized | 1999–2003 | 32 patients (mean age 75 (56–92), 15) | Unresectable and previously untreated malignant biliary obstruction | Lesions involved the bifurcation of the common hepatic bile duct; distance from the stenosis to the sphincter of Oddi was less than 15 mm on X-ray examination | plastic vs. plastic | No | Stent patency, stent occlusion, stent migration, post-ERCP pancreatitis, post-ERCP cholangitis, other procedure-related complications: bleeding, cholecystitis, or perforation |
| Yamaguchi et al. 2019 (abstract) [14], N/A | Retrospective cohort | 2008–2018 | 74 patients (N/A, N/A) | Unresectable malignant hilar or middle bile duct obstruction | N/A | plastic vs. plastic | N/A | Stent patency, stent migration, post-ERCP cholangitis, post-ERCP pancreatitis, other procedure-related complications: bleeding or cholecystitis |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kovács, N.; Pécsi, D.; Sipos, Z.; Farkas, N.; Földi, M.; Hegyi, P.; Bajor, J.; Erőss, B.; Márta, K.; Mikó, A.; et al. Suprapapillary Biliary Stents Have Longer Patency Times than Transpapillary Stents—A Systematic Review and Meta-Analysis. J. Clin. Med. 2023, 12, 898. https://doi.org/10.3390/jcm12030898
Kovács N, Pécsi D, Sipos Z, Farkas N, Földi M, Hegyi P, Bajor J, Erőss B, Márta K, Mikó A, et al. Suprapapillary Biliary Stents Have Longer Patency Times than Transpapillary Stents—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2023; 12(3):898. https://doi.org/10.3390/jcm12030898
Chicago/Turabian StyleKovács, Norbert, Dániel Pécsi, Zoltán Sipos, Nelli Farkas, Mária Földi, Péter Hegyi, Judit Bajor, Bálint Erőss, Katalin Márta, Alexandra Mikó, and et al. 2023. "Suprapapillary Biliary Stents Have Longer Patency Times than Transpapillary Stents—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 12, no. 3: 898. https://doi.org/10.3390/jcm12030898