
Building Blocks for Deep Phenotyping in Infancy: A Use Case Comparing Spontaneous Neuromotor Functions in Prader-Willi Syndrome and Cerebral Palsy

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Procedure
2.3. Statistics
3. Results
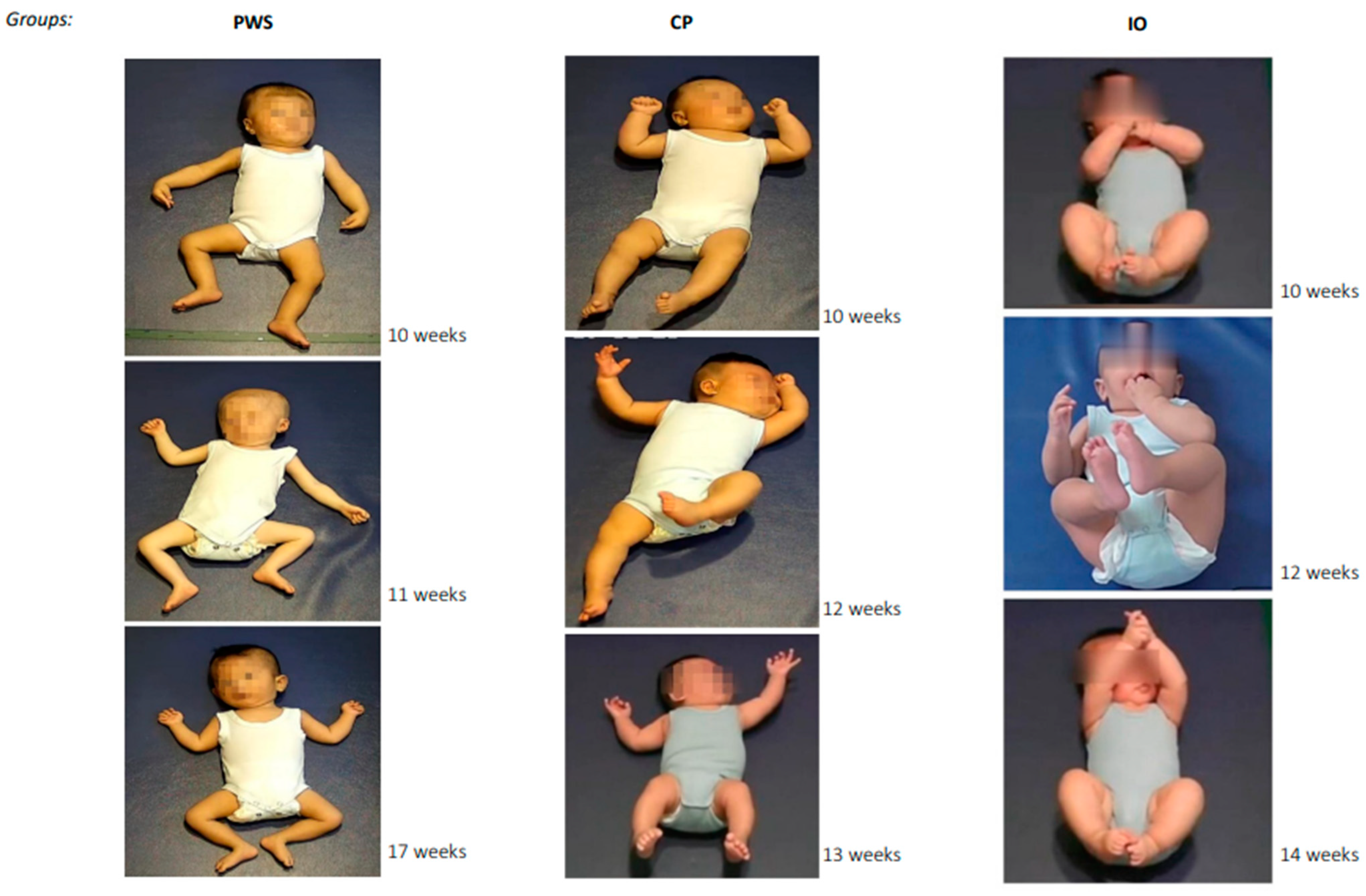
3.1. Spontaneous Motor Patterns of Infants with PWS
3.2. Spontaneous Motor Patterns of Infants with PWS Compared with Infants with CP and Infants with Inconspicuous Outcomes (IOs)
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Prechtl, H.F.R.; Einspieler, C.; Cioni, G.; Bos, A.F.; Ferrari, F.; Sontheimer, D. An early marker for neurological deficits after perinatal brain lesions. Lancet 1997, 349, 1361–1363. [Google Scholar] [CrossRef] [PubMed]
- Marschik, P.B.; Soloveichick, M.; Windpassinger, C.; Einspieler, C. General movements in genetic disorders: A first look into Cornelia de Lange syndrome. Dev. Neurorehabil. 2015, 18, 280–282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Herrero, D.; Einspieler, C.; Panvequio Aizawa, C.Y.; Mutlu, A.; Yang, H.; Nogolova, A.; Pansy, J.; Nielsen-Saines, K.; Marschik, P.B. The motor repertoire in 3- to 5-month old infants with Down syndrome. Res. Dev. Disabil. 2017, 67, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Utsch, F.; Brasil, P.; Panvequio Aizawa, C.Y.; Peyton, C.; Hydee Hasue, R.; Francoso Genovesi, F.; Damasceno, L.; Moreira, M.E.; Adachi, K.; et al. Association of infants exposed to prenatal zika virus infection with their clinical, neurologic, and developmental status evaluated via the general movement assessment tool. JAMA Netw. Open 2019, 2, e187235. [Google Scholar] [CrossRef] [Green Version]
- Palchik, A.B.; Einspieler, C.; Evstafeyeva, I.V.; Talisa, V.B.; Marschik, P.B. Intra-uterine exposure to maternal opiate abuse and HIV: The impact on the developing nervous system. Early Hum. Dev. 2013, 89, 229–235. [Google Scholar] [CrossRef]
- Silva, N.; Zhang, D.; Kulvicius, T.; Gail, A.; Barreiros, C.; Lindstaedt, S.; Kraft, M.; Bölte, S.; Poustka, L.; Nielsen-Saines, K.; et al. The future of general movement assessment: The role of computer vision and machine learning-a scoping review. Res. Dev. Disabil. 2021, 110, 103854. [Google Scholar] [CrossRef]
- Einspieler, C.; Peharz, R.; Marschik, P.B. Fidgety movements-tiny in appearance, but huge in impact. J. Pediatr. 2016, 92, 64–70. [Google Scholar] [CrossRef] [Green Version]
- Westermann, G.; Mareschal, D.; Johnson, M.H.; Sirois, S.; Spratling, M.W.; Thomas, M.S.C. Neuroconstructivism. Dev. Sci. 2007, 10, 75–83. [Google Scholar] [CrossRef]
- Sur, M.; Rubenstein, J.L.R. Patterning and plasticity of the cerebral cortex. Science 2005, 310, 805–810. [Google Scholar] [CrossRef] [Green Version]
- D’Souza, D.; Karmiloff-Smith, A. When modularization fails to occur: A developmental perspective. Cogn. Neuropsychol. 2011, 28, 276–287. [Google Scholar] [CrossRef]
- Einspieler, C.; Bos, A.F.; Libertus, M.E.; Marschik, P.B. The general movement assessment helps us to identify preterm infants at risk for cognitive dysfunction. Front. Psychol. 2016, 7, 406. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hitzert, M.M.; Roze, E.; Van Braeckel, K.N.; Bos, A.F. Motor development in 3-month-old healthy term-born infants is associated with cognitive and behavioural outcomes at early school age. Dev. Med. Child Neurol. 2014, 56, 869–876. [Google Scholar] [CrossRef] [PubMed]
- Salavati, S.; Bos, A.F.; Doyle, L.W.; Anderson, P.J.; Spittle, A.J. Very preterm early motor repertoire and neurodevelopmental outcomes at 8 years. Pediatrics 2021, 148, e2020049572. [Google Scholar] [CrossRef] [PubMed]
- Salavati, S.; Einspieler, C.; Vagelli, G.; Zhang, D.; Pansy, J.; Burgerhof, J.G.M.; Marschik, P.B.; Bos, A.F. The association between the early motor repertoire and language development in term children born after normal pregnancy. Early Hum. Dev. 2017, 111, 30–35. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Einspieler, C.; Marschik, P.B.; Prechtl, H.F.R. Human motor behavior. Z. Für. Psychol. J. Psychol. 2008, 216, 147–153. [Google Scholar] [CrossRef]
- Einspieler, C.; Prechtl, H.; Bos, A.; Ferrari, F.; Cioni, G. Prechtl’s Method on the Qualitative Assessment of General Movements in Preterm, Term and Young Infants; Mac Keith Press: London, UK, 2004. [Google Scholar]
- Einspieler, C.; Bos, A.F.; Krieber-Tomantschger, M.; Alvarado, E.; Barbosa, V.M.; Bertoncelli, N.; Burger, M.; Chorna, O.; Del Secco, S.; DeRegnier, R.A.; et al. Cerebral palsy: Early markers of clinical phenotype and functional outcome. J. Clin. Med. 2019, 8, 1616. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pansy, J.; Barones, C.; Urlesberger, B.; Pokorny, F.B.; Bartl-Pokorny, K.D.; Verheyen, S.; Marschik, P.B.; Einspieler, C. Early motor and pre-linguistic verbal development in Prader-Willi syndrome-A case report. Res. Dev. Disabil. 2019, 88, 16–21. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.B.; Schwartz, S.; Miller, J.L.; Driscoll, D.J. Prader-Willi syndrome. Genet. Med. 2012, 14, 10–26. [Google Scholar] [CrossRef] [Green Version]
- Whittington, J.; Holland, A. Neurobehavioral phenotype in Prader-Willi syndrome. Am. J. Med. Genet. C Semin. Med. Genet. 2010, 154, 438–447. [Google Scholar] [CrossRef]
- Wang, J.; Shen, X.; Yang, H.; Shi, W.; Zhu, X.; Gao, H.; Yin, H.; Meng, F.; Wu, Y. Inter- and intra-observer reliability of the "Assessment of Motor Repertoire- 3 to 5 Months" based on video recordings of infants with Prader-Willi syndrome. BMC Pediatr. 2022, 22, 150. [Google Scholar] [CrossRef]
- Irshad, M.T.; Nisar, M.A.; Gouverneur, P.; Rapp, M.; Grzegorzek, M. AI approaches towards Prechtl’s assessment of general movements: A systematic literature review. Sensors 2020, 20, 5321. [Google Scholar] [CrossRef]
- Reich, S.; Zhang, D.; Kulvicius, T.; Bölte, S.; Nielsen-Saines, K.; Pokorny, F.B.; Peharz, R.; Poustka, L.; Wörgötter, F.; Einspieler, C.; et al. Novel AI driven approach to classify infant motor functions. Sci. Rep. 2021, 11, 9888. [Google Scholar] [CrossRef] [PubMed]
- Groos, D.; Adde, L.; Aubert, S.; Boswell, L.; de Regnier, R.A.; Fjørtoft, T.; Gaebler-Spira, D.; Haukeland, A.; Loennecken, M.; Msall, M.; et al. Development and validation of a deep learning method to predict cerebral palsy from spontaneous movements in infants at high risk. JAMA Netw. Open 2022, 5, e2221325. [Google Scholar] [CrossRef] [PubMed]
- Marschik, P.B.; Kulvicius, T.; Flügge, S.; Widmann, C.; Nielsen-Saines, K.; Schulte-Rüther, M.; Hüning, B.; Bölte, S.; Poustka, L.; Sigafoos, J.; et al. Open video data sharing in developmental and behavioural science. arXiv 2022, arXiv:2207.11020. [Google Scholar] [CrossRef]
- Kulvicius, T.; Zhang, D.; Nielsen-Saines, K.; Bölte, S.; Kraft, M.; Einspieler, C.; Poustka, L.; Wörgötter, F.; Marschik, P.B. Infant movement classification through pressure distribution analysis-added value for research and clinical implementation. arXiv 2022, arXiv:2208.00884. [Google Scholar]
- Crowle, C.; Jackman, M.; Morgan, C. The general movements motor optimality score in high-risk infants: A systematic scoping review. Pediatr. Phys. Ther. 2023, 35, 2–26. [Google Scholar] [CrossRef]
- Butler, M.G.; Miller, J.L.; Forster, J.L. Prader-Willi syndrome-clinical genetics, diagnosis and treatment approaches: An update. Curr. Pediatr. Rev. 2019, 15, 207–244. [Google Scholar] [CrossRef]
- Tomantschger, I.; Herrero, D.; Einspieler, C.; Hamamura, C.; Voos, M.C.; Marschik, P.B. The general movement assessment in non-European low- and middle-income countries. Rev. Saude Publica 2018, 52, 6. [Google Scholar] [CrossRef]
- Kaler, J.; Hussain, A.; Patel, S.; Majhi, S. Neuromuscular junction disorders and floppy infant syndrome: A comprehensive review. Cureus 2020, 12, e6922. [Google Scholar] [CrossRef]
- Sparks, S.E. Neonatal hypotonia. Clin. Perinatol. 2015, 42, 363–371. [Google Scholar] [CrossRef]
- Marschik, P.B.; Pokorny, F.B.; Peharz, R.; Zhang, D.; O’Muircheartaigh, J.; Roeyers, H.; Bölte, S.; Spittle, A.J.; Urlesberger, B.; Schuller, B.; et al. A novel way to measure and predict development: A heuristic approach to facilitate the early detection of neurodevelopmental disorders. Curr. Neurol. Neurosci. Rep. 2017, 17, 43. [Google Scholar] [CrossRef] [PubMed]
- Einspieler, C.; Prayer, D.; Marschik, P.B. Fetal movements: The origin of human behaviour. Dev. Med. Child Neurol. 2021, 63, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Lord, C.; Brugha, T.S.; Charman, T.; Cusack, J.; Dumas, G.; Frazier, T.; Jones, E.J.H.; Jones, R.M.; Pickles, A.; State, M.W.; et al. Autism spectrum disorder. Nat. Rev. Dis. Primers 2020, 6, 5. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variable | Mean ± SD; N (%); or Median and Interquartile (Range) | p-Values a | |||
|---|---|---|---|---|---|
| PWS | CP | IOs | PWS vs. CP | PWS vs. IOs | |
| Maternal Age | 34.2 y ± 4.4 | 29.9 y ± 3.8 | 33.9 y ± 3.2 | 0.01 | 0.87 |
| Paternal Age | 31.5 y ± 5.2 | 28.2 y ± 3.3 | 33.1 y ± 2.9 | 0.05 | 0.33 |
| Male Gender | 14 (77.8%) | 11 (61.1%) | 13 (72.2%) | n.a. | n.a. |
| Parity | Median = 1; P25 = 1; P75 = 2 | Median = 1; P25 = 1; P75 = 2 | Median = 1; P25 = 1; P75 = 2 | n.a. | n.a. |
| (1–3) | (1–2) | (1–3) | |||
| Preterm Birth | 3 (16.7%) | 3 (16.7%) | 3 (16.7%) | n.a. | n.a. |
| Caesarean Section | 11 (61.1%) | 7 (38.9%) | 4 (22.2%) | n.a. | n.a. |
| Birth Weight | 2698.7 ± 448.1 | 3110.8 ± 606.8 | 3061.39 ± 765.6 | 0.03 | 0.12 |
| PWS | CP | IOs | p-Values a | |
|---|---|---|---|---|
| Recording age | ||||
| 9–12 weeks | 7 | 7 | 7 | |
| 13–16 weeks | 6 | 6 | 6 | n.a. |
| 17–20 weeks | 5 | 5 | 5 | |
| MOS | Median = 6 | Median = 7 | Median = 24 | PWS vs. CP: |
| P25 = 6, P75 = 7 | P25 = 6, P75 = 9 | P25 = 24, P75 = 26 | p > 0.05 | |
| Range: 6–18 | Range: 6–9 | Range: 21–28 | PWS vs. N: p < 0.01 | |
| Fidgety movements | ||||
| Normal | 1 | 0 | 18 | PWS vs. CP: |
| Abnormal | 1 | 0 | 0 | p > 0.05 |
| Absent | 16 | 18 | 0 | PWS vs. N: p < 0.01 |
| Other Movements | ||||
| N > A | 2 | 5 | 18 | PWS vs. CP: |
| N = A | 2 | 6 | 0 | p > 0.05 |
| N < A | 14 | 7 | 0 | PWS vs. N: p < 0.01 |
| Age-adequate Repertoire | ||||
| Present | 0 | 0 | 4 | PWS vs. CP: |
| Reduced | 1 | 0 | 9 | p > 0.05 |
| Absent | 17 | 18 | 5 | PWS vs. N: p < 0.01 |
| Posture | ||||
| N > A | 0 | 0 | 15 | PWS vs. CP: |
| N = A | 2 | 0 | 1 | p > 0.05 |
| N < A | 16 | 18 | 2 | PWS vs. N: p < 0.01 |
| Movement character | ||||
| Smooth, fluent | 0 | 0 | 6 | |
| Abnormal, not CS | 18 | 18 | 12 | PWS vs. N: |
| CS | 0 | 0 | 0 | p > 0.05 |
| Subscale | Group | Item on MOS-R | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Movement Pattern | Wiggling-Oscillating | Smiles | Mouth Movements | Tongue Movements a | Side-to-Side Movements of the Head | Hand-to-Mouth Contact | Foot-to-foot Contact | Leg Lift | Visual Exploration | Almost No Leg Movements a | ||
| N | IOs | 6 | 5 | 12 | 13 | 5 | 9 | 12 | 11 | |||
| PWS | 1 | 1 | 3 | 1 | 1 | 2 | 2 | |||||
| CP | 2 | 4 | 8 | 3 | 2 | 2 | 7 | |||||
| A | IOs | 1 | 2 | |||||||||
| PWS | 1 | 3 | 1 | 4 | 2 | 1 | 1 | 3 | 9 | |||
| CP | 3 | 9 | 12 | 6 | ||||||||
| Postural Pattern | Head centred | Body symmetry | Asymmetric tonic neck | Flat posture a | Variability of finger postures | Predominant fisting a | Hyperextension of neck a | Hyperextension of trunk a | Extended arms a | Extended legs a | ||
| N | IOs | 13 | 12 | 18 | 16 | |||||||
| PWS | 3 | 2 | 18 | 1 | ||||||||
| CP | 6 | 12 | ||||||||||
| A | IOs | 5 | 6 | |||||||||
| PWS | 15 | 16 | 13 | 17 | 1 | 2 | 3 | 5 | ||||
| CP | 12 | 18 | 6 | 2 | 18 | 5 | 14 | 8 | 7 | 3 | ||
| Movement Character | Smooth and fluent | Monotonous a | Jerky a | Stiff a | Predominantly slow a | |||||||
| - | IOs | 6 | 7 | 7 | ||||||||
| PWS | 18 | 5 | 1 | 11 | ||||||||
| CP | 17 | 6 | 5 | |||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marschik-Zhang, D.; Wang, J.; Shen, X.; Zhu, X.; Gao, H.; Yang, H.; Marschik, P.B. Building Blocks for Deep Phenotyping in Infancy: A Use Case Comparing Spontaneous Neuromotor Functions in Prader-Willi Syndrome and Cerebral Palsy. J. Clin. Med. 2023, 12, 784. https://doi.org/10.3390/jcm12030784
Marschik-Zhang D, Wang J, Shen X, Zhu X, Gao H, Yang H, Marschik PB. Building Blocks for Deep Phenotyping in Infancy: A Use Case Comparing Spontaneous Neuromotor Functions in Prader-Willi Syndrome and Cerebral Palsy. Journal of Clinical Medicine. 2023; 12(3):784. https://doi.org/10.3390/jcm12030784
Chicago/Turabian StyleMarschik-Zhang, Dajie, Jun Wang, Xiushu Shen, Xiaoyun Zhu, Herong Gao, Hong Yang, and Peter B. Marschik. 2023. "Building Blocks for Deep Phenotyping in Infancy: A Use Case Comparing Spontaneous Neuromotor Functions in Prader-Willi Syndrome and Cerebral Palsy" Journal of Clinical Medicine 12, no. 3: 784. https://doi.org/10.3390/jcm12030784