
REVersal of nEuromusculAr bLocking Agents in Patients Undergoing General Anaesthesia (REVEAL Study)

 , , , , ,
, , , , ,
Abstract
:1. Introduction
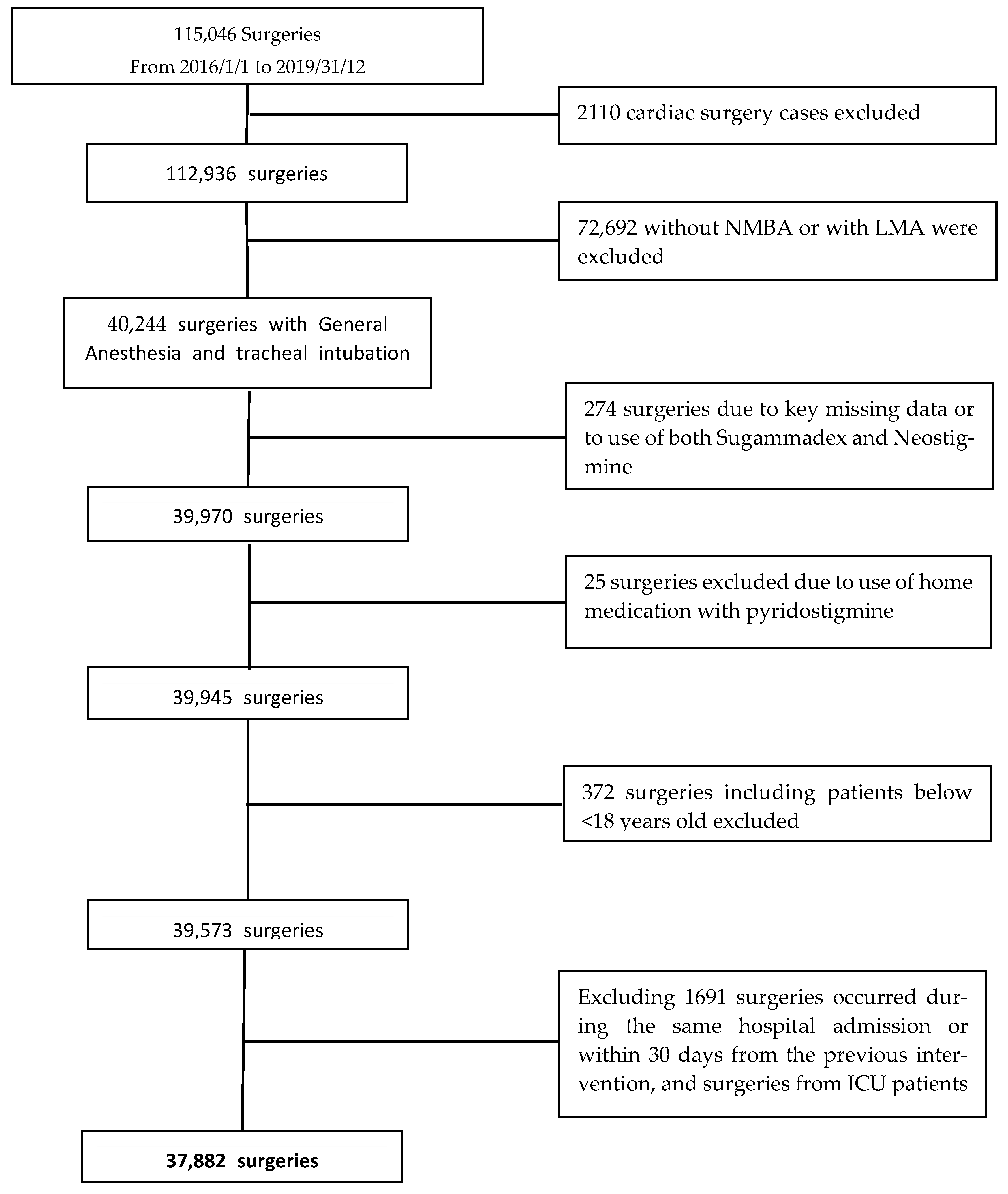
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goerig, M. Pioneering Curare in Anesthesia. Anesthesiology 1990, 73, 189–190. [Google Scholar] [CrossRef]
- Jarcho, L.W.; Berman, B.; Eyzaguirre, C.; Lilienthal, J.L. Curarization of Denervated Muscle. Ann. N. Y. Acad. Sci. 1951, 54, 337–346. [Google Scholar] [CrossRef]
- Aytac, I.; Postaci, A.; Aytac, B.; Sacan, O.; Alay, G.H.; Celik, B.; Kahveci, K.; Dikmen, B. Survey of Postoperative Residual Curarization, Acute Respiratory Events and Approach of Anesthesiologists. Braz. J. Anesthesiol. 2016, 66, 55–62. [Google Scholar] [CrossRef] [Green Version]
- Carron, M.; Baratto, F.; Zarantonello, F.; Ori, C. Sugammadex for Reversal of Neuromuscular Blockade: A Retrospective Analysis of Clinical Outcomes and Cost-Effectiveness in a Single Center. Clinicoecon Outcomes Res. 2016, 8, 43–52. [Google Scholar] [CrossRef] [Green Version]
- Gratarola, A.; Piccioni, F.; Della Casa, P.; Murabito, P.; Langiano, N.; Guadagnin, G.M.; Della Rocca, G. Miorisoluzione, Monitoraggio Neuromuscolare E Antagonismo. In Buone Pratiche Cliniche; SIAARTI (Società Italiana Anestesia, Analgesia, Rianimazione e Terapia Intensiva): Rome, Italy, 2018. [Google Scholar]
- Plaud, B.; Baillard, C.; Bourgain, J.-L.; Bouroche, G.; Desplanque, L.; Devys, J.-M.; Fletcher, D.; Fuchs-Buder, T.; Lebuffe, G.; Meistelman, C.; et al. Guidelines on Muscle Relaxants and Reversal in Anaesthesia. Anaesth. Crit. Care Pain Med. 2020, 39, 125–142. [Google Scholar] [CrossRef]
- Della Rocca, G.; Iannuccelli, F.; Pompei, L.; Pietropaoli, P.; Reale, C.; Di Marco, P. Neuromuscular Block in Italy: A Survey of Current Management. Minerva Anestesiol 2012, 78, 767–773. [Google Scholar]
- Kheterpal, S. Clinical Research Using an Information System: The Multicenter Perioperative Outcomes Group. Anesthesiol. Clin. 2011, 29, 377–388. [Google Scholar] [CrossRef]
- Ercole, A.; Brinck, V.; George, P.; Hicks, R.; Huijben, J.; Jarrett, M.; Vassar, M.; Wilson, L.; DAQCORD Collaborators. Guidelines for Data Acquisition, Quality and Curation for Observational Research Designs (DAQCORD). J. Clin. Transl. Sci. 2020, 4, 354. [Google Scholar] [CrossRef] [Green Version]
- Tacconelli, E.; Cataldo, M.A.; Paul, M.; Leibovici, L.; Kluytmans, J.; Schröder, W.; Foschi, F.; De Angelis, G.; De Waure, C.; Cadeddu, C.; et al. STROBE-AMS: Recommendations to Optimise Reporting of Epidemiological Studies on Antimicrobial Resistance and Informing Improvement in Antimicrobial Stewardship. BMJ Open 2016, 6, e010134. [Google Scholar] [CrossRef]
- Popat, M.; Mitchell, V.; Dravid, R.; Patel, A.; Swampillai, C.; Higgs, A. Difficult Airway Society Guidelines for the Management of Tracheal Extubation. Anaesthesia 2012, 67, 318–340. [Google Scholar] [CrossRef]
- Eldawlatly, A.; El-Tahan, M. A Survey of the Current Use of Neuromuscular Blocking Drugs among the Middle Eastern Anesthesiologists. Saudi J. Anaesth 2013, 7, 146–150. [Google Scholar] [CrossRef]
- Nemes, R.; Renew, J.R. Clinical Practice Guideline for the Management of Neuromuscular Blockade: What Are the Recommendations in the USA and Other Countries? Curr. Anesthesiol. Rep. 2020, 10, 90–98. [Google Scholar] [CrossRef] [Green Version]
- Honing, G.; Martini, C.H.; Bom, A.; van Velzen, M.; Niesters, M.; Aarts, L.; Dahan, A.; Boon, M. Safety of Sugammadex for Reversal of Neuromuscular Block. Expert Opin. Drug Saf. 2019, 18, 883–891. [Google Scholar] [CrossRef]
- Hristovska, A.-M.; Duch, P.; Allingstrup, M.; Afshari, A. Efficacy and Safety of Sugammadex versus Neostigmine in Reversing Neuromuscular Blockade in Adults. Cochrane Database Syst. Rev. 2017, 8, CD012763. [Google Scholar] [CrossRef]
- Martini, C.H.; Honing, G.H.M.; Bash, L.D.; Olofsen, E.; Niesters, M.; van Velzen, M.; Dahan, A.; Boon, M. The Use of Muscle Relaxants and Reversal Agents in a Setting Without Cost Restrictions: Experience from a Tertiary Academic Hospital in the Netherlands. Ther. Clin. Risk Manag. 2022, 18, 379–390. [Google Scholar] [CrossRef]
- Bash, L.D.; Turzhitsky, V.; Black, W.; Urman, R.D. Neuromuscular Blockade and Reversal Agent Practice Variability in the US Inpatient Surgical Settings. Adv. Ther. 2021, 38, 4736–4755. [Google Scholar] [CrossRef]
- Chambers, D.; Paulden, M.; Paton, F.; Heirs, M.; Duffy, S.; Craig, D.; Hunter, J.; Wilson, J.; Sculpher, M.; Woolacott, N. Sugammadex for the Reversal of Muscle Relaxation in General Anaesthesia: A Systematic Review and Economic Assessment. Health Technol. Assess (Rockv.) 2010, 14, 1–211. [Google Scholar] [CrossRef] [Green Version]
- Kajiura, A.; Nagata, O.; Takizawa, Y.; Nakatomi, T.; Kodera, S.; Murayama, T. A Large Individual Variation in Both the Infusion Rate and the Blood Concentration of Rocuronium Necessary for Obtain Adequate Surgical Muscle Relaxation during Total Intravenous Anesthesia with Propofol and Remifentanil. J. Anesth. 2015, 29, 9–14. [Google Scholar] [CrossRef]
- Wastila, W.B.; Maehr, R.B.; Turner, G.L.; Hill, D.A.; Savarese, J.J. Comparative Pharmacology of Cisatracurium (51W89), Atracurium, and Five Isomers in Cats. Anesthesiology 1996, 85, 169–177. [Google Scholar] [CrossRef]
- Van Gestel, L.; Cammu, G. Is the Effect of Sugammadex Always Rapid in Onset? Acta Anaesthesiol. Belg. 2013, 64, 41–47. [Google Scholar]
- Carron, M.; Veronese, S.; Foletto, M.; Ori, C. Sugammadex Allows Fast-Track Bariatric Surgery. Obes. Surg. 2013, 23, 1558–1563. [Google Scholar] [CrossRef]
- Goshtasbi, K.; Birkenbeuel, J.L.; Abiri, A.; Lehrich, B.M.; Kuan, E.C. The Association of Frailty, Age, and ASA Classification with Postoperative Outcomes in Endoscopic Sinus Surgery. Int. Forum Allergy Rhinol. 2021, 11, 1596–1598. [Google Scholar] [CrossRef]
- Fitz-Henry, J. The ASA Classification and Peri-Operative Risk. Ann. R. Coll. Surg. Engl. 2011, 93, 185–187. [Google Scholar] [CrossRef] [Green Version]
- McLean, D.J.; Diaz-Gil, D.; Farhan, H.N.; Ladha, K.S.; Kurth, T.; Eikermann, M. Dose-Dependent Association between Intermediate-Acting Neuromuscular-Blocking Agents and Postoperative Respiratory Complications. Anesthesiology 2015, 122, 1201–1213. [Google Scholar] [CrossRef]
- Becerra-Bolaños, A.; Muiño-Palomar, V.; Cabrera-Doreste, S.; Rodríguez-Pérez, A. Sugammadex in systemic mastocytosis. Anaesthesiologie 2022, 71 (Suppl. S2), 165–170. [Google Scholar] [CrossRef]
- Teng, I.C.; Chang, Y.J.; Lin, Y.T.; Chu, C.C.; Chen, J.Y.; Wu, Z.F. Sugammadex induced bradycardia and hypotension: A case report and literature review. Medicine 2021, 100, e26796. [Google Scholar] [CrossRef]
- Hunter, J.M.; Naguib, M. Sugammadex-induced bradycardia and asystole: How great is the risk? Br. J. Anaesth. 2018, 121, 8–12. [Google Scholar] [CrossRef] [Green Version]
- Fierro, C.; Medoro, A.; Mignogna, D.; Porcile, C.; Ciampi, S.; Foderà, E.; Flocco, R.; Russo, C.; Martucci, G. Severe Hypotension, Bradycardia and Asystole after Sugammadex Administration in an Elderly Patient. Medicina 2021, 57, 79. [Google Scholar] [CrossRef]
- BRIDION: Highlights of Prescribing Information. Available online: https://www.merck.com/product/usa/pi_circulars/b/bridion/bridion_pi.pdf (accessed on 3 January 2023).
- NDA 22225: Sugammadex Injection. Anesthetic and Analgesic Drug Products Advisory Committee (AC) Meeting November 6, 2015 Sugammadex AC Briefing Document. Available online: https://www.fdanews.com/ext/resources/files/11–15/110615-merck.pdf?1515434323 (accessed on 3 January 2023).
- Ju, J.-W.; Kim, N.; Yang, S.M.; Kim, W.H.; Lee, H.-J. Estimated Incidence of Sugammadex-Induced Anaphylaxis Using the Korea Adverse Event Reporting System Database. J. Clin. Med. 2021, 10, 3202. [Google Scholar] [CrossRef]
- Gaver, R.S.; Brenn, B.R.; Gartley, A.; Donahue, B.S. Retrospective Analysis of the Safety and Efficacy of Sugammadex Versus Neostigmine for the Reversal of Neuromuscular Blockade in Children. Anesth. Analg. 2019, 129, 1124–1129. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Overall (37,882) | Spontaneous Reversal (24,583; 64.9%) | Pharmacological Reversal (13,299; 35.1%) | p-Value | |
|---|---|---|---|---|
| Age (continuous) | 57 (45–69) | 59 (47–70) | 52 (41–66) | <0.001 |
| Age bins | ||||
| 18–40 | 6354 (17.4%) | 3347 (14.2%) | 3007 (23.3%) | <0.001 |
| 40–50 | 6987 (19.1%) | 4149 (17.6%) | 2838 (22.0%) | |
| 50–60 | 7766 (21.3%) | 5034 (21.3%) | 2732 (21.1%) | |
| 60–70 | 7791 (21.3%) | 5533 (23.5%) | 2258 (17.5%) | |
| 70–80 | 6214 (17.0%) | 4549 (19.3%) | 1665 (12.9%) | |
| 80–90 | 1391 (3.8%) | 973 (4.1%) | 418 (3.2%) | |
| Male | 16,256 (44.5%) | 11,042 (46.8%) | 5214 (40.4%) | <0.001 |
| ASA class | ||||
| I | 9667 (26.5%) | 6865 (29.4%) | 2802 (21.4%) | <0.001 |
| II | 17,550 (48.2%) | 12,183 (52.2%) | 5367 (41.0%) | |
| III | 9099 (25.0%) | 4219 (18.1%) | 4880 (37.3%) | |
| IV | 130 (0.4%) | 92 (0.4%) | 38 (0.3%) | |
| BMI class | ||||
| Underweight (<18.5) | 1384 (3.8%) | 945 (4.1%) | 439 (3.4%) | <0.001 |
| Normal weight (18.5–24.9) | 15,555 (42.8%) | 11,034 (47.4%) | 4521 (34.7%) | |
| Overweight (25–29.9) | 11,164 (30.7%) | 8076 (34.7%) | 3088 (23.7%) | |
| Obesity class I (30–34.9) | 3515 (9.7%) | 2440 (10.5%) | 1075 (8.2%) | |
| Obesity class II (35–39.9) | 1556 (4.3%) | 538 (2.3%) | 1018 (7.8%) | |
| Obesity class III (>40) | 3134 (8.6%) | 229.0 (1.0%) | 2905 (22.3%) | |
| Allergy | 12,081 (33.1%) | 7555 (32.3%) | 4526 (34.6%) | <0.001 |
| Smoker | 23,925 (74.3%) | 14,960 (74.3%) | 8965 (74.3%) | 0.9 |
| METS < 4 | 925 (2.7%) | 663 (3.1%) | 262 (2.1%) | <0.001 |
| Comorbidities | ||||
| Arterial hypertension | 12,037 (47.2%) | 7892 (47.2%) | 4145 (47.2%) | >0.9 |
| Arrhythmias | 1993 (7.8%) | 1414 (8.5%) | 579 (6.6%) | <0.001 |
| Vascular disease | 1294 (5.1%) | 988 (5.9%) | 306 (3.5%) | <0.001 |
| Ischemic heart disease | 1652 (6.5%) | 1184 (7.1%) | 468 (5.3%) | <0.001 |
| Heart Failure | 442 (1.7%) | 290 (1.7%) | 152 (1.7%) | >0.9 |
| Other cardiologic comorbidities | 1728 (6.8%) | 1119 (6.7%) | 609 (6.9%) | 0.5 |
| Liver disease | 882 (2.7%) | 680 (3.2%) | 202 (1.7%) | <0.001 |
| Chronic Kidney failure | 779 (2.3%) | 543 (2.5%) | 236 (2.0%) | 0.003 |
| Asthma | 1316 (4.2%) | 711 (3.3%) | 605 (6.2%) | <0.001 |
| COPD | 2520 (8.1%) | 1747 (8.2%) | 773 (7.9%) | 0.4 |
| OSAS | 925 (3.0%) | 267 (1.2%) | 658 (6.7%) | <0.001 |
| Other respiratory comorbidities | 2816 (9.0%) | 1426 (6.7%) | 1390 (14.2%) | <0.001 |
| Epilepsy | 570 (1.7%) | 472 (2.2%) | 98 (0.9%) | <0.001 |
| Stroke | 762 (2.3%) | 524 (2.4%) | 238 (2.1%) | 0.038 |
| Dementia | 205 (0.6%) | 150 (0.7%) | 55 (0.5%) | 0.017 |
| Surgical characteristics | ||||
| Day surgery | 1570 (4.3%) | 720 (3.1%) | 850 (6.6%) | <0.001 |
| Type of surgery | ||||
| General/Abdominal surgery | 10,932 (28.9%) | 4719 (19.2%) | 6213 (46.7%) | <0.001 |
| ENT-Ophthalmic-Plastic | 4772 (12.6%) | 2511 (10.2%) | 2261 (17.0%) | |
| Neurosurgery | 7960 (21.0%) | 7608 (30.9%) | 352 (2.6%) | |
| Orthopedic surgery | 1144 (3.0%) | 897 (3.6%) | 247 (1.9%) | |
| Other surgeries | 1099 (2.9%) | 730 (3.0%) | 369 (2.8%) | |
| Thoracic surgery | 6181 (16.3%) | 4336 (17.6%) | 1845 (13.9%) | |
| Urologic and gynecologic surgery | 5007 (13.2%) | 3111 (12.7%) | 1896 (14.3%) | |
| Vascular surgery | 787 (2.1%) | 671 (2.7%) | 116 (0.9%) | |
| Urgent\Emergency surgery | ||||
| Elective surgery | 34,367 (95.5%) | 21,952 (94.9%) | 12,415 (96.6%) | <0.001 |
| Urgent\Emergency surgery | 1627 (4.5%) | 1189 (5.1%) | 438 (3.4%) | |
| Type of Anaesthesia | ||||
| Inhaled | 32,128 (84.8%) | 20,527 (83.5%) | 11,601 (87.2%) | <0.001 |
| TIVA | 5754 (15.2%) | 4056 (16.5%) | 1698 (12.8%) | |
| Rocuronium (median-IQR dose) | 30,896 (81.6%) | 21.8 mg (14.2) | 35.3 (54.1) | |
| Cisatracurium (median-IQR dose) | 6710 (17.7%) | 16 (8) | 18 (8) | |
| Length of surgery (min) | 120 (80, 190) | 134 (90, 200) | 95 (64, 175) | <0.001 |
| Year of enrolment | ||||
| 2016 | 8354 (22.1%) | 6225 (25.4%) | 2129 (16.0%) | <0.001 |
| 2017 | 9026 (23.9%) | 6105 (24.9%) | 2921 (22.0%) | |
| 2018 | 10,011 (26.5%) | 6197 (25.3%) | 3814 (28.7%) | |
| 2019 | 10,376 (27.5%) | 5970 (24.4%) | 4406 (33.2%) | |
| Total 1 | By Year 1 | ||||||
|---|---|---|---|---|---|---|---|
| Characteristic | N = 37,882 | 2016, N = 8354 | 2017, N = 9026 | 2018, N = 10,011 | 2019, N = 10,376 | p-Value 2 | p-for-Trend |
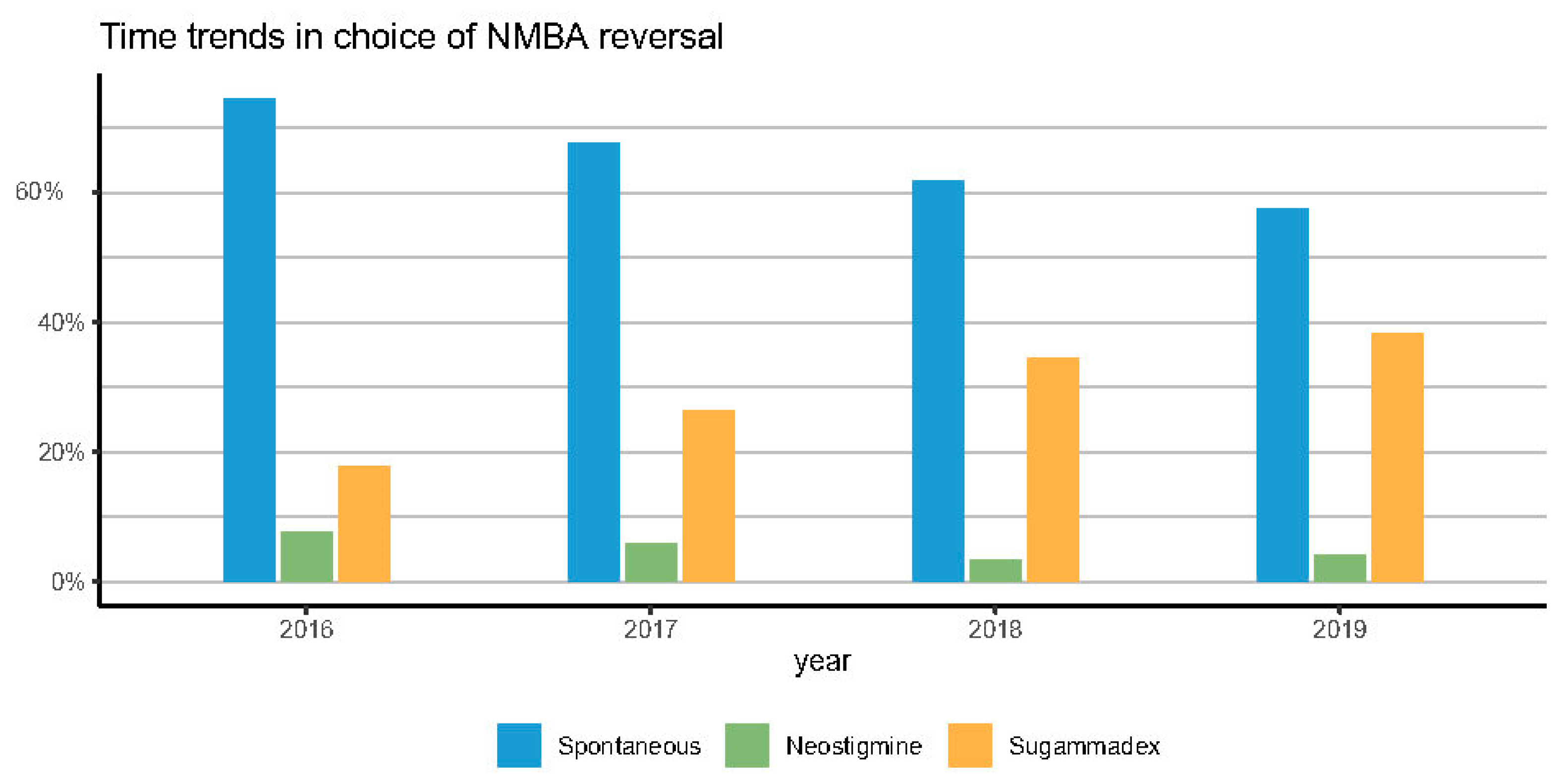
| Pharmacological reversal (NMBRA) | 13,299.0 (35.1%) | 2129.0 (25.5%) | 2921.0 (32.4%) | 3814.0 (38.1%) | 4406.0 (42.5%) | <0.001 | <0.001 |
| Type of NMBRA | |||||||
| Neostigmine | 1962.0 (5.2%) | 642.0 (7.7%) | 528.0 (5.8%) | 348.0 (3.5%) | 434.0 (4.2%) | <0.001 | <0.001 |
| Sugammadex | 11,337.0 (29.9%) | 1487.0 (17.8%) | 2393.0 (26.5%) | 3466.0 (34.6%) | 3972.0 (38.3%) | ||
| Spontaneous reversal | 24,583.0 (64.9%) | 6225.0 (74.5%) | 6105.0 (67.6%) | 6197.0 (61.9%) | 5970.0 (57.5%) | ||
| Type of NMBA | |||||||
| Rocuronium | 30,896.0 (81.6%) | 4881.0 (58.4%) | 7121.0 (78.9%) | 9013.0 (90.0%) | 9797.0 (94.4%) | <0.001 | <0.001 |
| Cisatracurium | 6710.0 (17.7%) | 3301.0 (39.5%) | 1843.0 (20.4%) | 974.0 (9.7%) | 563.0 (5.4%) | ||
| Other NMBA | 276.0 (0.7%) | 172.0 (2.1%) | 62.0 (0.7%) | 24.0 (0.2%) | 16.0 (0.2%) | ||
| Age | 57 (45, 69) | 57 (45, 69) | 56 (45, 69) | 57 (45, 69) | 57 (45, 69) | 0.5 | |
| Age bins | |||||||
| 18–40 | 6354.0 (17.4%) | 1339.0 (17.4%) | 1467.0 (17.1%) | 1717.0 (17.3%) | 1831.0 (17.8%) | 0.002 | 0.9 |
| 40–50 | 6987.0 (19.1%) | 1506.0 (19.6%) | 1720.0 (20.0%) | 1808.0 (18.2%) | 1953.0 (19.0%) | ||
| 50–60 | 7766.0 (21.3%) | 1534.0 (20.0%) | 1789.0 (20.8%) | 2196.0 (22.1%) | 2247.0 (21.8%) | ||
| 60–70 | 7791.0 (21.3%) | 1716.0 (22.3%) | 1855.0 (21.6%) | 2079.0 (20.9%) | 2141.0 (20.8%) | ||
| 70–80 | 6214.0 (17.0%) | 1315.0 (17.1%) | 1459.0 (17.0%) | 1735.0 (17.5%) | 1705.0 (16.6%) | ||
| 80–90 | 1391.0 (3.8%) | 279.0 (3.6%) | 301.0 (3.5%) | 394.0 (4.0%) | 417.0 (4.1%) | ||
| Male | 16,256.0 (44.5%) | 3512.0 (45.7%) | 3745.0 (43.6%) | 4389.0 (44.2%) | 4610.0 (44.8%) | 0.049 | 0.51 |
| ASA | |||||||
| II | 17,550.0 (48.2%) | 3923.0 (51.4%) | 4096.0 (46.8%) | 4604.0 (47.1%) | 4877.0 (47.9%) | <0.001 | <0.001 |
| I | 9667.0 (26.5%) | 2030.0 (26.6%) | 2349.0 (26.8%) | 2605.0 (26.7%) | 2651.0 (26.0%) | ||
| III | 9099.0 (25.0%) | 1661.0 (21.8%) | 2267.0 (25.9%) | 2531.0 (25.9%) | 2620.0 (25.7%) | ||
| IV | 130.0 (0.4%) | 21.0 (0.3%) | 43.0 (0.5%) | 33.0 (0.3%) | 32.0 (0.3%) | ||
| BMI class | |||||||
| Underweight (<18.5) | 1384.0 (3.8%) | 279.0 (3.7%) | 347.0 (4.0%) | 389.0 (4.0%) | 366.0 (3.6%) | 0.004 | 0.042 |
| Normal weight (18.5–24.9) | 15,555.0 (42.8%) | 3247.0 (42.6%) | 3712.0 (42.5%) | 4233.0 (43.5%) | 4321.0 (42.6%) | ||
| Overweight (25–29.9) | 11,164.0 (30.7%) | 2386.0 (31.3%) | 2713.0 (31.1%) | 2942.0 (30.2%) | 3078.0 (30.4%) | ||
| Obesity class I (30–34.9) | 3515.0 (9.7%) | 782.0 (10.3%) | 842.0 (9.7%) | 950.0 (9.8%) | 932.0 (9.2%) | ||
| Obesity class II (35–39.9) | 1556.0 (4.3%) | 308.0 (4.0%) | 388.0 (4.4%) | 408.0 (4.2%) | 448.0 (4.4%) | ||
| Obesity class III (>40) | 3134.0 (8.6%) | 617.0 (8.1%) | 722.0 (8.3%) | 807.0 (8.3%) | 988.0 (9.8%) | ||
| History of allergy | 12,081.0 (33.1%) | 2441.0 (32.0%) | 2953.0 (33.7%) | 3305.0 (33.8%) | 3356.0 (33.0%) | 0.042 | 0.25 |
| Smoking | 8281.0 (25.7%) | 1751.0 (26.1%) | 1994.0 (26.2%) | 2221.0 (25.6%) | 2291.0 (25.2%) | 0.4 | 0.114 |
| Low METS (<4) | 925.0 (2.7%) | 179.0 (3.3%) | 307.0 (3.5%) | 221.0 (2.3%) | 214.0 (2.1%) | <0.001 | <0.001 |
| Hypertension | 12,037.0 (47.2%) | 2554.0 (70.4%) | 2942.0 (43.1%) | 3217.0 (42.8%) | 3284.0 (44.1%) | <0.001 | <0.001 |
| History of arrhythmia | 1993.0 (7.8%) | 343.0 (9.5%) | 480.0 (7.0%) | 576.0 (7.7%) | 585.0 (7.9%) | <0.001 | <0.001 |
| Vasculopathy | 1294.0 (5.1%) | 232.0 (6.4%) | 310.0 (4.5%) | 355.0 (4.7%) | 392.0 (5.3%) | <0.001 | 0.2 |
| Ischemic heart disease | 1652.0 (6.5%) | 381.0 (10.5%) | 398.0 (5.8%) | 463.0 (6.2%) | 397.0 (5.3%) | <0.001 | <0.001 |
| Heart failure | 442.0 (1.7%) | 88.0 (2.4%) | 90.0 (1.3%) | 137.0 (1.8%) | 125.0 (1.7%) | <0.001 | 0.2 |
| Other cardiac disease | 1728.0 (6.8%) | 303.0 (8.4%) | 360.0 (5.3%) | 506.0 (6.7%) | 555.0 (7.4%) | <0.001 | 0.34 |
| Liver disease | 882.0 (2.7%) | 141.0 (2.0%) | 232.0 (2.9%) | 228.0 (2.6%) | 278.0 (3.0%) | <0.001 | 0.002 |
| Chronic Kidney disease | 779.0 (2.3%) | 154.0 (2.2%) | 177.0 (2.2%) | 235.0 (2.6%) | 210.0 (2.3%) | 0.2 | 0.47 |
| Asthma | 1316.0 (4.2%) | 275.0 (4.1%) | 280.0 (3.7%) | 356.0 (4.3%) | 404.0 (4.7%) | 0.015 | 0.01 |
| COPD | 2520.0 (8.1%) | 515.0 (7.6%) | 601.0 (7.9%) | 685.0 (8.4%) | 711.0 (8.3%) | 0.3 | 0.1 |
| OSAS | 925.0 (3.0%) | 174.0 (2.6%) | 198.0 (2.6%) | 249.0 (3.0%) | 304.0 (3.5%) | <0.001 | <0.001 |
| Other respiratory disease | 2816.0 (9.0%) | 604.0 (8.9%) | 599.0 (7.9%) | 709.0 (8.7%) | 894.0 (10.4%) | <0.001 | <0.001 |
| Epilepsy | 570.0 (1.7%) | 133.0 (1.9%) | 146.0 (1.8%) | 154.0 (1.7%) | 135.0 (1.5%) | 0.2 | 0.045 |
| Stroke | 762.0 (2.3%) | 156.0 (2.2%) | 214.0 (2.7%) | 185.0 (2.1%) | 204.0 (2.3%) | 0.055 | 0.47 |
| Dementia | 205.0 (0.6%) | 41.0 (0.6%) | 52.0 (0.7%) | 58.0 (0.7%) | 53.0 (0.6%) | 0.9 | 0.9 |
| Day surgery | 1570.0 (4.3%) | 190.0 (2.5%) | 296.0 (3.4%) | 498.0 (5.0%) | 586.0 (5.7%) | <0.001 | <0.001 |
| Type of surgery | |||||||
| ENT-Ophthalmic-Plastic | 4772.0 (12.6%) | 907.0 (10.9%) | 923.0 (10.2%) | 1294.0 (12.9%) | 1642.0 (15.8%) | <0.001 | 0.117 |
| Neurosurgery | 7960.0 (21.0%) | 1888.0 (22.6%) | 1938.0 (21.5%) | 2059.0 (20.6%) | 2038.0 (19.6%) | ||
| Thoracic surgery | 6181.0 (16.3%) | 1277.0 (15.3%) | 1484.0 (16.4%) | 1688.0 (16.9%) | 1721.0 (16.6%) | ||
| Abdominal surgery | 10,932.0 (28.9%) | 2418.0 (28.9%) | 2605.0 (28.9%) | 2883.0 (28.8%) | 3002.0 (28.9%) | ||
| Orthopedic surgery | 1144.0 (3.0%) | 303.0 (3.6%) | 280.0 (3.1%) | 270.0 (2.7%) | 279.0 (2.7%) | ||
| Uro-gynecological surgery | 5007.0 (13.2%) | 1208.0 (14.5%) | 1265.0 (14.0%) | 1296.0 (12.9%) | 1221.0 (11.8%) | ||
| Vascular surgery | 787.0 (2.1%) | 220.0 (2.6%) | 227.0 (2.5%) | 196.0 (2.0%) | 139.0 (1.3%) | ||
| Other surgery | 1099.0 (2.9%) | 133.0 (1.6%) | 304.0 (3.4%) | 325.0 (3.2%) | 334.0 (3.2%) | ||
| Elective Surgery | 34,367.0 (95.5%) | 7142.0 (94.8%) | 8173.0 (94.8%) | 9255.0 (95.7%) | 9702.0 (96.4%) | <0.001 | <0.001 |
| Urgent\Emergency Surgery | 1627.0 (4.5%) | 392.0 (5.2%) | 448.0 (5.2%) | 416.0 (4.3%) | 363.0 (3.6%) | ||
| TIVA | 5754.0 (15.2%) | 1205.0 (14.4%) | 1287.0 (14.3%) | 1651.0 (16.5%) | 1593.0 (15.4%) | <0.001 | 0.003 |
| Median rocuronium dose (mg) | 60.2 (32.1) | 56.3 (32.0) | 59.0 (31.0) | 60.0 (32.5) | 63.2 (32.5) | <0.001 | |
| Median cisatracurium dose (mg) | 17.9 (9.0) | 18.1 (9.3) | 19.8 (20.2) | 18.8 (13.8) | <0.001 | ||
| Length of surgery | 120 (80, 190) | 121 (80, 190) | 125 (80, 195) | 120 (77, 190) | 115 (75, 188) | <0.001 | |
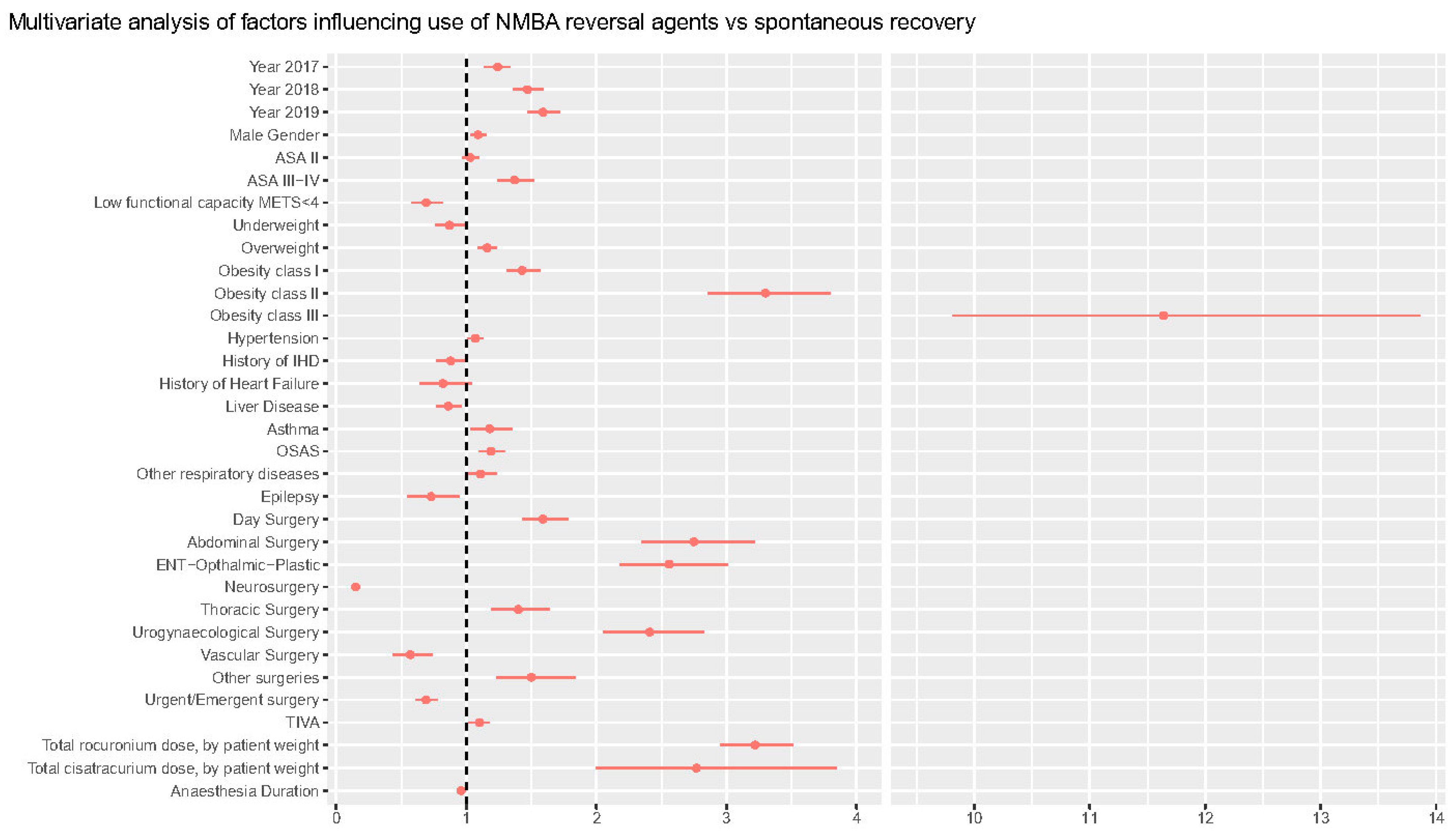
| Characteristic | OR 1 | 95% CI 2 | p-Value |
|---|---|---|---|
| Year (vs. 2016) | |||
| 2017 | 1.24 | 1.14–1.34 | <0.001 |
| 2018 | 1.47 | 1.36–1.59 | <0.001 |
| 2019 | 1.59 | 1.47–1.72 | <0.001 |
| Male Gender | 1.09 | 1.03–1.15 | 0.003 |
| ASA class (vs. class I) | |||
| Class II | 1.03 | 0.97–1.10 | 0.3 |
| Class III-IV | 1.37 | 1.24–1.52 | <0.001 |
| METS < 4 | 0.69 | 0.58–0.82 | <0.001 |
| BMI class (vs. Normal weight) | |||
| Underweight (<18.5) | 0.87 | 0.76–0.99 | 0.03 |
| Overweight (25–29.9) | 1.16 | 1.09–1.23 | <0.001 |
| Obesity class I (30–34.9) | 1.43 | 1.31–1.57 | <0.001 |
| Obesity class II (35–39.9) | 3.30 | 2.86–3.80 | <0.001 |
| Obesity class III (>40) | 11.1 | 9.81–13.9 | <0.001 |
| Day surgery vs. inpatient surgery | 1.59 | 1.43–1.78 | <0.001 |
| Type of surgery | |||
| Orthopedic surgery (ref) | — | — | |
| Abdominal surgery | 2.75 | 2.35–3.22 | <0.001 |
| ENT-Ophthalmic-Plastic surgery | 2.56 | 2.18–3.01 | <0.001 |
| Neurosurgery | 0.15 | 0.13–0.18 | <0.001 |
| Thoracic surgery | 1.40 | 1.19–1.64 | <0.001 |
| Uro-gynecology surgery | 2.41 | 2.05–2.83 | <0.001 |
| Vascular surgery | 0.57 | 0.44–0.74 | 0.013 |
| Other surgeries | 1.50 | 1.23–1.84 | <0.001 |
| Urgent\Emergency surgery | 0.69 | 0.61–0.78 | <0.001 |
| TIVA | 1.10 | 1.02–1.18 | 0.015 |
| Anaesthesia length (per 10-min increase) | 0.96 | 0.96–0.97 | <0.001 |
| Total rocuronium dose (on patient weight) | 3.22 | 2.95–3.51 | <0.001 |
| Total cisatracurium dose (on patient weight) | 2.77 | 2.00–3.85 | <0.001 |
| Hypertension | 1.07 | 1.01–1.13 | 0.02 |
| History of IHD | 0.88 | 0.77–1.01 | 0.07 |
| History of heart failure | 0.82 | 0.64–1.04 | 0.11 |
| Liver disease | 0.86 | 0.77–0.96 | 0.005 |
| Asthma | 1.18 | 1.03–1.35 | 0.015 |
| OSAS | 1.19 | 1.10–1.30 | <0.001 |
| Other respiratory comorbidities | 1.11 | 1.00–1.23 | 0.056 |
| Epilepsy | 0.73 | 0.55–0.95 | 0.022 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Greco, M.; Caruso, P.F.; Angelotti, G.; Aceto, R.; Coppalini, G.; Martinetti, N.; Albini, M.; Bash, L.D.; Carvello, M.; Piccioni, F.; et al. REVersal of nEuromusculAr bLocking Agents in Patients Undergoing General Anaesthesia (REVEAL Study). J. Clin. Med. 2023, 12, 563. https://doi.org/10.3390/jcm12020563
Greco M, Caruso PF, Angelotti G, Aceto R, Coppalini G, Martinetti N, Albini M, Bash LD, Carvello M, Piccioni F, et al. REVersal of nEuromusculAr bLocking Agents in Patients Undergoing General Anaesthesia (REVEAL Study). Journal of Clinical Medicine. 2023; 12(2):563. https://doi.org/10.3390/jcm12020563
Chicago/Turabian StyleGreco, Massimiliano, Pier Francesco Caruso, Giovanni Angelotti, Romina Aceto, Giacomo Coppalini, Nicolò Martinetti, Marco Albini, Lori D. Bash, Michele Carvello, Federico Piccioni, and et al. 2023. "REVersal of nEuromusculAr bLocking Agents in Patients Undergoing General Anaesthesia (REVEAL Study)" Journal of Clinical Medicine 12, no. 2: 563. https://doi.org/10.3390/jcm12020563