
Newly Diagnosed Crohn’s Disease Patients in India and Israel Display Distinct Presentations and Serological Markers: Insights from Prospective Cohorts
 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient Selection
2.2. Definitions and Outcomes
2.3. Serologic Analysis
2.4. Genetic Analysis
2.5. Statistical Analysis
2.6. Ethical Statement
3. Results
3.1. Distinctive Serologic Response to Antiglycans
3.2. Assessing Factors Associated with Complicated Phenotype at Diagnosis
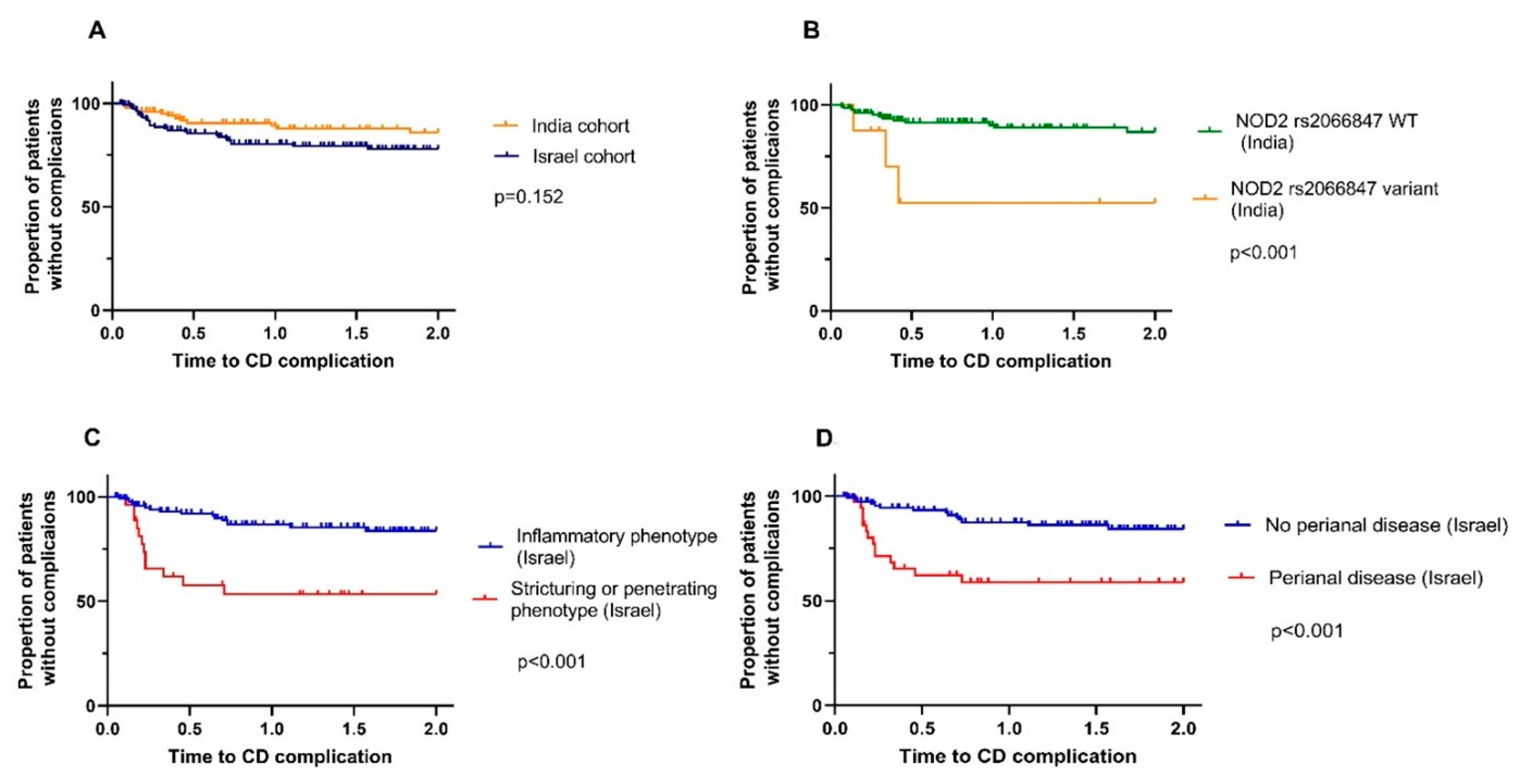
3.3. Assessing Factors Associated with Early Complicated Course
3.4. No Genotype–Serotype Interactions Were Identified
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Kaplan, G.G.; Windsor, J.W. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat. Rev. Gastroenterol. Hepatol. 2020, 18, 56–66. [Google Scholar] [CrossRef] [PubMed]
- Molodecky, N.A.; Soon, I.S.; Rabi, D.M.; Ghali, W.A.; Ferris, M.; Chernoff, G.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Barkema, H.W.; et al. Increasing Incidence and Prevalence of the Inflammatory Bowel Diseases with Time, Based on Systematic Review. Gastroenterology 2012, 142, 46–54.e42. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Ray, G. Inflammatory bowel disease in India—Past, present and future. World J. Gastroenterol. 2016, 22, 8123–8136. [Google Scholar] [CrossRef] [PubMed]
- Kedia, S.; Ahuja, V. Epidemiology of Inflammatory Bowel Disease in India: The Great Shift East. Inflamm. Intest. Dis. 2017, 2, 102–115. [Google Scholar] [CrossRef]
- Philip, M.; the Kerala Inflammatory Bowel Disease Study Group; Augustine, P.; Thomas, V.; Ramesh, G.N.; Vinayakumar, K.R.; Ramachandran, T.M.; Siyad, I.; Mukkada, R.J.; Devi, R.S.; et al. Multi-center prospective survey of inflammatory bowel diseases in Kerala: More than 2000 cases. Indian J. Gastroenterol. 2017, 36, 459–467. [Google Scholar] [CrossRef]
- Makharia, G.K.; Ramakrishna, B.S.; Abraham, P.; Choudhuri, G.; Misra, S.P.; Ahuja, V.; Bhatia, S.J.; Bhasin, D.K.; Dadhich, S.; Dhali, G.K.; et al. Survey of inflammatory bowel diseases in India. Indian J. Gastroenterol. 2012, 31, 299–306. [Google Scholar] [CrossRef]
- Prideaux, L.; Kamm, M.A.; De Cruz, P.P.; Chan, F.K.L.; Ng, S.C. Inflammatory bowel disease in Asia: A systematic review. J. Gastroenterol. Hepatol. 2012, 27, 1266–1280. [Google Scholar] [CrossRef]
- Kalaria, R.; Desai, D.; Abraham, P.; Joshi, A.; Gupta, T.; Shah, S. Temporal Change in Phenotypic Behaviour in Patients with Crohn’s Disease: Do Indian Patients Behave Differently from Western and Other Asian Patients? J. Crohn’s Colitis 2016, 10, 255–261. [Google Scholar] [CrossRef] [Green Version]
- Banerjee, R.; Pal, P.; Nugent, Z.; Ganesh, G.; Adigopula, B.; Pendyala, S.; Bernstein, C.N. IBD in India: Similar phenotype but different demographics than the west. J. Clin. Gastroenterol. 2020, 54, 725–732. [Google Scholar] [CrossRef]
- Banerjee, R.; Pal, P.; Mak, J.W.Y.; Ng, S.C. Challenges in the diagnosis and management of inflammatory bowel disease in resource-limited settings in Asia. Lancet Gastroenterol. Hepatol. 2020, 5, 1076–1088. [Google Scholar] [CrossRef]
- Banerjee, R.; Pal, P.; Girish, B.G.; Reddy, D.N. Risk factors for diagnostic delay in Crohn’s disease and their impact on long-term complications: How do they differ in a tuberculosis endemic region? Aliment. Pharmacol. Ther. 2018, 47, 1367–1374. [Google Scholar] [CrossRef] [Green Version]
- Dotan, I.; Fishman, S.; Dgani, Y.; Schwartz, M.; Karban, A.; Lerner, A.; Weishauss, O.; Spector, L.; Shtevi, A.; Altstock, R.T.; et al. Antibodies Against Laminaribioside and Chitobioside Are Novel Serologic Markers in Crohn’s Disease. Gastroenterology 2006, 131, 366–378. [Google Scholar] [CrossRef]
- Ferrante, M.; Henckaerts, L.; Joossens, M.; Pierik, M.; Joossens, S.; Dotan, N.; Norman, G.L.; Altstock, R.T.; Van Steen, K.; Rutgeerts, P.; et al. New serological markers in inflammatory bowel disease are associated with complicated disease behaviour. Gut 2007, 56, 1394–1403. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hampe, J.; Grebe, J.; Nikolaus, S.; Solberg, C.; Croucher, P.J.; Mascheretti, S.; Jahnsen, J.; Moum, B.; Klump, B.; Krawczak, M.; et al. Association of NOD2 (CARD 15) genotype with clinical course of Crohn’s disease: A cohort study. Lancet 2002, 359, 1661–1665. [Google Scholar] [CrossRef] [PubMed]
- Pugazhendhi, S.; Santhanam, S.; Venkataraman, J.; Creveaux, I.; Ramakrishna, B.S. NOD2 gene mutations associate weakly with ulcerative colitis but not with Crohn’s disease in Indian patients with inflammatory bowel disease. Gene 2013, 512, 309–313. [Google Scholar] [CrossRef]
- Walker, D.G.; Bancil, A.S.; Williams, H.R.; Bunn, C.; Orchard, T.R. How helpful are serological markers in differentiating crohn’s disease from ulcerative colitis in indian asian inflammatory bowel disease patients? Gut 2011, 60, A222–A223. [Google Scholar] [CrossRef]
- Satsangi, J.; Silverberg, M.S.; Vermeire, S.; Colombel, J.F. The Montreal classification of inflammatory bowel disease: Controversies, consensus, and implications. Gut 2006, 55, 749–753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liu, J.Z.; Van Sommeren, S.; Huang, H.; Ng, S.C.; Alberts, R.; Takahashi, A.; Ripke, S.; Lee, J.C.; Jostins, L.; Shah, T.; et al. Association analyses identify 38 susceptibility loci for inflammatory bowel disease and highlight shared genetic risk across populations. Nat. Genet. 2015, 47, 979–986. [Google Scholar] [CrossRef]
- Pugazhendhi, S.; Baskaran, K.; Santhanam, S.; Ramakrishna, B.S. Association of ATG16L1 gene haplotype with inflammatory bowel disease in Indians. PLoS ONE 2017, 12, e0178291. [Google Scholar] [CrossRef] [PubMed]
- Baskaran, K.; Pugazhendhi, S.; Ramakrishna, B.S. Association of IRGM Gene Mutations with Inflammatory Bowel Disease in the Indian Population. PLoS ONE 2014, 9, e106863. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Biasci, D.; Roberts, R.; Gearry, R.; Mansfield, J.; Ahmad, T.; Prescott, N.; Satsangi, J.; Wilson, D.; Jostins, L.; et al. Genome-wide association study identifies distinct genetic contributions to prognosis and susceptibility in Crohn’s disease. Nat. Genet. 2017, 49, 262–268. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Siegel, C.A.; Horton, H.; Siegel, L.S.; Thompson, K.D.; Mackenzie, T.; Stewart, S.K.; Rice, P.W.; Stempak, J.M.; Dezfoli, S.; Haritunians, T.; et al. A validated web-based tool to display individualised Crohn’s disease predicted outcomes based on clinical, serologic and genetic variables. Aliment. Pharmacol. Ther. 2016, 43, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Adler, J.; Rangwalla, S.C.; Dwamena, B.; Higgins, P. The Prognostic Power of the NOD2 Genotype for Complicated Crohn’s Disease: A Meta-Analysis. Am. J. Gastroenterol. 2011, 106, 699–712. [Google Scholar] [CrossRef]
- Palomino-Morales, R.; Oliver, J.; Gómez-García, M.; López-Nevot, M.A.; Rodrigo, L.; Nieto, A.; Alizadeh, B.Z.; Martin, J. Association of ATG16L1 and IRGM genes polymorphisms with inflammatory bowel disease: A meta-analysis approach. Genes Immun. 2009, 10, 356–364. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.R.K.; Arnott, I.D.R.; Drummond, H.E.; Nimmo, E.R.; Satsangi, J. Disease Location, Anti-Saccharomyces cerevisiae Antibody, and NOD2/CARD15 Genotype Influence the Progression of Disease Behavior in Crohn’s Disease. Inflamm. Bowel Dis. 2004, 10, 521–528. [Google Scholar] [CrossRef]
- Ben-Shachar, S.; Finezilber, Y.; Elad, H.; Rabinowitz, K.; Goren, I.; Isakov, O.; Yanai, H.; Dotan, I. Genotype–Serotype Interactions Shed Light on Genetic Components of Inflammatory Bowel Diseases. Inflamm. Bowel Dis. 2018, 25, 336–344. [Google Scholar] [CrossRef]
- Burisch, J.; Kiudelis, G.; Kupcinskas, L.; Kievit, H.A.L.; Andersen, K.W.; Andersen, V.; Salupere, R.; Pedersen, N.; Kjeldsen, J.; D’Incà, R.; et al. Natural disease course of Crohn’s disease during the first 5 years after diagnosis in a European population-based inception cohort: An Epi-IBD study. Gut 2018, 68, 423–433. [Google Scholar] [CrossRef]
- Thia, K.T.; Sandborn, W.J.; Harmsen, W.S.; Zinsmeister, A.R.; Loftus, E.V., Jr. Risk Factors Associated with Progression to Intestinal Complications of Crohn’s Disease in a Population-Based Cohort. Gastroenterology 2010, 139, 1147–1155. [Google Scholar] [CrossRef] [Green Version]
- Castaño-Rodríguez, N.; Kaakoush, N.O.; Lee, W.S.; Mitchell, H.M. Dual role of Helicobacter and Campylobacter species in IBD: A systematic review and meta-analysis. Gut 2017, 66, 235–249. [Google Scholar] [CrossRef]
- Walker, D.G.; Williams, H.R.T.; Kane, S.P.; Mawdsley, J.E.; Arnold, J.; McNeil, I.; Thomas, H.J.W.; Teare, J.; Hart, A.L.; Pitcher, M.C.L.; et al. Differences in Inflammatory Bowel Disease Phenotype between South Asians and Northern Europeans Living in North West London, UK. Am. J. Gastroenterol. 2011, 106, 1281–1289. [Google Scholar] [CrossRef]
- Gracie, D.; Williams, C.; Sood, R.; Mumtaz, S.; Bholah, H.M.; Hamlin, J.P.; Ford, A. Poor Correlation Between Clinical Disease Activity and Mucosal Inflammation, and the Role of Psychological Comorbidity, in Inflammatory Bowel Disease. Am. J. Gastroenterol. 2016, 111, 541–551. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, H.; Main, J.; Pennington, C.R.; Parratt, D. Antibody to selected strains of Saccharomyces cerevisiae (baker’s and brewer’s yeast) and Candida albicans in Crohn’s disease. Gut 1990, 31, 536–538. [Google Scholar] [CrossRef] [Green Version]
- McGuckin, M.A.; Eri, R.; Simms, L.A.; Florin, T.H.; Radford-Smith, G. Intestinal barrier dysfunction in inflammatory bowel diseases. Inflamm. Bowel Dis. 2009, 15, 100–113. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rieder, F.; Schleder, S.; Wolf, A.; Dirmeier, A.; Strauch, U.; Obermeier, F.; Lopez, R.; Spector, L.; Fire, E.; Yarden, J.; et al. Serum anti-glycan antibodies predict complicated Crohn’s disease behavior. Inflamm. Bowel Dis. 2010, 16, 1367–1375. [Google Scholar] [CrossRef]
- Makharia, G.K.; Sachdev, V.; Gupta, R.; Lal, S.; Pandey, R.M. Anti-Saccharomyces cerevisiae Antibody Does Not Differentiate Between Crohn’s Disease and Intestinal Tuberculosis. Am. J. Dig. Dis. 2006, 52, 33–39. [Google Scholar] [CrossRef] [PubMed]
- Prideaux, L.; Kamm, M.A.; De Cruz, P.; Van Langenberg, D.R.; Ng, S.C.; Dotan, I. Inflammatory bowel disease serology in Asia and the West. World J. Gastroenterol. 2013, 19, 6207–6213. [Google Scholar] [CrossRef] [PubMed]
- Lawrance, I.C.; Hall, A.; Leong, R.; Pearce, C.; Murray, K. A Comparative Study of Goblet Cell and Pancreatic Exocine Autoantibodies Combined with ASCA and pANCA in Chinese and Caucasian Patients with IBD. Inflamm. Bowel Dis. 2005, 11, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Hisabe, T.; Matsui, T.; Sakurai, T.; Murakami, Y.; Tanabe, H.; Matake, H.; Yao, T.; Kamachi, S.; Iwashita, A. Anti- Saccharomyces cerevisiae antibodies in Japanese patients with inflammatory bowel disease: Diagnostic accuracy and clinical value. J. Gastroenterol. 2003, 38, 121–126. [Google Scholar] [CrossRef]
- Lawrance, I.C.; Murray, K.; Hall, A.; Sung, J.J.; Leong, R. A Prospective Comparative Study of ASCA and pANCA in Chinese and Caucasian IBD Patients. Am. J. Gastroenterol. 2004, 99, 2186–2194. [Google Scholar] [CrossRef]
- Kim, B.; Park, S.; Han, J.; Kim, J.; Kim, T.; Kim, W. Clinical significance of anti-Saccharomyces cerevisiae antibody (ASCA) in Korean patients with Crohn’s disease and its relationship to the disease clinical course. Dig. Liver Dis. 2007, 39, 610–616. [Google Scholar] [CrossRef] [PubMed]
- Murdoch, T.B.; Xu, W.; Stempak, J.M.; Landers, C.; Targan, S.R.; Rotter, J.I.; Silverberg, M.S. Pattern recognition receptor and autophagy gene variants are associated with development of antimicrobial antibodies in Crohn’s disease. Inflamm. Bowel Dis. 2012, 18, 1743–1748. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cleynen, I.; González, J.R.; Figueroa, C.; Franke, A.; McGovern, D.; Bortlík, M.; Crusius, B.J.A.; Vecchi, M.; Artieda, M.; Szczypiorska, M.; et al. Genetic factors conferring an increased susceptibility to develop Crohn’s disease also influence disease phenotype: Results from the IBDchip European Project. Gut 2013, 62, 1556–1565. [Google Scholar] [CrossRef] [Green Version]
- Schnitzler, F.; Friedrich, M.; Wolf, C.; Angelberger, M.; Diegelmann, J.; Olszak, T.; Beigel, F.; Tillack, C.; Stallhofer, J.; Göke, B.; et al. The NOD2 p.Leu1007fsX1008 Mutation (rs2066847) Is a Stronger Predictor of the Clinical Course of Crohn’s Disease than the FOXO3A Intron Variant rs12212067. PLoS ONE 2014, 9, e108503. [Google Scholar] [CrossRef] [Green Version]
- Ng, S.C.; Tang, W.; Ching, J.Y.; Wong, M.; Chow, C.M.; Hui, A.J.; Wong, T.C.; Leung, V.K.; Tsang, S.W.; Yu, H.H.; et al. Incidence and Phenotype of Inflammatory Bowel Disease Based on Results from the Asia-Pacific Crohn’s and Colitis Epidemiology Study. Gastroenterology 2013, 145, 158–165.e2. [Google Scholar] [CrossRef] [PubMed]
- Mak, W.Y.; Zhao, M.; Ng, S.C.; Burisch, J. The epidemiology of inflammatory bowel disease: East meets west. J. Gastroenterol. Hepatol. 2019, 35, 380–389. [Google Scholar] [CrossRef]
- Bernstein, C.N.; Loftus, E.V.; Ng, S.C.; Lakatos, P.L.; Moum, B. Hospitalisations and surgery in Crohn’s disease. Gut 2012, 61, 622–629. [Google Scholar] [CrossRef] [Green Version]
- Ramadas, A.V.; Gunesh, S.; Thomas GA, O.; Williams, G.T.; Hawthorne, A.B. Natural history of Crohn’s disease in a population-based cohort from Cardiff (1986-2003): A study of changes in medical treatment and surgical resection rates. Gut 2010, 59, 1200–1206. [Google Scholar] [CrossRef]
- Ungaro, R.C.; Yzet, C.; Bossuyt, P.; Baert, F.J.; Vanasek, T.; D’Haens, G.R.; Joustra, V.W.; Panaccione, R.; Novacek, G.; Reinisch, W.; et al. Deep Remission at 1 Year Prevents Progression of Early Crohn’s Disease. Gastroenterology 2020, 159, 139–147. [Google Scholar] [CrossRef]
- Kaplan, G.G.; Jess, T. The Changing Landscape of Inflammatory Bowel Disease: East Meets West. Gastroenterology 2016, 150, 24–26. [Google Scholar] [CrossRef]


{kind=link}
| (a) | Indian Cohort (n = 104) | Israeli Cohort (n = 156) | p-Value |
| Sex, male, n (%) | 68 (65.4) | 77 (49.4) | 0.019 |
| Age, years ±SD | 37.8 ± 12.8 | 31.8 ± 12.9 | <0.001 |
| BMI, kg/m2 ± SD | 19.9 ± 4.3 | 23.4 ± 4.5 | <0.001 |
| Active smokers, n (%) | 9 (8.7) | 34 (21.8) | <0.001 |
| Family history of Crohn’s disease, n (%) | 4 (3.8) | 35 (22.4) | <0.001 |
| Extraintestinal manifestations, n (%) | 22 (21.2) | 53 (39.6) | 0.003 |
| Treatment | |||
| Corticosteroids, n (%) | 58 (55.8) | 74 (47.4) | 0.187 |
| 5-ASA, n (%) | 99 (95.2) | 60 (38.5) | <0.001 |
| IMM, n (%) | 54 (51.9) | 69 (44.2) | 0.223 |
| Biologic therapy, n (%) | 6 (5.8) | 65 (41.7) | <0.001 |
| Disease location | |||
| Ileal, n (%) a | 45 (43.3) | 70 (44.9) | 0.004 |
| Colonic, n (%) b | 37 (35.6) | 30 (19.2) | |
| Ileocolonic, n (%) c | 22 (21.2) | 55 (35.3) | |
| Upper GI involvement, n (%) | 14 (13.5) | 8 (5.1) | 0.018 |
| Perianal, n (%) | 6 (5.8) | 37 (23.7) | <0.001 |
| Disease phenotype | |||
| Inflammatory, n (%) d | 56 (53.8) | 129 (82.7) | <0.001 |
| Stricturing, n (%) e | 37 (35.6) | 10 (6.4) | |
| Penetrating, n (%) f | 11 (10.6) | 17 (10.9) | |
| Complicated phenotype at diagnosis | |||
| Stricturing and/or penetrating and/or perianal, n (%) | 50 (48.1) | 47 (30.1) | 0.003 |
| Lag time from symptoms to diagnosis, months, median (IQR) | 10.5 (3–38) | 3 (1–8) | p < 0.001 |
| (b) | Indian Cohort (n = 104) | Israeli Cohort (n = 156 *) | p-Value |
| Hemoglobin, g/dL, median (IQR) | 11.3 (9.9–12.8) | 13.1 (12.1–14.3) | <0.001 |
| White blood cells, K/uL, median (IQR) | 7.9 (6.0–9.4) | 8.2 (6.8–10.2) | 0.019 |
| C-reactive protein, mg/L, median (IQR) | 9.3 (5.4–15.5) | 9.9 (2.5–21.6) | 0.447 |
| Vitamin B12, pg/mL, median (IQR) | 298 (213–479) | 393 (309–522) | <0.001 |
| ASCA, IU/mL, mean ± SD | 24.2 ± 21.3 | 43.0 ± 39.0 * | <0.001 |
| ALCA, IU mean ± SD | 26.6 ± 23.6 | 18.2 ± 14.5 * | 0.005 |
| ACCA, IU/mL, mean ± SD | 41.4 ± 36.9 | 31.5 ± 24.9 * | 0.396 |
| AMCA, IU mean ± SD | 43.1 ± 42.3 | 57.2 ± 61.1 * | <0.001 |
| ASCA-positive, n (%) | 14 (13.5) | 47 (32.6) * | 0.001 |
| ALCA-positive, n (%) | 13 (12.5) | 3 (2.1) * | 0.001 |
| ACCA-positive, n (%) | 18 (17.3) | 5 (3.5) * | <0.001 |
| AMCA-positive, n (%) | 13 (12.5) | 15 (10.3) * | 0.685 |
| Any positive serology, n (%) | 30 (28.8) | 53 (36.8) * | 0.180 |
| Indian Cohort (n = 104) | Israeli Cohort (n = 144 *) | |||||
|---|---|---|---|---|---|---|
| Complicated Phenotype & (n = 50) | Uncomplicated Phenotype (n = 54) | p Value | Complicated Phenotype & (n = 46) | Uncomplicated Phenotype (n = 98) | p Value | |
| Any positive serology, n (%) | 13 (26.0) | 17 (31.5) | 0.665 | 24 (52.2) | 29 (29.6) | 0.01 |
| ASCA-positive serology, n (%) | 8 (16) | 6 (11.1) | 0.570 | 24 (52.2) | 23 (23.5) | 0.001 |
| ALCA-positive serology, n (%) | 5 (10) | 8 (14.8) | 0.559 | 1 (2.2) | 2 (2) | 0.999 |
| ACCA-positive serology, n (%) | 7 (14) | 11 (20.4) | 0.445 | 3 (6.5) | 2 (2) | 0.327 |
| AMCA-positive serology, n (%) | 3 (6) | 10 (18.5) | 0.075 | 8 (17.4) | 7 (7.1) | 0.08 |
| Genetic Variant | Israeli Cohort (n = 122) | Indian Cohort (n = 103) | p Value |
|---|---|---|---|
| ATG16L1_rs2241880, n (%) | |||
| Wild type | 16 (13.1) | 25 (24.3) | 0.061 |
| Heterozygous | 59 (48.4) | 49 (47.6) | |
| Homozygous | 47 (38.5) | 29 (28.2) | |
| CARD8_rs2043211, n (%) | |||
| Wild type | 65 (53.3) | 42 (40.8) | 0.17 |
| Heterozygous | 46 (37.7) | 49 (47.6) | |
| Homozygous | 11 (9.0) | 12 (11.7) | |
| CARD9_rs10781499, n (%) | |||
| Wild type | 48 (39.3) | 39 (37.9) | 0.9 |
| Heterozygous | 58 (47.5) | 52 (50.5) | |
| Homozygous | 16 (13.1) | 12 (11.7) | |
| NOX3_rs6557421, n (%) | |||
| Wild type | 53 (43.4) | 59 (57.3) | 0.11 |
| Heterozygous | 61 (50.0) | 40 (38.8) | |
| Homozygous | 8 (6.6) | 4 (3.9) | |
| NOD2_rs2066844, n (%) | |||
| Wild type | 117 (95.9) | 103 (100) | 0.064 |
| Heterozygous | 5 (4.1) | 0 (0) | |
| Homozygous | 0 (0) | 0 (0) | |
| NOD2_rs2066845, n (%) | |||
| Wild type | 101 (82.8) | 101 (98.1) | <0.001 |
| Heterozygous | 21 (17.2) | 2 (1.9) | |
| Homozygous | 0 (0) | 0 (0) | |
| NOD2_rs2066847, n (%) | |||
| Wild type | 113 (92.6) | 95 (92.2) | 0.052 |
| Heterozygous | 9 (7.4) | 4 (3.9) | |
| Homozygous | 0 (0) | 4 (3.9) | |
| IRGM_rs11741861, n (%) | |||
| Wild type | 70 (57.4) | 62 (60.2) | 0.926 |
| Heterozygous | 45 (36.9) | 35 (34.0) | |
| Homozygous | 7 (5.7) | 6 (5.8) | |
| IRGM_rs4958847, n (%) | |||
| Wild type | 62 (50.8) | 46 (44.7) | 0.2 |
| Heterozygous | 51 (41.8) | 42 (40.8) | |
| Homozygous | 9 (7.4) | 15 (14.6) | |
| MHC_ rs9279411, n (%) | |||
| Wild type | 117 (95.9) | 103 (100) | 0.064 |
| Heterozygous | 5 (4.1) | 0 (0) | |
| Homozygous | 0 (0) | 0 (0) | |
| XACT _rs5929166, n (%) | |||
| Wild type | 121 (99.2) | 102 (99) | 0.999 |
| Heterozygous | 1 (0.8) | 1 (1.0) | |
| Homozygous | 0 (0) | 0 (0) | |
| IGFBP_rs75764599, n (%) | |||
| Wild type | 116 (95.1) | 103 (100) | 0.032 |
| Heterozygous | 6 (4.9) | 0 (0) | |
| Homozygous | 0 (0) | 0 (0) | |
| FOXO3_rs147856773, n (%) | |||
| Wild type | 92 (75.4) | 81 (78.6) | 0.815 |
| Heterozygous | 29 (23.8) | 21 (20.4) | |
| Homozygous | 1 (0.8) | 1 (1.0) | |
| ATG16L1_rs4663402, n (%) | |||
| Wild type | 116 (95.1) | 88 (85.4) | 0.028 |
| Heterozygous | 5 (4.1) | 13 (12.6) | |
| Homozygous | 1 (0.8) | 2 (1.9) | |
| ATG16L1_rs4663421, n (%) | |||
| Wild type | 116 (95.1) | 88 (85.4) | 0.028 |
| Heterozygous | 5 (4.1) | 13 (12.6) | |
| Homozygous | 1 (0.8) | 2 (1.9) | |
| IRGM_rs1000113, n (%) | |||
| Wild type | 70 (57.4) | 63 (61.2) | 0.838 |
| Heterozygous | 45 (36.9) | 34 (33) | |
| Homozygous | 7 (5.7) | 6 (5.8) | |
| IRGM_rs180802994, n (%) | |||
| Wild type | 118 (96.7) | 95 (92.2) | 0.150 |
| Heterozygous | 4 (3.2) | 8 (7.8) | |
| Homozygous | 0 (0) | 0 (0) | |
| TNF-α_rs1799964, n (%) | |||
| Wild type | 82 (67.2) | 41 (39.8) | <0.001 |
| Heterozygous | 33 (27) | 51 (49.5) | |
| Homozygous | 7 (5.7) | 11 (10.7) | |
| TNF-α_rs1799724, n (%) | |||
| Wild type | 79 (64.8) | 81 (78.6) | 0.012 |
| Heterozygous | 37 (30.3) | 22 (21.4) | |
| Homozygous | 6 (4.9) | 0 (0) | |
| JAK2_rs1887428, n (%) | |||
| Wild type | 49 (40.2) | 28 (27.2) | 0.050 |
| Heterozygous | 55 (45.1) | 49 (47.6) | |
| Homozygous | 18 (14.8) | 26 (25.2) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Goren, I.; Sharar Fischler, T.; Yanai, H.; Pal, P.; Adigopula, B.; Pendyala, S.; Ganesh, G.; Vishnubhotla, R.; Rabinowitz, K.M.; Shaham Barda, E.; et al. Newly Diagnosed Crohn’s Disease Patients in India and Israel Display Distinct Presentations and Serological Markers: Insights from Prospective Cohorts. J. Clin. Med. 2022, 11, 6899. https://doi.org/10.3390/jcm11236899
Goren I, Sharar Fischler T, Yanai H, Pal P, Adigopula B, Pendyala S, Ganesh G, Vishnubhotla R, Rabinowitz KM, Shaham Barda E, et al. Newly Diagnosed Crohn’s Disease Patients in India and Israel Display Distinct Presentations and Serological Markers: Insights from Prospective Cohorts. Journal of Clinical Medicine. 2022; 11(23):6899. https://doi.org/10.3390/jcm11236899
Chicago/Turabian StyleGoren, Idan, Tali Sharar Fischler, Henit Yanai, Partha Pal, Bhargavi Adigopula, Sushmitha Pendyala, Girish Ganesh, Ravikanth Vishnubhotla, Keren Masha Rabinowitz, Efrat Shaham Barda, and et al. 2022. "Newly Diagnosed Crohn’s Disease Patients in India and Israel Display Distinct Presentations and Serological Markers: Insights from Prospective Cohorts" Journal of Clinical Medicine 11, no. 23: 6899. https://doi.org/10.3390/jcm11236899