

Recommendations for Diversifying Racial and Ethnic Representation in Autism Intervention Research: A Crossover Review of Recruitment and Retention Practices in Pediatric Mental Health
 , , , ,
, , , ,
Abstract
:1. Introduction
Purpose of the Present Study
2. Methods
2.1. Design and Research Questions
- What practices have researchers reported to recruit and retain ethnically/racially diverse participants in parenting models and programs targeting children with mental health disorders?
- Are there opportunities for cross-fertilization from recruitment and retention strategies of racially and ethnically diverse populations used in parenting intervention research to address mental health disorders to improve the same practices in ASD intervention research?
2.2. Electronic Databases and Search Strategies
2.3. Inclusion and Exclusion Selection Criteria
2.4. Data Extraction and Coding
2.5. Interrater Reliability
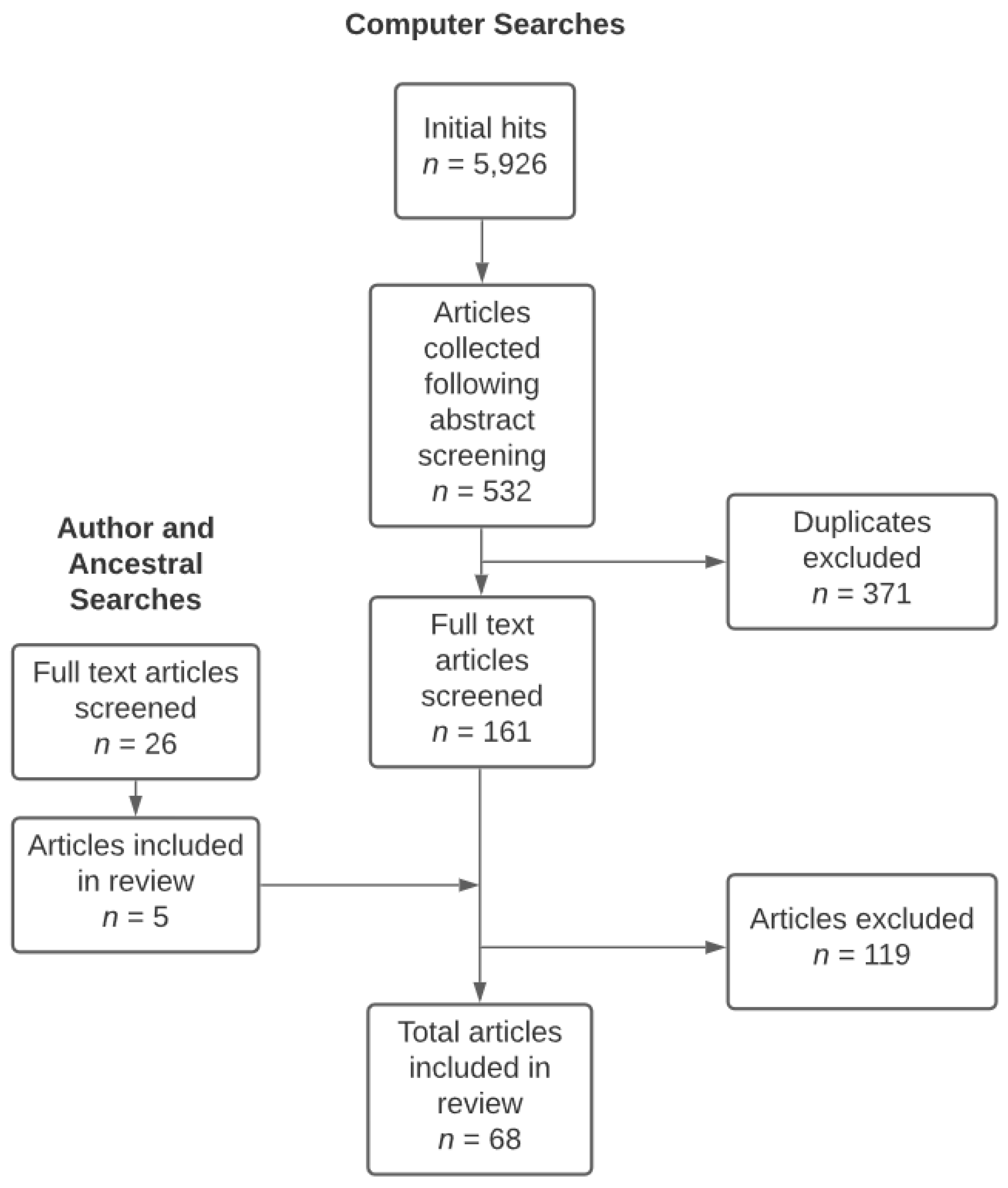
Article Inclusion and Coding
3. Results
3.1. Participant Characteristics
3.1.1. Children
3.1.2. Parents
3.2. Intervention Settings and Types of Intervention
3.3. Parenting Programs, Models, and Delivery Format
3.4. Recruitment and Retention Strategies
3.5. Cultural Adaptation
3.6. Attrition
4. Discussion
4.1. Practices Reported by Researchers to Recruit and Retain Minoritized Participants
4.2. Opportunities for Recruitment and Retention in ASD Parenting Intervention Research
4.2.1. Reporting Requirements for Recruitment and Retention Strategies
4.2.2. Develop Interventions That Address Population Relevant Issues
4.2.3. Relational and Culturally Relevant Approaches to Intervention Development
4.2.4. Identify and Minimize Barriers to Engagement in Intervention Research
4.3. Limitations of the Review
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Artiles, A.J.; Trent, S.C.; Kuan, L.A. Learning disabilities empirical research on ethnic minority students: An analysis of 22 years of studies published in selected refereed journals. Learn. Disabil. Res. Pract. 1997, 12, 82–91. [Google Scholar]
- Broder-Fingert, S.; Shui, A.; Pulcini, C.D.; Kurowski, D.; Perrin, J.M. Racial and ethnic differences in subspecialty service use by children with autism. Pediatrics 2013, 132, 94–100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Centers for Disease Control and Prevention. 2018. Available online: https://www.cdc.gov/ncbddd/autism/addm-community-report/executive-summary.html (accessed on 15 May 2022).
- Harstad, E.; Huntington, N.; Bacic, J.; Barbaresi, W. Disparity of care for children with parent-reported autism spectrum disorders. Acad. Pediatr. 2013, 13, 334–339. [Google Scholar] [CrossRef] [PubMed]
- Magaña, S.; Lopez, K.; Aguinaga, A.; Morton, H. Access to diagnosis and treatment services among Latino children with autism spectrum disorders. Intellect. Dev. Disabil. 2013, 51, 141–153. [Google Scholar] [CrossRef] [PubMed]
- Mandell, D.S.; Morales, K.H.; Xie, M.; Lawer, L.J.; Stahmer, A.C.; Marcus, S.C. Age of diagnosis among Medicaid-enrolled children with autism, 2001–2004. Psychiatr. Serv. 2010, 61, 822–829. [Google Scholar] [CrossRef]
- Sinclair, J.; Hansen, S.G.; Machalicek, W.; Knowles, C.; Hirano, K.A.; Dolata, J.K.; Blakely, A.W.; Seeley, J.; Murray, C. A 16-year review of participant diversity in intervention research across a selection of 12 special education journals. Except. Child. 2018, 84, 312–329. [Google Scholar] [CrossRef] [Green Version]
- Norbury, C.F.; Sparks, A. Difference or disorder? Cultural issues in understanding neurodevelopmental disorders. Dev. Psychol. 2013, 49, 45–58. [Google Scholar] [CrossRef] [Green Version]
- Ratto, A.B.; Anthony, B.J.; Pugliese, C.; Mendez, R.; Safer-Lictenstein, J.; Dudley, K.M.; Kahn, N.F.; Kenworthy, L.; Biel, M.; Martucci, J.L.; et al. Lessons learned: Engaging culturally diverse families in neurodevelopmental disorders intervention research. Autism 2016, 21, 622–634. [Google Scholar] [CrossRef] [Green Version]
- Safer-Lichtenstein, J.; Hamilton, J.C.; McIntyre, L. Examining demographics in randomized controlled trials of group-based social skills interventions for individuals with autism spectrum disorders. J. Autism Dev. Disord. 2019, 49, 3453–3461. [Google Scholar] [CrossRef]
- Hussar, W.J.; Bailey, T.M. Projections of Education Statistics to 2022 (NCES 2014-051); U.S. Department of Education, National Center for Education Statistics, U.S. Government Printing Office: Washington, DC, USA, 2013.
- Harris, B.; Barton, E.E.; Brunson McClain, M. Inclusion of racially and ethnically diverse populations in ASD intervention research. Res. Autism Spectr. Disord. 2020, 73, 101551. [Google Scholar] [CrossRef]
- Buzhardt, J.; Rusinko, L.; Heitzman-Powell, L.; Trevino-Maack, S.; McGrath, A. Exploratory evaluation and initial adaptation of a parent training program for Hispanic families of children with autism. Fam. Process 2015, 55, 107–122. [Google Scholar] [CrossRef]
- Carr, T.; Lord, C. A pilot study promoting participation of families with limited resources in early autism intervention. Res. Autism Spectr. 2016, 2, 87–96. [Google Scholar] [CrossRef] [Green Version]
- Kasari, C.; Dean, M.; Kretzmann, M.; Shih, W.; Orlich, F.; Whitney, R.; Landa, R.; Lord, C.; King, B. Children with autism spectrum disorder and social skills groups at school: A randomized trial comparing intervention approach and peer composition. J. Child Psychol. Psychiatry 2016, 57, 171–179. [Google Scholar] [CrossRef]
- Magaña, S.; Lopez, K.; Salkas, K.; Illand, E.; Morales, M.A.; Garcia Torres, M.; Zeng, W.; Machalicek, W. A randomized waitlist control group study of a culturally tailored parent education intervention for Latino parents of children with ASD. J. Autism Dev. Disord. 2020, 49, 250–262. [Google Scholar] [CrossRef]
- Stadnick, N.A.; Stahmer, A.; Brookman-Frazee, L. Preliminary effectiveness of project impact: A parent-mediated intervention for children with autism spectrum disorder delivered in a community program. J. Autism Dev. Disord. 2015, 45, 2092–2104. [Google Scholar] [CrossRef] [Green Version]
- Lopez, K.; Magaña, S.; Morales, M.; Iland, E. Parents taking action: Reducing disparities through a culturally informed intervention for Latinx parents of children with autism. J. Ethn. Cult. Divers. Soc. Work. 2019, 28, 31–49. [Google Scholar] [CrossRef]
- Magaña, S.; Lopez, K.; Machalicek, W. Parents taking action: A psycho-educational intervention for Latino parents of children with autism spectrum disorder. Fam. Process 2017, 56, 59–74. [Google Scholar] [CrossRef]
- Jo, B. Statistical power in randomized intervention studies with noncompliance. Psychol. Methods 2002, 7, 178–193. [Google Scholar] [CrossRef]
- Nunan, D.; Aronson, J.; Bankhead, C. Catalogue of bias: Attrition bias. BMJ Evid.-Based Med. 2018, 23, 21–22. [Google Scholar] [CrossRef]
- Gonzalez, A.; Weersing, V.R.; Warnick, E.M.; Scahill, L.D.; Woolston, J.L. Predictors of treatment attrition among an outpatient clinic sample of youths with clinically significant anxiety. Adm. Policy Ment. Health 2011, 38, 356–367. [Google Scholar] [CrossRef] [Green Version]
- Pellerin, K.A.; Costa, N.M.; Weems, C.F.; Dalton, R.F. An examination of treatment completers and non-completers at a child and adolescent community mental health clinic. Community Ment. Health J. 2010, 46, 273–281. [Google Scholar] [CrossRef] [PubMed]
- Matson, J.L.; Goldin, R.L. Comorbidity and autism: Trends, topics and future directions. Res. Autism Spectr. Disord. 2013, 7, 1228–1233. [Google Scholar] [CrossRef]
- Hunter, W.C.; Elswick, S.E.; Casey, L.B. Efficient wraparound service model for students with emotional and behavioral disorders: A collaborative model for school social workers and teachers. Child. Sch. 2018, 40, 59–61. [Google Scholar] [CrossRef]
- Lee, P.C.; Niew, W.I.; Yang, H.J.; Chen, V.C.; Lin, K.C. A meta-analysis of behavioral parent training for children with attention deficit hyperactivity disorder. Res. Dev. Disabil. 2012, 33, 2040–2049. [Google Scholar] [CrossRef]
- Eyberg, S.M.; Nelson, M.M.; Boggs, S.R. Evidence-based psychosocial treatments for children and adolescents with disruptive behavior. J. Clin. Child Adolesc. Psychol. 2008, 37, 215–237. [Google Scholar] [CrossRef]
- Karst, J.S.; Van Hecke, A.V. Parent and family impact of autism spectrum disorders: A review and proposed model for intervention evaluation. Clin. Child Fam. Psychol. Rev. 2012, 15, 247–277. [Google Scholar] [CrossRef]
- American Psychological Association. Multicultural Guidelines: An Ecological Approach to Context, Identity, and Intersectionality. 2017. Available online: https://www.apa.org/about/policy/multicultural-guidelines.pdf (accessed on 15 May 2022).
- National Institutes of Health Revitalization Act of 1993. Subtitle B: Clinical Research Equity Regarding Women and Minorities. Available online: https://orwh.od.nih.gov/sites/orwh/files/docs/NIH-Revitalization-Act-1993.pdf (accessed on 15 May 2022).
- Bierman, K.L.; Nix, R.L.; Heinrichs, B.S.; Domitrovich, C.E.; Gest, S.D.; Welsh, J.A.; Gill, S. Effects of head start REDI on children’s outcomes 1 year later in different kindergarten contexts. Child Dev. 2014, 85, 140–159. [Google Scholar] [CrossRef] [Green Version]
- Dawson-McClure, S.; Calzada, E.; Huang, K.-Y.; Kamboukos, D.; Rhule, D.; Kolawole, B.; Petkova, E.; Miller Brotman, L. A population-level approach to promoting healthy child development and school success in low-income, urban neighborhoods: Impact on parenting and child conduct problems. Prev. Sci. 2015, 16, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Fernandez, M.A.; Butler, A.M.; Eyberg, S.M. Treatment outcome for low socioeconomic status African American families in parent-child interaction therapy: A pilot study. Child Fam. Behav. Ther. 2011, 33, 32–48. [Google Scholar] [CrossRef]
- Graziano, P.; Slavec, J.; Hart, K.; Garcia, A.; Pelham, W. Improving school readiness in preschoolers with behavior problems: Results from a summer treatment program. J. Psychopathol. Behav. Assess. 2014, 36, 555–569. [Google Scholar] [CrossRef]
- Graziano, P.A.; Hart, K. Beyond behavior modification: Benefits of social emotional/self-regulation training for preschoolers with behavior problems. J. Sch. Psychol. 2016, 58, 91–111. [Google Scholar] [CrossRef]
- Gross, D.A.; Belcher, H.M.D.; Ofonedu, M.E.; Breitenstein, S.; Frick, K.D.; Chakra, B. Study protocol for a comparative effectiveness trial of two parent training programs in a fee-for-service mental health clinic: Can we improve mental health services to low income families? Trials 2014, 15, 70. Available online: https://www.trialsjournal.com/content/15/1/70 (accessed on 15 May 2022). [CrossRef] [Green Version]
- Hart, K.C.; Graziano, P.A.; Kent, K.M.; Kuriyan, A.; Garcia, A.; Rodriguez, M.; Pelham, W.E., Jr. Early intervention for children with behavior problems in summer settings: Results from a pilot evaluation in Head Start preschools. J. Early Interv. 2016, 38, 92–117. [Google Scholar] [CrossRef]
- He, Y.; Gewirtz, A.H.; Lee, S.; August, G. Do parent preferences for child conduct problem interventions impact parenting outcomes? A pilot study in community children’s mental health settings. J. Marital. Fam. Ther. 2018, 44, 716–729. [Google Scholar] [CrossRef]
- Jones, S.; Calam, R.; Sanders, M.; Diggle, P.J.; Dempsey, R.; Sadhnani, V. A pilot web based positive parenting intervention to help bipolar parents to improve perceived parnting skills and child outcomes. Behav. Cogn. Psychother. 2014, 42, 283–296. [Google Scholar] [CrossRef] [Green Version]
- Lebowitz, E.R.; Marin, C.; Martino, A.; Shimshoni, Y.; Silverman, W.K. Parent-based treatment as efficacious as cognitive-behavioral therapy for childhood anxiety: A randomized noninferiority study of supportive parenting for anxious childhood emotions. J. Am. Acad. Child Adolesc. Psychiatry 2020, 59, 362–372. [Google Scholar] [CrossRef]
- McDonald, R.; Dodson, M.C.; Rosenfield, D.; Jouriles, E.N. Effects of a parenting intervention on features of psychopathy in children. J. Abnorm. Child Psychol. 2011, 39, 1013–1023. [Google Scholar] [CrossRef]
- McNaughton, D.B.; Cowell, J.M.; Fogg, L. Efficacy of a Latino mother-child communication intervention in elementary schools. J. Sch. Nurs. 2015, 31, 126–134. [Google Scholar] [CrossRef] [Green Version]
- Santisteban, D.A.; Czaja, S.J.; Nair, S.N.; Mena, M.P.; Tulloch, A.R. Computer informed and flexible family-based treatment for adolescents: A randomized clinical trial for at-risk racial/ethnic minority adolescents. Behav. Ther. 2017, 48, 474–489. [Google Scholar] [CrossRef]
- Sheridan, S.M.; Bovaird, J.A.; Glover, T.A.; Garbacz, S.A.; Witte, A.; Kwon, K. A randomized trial examining the effects of conjoint behavioral consultation and the mediating role of the parent-teacher relationship. Sch. Psychol. Rev. 2012, 41, 23–46. [Google Scholar] [CrossRef]
- Sheridan, S.M.; Ryoo, J.H.; Garbacz, S.A.; Kunz, G.M.; Chumney, F.L. The efficacy of conjoint behavioral consultation on parents and children in the home setting: Results of a randomized controlled trial. J. Sch. Psychol. 2013, 51, 717–733. [Google Scholar] [CrossRef] [PubMed]
- Stein, G.L.; Kulish, A.L.; Williams, C.S.; Mejia, Y.C.; Prandoni, J.I.; Thomas, K.C. Latina/o parent activation in children’s mental health treatment: The role of demographic and psychological factors. J. Lat. Psychol. 2017, 5, 290–305. [Google Scholar] [CrossRef] [Green Version]
- Eckshtain, D.; Kuppens, S.; Weisz, J.R. Amelioration of child depression through behavioral parent training: A preliminary study. J. Clin. Child Adolesc. Psychol. 2017, 46, 611–618. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Love, S.M.; Sanders, M.R.; Turner, K.M.T.; Maurange, M.; Knott, T.; Prinz, R.; Metzler, C.; Ainsworth, A.T. Social media and gamification: Engaging vulnerable parents in an online evidence-based parenting program. Child Abus. Negl. 2016, 53, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Myers, K.; Vander Stoep, A.; Lobdell, C. Feasibility of conducting a randomized controlled trial of telemental health with children diagnosed with attention-deficit/hyperactivity disorder in underserved communities. J. Child Adolesc. Psychopharmacol. 2013, 23, 372–378. [Google Scholar] [CrossRef] [Green Version]
- Pasalich, D.S.; Witkiewitz, K.; McMahon, R.J.; Pinderhughes, E.E. The Conduct Problems Prevention Research Group. Indirect effects of the fast track intervention on conduct disorder symptoms and callous-unemotional traits: Distinct pathways involving discipline and warmth. J. Abnorm. Child Psychol. 2016, 44, 587–597. [Google Scholar] [CrossRef] [Green Version]
- Villodas, M.T.; McBurnett, K.; Kaiser, N.; Rooney, M.; Pfiffner, L.J. Additive effects of parent adherence on social and behavioral outcomes of a collaborative school-home behavioral intervention for ADHD. Child Psychiatry Hum. Dev. 2014, 45, 348–360. [Google Scholar] [CrossRef] [Green Version]
- Breitenstein, S.M.; Gross, D.; Fogg, L.; Ridge, A.; Garvey, C.; Julion, W.; Tucker, S. The Chicago Parent Program: Comparing 1-year outcomes for African American and Latino parents of young children. Res. Nurs. Health 2012, 35, 475–489. [Google Scholar] [CrossRef] [Green Version]
- Dumas, J.E.; Arriaga, X.B.; Begle, A.M.; Longoria, Z.N. Child and parental outcomes of a group parenting intervention for Latino families: A pilot study of the CANNE Program. Cult. Divers. Ethn. Minor. Psychol. 2011, 17, 107–115. [Google Scholar] [CrossRef] [Green Version]
- Graziano, P.A.; Bagner, D.M.; Slavec, J.; Hungerford, G.; Kent, K.; Babinski, D.; Derefinko, K.; Pasalich, D. Feasibility of intensive parent–child interaction therapy (IPCIT): Results from an open trial. J. Psychopathol. Behav. Assess. 2015, 37, 38–49. [Google Scholar] [CrossRef] [Green Version]
- Pina, A.A.; Zerr, A.A.; Villalta, I.K.; Gonzales, N.A. Brief report: Indicated prevention and early intervention for childhood anxiety: A randomized trial with Caucasian and Hispanic/Latino youth. J. Consult. Clin. Psychol. 2012, 80, 940–946. [Google Scholar] [CrossRef]
- Stokes, J.O.; Jent, J.F.; Weinstein, A.; Davis, E.M.; Brown, T.M.; Cruz, L.; Wavering, H. Does practice make perfect? The relationship between self-reported treatment homework completion and parental skill acquisition and child behaviors. Behav. Ther. 2016, 47, 538–549. [Google Scholar] [CrossRef]
- McCabe, K.; Yeh, M.; Lau, A.; Argote, C.B. Parent-child interaction therapy for Mexican Americans: Results of a pilot randomized clinical trial at follow-up. Behav. Ther. 2012, 43, 606–618. [Google Scholar] [CrossRef]
- Weiss, B.; Han, S.; Harris, V.; Catron, T.; Ngo, V.K.; Caron, A.; Gallop, R.; Guth, C. An independent randomized clinical trial of multisystemic therapy with non-court-referred adolescents with serious conduct problems. J. Consult. Clin. Psychol. 2013, 81, 1027–1039. [Google Scholar] [CrossRef] [Green Version]
- Lau, A.S.; Fung, J.; Ho, L.; Liu, L.; Gudino, O. Parent training with high-risk imigrant Chinese families: A pilot group randomized trial yielding practice-based evidence. Behav. Ther. 2011, 42, 413–426. [Google Scholar] [CrossRef] [Green Version]
- Pfiffner, L.J.; Kaiser, N.M.; Curner, C.; Zalecki, C.; Rooney, M.; Setty, P.; McBurnett, K. From clinic to school: Translating a collaborative school-home behavioral Intervention for ADHD. Sch. Ment. Health 2011, 3, 127–142. [Google Scholar] [CrossRef]
- Bagner, D.M.; Graziano, P.A. Barriers to success in parent training for young children with developmental delay: The role of cumulative risk. Behav. Modif. 2013, 37, 356–377. [Google Scholar] [CrossRef] [Green Version]
- Chronis-Tuscano, A.; O’Brien, K.A.; Johnston, C.; Jones, H.A.; Clarke, T.L.; Raggi, V.L.; Rooney, M.E.; Diaz, Y.; Pian, J.; Seymour, K.E. The relation between maternal ADHD symptoms & improvement in child behavior following brief behavioral parent training is mediated by change in negative parenting. J. Abnorm. Child Psychol. 2011, 39, 1047–1057. [Google Scholar] [CrossRef] [Green Version]
- Chacko, A.; Gopalan, G.; Franco, L.; Dean-Assaei, K.; Jackson, J.; Marcus, S.; Hoagwood, K.; McKay, M. Multiple family group service model for children with disruptive behavior disorders: Child outcomes at post-treatment. J. Emot. Behav. Disord. 2015, 23, 67–77. [Google Scholar] [CrossRef] [Green Version]
- Carrion, V.G.; Kletter, H.; Weems, C.F.; Berry, R.R.; Rettger, J.P. Cue-centered treatment for youth exposed to interpersonal violence: A randomized controlled trial. J. Trauma. Stress 2013, 26, 654–662. [Google Scholar] [CrossRef]
- Walton, J.R.; Mautone, J.A.; Nissley-Tsiopinis, J.; Blum, N.J.; Power, T.J. Correlates of treatment engagement in an ADHD primary care-based intervention for urban families. J. Behav. Health Serv. Res. 2014, 41, 539–547. [Google Scholar] [CrossRef]
- Newington, L.; Metcalfe, A. Researchers’ and clinicians’ perceptions of recruiting participants to clinical research: A thematic meta-synthesis. J. Clin. Med. Res. 2014, 6, 162–172. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yancey, A.K.; Ortega, A.N.; Kumanyika, S.K. Effective recruitment and retention of minority research participants. Annu. Rev. Public Health 2006, 27, 1–28. [Google Scholar] [CrossRef] [Green Version]
- Haack, L.M.; Gerdes, A.C.; Lawton, K.E. Conducting research with Latino families: Examination of strategies to improve recruitment, retention, and satisfaction with an at-risk and underserved population. J. Child Fam. Stud. 2014, 23, 410–421. [Google Scholar] [CrossRef]
- Zamora, I.; Williams, M.E.; Higareda, M.; Wheeler, B.Y.; Levitt, P. Brief report: Recruitment and retention of minority children for autism research. J. Autism Dev. Disord. 2016, 46, 698–703. [Google Scholar] [CrossRef] [PubMed]
- Wetherby, A.M.; Guthrie, W.; Woods, J.; Schatschneider, C.; Holland, R.D.; Morgan, L.; Lord, C. Parent implemented social intervention for toddlers with autism: An RCT. Pediatrics 2014, 134, 1084–1093. [Google Scholar] [CrossRef] [Green Version]
- Powers, L.E. Contributing meaning to research in developmental disabilities: Integrating participatory action and methodological rigor. Res. Pract. Pers. Sev. Disabil. 2017, 42, 42–52. [Google Scholar] [CrossRef]
- Cornwall, A.; Jewkes, R. What is participatory research? Soc. Sci. Med. 1995, 41, 1667–1676. [Google Scholar] [CrossRef]
- Fletcher-Watson, S.; Adams, J.; Brook, K.; Charman, T.; Crane, L.; Cusack, J.; Leekam, S.; Milton, D.; Parr, J.R.; Pellicano, E. Making the future together: Shaping autism research through meaningful participation. Autism 2019, 23, 942–953. [Google Scholar] [CrossRef]
- Long, J.; Panese, J.; Ferguson, J.; Hamill, M.A.; Miller, J. Enabling voice and participation in autism services: Using practitioner research to develop inclusive practice. Good Autism Pract. 2017, 18, 6–14. [Google Scholar]
- Anderson, C.M.; Smith, T.; Iovannone, R. Building capacity to support students with autism spectrum disorder: A modular approach to intervention. Educ. Treat. Child. 2018, 41, 107–137. [Google Scholar] [CrossRef]
- Smith, T.; Iadarola, S.; Mandell, D.S.; Harwood, R.; Kasari, C. Community-partnered research with urban school districts that serve children with autism spectrum disorder. Acad. Pediatr. 2017, 17, 614–619. [Google Scholar] [CrossRef]
- Croen, L.A.; Shankute, N.; Davignon, M.; Massolo, M.L.; Yoshida, C. Demographic and clinical characteristics associated with engagement in behavioral health treatment among children with autism spectrum disorders. J. Autism Dev. Disord. 2017, 47, 3347–3357. [Google Scholar] [CrossRef] [Green Version]
- Dumas, J.E.; Wolf, L.C.; Fisman, S.N.; Culligan, A. Parenting stress, child behavior problems, and dysphoria in parents of children with autism, down syndrome, behavior disorders, and normal development. Except. Spec. Educ. J. 1991, 2, 97–110. [Google Scholar] [CrossRef]
- Stuart, M.; McGrew, J.H. Caregiver burden after receiving a diagnosis of an autism spectrum disorder. Res. Autism Spectr. Disord. 2009, 3, 86–97. [Google Scholar] [CrossRef]
- Shine, R.; Perry, A. Brief report: The relationship between parental stress and intervention outcome of children with autism. J. Dev. Disabil. 2010, 16, 64–66. [Google Scholar]
- Raulston, T.J.; Hieneman, M.; Caraway, N.; Pennefather, J.; Bhana, N. Enablers of behavioral parent training for families of children with autism spectrum disorder. J. Child Fam. Stud. 2019, 28, 693–703. [Google Scholar] [CrossRef]
- Coard, S.I.; Wallace, S.A.; Stevenson, H.C., Jr.; Brotman, L.M. Towards culturally relevant preventive interventions: The consideration of racial socialization in parent training with African American families. J. Child Fam. Stud. 2004, 13, 277–293. [Google Scholar] [CrossRef]
- Forehand, R.; Kotchick, B.A. Behavioral parent training: Current challenges and potential solutions. J. Child Fam. Stud. 2002, 11, 377–384. [Google Scholar] [CrossRef]
- Lau, A.S. Making the case for selective and directed cultural adaptations of evidence-based treatments: Examples from parent training. Clin. Psychol. Sci. Pract. 2006, 13, 295–310. [Google Scholar] [CrossRef] [Green Version]
- McCabe, K.M.; Yeh, M.; Garland, A.F.; Lau, A.S.; Chavez, G. The GANA program: A tailoring approach to adapting parent–child interaction therapy for Mexican Americans. Educ. Treat. Child. 2005, 28, 111–129. Available online: https://www.jstor.org/stable/42899836 (accessed on 15 May 2022).
- Gopalan, G.; Chacko, A.; Franco, L.; Dean-Assael, K.M.; Rotko, L.E.; Marcus, S.M.; Hoagwood, K.E.; McKay, M.M. Multiple family groups for children with disruptive behavior disorders: Child outcomes at 6-month follow-up. J. Child Fam. Stud. 2015, 24, 2721–2733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoagwood, K.E.; Cavaleri, M.A.; Olin, S.S.; Burns, B.J.; Slaton, E.; Gruttadaro, D.; Hughes, R. Family support in children’s mental health: A review and synthesis. Clin. Child Fam. Psychol. Rev. 2010, 13, 1–45. [Google Scholar] [CrossRef] [PubMed]
- Jamison, J.M.; Fourie, E.; Siper, P.M.; Trelles, M.P.; George-Jones, J.; Grice, A.B.; Krata, J.; Holl, E.; Shaoul, J.; Hernandez, B.; et al. Examining the efficacy of a family peer advocate model for Black and Hispanic caregivers of children with autism spectrum disorder. J. Autism Dev. Disord. 2017, 47, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- McKay, M.M.; Gopalan, G.; Franco, L.; Dean-Assael, K.; Chacko, A.; Jackson, J.M.; Fuss, A. A collaboratively designed child mental health service model: Multiple family groups for urban children with conduct difficulties. Res. Soc. Work. Pract. 2011, 21, 664–674. [Google Scholar] [CrossRef] [Green Version]
- Flores, G.; Fuentes-Afflick, E.; Barbot, O.; Carter-Pokras, O.; Claudio, L.; Lara, M.; Weitzman, M. The health of Latino children: Urgent priorities, unanswered questions, and a research agenda. J. Am. Med. Assoc. 2002, 288, 82–90. [Google Scholar] [CrossRef]
- Wendler, D.; Kington, R.; Madans, J.; Van Wye, G.; Christ-Schmidt, H.; Pratt, L.A.; Brawley, O.W.; Gross, C.P.; Emanuel, E. Are racial and ethnic minorities less willing to participate in health research? PLoS Med. 2005, 3, e19. [Google Scholar] [CrossRef] [Green Version]
- Tran, A.G. Family contexts: Parental experiences of discrimination and child mental health. Am. J. Community Psychol. 2014, 53, 37–46. [Google Scholar] [CrossRef]
- Lorenzo-Blanco, E.I.; Meca, A.; Unger, J.B.; Romero, A.; Szapocznik, J.; Piña-Watson, B.; Cano, M.Á.; Zamboanga, B.L.; Baezconde-Garbanati, L.; Des Rosiers, S.E.; et al. Longitudinal effects of Latino parent cultural stress, depressive symptoms, and family functioning on youth emotional well-being and health risk behaviors. Fam. Process 2017, 56, 981–996. [Google Scholar] [CrossRef]
- Shedlin, M.G.; Decena, C.U.; Mangadu, T.; Martinez, A. Research participant recruitment in Hispanic communities: Lessons learned. J. Immigr. Minor. Health 2011, 13, 352–360. [Google Scholar] [CrossRef]
- Cole, E.R. Intersectionality and research in psychology. Am. Psychol. 2009, 64, 170–180. [Google Scholar] [CrossRef] [Green Version]
- Crenshaw, K. Race, reform and retrenchment: Transformation and legitimation in anti discrimination law. Harv. Law Rev. 1988, 101, 1331–1387. Available online: https://www.jstor.org/stable/1341398 (accessed on 15 May 2022). [CrossRef]
- Rogers, J.; Kelly, U.A. Feminist intersectionality: Bringing social justice to health disparities research. Nurs. Ethics 2011, 18, 397–407. [Google Scholar] [CrossRef]
- Corbie-Smith, G.; Miller, W.C.; Ransohoff, D.F. Interpretations of ‘appropriate’ minority inclusion in clinical research. Am. J. Med. 2004, 116, 249–252. [Google Scholar] [CrossRef]


{kind=link}
| Demographic Characteristic | n | Percentage of Studies |
|---|---|---|
| Participant age | ||
| Birth—2 years old | 6 | 18% |
| 3–6 years old | 24 | 73% |
| 7 years old and older | 25 | 76% |
| Ethnicity | ||
| White | 24 | 73% |
| Black or African American | 19 | 58% |
| Hispanic or Latino/a | 17 | 52% |
| Bi- or multi-racial | 13 | 39% |
| Other | 8 | 24% |
| Native American or American Indian | 6 | 18% |
| Asian | 5 | 15% |
| Non-Hispanic | 4 | 12% |
| Not reported | 2 | 6% |
| Non-white | 1 | 3% |
| Socioeconomic status | ||
| Indicators of low- or under-resourced families | 20 | 61% |
| Not reported or cannot be determined | 11 | 33% |
| Retention Strategies | |||||||
|---|---|---|---|---|---|---|---|
| Recruitment Strategies | Money or Gift Cards | Free Services or Childcare | Educational Materials | Flexible Scheduling | Reminders | Choice of Intervention | Not Reported |
| School | 8 | 3 | 2 | 1 | 1 | 4 | |
| Direct referral | 3 | 3 | 1 | 1 | 1 | 1 | 8 |
| Community agencies or setting | 5 | 3 | 1 | 1 | 2 | 5 | |
| Physicians or service providers | 4 | 3 | 1 | 1 | 1 | 5 | |
| Flyers or mailings | 6 | 1 | 2 | 1 | 5 | ||
| Workshops or open house | 2 | 1 | |||||
| Self-referral | 1 | 2 | 4 | ||||
| Trusted person | 2 | 1 | 1 | 1 | |||
| Word-of-mouth | 3 | 1 | 1 | ||||
| Radio or newspaper | 2 | 1 | |||||
| University clinic or faculty | 1 | 1 | 1 | ||||
| Online or social media | 2 | ||||||
| Child Protective Services | 1 | ||||||
| Not reported | 1 | 1 | 1 | 2 | 2 | ||
| Reason | Study n | Participant n |
|---|---|---|
| Not reported | 18 | 394 (77%) |
| Withdrew consent | 5 | 11 (2%) |
| Relocation | 6 | 35 (7%) |
| Lost or could not contact (e.g., disconnected phone, unreturned communication attempts) | 3 | 35 (7%) |
| Medication or medical conflicts | 3 | 11 (2%) |
| Transportation | 2 | 3 (1%) |
| Family reasons | 1 | 3 (1%) |
| Perceived lack of need | 1 | 11 (2%) |
| Teacher refused | 1 | 3 (1%) |
| Recruitment Strategy | Definition | Exemplar Article |
|---|---|---|
| School referral | School personnel involved in recruitment (referral or direct involvement | 60 |
| Community agency | Community agency (physician, early childhood provided, mental health, etc.) involved in recruitment (referral or other) | 39 |
| Direct referral | Community provider directly refers a participant to the researcher | 35 |
| Self-referral | Families contact the researcher directly | 61 |
| Flyers | Posted, mailed, e-mailed, or handed out in person | 49 |
| Community setting/outreach | Face-to-face outreach in community settings that provide leisure or recreation services | 37 |
| Radio or TV advertisements | Advertisements created for radio or television mediums | 35 |
| Retention Strategy | Exemplar Study | Studies n |
|---|---|---|
| Money | 62 | 19 |
| Flexible scheduling | 63 | 8 |
| Childcare | 53 | 6 |
| Gift card | 64 | 6 |
| Reminder | 48 | 6 |
| Educational materials | 37 | 6 |
| Food | 32 | 3 |
| Motivational interviewing Choice of intervention | 65 38 | 1 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Machalicek, W.; Glugatch, L.; Erturk, B.; Brafford, T.; Kunze, M.; Drew, C.; Douglas, A.; Storie, S.; Crowe, R.; Magaña, S. Recommendations for Diversifying Racial and Ethnic Representation in Autism Intervention Research: A Crossover Review of Recruitment and Retention Practices in Pediatric Mental Health. J. Clin. Med. 2022, 11, 6468. https://doi.org/10.3390/jcm11216468
Machalicek W, Glugatch L, Erturk B, Brafford T, Kunze M, Drew C, Douglas A, Storie S, Crowe R, Magaña S. Recommendations for Diversifying Racial and Ethnic Representation in Autism Intervention Research: A Crossover Review of Recruitment and Retention Practices in Pediatric Mental Health. Journal of Clinical Medicine. 2022; 11(21):6468. https://doi.org/10.3390/jcm11216468
Chicago/Turabian StyleMachalicek, Wendy, Lindsay Glugatch, Buket Erturk, Tasia Brafford, Megan Kunze, Christine Drew, Allaina Douglas, Sloan Storie, Rebecca Crowe, and Sandy Magaña. 2022. "Recommendations for Diversifying Racial and Ethnic Representation in Autism Intervention Research: A Crossover Review of Recruitment and Retention Practices in Pediatric Mental Health" Journal of Clinical Medicine 11, no. 21: 6468. https://doi.org/10.3390/jcm11216468