
Hidden Unstable Flap Should Be Suspected in Treating Intractable Pain from Medial Meniscus Horizontal Tear

1
Department of Orthopedic Surgery, Chungnam National University Hospital, Chungnam National University College of Medicine, Daejeon 35015, Korea
2
Department of Orthopedic Surgery, Chungnam National University Sejong Hospital, Chungnam National University College of Medicine, Sejong 30099, Korea
*
Author to whom correspondence should be addressed.
J. Clin. Med. 2022, 11(21), 6245; https://doi.org/10.3390/jcm11216245
Submission received: 21 September 2022
/
Revised: 17 October 2022
/
Accepted: 21 October 2022
/
Published: 23 October 2022
(This article belongs to the Section Orthopedics)
Abstract
:(1) Background: The medial meniscus horizontal tear (MMHT) is known as a lesion that can be treated nonoperatively. However, some patients show persistent pain despite conservative treatments. In arthroscopic surgery for MMHT, surgeons often encounter unexpected unstable flaps, which can explain the intractable pain. This study aimed to determine whether preoperative factors could predict the hidden unstable flaps in MMHT. (2) Materials and Methods: Medical records of 65 patients who underwent arthroscopic partial meniscectomy (APM) for isolated MMHT during 2016–2020 were retrospectively reviewed. APM was indicated when there was no severe chondral degeneration and intractable localized knee pain in the medial compartment did not resolve despite conservative treatments. Unstable flap was confirmed based on arthroscopic images and operation notes. Each of the following preoperative factors were investigated using logistic regression analyses to determine whether they can predict an unstable flap: age, sex, body mass index, lower limb alignment, trauma history, mechanical symptoms, symptom duration, visual analogue scale (VAS), Lysholm score, cartilage wear of the medial compartment, and subchondral bone marrow lesion (BML). (3) Results: Hidden unstable flaps were noted in 45 (69.2%) patients. Based on univariate analyses for each preoperative factor, age, symptom duration, cartilage wear (of the femoral condyle and the tibial plateau), and subchondral BML were included in the multivariate logistic regression analysis. The results showed that symptom duration (p = 0.026, odds ratio = 0.99) and high-grade cartilage wear of the medial femoral condyle (p = 0.017, odds ratio = 0.06) were negatively associated with unstable flaps. A receiver operating characteristic curve was used to calculate the symptom duration at which the prediction of unstable flaps was maximized, and the cutoff point was 14.0 months. (4) Conclusions: More than two thirds of patients suffering intractable pain from MMHT had hidden unstable flaps. However, APM should not be considered when the symptom duration is more than 14 months or high-grade cartilage wear of the medial femoral condyle is noted.
1. Introduction
The paradigm has been shifted from “If it is torn, take it out!” to “Save the meniscus!” in the treatment of meniscal tear [1,2]. Several randomized controlled studies showed that arthroscopic partial meniscectomy (APM) had no clinical advantage over conservative treatments [3,4,5,6,7,8]. In particular, the medial meniscus horizontal tear (MMHT) is regarded as a degenerative lesion that should be addressed in a non-surgical approach [6,9,10]. However, not every patient with MMHT can be treated with non-steroidal anti-inflammatory drugs and muscle strengthening exercises. The randomized trials questioning the efficacy of APM included only a subset of patients who responded to conservative treatments [11]. If MMHT is not accompanied by severe chondral degeneration and pain that is not relieved despite conservative treatments, APM is a remaining option to resolve the intractable pain.
Some previous studies found that APM was more effective in patients with mechanical symptoms than in those without these symptoms [12,13]. The meniscal flap, being lodged between the femoral condyle and the tibia plateau, has been recognized as a lesion inducing mechanical symptoms [14,15,16]. However, the unstable flap is often difficult to discern on MRI scans [17,18] and is not detected during arthroscopy unless it is probed using a hook [19,20]. The hidden flap might be the reason that conservative treatments fail in some cases of MMHT.
Recent studies attempted to identify a subgroup of patients who could show particularly favorable surgical outcomes after APM [21,22]. If surgeons preoperatively distinguish between those who would benefit from APM and those who would not, unnecessary surgery could be avoided and the outcomes of APM will be improved. Moreover, there is a growing interest in the arthroscopic repair of MMHT [23,24]. Predicting unstable flaps is closely related to surgical indications. Thus, this study reviewed patients complaining of intractable pain from MMHT that necessitated APM. The incidence of hidden meniscal flaps was investigated and the preoperative predictive factors for the hidden unstable flaps were identified. It was hypothesized that certain preoperative factors differ according to the unstable meniscal flap, which was confirmed based on the arthroscopic findings.
2. Materials and Methods
Medical records of 65 patients who underwent APM for isolated MMHT during 2016–2021 were retrospectively reviewed after approval was obtained from the institutional review board of Chungnam National University Hospital (No. 2022-05-075). Patients with a discernable meniscal flap on preoperative magnetic resonance imaging (MRI) scans were not included in this study. The exclusion criteria also included combined ligament injury, lateral meniscus tear, and previous knee surgery. APM was indicated when intractable localized knee pain in the medial compartment did not resolve despite conservative treatments, such as non-steroidal anti-inflammatory drugs and muscle strengthening exercises. Patients showing severe medial OA on radiographs (Kellgren–Lawrence grade ≥ 3) were not deemed suitable for APM.
All APMs were performed by a single senior surgeon. Arthroscopic findings were documented as photos, videos, and intraoperative notes. To resolve mechanical symptoms such as catching, locking, and pain during squatting, the displaceable meniscal flap and unstable superior or inferior leaves of MMHT were resected, while, at the same time, every effort was made to preserve intact meniscal tissue. No patient underwent subtotal or total meniscectomy. Full range of motion and muscle strengthening exercises were encouraged immediately after surgery.
2.1. Study Design
The unstable flap was confirmed on arthroscopic images and operation notes (Figure 1). An unstable flap was defined based on the ISAKOS classification: <3 mm displacement on arthroscopic probing [25]. The patients were divided into a flap group and non-flap group. To identify predictive factors for unstable flaps, the following factors were investigated: age, sex, body mass index (BMI), lower limb alignment, trauma history, mechanical symptoms, symptom duration (from the onset of symptoms to surgery), visual analogue scale (VAS), Lysholm score, cartilage wear of the medial compartment, and subchondral bone marrow lesion (BML). For the alignment, varus and valgus mechanical alignments were defined as positive and negative, respectively. The cartilage wear in the medial femoral condyle and the medial tibial plateau was separately assessed on MRI scans according to the Yulish grading system: grade 0, normal; grade 1, normal cartilage contour with abnormal signal; grade 2, superficial fraying, erosion, or ulceration of <50%; grade 3, partial-thickness defect of >50%; and grade 4, full-thickness defect [26]. High-grade cartilage wear was deemed as that of ≥grade 3 [27]. Subchondral BML was defined as a locus of increased signal in the subchondral area with internal trabecular marrow in it [28]. The presence of subchondral BML was investigated on MRI scans. The evaluation of the unstable flap, cartilage wear, and subchondral BML was independently performed by three orthopedic surgeons, and all disagreements were resolved by discussion.
2.2. Statistical Analysis
Predictive factors for unstable flaps were identified using logistic regression analyses. Univariate analyses for each factor were performed first; thereafter, a multivariate regression analysis was conducted to avoid overfitting problems. Between the flap group and the non-flap group, categorical variables were analyzed by Chi-square test when the expected value of the cell was 5 or more in at least 80% of the cells; otherwise, Fisher exact test was used. Continuous variables were analyzed by t-test. When continuous variables were found to be significant factors in the multivariate regression analysis, a receiver operating characteristic curve (ROC) was used to obtain the cutoff point at which the sensitivity and the specificity for the unstable flap were maximized. All statistical analyses were performed using R software version 4.1.1 (R foundation for Statistical Computing, Vienna, Austria), with a p value < 0.05 considered statistically significant.
3. Results
Of 65 patients with a mean age of 52.2 ± 12.6 years (range, 18–75 years), hidden unstable flaps were noted in 45 (69.2%) patients. The mean symptom duration was 13.0 ± 5.8 weeks. The flap group and the non-flap group showed significant differences in age, symptom duration, cartilage wear of the femoral condyle and the tibial plateau, and subchondral BML. The patient characteristics among the groups are summarized in Table 1.
Logistic Regression Analyses Regarding Unstable Flap
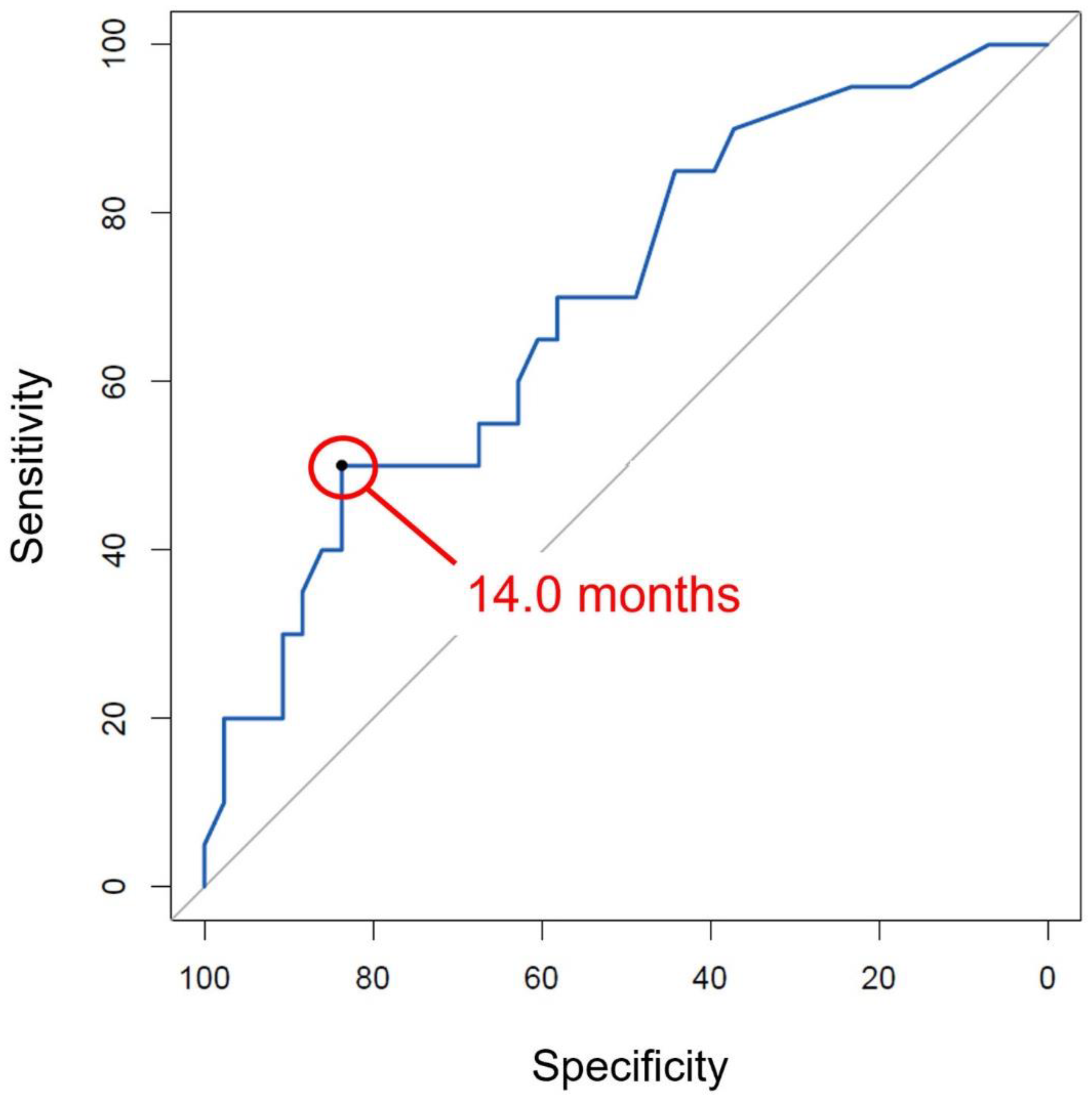
Based on univariate analyses, age, symptom duration, cartilage wear of the femoral condyle and the tibial plateau, and subchondral BML were included in a multivariate logistic regression analysis. The results showed that symptom duration (p = 0.026, odds ratio = 0.99) and high-grade cartilage wear of the medial femoral condyle (p = 0.017, odds ratio = 0.06) were negatively associated with an unstable flap (Table 2). An ROC curve was used to calculate the symptom duration at which the sensitivity and the specificity for unstable flaps were maximized (Figure 2), and the cutoff point was 14.0 months, with the area under curve being 0.70 (sensitivity, 50.0%; specificity, 83.7%).
4. Discussion
The most important findings of the present study were that (1) approximately 70% of patients suffering intractable pain had hidden unstable flaps that would have been lodged and could be a source of pain, and (2) the symptom duration and cartilage wear of the medial femoral condyle had negative correlations with unstable flaps. Pain was not likely from an unstable flap if the symptom duration was more than 14 months or high-grade cartilage wear of the femoral condyle was noted on preoperative MRI scans.
MMHT usually occurs in middle-aged patients as a degenerative lesion without a definite trauma history [29,30]. The tear dividing the meniscus into the upper and the lower leaves is often asymptomatic, and, if pain occurs, the patient responds well to conservative treatments [6,31]. When the stable leaf receiving additional damage develops an unstable flap, APM will be required [9,18]. Recently, arthroscopic repair was also considered as a reliable option in treating MMHT because the benefit of meniscal repair had been documented [23,32]. However, it is not always possible to confirm the unstable flap on MRI scans [17,18]. Identification of the predictive factors for unstable flaps can help surgeons to determine the necessity of APM before several months of conservative treatments fail. In their recent study based on the Knee Arthroscopy Cohort of Southern Denmark, Pihl et al. tried to identify a subgroup of patients who would benefit from APM. Although they investigated a number of preoperative factors, including patient demographics and knee-related symptoms, the predictive performance of the prognostic model was poor [21]. Noorduyn et al. also found that there was no clear subgroup of patients who would benefit from either surgery or physical therapy for a degenerative meniscal tear [22].
This study found two significant factors in the logistic regression analysis regarding unstable flaps: symptom duration and cartilage wear of the femoral condyle. Kim et al. also reported similar results on symptom duration [9]. They found that patients with flap tears had a shorter symptom duration to surgery than those without a flap tear (6 months vs. 22 months). However, they did not find a significant difference in the severity of osteoarthritis on plain radiographs (Kellgren–Lawrence grade) according to flap tear. In the present study, the cartilage status of the medial compartment was assessed based on MRI scans, and high-grade cartilage wear of the femoral condyle had a negative correlation with unstable flaps. Thus, the mechanical symptoms of the non-flap group were likely to result from the complex process of osteoarthritis [33].
It is noteworthy that mechanical symptoms and the severity of pain (VAS) did not differ significantly between the flap group and the non-flap group. Because a displaced flap can lead to mechanical symptoms that require arthroscopic management [14,15,16], mechanical symptoms and a positive McMurray test considerably influence a surgeon’s decision to recommend APM [11]. However, they were not useful in predicting unstable flaps. The severity of pain was not a predictive factor either. Regarding this, van de Graaf et al. performed an interesting investigation based on a survey of 194 orthopedic surgeons [34]. Each surgeon was informed about patient profiles, including pain score, the results of physical examination, and the type of meniscal tear. In predicting the outcome of APM, experienced knee surgeons were not better than other orthopedic surgeons. Clinical symptoms were not reliable criteria for deciding whether to use APM.
Several limitations should be noted. First, patients who had conservative treatments for MMHT were not included in this study. The necessity of APM would have been determined better if these patients had been included. Second, patients who underwent APM for MMHT were relatively rare, which made it difficult to attain a large number of patients in this study. The small sample size would compromise the statistical power. Third, this study failed to identify positive predictive factors for unstable flaps. The two significant factors (symptom duration and cartilage wear) were negatively correlated with unstable flaps. Thus, preoperative factors that support the necessity of APM are not revealed.
5. Conclusions
More than two thirds of patients suffering intractable pain from MMHT had hidden unstable flaps. However, APM should not be considered when the symptom duration is more than 14 months or high-grade cartilage wear of the medial femoral condyle is noted.
Author Contributions
Y.M.K.: writing, review and editing. Y.B.J.: supervision. B.K.A.: data gathering. J.-H.S.: writing, data gathering, statistical analysis, conceptualization. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the research fund of Chungnam National University.
Institutional Review Board Statement
This retrospective study was conducted in accordance with the ethical standards of the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Approval for this study was obtained from the institutional review board of Chungnam National University Hospital (No. 2022-05-075).
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Beaufils, P.; Pujol, N. Management of traumatic meniscal tear and degenerative meniscal lesions. Save the meniscus. Orthop Traumatol. Surg. Res. 2017, 103, S237–S244. [Google Scholar] [CrossRef] [PubMed]
- Abram, S.G.F.; Hopewell, S.; Monk, A.P.; Bayliss, L.E.; Beard, D.J.; Price, A.J. Arthroscopic partial meniscectomy for meniscal tears of the knee: A systematic review and meta-analysis. Br. J. Sports Med. 2020, 54, 652–663. [Google Scholar] [CrossRef] [PubMed]
- Herrlin, S.V.; Wange, P.O.; Lapidus, G.; Hållander, M.; Werner, S.; Weidenhielm, L. Is arthroscopic surgery beneficial in treating non-traumatic, degenerative medial meniscal tears? A five year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2013, 21, 358–364. [Google Scholar] [CrossRef] [PubMed]
- Katz, J.N.; Brophy, R.H.; Chaisson, C.E.; de Chaves, L.; Cole, B.J.; Dahm, D.L.; Donnell-Fink, L.A.; Guermazi, A.; Haas, A.K.; Jones, M.H.; et al. Surgery versus physical therapy for a meniscal tear and osteoarthritis. N. Engl. J. Med. 2013, 368, 1675–1684. [Google Scholar] [CrossRef] [Green Version]
- Kise, N.J.; Risberg, M.A.; Stensrud, S.; Ranstam, J.; Engebretsen, L.; Roos, E.M. Exercise therapy versus arthroscopic partial meniscectomy for degenerative meniscal tear in middle aged patients: Randomised controlled trial with two year follow-up. BMJ 2016, 354, i3740. [Google Scholar] [CrossRef] [Green Version]
- Yim, J.-H.; Seon, J.-K.; Song, E.-K.; Choi, J.-I.; Kim, M.-C.; Lee, K.-B.; Seo, H.-Y. A Comparative study of meniscectomy and nonoperative treatment for degenerative horizontal tears of the medial meniscus. Am. J. Sports Med. 2013, 41, 1565–1570. [Google Scholar] [CrossRef]
- van de Graaf, V.A.; Noorduyn, J.C.A.; Willigenburg, N.W.; Butter, I.K.; de Gast, A.; Mol, B.W.; Saris, D.B.F.; Twisk, J.W.R.; Poolman, R.W.; ESCAPE Research Group. Effect of early surgery vs physical therapy on knee function among patients with nonobstructive meniscal tears: The ESCAPE randomized clinical trial. JAMA 2018, 320, 1328–1337. [Google Scholar] [CrossRef] [Green Version]
- Thorlund, J.B.; Juhl, C.B.; Roos, E.M.; Lohmander, L.S. Arthroscopic surgery for degenerative knee: Systematic review and meta-analysis of benefits and harms. BMJ 2015, 350, h2747. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.G.; Lee, S.-Y.; Chay, S.; Lim, H.C.; Bae, J.-H. Arthroscopic meniscectomy for medial meniscus horizontal cleavage tears in patients under age 45. Knee Surg. Relat. Res 2016, 28, 225–232. [Google Scholar] [CrossRef] [Green Version]
- Noorduyn, J.C.A.; van de Graaf, V.A.; Willigenburg, N.W.; Scholten-Peeters, G.G.M.; Kret, E.J.; van Dijk, R.A.; Buchbinder, R.; Hawker, G.A.; Coppieters, M.W.; Poolman, R.W.; et al. Effect of physical therapy vs arthroscopic partial meniscectomy in people with degenerative meniscal tears: Five-year follow-up of the ESCAPE randomized clinical Trial. JAMA Netw. Open 2022, 5, e2220394. [Google Scholar] [CrossRef] [PubMed]
- Lyman, S.; Oh, L.S.; Reinhardt, K.R.; Mandl, L.A.; Katz, J.N.; Levy, B.A.; Marx, R.G. Surgical decision making for arthroscopic partial meniscectomy in patients aged over 40 years. Arthroscopy 2012, 28, 492–501.e1. [Google Scholar] [CrossRef] [PubMed]
- Jevsevar, D.S.; Yates, A.J.; Sanders, J.O. Arthroscopic partial meniscectomy for degenerative meniscal tear. N. Engl. J. Med. 2014, 370, 1260. [Google Scholar] [CrossRef] [PubMed]
- Krych, A.J.; Carey, J.L.; Marx, R.G.; Dahm, D.L.; Sennett, B.J.; Stuart, M.J.; Levy, B.A. Does arthroscopic knee surgery work? Arthroscopy 2014, 30, 544–545. [Google Scholar] [CrossRef] [PubMed]
- Lefevre, N.; Klouche, S.; Sezer, H.B.; Gerometta, A.; Bohu, Y.; Lefevre, E. The “sleeper’s sign” is valid and suggestive of a medial sub-meniscal flap tear. Knee Surg. Sports Traumatol. Arthrosc. 2021, 29, 51–58. [Google Scholar] [CrossRef]
- Herschmiller, T.A.; Anderson, J.A.; Garrett, W.E.; Taylor, D.C. The trapped medial meniscus tear: An examination maneuver helps predict arthroscopic findings. Orthop. J. Sports Med. 2015, 3, 2325967115583954. [Google Scholar] [CrossRef] [Green Version]
- Becker, R.; Bernard, M.; Scheffler, S.; Kopf, S. Treatment of degenerative meniscal lesions: From eminence to evidence-based medicine. Orthopade 2017, 46, 808–821. [Google Scholar] [CrossRef]
- Vande Berg, B.C.; Malghem, J.; Poilvache, P.; Maldague, B.; Lecouvet, F.E. Meniscal Tears with fragments displaced in notch and recesses of knee: MR imaging with arthroscopic comparison. Radiology 2005, 234, 842–850. [Google Scholar] [CrossRef]
- Lance, V.; Heilmeier, U.R.; Joseph, G.B.; Steinbach, L.; Ma, B.; Link, T.M. MR imaging characteristics and clinical symptoms related to displaced meniscal flap tears. Skeletal Radiol. 2015, 44, 375–384. [Google Scholar] [CrossRef]
- Davis, K.W.; Rosas, H.G.; Graf, B.K. Magnetic resonance imaging and arthroscopic appearance of the menisci of the knee. Clin. Sports Med. 2013, 32, 449–475. [Google Scholar] [CrossRef]
- Lecas, L.K.; Helms, C.A.; Kosarek, F.J.; Garret, W.E. Inferiorly displaced flap tears of the medial meniscus: MR appearance and clinical significance. AJR Am. J. Roentgenol. 2000, 174, 161–164. [Google Scholar] [CrossRef]
- Pihl, K.; Ensor, J.; Peat, G.; Englund, M.; Lohmander, S.; Jørgensen, U.; Nissen, N.; Fristed, J.V.; Thorlund, J.B. Wild goose chase—No predictable patient subgroups benefit from meniscal surgery: Patient-reported outcomes of 641 patients 1 year after surgery. Br. J. Sports Med. 2020, 54, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Noorduyn, J.C.A.; van de Graaf, V.A.; Willigenburg, N.W.; Scholten-Peeters, G.G.M.; Mol, B.W.; Heymans, M.W.; Coppieters, M.W.; Poolman, R.W.; ESCAPE Research Group. An individualized decision between physical therapy or surgery for patients with degenerative meniscal tears cannot be based on continuous treatment selection markers: A marker-by-treatment analysis of the ESCAPE study. Knee Surg. Sports Traumatol. Arthrosc. 2022, 30, 1937–1948. [Google Scholar] [CrossRef] [PubMed]
- Zhu, S.; Li, X.; Lu, Z.; Koh, J.L.; Wang, C.; Wang, P.; Shao, X.; Wang, J. Arthroscopic repair of degenerative medial meniscus tears in patients aged over 45 years resulted in favorable clinical outcomes and low clinical failure rates at a minimum 2-year follow-up. Knee Surg. Sports Traumatol. Arthrosc. 2022. preprint. [Google Scholar] [CrossRef] [PubMed]
- Ogawa, H.; Matsumoto, K.; Sengoku, M.; Yoshioka, H.; Akiyama, H. Arthroscopic repair of horizontal cleavage meniscus tears provides good clinical outcomes in spite of poor meniscus healing. Knee Surg. Sports Traumatol. Arthrosc. 2020, 28, 3474–3480. [Google Scholar] [CrossRef]
- Wadhwa, V.; Omar, H.; Coyner, K.; Khazzam, M.; Robertson, W.; Chhabra, A. ISAKOS classification of meniscal tears-illustration on 2D and 3D isotropic spin echo MR imaging. Eur. J. Radiol. 2016, 85, 15–24. [Google Scholar] [CrossRef]
- Yulish, B.S.; Montanez, J.; Goodfellow, D.B.; Bryan, P.J.; Mulopulos, G.P.; Modic, M.T. Chondromalacia patellae: Assessment with MR imaging. Radiology 1987, 164, 763–766. [Google Scholar] [CrossRef]
- Song, J.-H.; Bin, S.-I.; Kim, J.-M.; Lee, B.-S. Cartilage status, rather than chronologic age, determines the outcomes of open wedge high tibial osteotomy: A cartilage status-matched cohort study. Arthroscopy 2021, 37, 2915–2922. [Google Scholar] [CrossRef]
- Peterfy, C.G.; Guermazi, A.; Zaim, S.; Tirman, P.F.J.; Miaux, Y.; White, D.; Kothari, M.; Lu, Y.; Fye, K.; Zhao, S.; et al. Whole-Organ Magnetic Resonance Imaging Score (WORMS) of the knee in osteoarthritis. Osteoarthr. Cartil. 2004, 12, 177–190. [Google Scholar] [CrossRef] [Green Version]
- Beaufils, P.; Becker, R.; Kopf, S.; Englund, M.; Verdonk, R.; Ollivier, M.; Seil, R. Surgical management of degenerative meniscus lesions: The 2016 ESSKA meniscus consensus. Knee Surg. Sports Traumatol. Arthrosc. 2017, 25, 335–346. [Google Scholar] [CrossRef] [Green Version]
- Christoforakis, J.; Pradhan, R.; Sanchez-Ballester, J.; Hunt, N.; Strachan, R.K. Is there an association between articular cartilage changes and degenerative meniscus tears? Arthroscopy 2005, 21, 1366–1369. [Google Scholar] [CrossRef]
- Englund, M. Meniscal tear—A feature of osteoarthritis. Acta Orthop. Scand. Suppl. 2004, 75, 1–45. [Google Scholar] [PubMed] [Green Version]
- Beamer, B.S.; Walley, K.C.; Okajima, S.; Manoukian, O.S.; Perez-Viloria, M.; DeAngelis, J.P.; Ramappa, A.J.; Nazarian, A. Changes in contact area in meniscus horizontal cleavage tears subjected to repair and resection. Arthroscopy 2017, 33, 617–624. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharyya, T.; Gale, D.; Dewire, P.; Totterman, S.; Gale, M.E.; McLaughlin, S.; Einhorn, T.A.; Felson, D.T. The clinical importance of meniscal tears demonstrated by magnetic resonance imaging in osteoarthritis of the knee. J. Bone Joint Surg. Am. 2003, 85, 4–9. [Google Scholar] [CrossRef]
- van de Graaf, V.A.; Bloembergen, C.H.; Willigenburg, N.W.; Noorduyn, J.C.A.; Saris, D.B.; Harris, I.A.; Poolman, R.W.; ESCAPE Research Group. Can even experienced orthopaedic surgeons predict who will benefit from surgery when patients present with degenerative meniscal tears? A survey of 194 orthopaedic surgeons who made 3880 predictions. Br. J. Sports Med. 2020, 54, 354–359. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
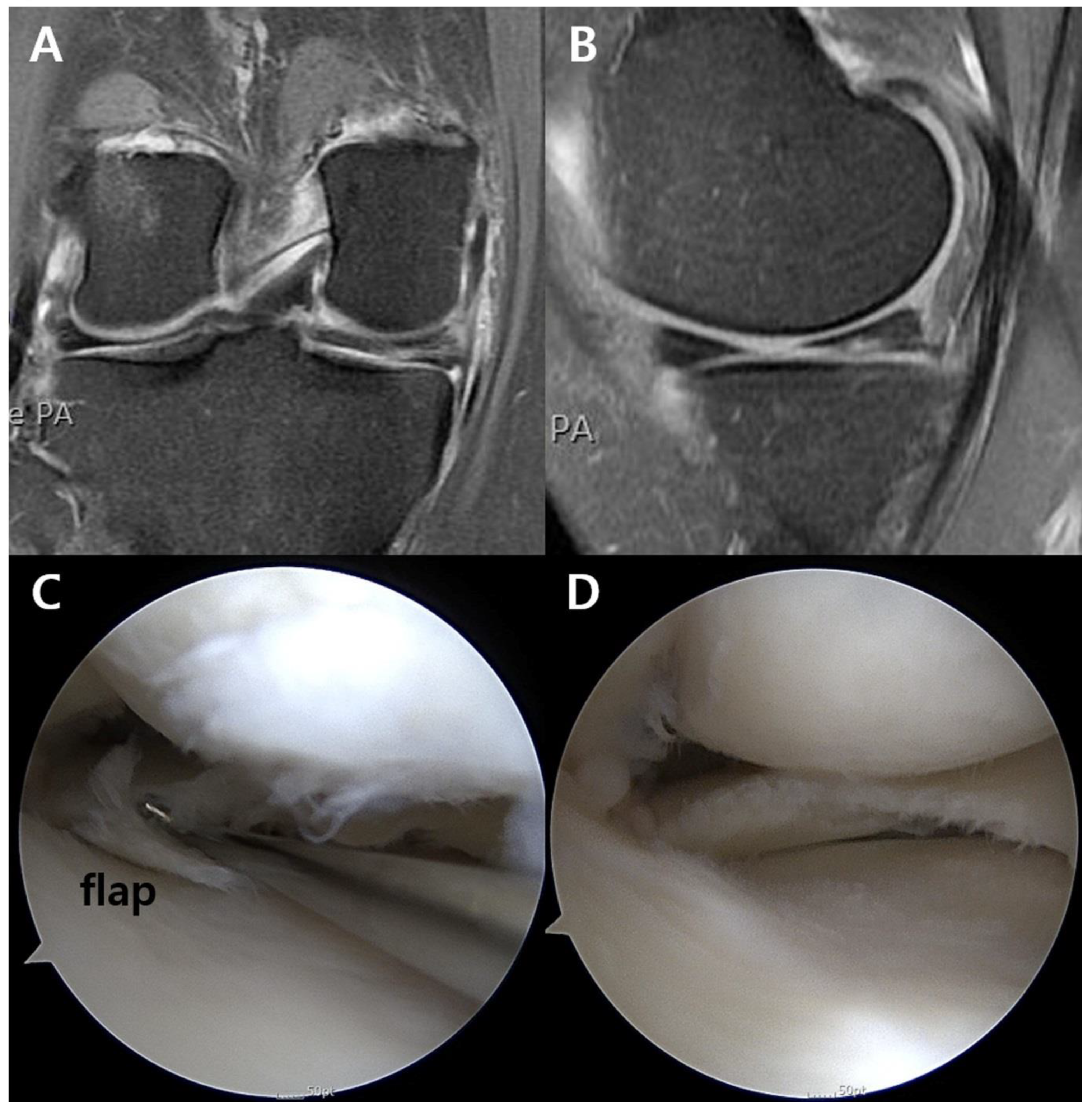
Unstable flap at the posterior horn of the medial meniscus in the right knee. (A) Coronal and (B) sagittal MRI images did not definitely show the flap, which was (C) confirmed and (D) debrided during arthroscopy. MRI, magnetic resonance imaging.
Figure 1.
Unstable flap at the posterior horn of the medial meniscus in the right knee. (A) Coronal and (B) sagittal MRI images did not definitely show the flap, which was (C) confirmed and (D) debrided during arthroscopy. MRI, magnetic resonance imaging.

Figure 2.
Receiver operating characteristic curve for unstable flap showed that the cutoff point of symptom duration was 14.0 months, with the area under curve being 0.70 (sensitivity, 50.0%; specificity, 83.7%).
Figure 2.
Receiver operating characteristic curve for unstable flap showed that the cutoff point of symptom duration was 14.0 months, with the area under curve being 0.70 (sensitivity, 50.0%; specificity, 83.7%).


{kind=link}
{kind=link}
Table 1.
Patient characteristics according to unstable flaps.
| Overall | Flap Group (n = 45) | Non-Flap Group (n = 20) | p Value | |
|---|---|---|---|---|
| Age, yr a | 52.2 ± 12.6 | 49.6 ± 12.8 | 57.7 ± 11.7 | 0.036 |
| Male/Female, n | 29/36 | 21/24 | 8/12 | 0.788 |
| BMI, kg/m2 a | 24.8 ± 6.1 | 24.4 ± 3.9 | 25.8 ± 9.6 | 0.394 |
| Lower limb alignment, deg a, b | 2.7 ± 2.7 | 2.3 ± 2.8 | 3.6 ± 2.4 | 0.116 |
| Trauma history, n | 29 | 22 | 7 | 0.418 |
| Mechanical symptom, n | 50 | 34 | 16 | 0.761 |
| Symptom duration, month a | 13.0 ± 5.8 | 9.3 ± 4.4 | 20.9 ± 11.3 | 0.017 |
| VAS score a | 5.9 ± 2.4 | 6.0 ± 2.5 | 5.8 ± 2.4 | 0.793 |
| Lysholm score a | 67.7 ± 17.6 | 65.9 ± 19.5 | 71.6 ± 11.9 | 0.284 |
| High-grade cartilage wear c | ||||
| Medial femoral condyle | 8 | 2 | 6 | 0.008 |
| Medial tibial plateau | 5 | 1 | 4 | 0.028 |
| Subchondral BML | 7 | 2 | 5 | 0.025 |
BMI, body mass index; VAS, visual analogue scale; BML, bone marrow lesion. a Data are reported as mean ± SD unless otherwise indicated. b Positive values indicate varus alignment, whereas negative values indicate valgus alignment. c High-grade cartilage wear was deemed as that of ≥grade 3 based on the Yulish grading system.
Table 2.
Logistic regression analyses regarding unstable flaps.
| p Value | Exp(β) Coefficient (95% CI) | |||
|---|---|---|---|---|
| Univariate | Multivariate | Univariate | Multivariate | |
| Age | 0.046 | 0.258 | 0.94 (0.89–0.99) | 0.96 (0.90–1.03) |
| Sex | 0.618 | 1.31 (0.45–3.82) | ||
| BMI | 0.409 | 0.97 (0.89–1.05) | ||
| Lower limb alignment | 0.119 | 0.83 (0.65–1.05) | ||
| Trauma history | 0.301 | 1.78 (0.60–5.28) | ||
| Mechanical symptom | 0.695 | 0.77 (0.21–2.81) | ||
| Symptom duration | 0.028 | 0.026 | 0.99 (0.98–0.99) | 0.99 (0.98–0.99) |
| VAS score | 0.788 | 1.04 (0.81–1.33) | ||
| Lysholm score | 0.281 | 0.98 (0.94–1.02) | ||
| High-grade cartilage wear a | ||||
| Medial femoral condyle | 0.011 | 0.017 | 0.11 (0.02–0.60) | 0.06 (0.01–0.61) |
| Medial tibial plateau | 0.038 | 0.95 | 0.09 (0.01–0.88) | 1.00 (0.99–1.00) |
| Subchondral BML | 0.027 | 0.187 | 0.14 (0.02–0.80) | 0.25 (0.03–1.98) |
BMI, body mass index; VAS, visual analogue scale; BML, bone marrow lesion. a High-grade cartilage wear was deemed as that of ≥grade 3 based on the Yulish grading system.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Kim, Y.M.; Joo, Y.B.; An, B.K.; Song, J.-H. Hidden Unstable Flap Should Be Suspected in Treating Intractable Pain from Medial Meniscus Horizontal Tear. J. Clin. Med. 2022, 11, 6245. https://doi.org/10.3390/jcm11216245
AMA Style
Kim YM, Joo YB, An BK, Song J-H. Hidden Unstable Flap Should Be Suspected in Treating Intractable Pain from Medial Meniscus Horizontal Tear. Journal of Clinical Medicine. 2022; 11(21):6245. https://doi.org/10.3390/jcm11216245
Chicago/Turabian StyleKim, Young Mo, Yong Bum Joo, Byung Kuk An, and Ju-Ho Song. 2022. "Hidden Unstable Flap Should Be Suspected in Treating Intractable Pain from Medial Meniscus Horizontal Tear" Journal of Clinical Medicine 11, no. 21: 6245. https://doi.org/10.3390/jcm11216245
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.