
Effects of Intraoperative Opioid Administration on Postoperative Pain and Pain Threshold: A Randomized Controlled Study
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
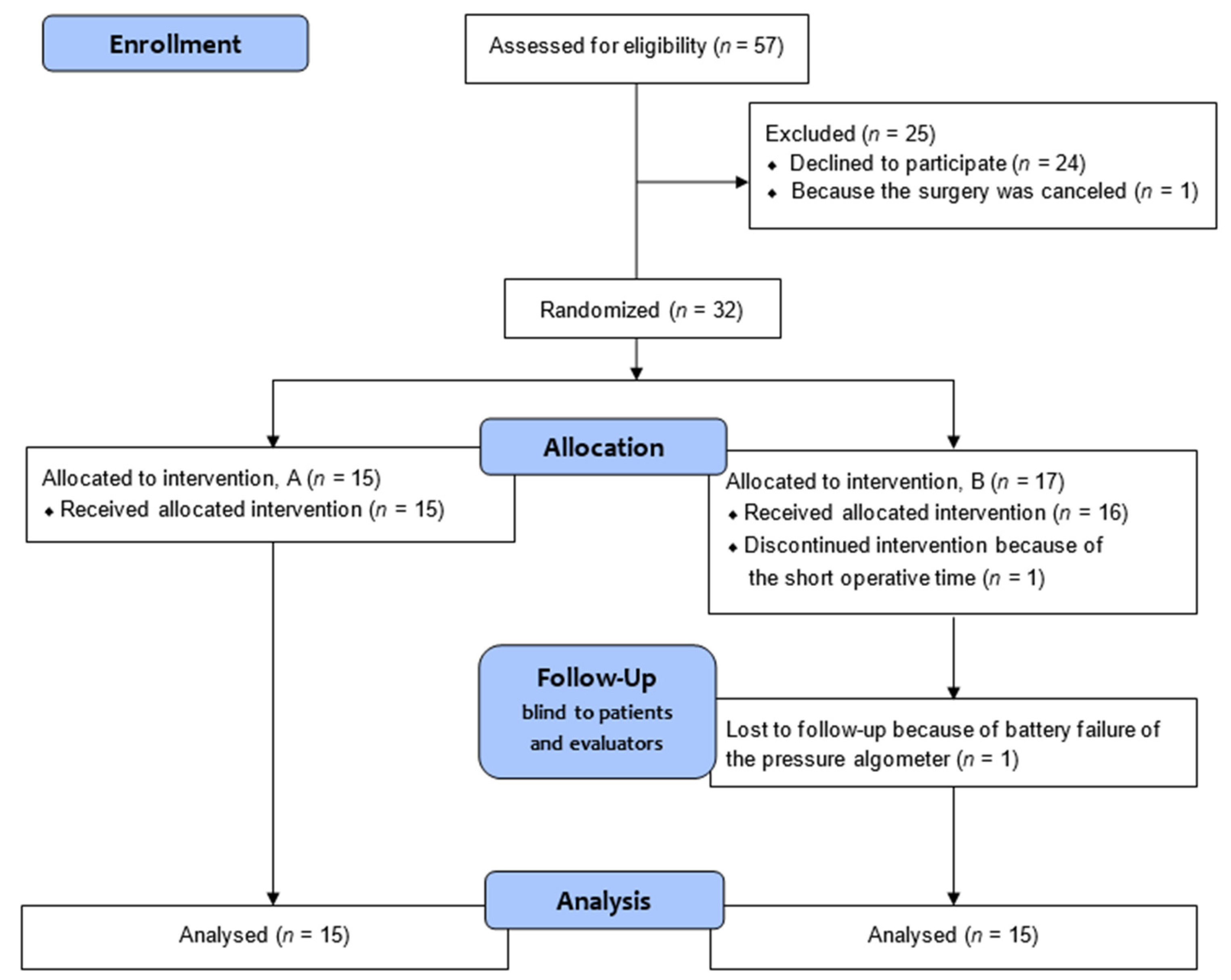
2.1. Participants
2.2. General Anesthesia
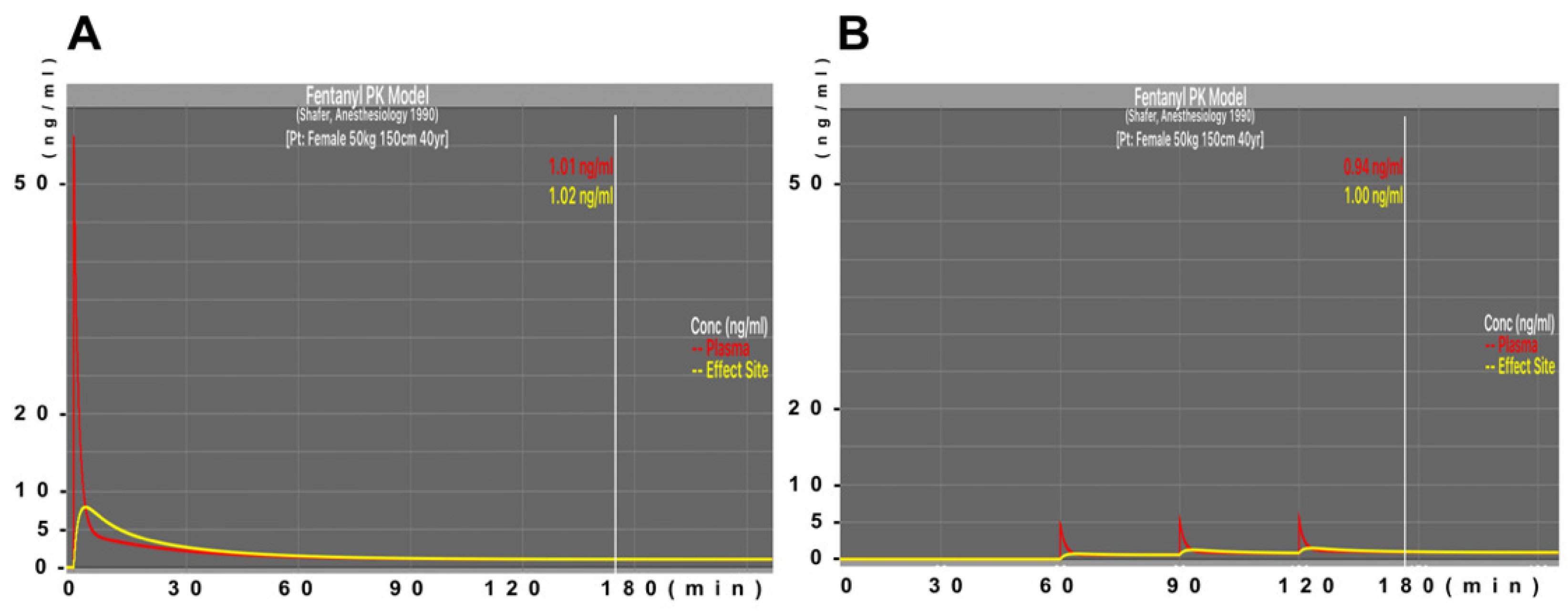
2.3. Remifentanil and Fentanyl Administration
2.4. Outcome Variables
- Pressure Pain Threshold
- 2.
- Numeric Rating Scale score
- 3.
- Total recorded dose of fentanyl administered during surgery.
- 4.
- The highest value during surgery and the value at the end of surgery for the effect site concentration of fentanyl, as estimated by pharmacokinetic simulation [16].
- 5.
- Number of analgesics (including flurbiprofen, acetaminophen and pentazocine) administered in the hospital room until 24 h after surgery, based on the medical records.
2.5. Outcomes
2.5.1. Primary Outcome
2.5.2. Secondary Outcomes
- Difference between the two groups in terms of pressure pain threshold value at 24 h after the end of operation.
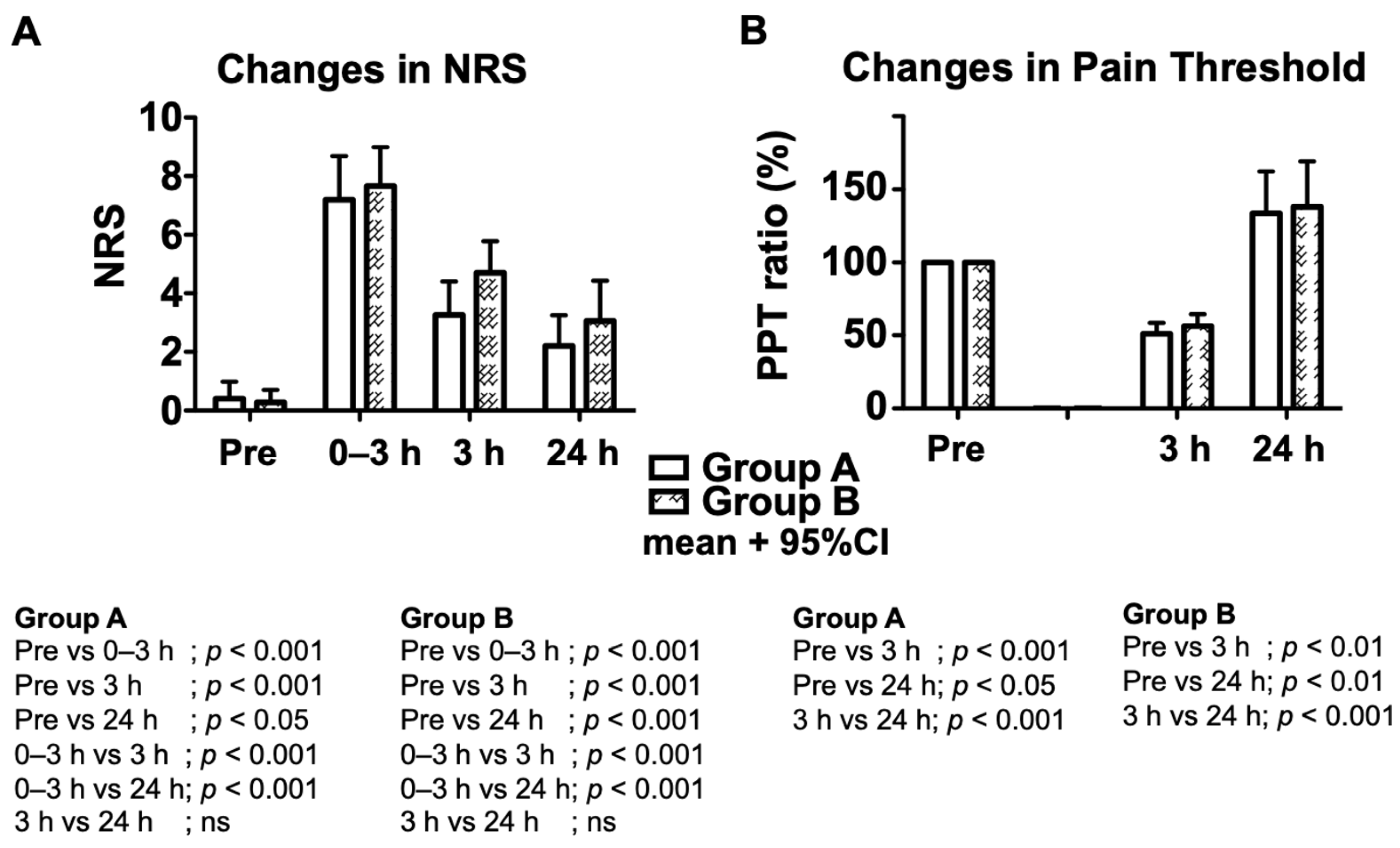
- Difference between the two groups in terms of numeric rating scale scores at 0–3 h, 3 h, and 24 h after the end of operation.
2.5.3. Explorative Outcomes
- Difference between the two groups in terms of the frequency of analgesic (including flurbiprofen, acetaminophen and pentazocine) use in the hospital room during 24 h after surgery.
- Changes in postoperative pressure pain threshold and numeric rating scale score values in each group compared to those before surgery.
2.6. Sample Size Estimation
2.7. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Somogyi, A.A.; Barratt, D.T.; Coller, J.K. Pharmacogenetics of opioids. Clin. Pharmacol. Ther. 2007, 81, 429–444. [Google Scholar] [CrossRef]
- Ghelardini, C.; Di Cesare Mannelli, L.; Bianchi, E. The pharmacological basis of opioids. Clin. Cases Miner. Bone Metab. 2015, 12, 219–221. [Google Scholar] [CrossRef]
- Volkow, N.D.; McLellan, A.T. Opioid Abuse in Chronic Pain--Misconceptions and Mitigation Strategies. N. Engl. J. Med. 2016, 374, 1253–1263. [Google Scholar] [CrossRef]
- Colvin, L.A.; Bull, F.; Hales, T.G. Perioperative opioid analgesia-when is enough too much? A review of opioid-induced tolerance and hyperalgesia. Lancet 2019, 393, 1558–1568. [Google Scholar] [CrossRef]
- Oquendo, M.A.; Volkow, N.D. Suicide: A Silent Contributor to Opioid-Overdose Deaths. N. Engl. J. Med. 2018, 378, 1567–1569. [Google Scholar] [CrossRef]
- Lavand’homme, P.; Steyaert, A. Opioid-free anesthesia opioid side effects: Tolerance and hyperalgesia. Best Pract. Res. Clin. Anaesthesiol. 2017, 31, 487–498. [Google Scholar] [CrossRef]
- Kharasch, E.D.; Clark, J.D. Opioid-free Anesthesia: Time to Regain Our Balance. Anesthesiology 2021, 134, 509–514. [Google Scholar] [CrossRef]
- Yildirim, V.; Doganci, S.; Cinar, S.; Eskin, M.B.; Ozkan, G.; Eksert, S.; Ince, M.E.; Dogrul, A. Acute high dose-fentanyl exposure produces hyperalgesia and tactile allodynia after coronary artery bypass surgery. Eur. Rev. Med. Pharmacol. Sci. 2014, 18, 3425–3434. [Google Scholar]
- Mauermann, E.; Filitz, J.; Dolder, P.; Rentsch, K.M.; Bandschapp, O.; Ruppen, W. Does Fentanyl Lead to Opioid-induced Hyperalgesia in Healthy Volunteers?: A Double-blind, Randomized, Crossover Trial. Anesthesiology 2016, 124, 453–463. [Google Scholar] [CrossRef]
- Yaksh, T.; Wallace, M. Opioids, Analgesia, and Pain Management. In Goodman & Gilman’s: The Pharmacological Basis of Therapeutics, 13th ed.; Brunton, L.L., Hilal-Dandan, R., Knollmann, B.C., Eds.; McGraw Hill: New York, NY, USA, 2017; Available online: https://accessmedicine.mhmedical.com/content.aspx?bookid=2189§ionid=170269577 (accessed on 26 March 2022).
- Fletcher, D.; Martinez, V. Opioid-induced hyperalgesia in patients after surgery: A systematic review and a meta-analysis. Br. J. Anaesth. 2014, 112, 991–1004. [Google Scholar] [CrossRef]
- Saxena, S.; Gonsette, K.; Terram, W.; Huybrechts, I.; Nahrwold, D.A.; Cappello, M.; Barvais, L.; Engelman, E. Gradual withdrawal of remifentanil delays initial post-operative analgesic demand after thyroid surgery; double-blinded, randomized controlled trial. BMC Anesth. 2019, 19, 60. [Google Scholar] [CrossRef] [Green Version]
- Woolf, C.J.; Chong, M.S. Preemptive analgesia—Treating postoperative pain by preventing the establishment of central sensitization. Anesth. Analg. 1993, 77, 362–379. [Google Scholar] [CrossRef]
- Swinhoe, C.F.; Peacock, J.E.; Glen, J.B.; Reilly, C.S. Evaluation of the predictive performance of a ‘Diprifusor’ TCI system. Anaesthesia 1998, 53 (Suppl. S1), 61–67. [Google Scholar] [CrossRef]
- Sigl, J.C.; Chamoun, N.G. An introduction to bispectral analysis for the electroencephalogram. J. Clin. Monit. 1994, 10, 392–404. [Google Scholar] [CrossRef]
- Shafer, S.L.; Varvel, J.R.; Aziz, N.; Scott, J.C. Pharmacokinetics of fentanyl administered by computer-controlled infusion pump. Anesthesiology 1990, 73, 1091–1102. [Google Scholar] [CrossRef]
- Maquet, D.; Croisier, J.L.; Demoulin, C.; Crielaard, J.M. Pressure pain thresholds of tender point sites in patients with fibromyalgia and in healthy controls. Eur. J. Pain 2004, 8, 111–117. [Google Scholar] [CrossRef]
- Haefeli, M.; Elfering, A. Pain assessment. Eur. Spine J. 2006, 15 (Suppl. S1), S17–S24. [Google Scholar] [CrossRef]
- Terzi, H.; Terzi, R.; Kale, A. The relationship between fibromyalgia and pressure pain threshold in patients with dyspareunia. Pain Res. Manag. 2015, 20, 137–140. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Lang, A.G.; Buchner, A. G*Power 3: A flexible statistical power analysis program for the social, behavioral, and biomedical sciences. Behav. Res. Methods 2007, 39, 175–191. [Google Scholar] [CrossRef]
- Williams, J.T.; Ingram, S.L.; Henderson, G.; Chavkin, C.; von Zastrow, M.; Schulz, S.; Koch, T.; Evans, C.J.; Christie, M.J. Regulation of mu-opioid receptors: Desensitization, phosphorylation, internalization, and tolerance. Pharmacol. Rev. 2013, 65, 223–254. [Google Scholar] [CrossRef]
- Bull, F.A.; Baptista-Hon, D.T.; Sneddon, C.; Wright, L.; Walwyn, W.; Hales, T.G. Src Kinase Inhibition Attenuates Morphine Tolerance without Affecting Reinforcement or Psychomotor Stimulation. Anesthesiology 2017, 127, 878–889. [Google Scholar] [CrossRef]
- Schrepf, A.; Harper, D.E.; Harte, S.E.; Wang, H.; Ichesco, E.; Hampson, J.P.; Zubieta, J.K.; Clauw, D.J.; Harris, R.E. Endogenous opioidergic dysregulation of pain in fibromyalgia: A PET and fMRI study. Pain 2016, 157, 2217–2225. [Google Scholar] [CrossRef]
- Lee, M.C.; Zambreanu, L.; Menon, D.K.; Tracey, I. Identifying brain activity specifically related to the maintenance and perceptual consequence of central sensitization in humans. J. Neurosci. 2008, 28, 11642–11649. [Google Scholar] [CrossRef]
- Minto, C.F.; Schnider, T.W.; Shafer, S.L. Pharmacokinetics and pharmacodynamics of remifentanil. II. Model application. Anesthesiology 1997, 86, 24–33. [Google Scholar] [CrossRef]
- Rutkow, L.; Vernick, J.S. Emergency Legal Authority and the Opioid Crisis. N. Engl. J. Med. 2017, 377, 2512–2514. [Google Scholar] [CrossRef]
- Volkow, N.D.; Collins, F.S. The Role of Science in Addressing the Opioid Crisis. N. Engl. J. Med. 2017, 377, 391–394. [Google Scholar] [CrossRef]
- Barry, C.L.; Saloner, B. Using Policy Tools to Improve Population Health—Combating the U.S. Opioid Crisis. N. Engl. J. Med. 2021, 385, 2113–2116. [Google Scholar] [CrossRef]
- Kharasch, E.D.; Clark, J.D.; Adams, J.M. Opioids and Public Health: The Prescription Opioid Ecosystem and Need for Improved Management. Anesthesiology 2022, 136, 10–30. [Google Scholar] [CrossRef]
- Barnett, M.L.; Olenski, A.R.; Jena, A.B. Opioid-Prescribing Patterns of Emergency Physicians and Risk of Long-Term Use. N. Engl. J. Med. 2017, 376, 663–673. [Google Scholar] [CrossRef]
- Glare, P.; Aubrey, K.R.; Myles, P.S. Transition from acute to chronic pain after surgery. Lancet 2019, 393, 1537–1546. [Google Scholar] [CrossRef]
- Drug Enforcement Administration, U.S. Department of Justice. Drugs of Abuse, A DEA RESOURCE GUIDE, 2020th ed.; Drug Enforcement Administration, U.S. Department of Justice: Washington, DC, USA. Available online: https://www.dea.gov/sites/default/files/2020-04/Drugs%20of%20Abuse%202020-Web%20Version-508%20compliant-4-24-20_0.pdf (accessed on 14 September 2022).
- Neuman, M.D.; Bateman, B.T.; Wunsch, H. Inappropriate opioid prescription after surgery. Lancet 2019, 393, 1547–1557. [Google Scholar] [CrossRef]
- Lee, B.; Zhao, W.; Yang, K.C.; Ahn, Y.Y.; Perry, B.L. Systematic Evaluation of State Policy Interventions Targeting the US Opioid Epidemic, 2007–2018. JAMA Netw. Open 2021, 4, e2036687. [Google Scholar] [CrossRef]
- Kiang, M.V.; Humphreys, K.; Cullen, M.R.; Basu, S. Opioid prescribing patterns among medical providers in the United States, 2003–2017: Retrospective, observational study. BMJ 2020, 368, l6968. [Google Scholar] [CrossRef]
- Brat, G.A.; Agniel, D.; Beam, A.; Yorkgitis, B.; Bicket, M.; Homer, M.; Fox, K.P.; Knecht, D.B.; McMahill-Walraven, C.N.; Palmer, N.; et al. Postsurgical prescriptions for opioid naive patients and association with overdose and misuse: Retrospective cohort study. BMJ 2018, 360, j5790. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef]
- Oppeltz, R.F.; Holloway, T.L.; Covington, C.J.; Schwacha, M.G. The contribution of opiate analgesics to the development of infectious complications in trauma patients. Int. J. Burns Trauma 2015, 5, 56–65. [Google Scholar]
- Chen, E.Y.; Marcantonio, A.; Tornetta, P., 3rd. Correlation Between 24-Hour Predischarge Opioid Use and Amount of Opioids Prescribed at Hospital Discharge. JAMA Surg. 2018, 153, e174859. [Google Scholar] [CrossRef]
- Wu, C.L.; King, A.B.; Geiger, T.M.; Grant, M.C.; Grocott, M.P.W.; Gupta, R.; Hah, J.M.; Miller, T.E.; Shaw, A.D.; Gan, T.J.; et al. American Society for Enhanced Recovery and Perioperative Quality Initiative Joint Consensus Statement on Perioperative Opioid Minimization in Opioid-Naive Patients. Anesth. Analg. 2019, 129, 567–577. [Google Scholar] [CrossRef]
- Kharasch, E.D.; Avram, M.J.; Clark, J.D. Rational Perioperative Opioid Management in the Era of the Opioid Crisis. Anesthesiology 2020, 132, 603–605. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Group A, n = 15 Mean ± SD | Group B, n = 15 Mean ± SD | p Value (Student’s t-Test) | |
|---|---|---|---|
| Age (years old) | 43.5 ± 7.0 | 41.5 ± 6.8 | 0.435 |
| Height (m) | 1.58 ± 0.05 | 1.59 ± 0.04 | 0.487 |
| actual Weight (kg) | 58.8 ± 10.1 | 57.5 ± 7.8 | 0.694 |
| Weight (kg) | 53.8 ± 5.0 | 53.9 ± 4.2 | 0.962 |
| ASA physical status (number of patients) | |||
| I | 7 | 11 | |
| II | 8 | 4 | |
| Surgical site (number of patients) | |||
| ovary | 5 | 5 | |
| uterus | 10 | 10 |
| Group A, n = 15 Mean ± SD | Group B, n = 15 Mean ± SD | p Value (Student’s t-Test) | |
|---|---|---|---|
| Duration of anesthesia (min) | 245.4 ± 65.7 | 200.3 ± 51.1 | 0.045 (p < 0.05) |
| Duration of surgery (min) | 193.7 ± 65.0 | 152.1 ± 51.2 | 0.062 |
| Amount of fentanyl (μg/kg/h) | 2.31 ± 0.47 | 1.25 ± 0.19 | 7.63 × 10−9 (p < 0.001) |
| Estimated effect site concentration of fentanyl (ng/mL) | |||
| Maximum value during surgery | 7.86 ± 0.0 | 1.52 ± 0.08 | 1.30 × 10−50 (p < 0.001) |
| Value at the end of surgery | 1.01 ± 0.02 | 1.07 ± 0.19 | 0.202 |
| Group A, n = 15 Mean (95% CI) | Group B, n = 15 Mean (95% CI) | p Value (Student’s t-Test) | |
|---|---|---|---|
| Numeric rating scale scores | |||
| Pre-operative | 0.4 (0–0.92) numeric rating scale score = 0; 12 patients | 0.27 (0–0.66) numeric rating scale score = 0; 13 patients | 0.699 |
| Maximum values during 0–3 h after surgery | 7.2 (5.9–8.5) | 7.7 (6.5–8.8) | 0.618 |
| 3 h after surgery | 3.3 (2.3–4.3) | 4.7 (3.7–5.7) | 0.060 |
| 24 h after surgery | 2.2 (1.3–3.1) | 3.1 (1.9–4.3) | 0.290 |
| Pressure pain threshold | |||
| Pre-operative (kg/0.5 cm2) | 2.40 (2.01–2.80) | 2.45 (2.10–2.80) | 0.871 |
| Pressure pain threshold ratio | |||
| Pre-operative (%) | 100 | 100 | - |
| 3 h after surgery (%) | 51.1 (44.4–57.8) | 56.6 (49.5–63.6) | 0.298 |
| 24 h after surgery (%) | 133.5 (108.2–158.8) | 138.0 (110.5–165.5) | 0.823 |
| Analgesic use after surgery | chi-square test | ||
| 0–3 h (number of times/group) | 11 | 8 | p = 0.332 |
| 3–24 h (number of times/group) | 9 | 3 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kawanaka, R.; Sakuma, S.; Kokubun, H.; Tetsu, S.; Tagaito, Y.; Igarashi, T.; Liang, S.-G.; Aoe, T. Effects of Intraoperative Opioid Administration on Postoperative Pain and Pain Threshold: A Randomized Controlled Study. J. Clin. Med. 2022, 11, 5587. https://doi.org/10.3390/jcm11195587
Kawanaka R, Sakuma S, Kokubun H, Tetsu S, Tagaito Y, Igarashi T, Liang S-G, Aoe T. Effects of Intraoperative Opioid Administration on Postoperative Pain and Pain Threshold: A Randomized Controlled Study. Journal of Clinical Medicine. 2022; 11(19):5587. https://doi.org/10.3390/jcm11195587
Chicago/Turabian StyleKawanaka, Ryoko, Shoko Sakuma, Hiroshi Kokubun, Shuhei Tetsu, Yugo Tagaito, Toshio Igarashi, Shan-Guang Liang, and Tomohiko Aoe. 2022. "Effects of Intraoperative Opioid Administration on Postoperative Pain and Pain Threshold: A Randomized Controlled Study" Journal of Clinical Medicine 11, no. 19: 5587. https://doi.org/10.3390/jcm11195587