
Lower Extremity Arterial Disease and Lumbar Spinal Stenosis: A Study of Exercise-Induced Arterial Ischemia in 5197 Patients Complaining of Claudication
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
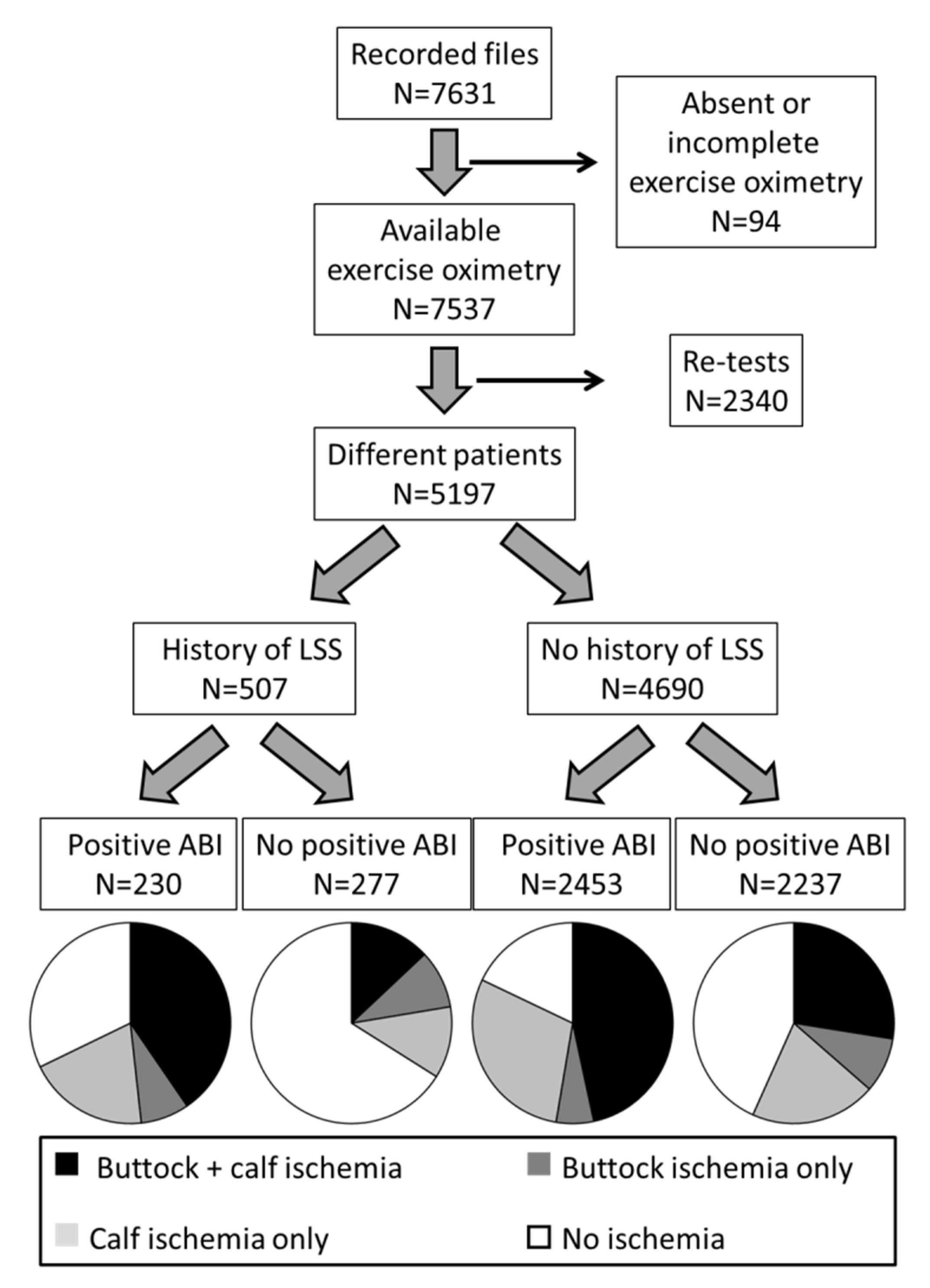
2.1. Population
2.2. Treadmill Tests
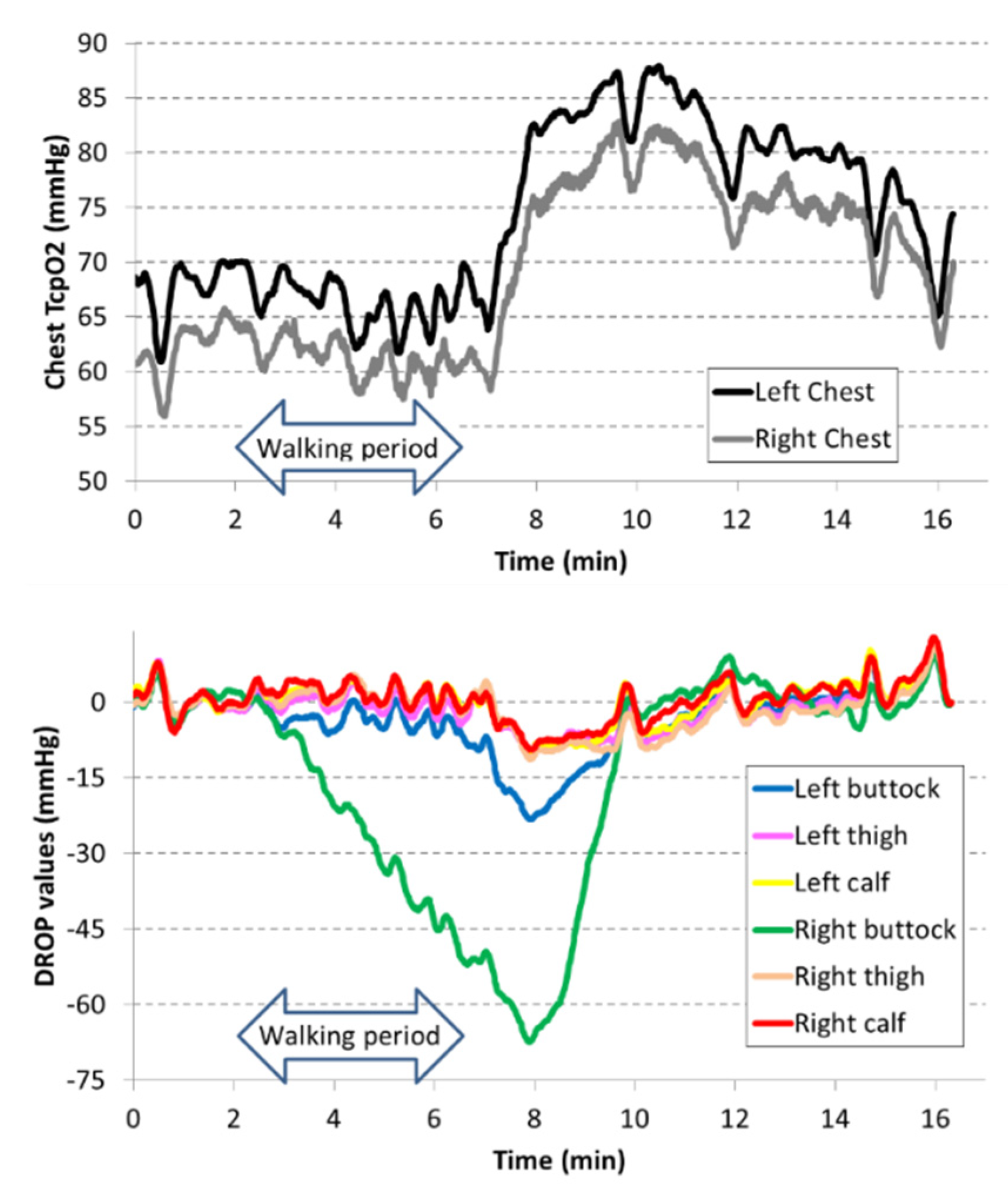
2.3. Exercise-Oximetry Recordings
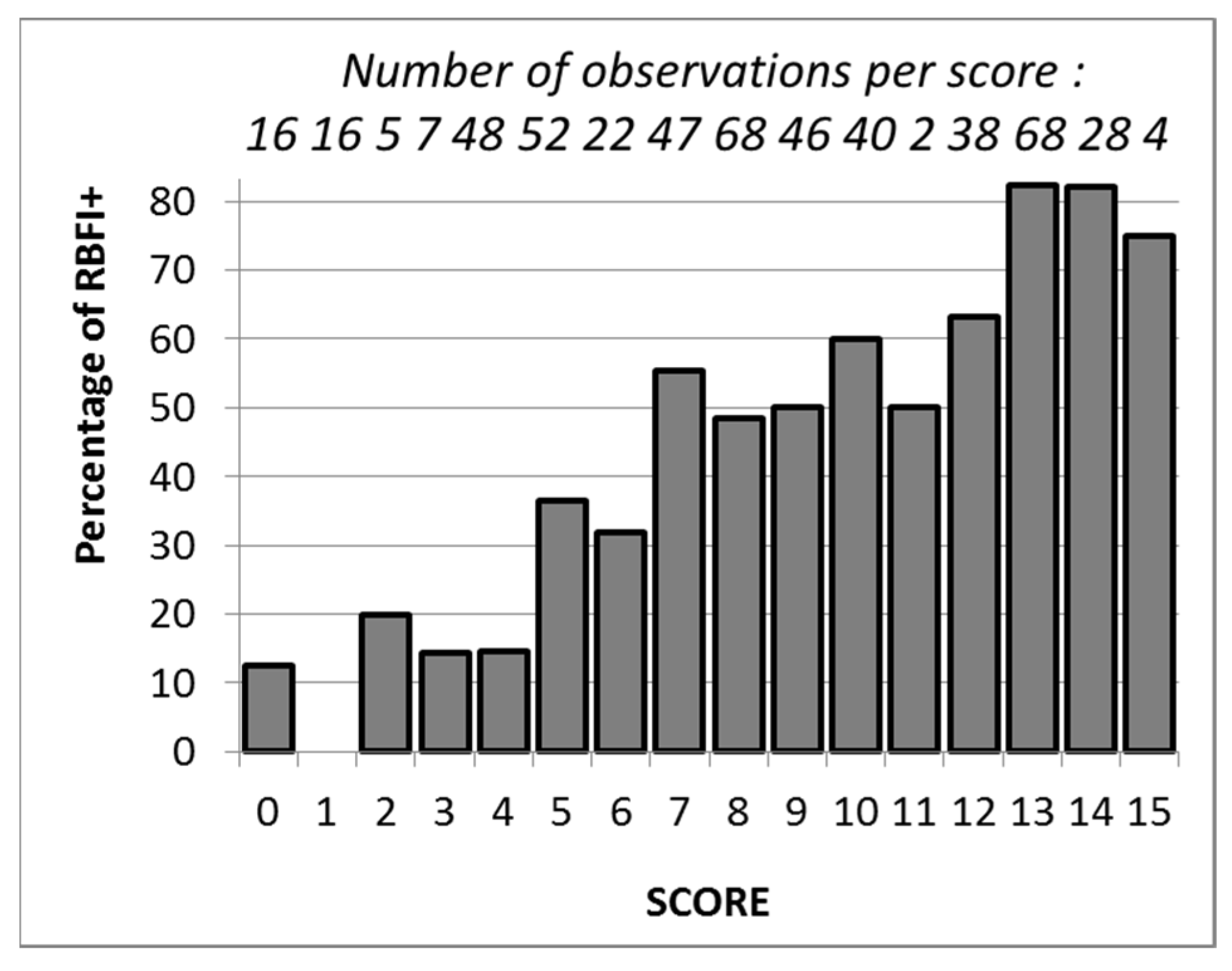
2.4. Score Determination and Validation
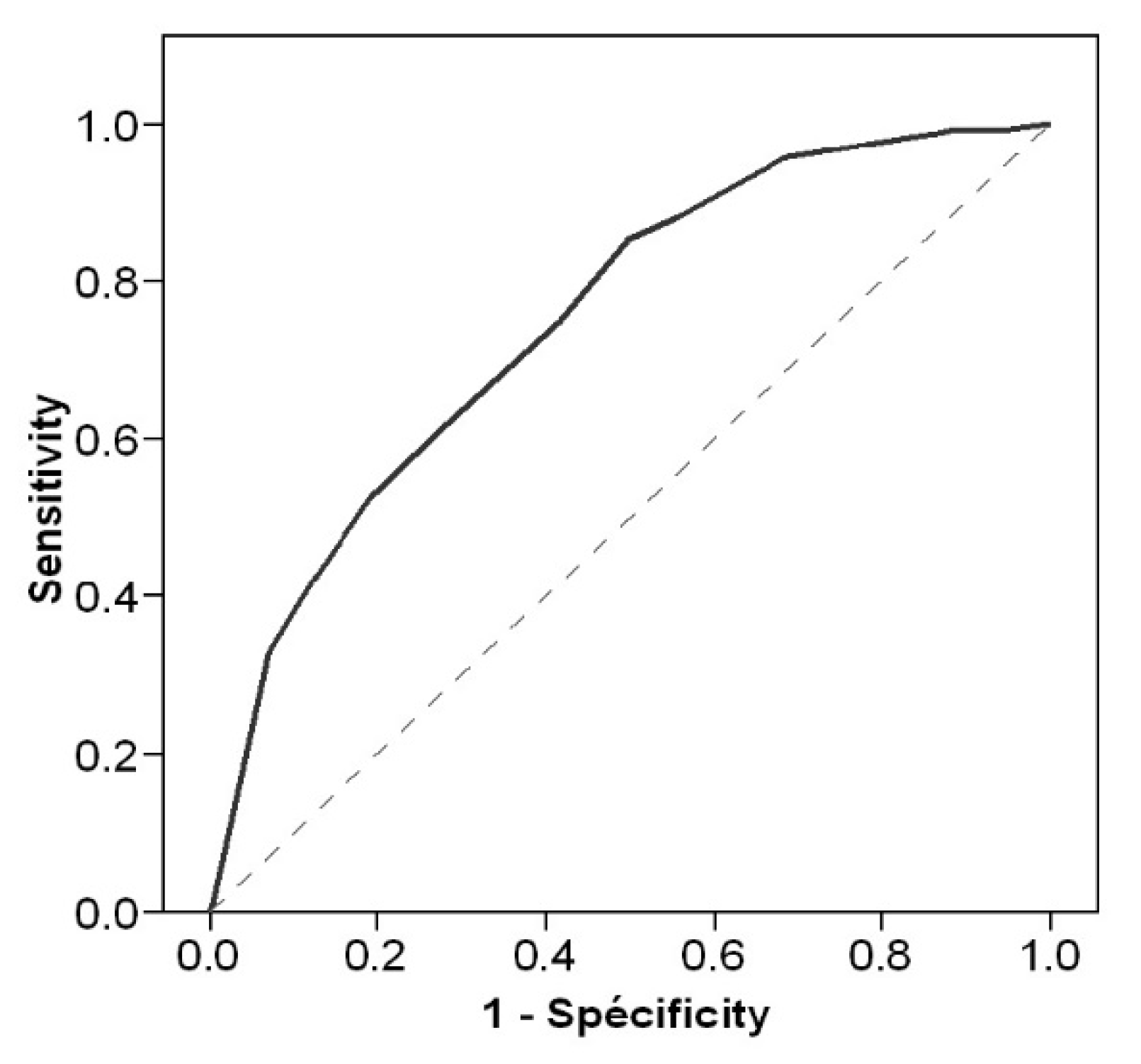
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kannel, W.B.; Skinner, J.J., Jr.; Schwartz, M.J.; Shurtleff, D. Intermittent claudication. Incidence in the Framingham Study. Circulation 1970, 41, 875–883. [Google Scholar] [CrossRef] [PubMed]
- Wattanakit, K.; Folsom, A.R.; Selvin, E.; Weatherley, B.D.; Pankow, J.S.; Brancati, F.L.; Hirsch, A.T. Risk factors for peripheral arterial disease incidence in persons with diabetes: The Atherosclerosis Risk in Communities (ARIC) Study. Atherosclerosis 2005, 180, 389–397. [Google Scholar] [CrossRef] [PubMed]
- Wyss, T.R.; Adam, L.; Haynes, A.G.; Kucher, N.; Silbernagel, G.; Do, D.D.; Schmidli, J.; Baumgartner, I. Impact of cardiovascular risk factors on severity of peripheral artery disease. Atherosclerosis 2015, 242, 97–101. [Google Scholar] [CrossRef]
- Maeda, T.; Hashizume, H.; Yoshimura, N.; Oka, H.; Ishimoto, Y.; Nagata, K.; Takami, M.; Tsutsui, S.; Iwasaki, H.; Minamide, A.; et al. Factors associated with lumbar spinal stenosis in a large-scale, population-based cohort: The Wakayama Spine Study. PLoS ONE 2018, 13, e0200208. [Google Scholar] [CrossRef] [PubMed]
- Aghayev, E.; Mannion, A.F.; Fekete, T.F.; Janssen, S.; Goodwin, K.; Zwahlen, M.; Berlemann, U.; Lorenz, T. Risk Factors for Negative Global Treatment Outcomes in Lumbar Spinal Stenosis Surgery: A Mixed Effects Model Analysis of Data from an International Spine Registry. World Neurosurg. 2020, 136, e270–e283. [Google Scholar] [CrossRef]
- Kim, G.U.; Park, J.; Kim, H.J.; Shen, F.; Cho, J.; Chang, B.S.; Lee, C.-K.; Chun, H.-J.; Yeom, J.S. Definitions of unfavorable surgical outcomes and their risk factors based on disability score after spine surgery for lumbar spinal stenosis. BMC Musculoskelet. Disord. 2020, 21, 288. [Google Scholar] [CrossRef]
- Banas, W.; Czerniak, B.; Budzynski, J. Physical and psychological functioning of patients with chronic limb ischemia during a 1-year period after endovascular revascularization. J. Vasc. Surg. 2022, 75, 1679–1686. [Google Scholar] [CrossRef]
- Heidrich, H.; Hermann, G.M. Concomitant neurological and orthopaedic diseases in the presence of peripheral arterial disease: A prospective study. Vasa 2006, 35, 101–105. [Google Scholar] [CrossRef]
- Kauppila, L.I. Prevalence of stenotic changes in arteries supplying the lumbar spine. A postmortem angiographic study on 140 subjects. Ann. Rheum. Dis. 1997, 56, 591–595. [Google Scholar] [CrossRef]
- Kauppila, L.I.; Penttila, A.; Karhunen, P.J.; Lalu, K.; Hannikainen, P. Lumbar disc degeneration and atherosclerosis of the abdominal aorta. Spine 1994, 19, 923–929. [Google Scholar] [CrossRef]
- Kurunlahti, M.; Karppinen, J.; Haapea, M.; Niinimaki, J.; Autio, R.; Vanharanta, H.; Suramo, I.; Tervonen, O. Three-year follow-up of lumbar artery occlusion with magnetic resonance angiography in patients with sciatica: Associations between occlusion and patient-reported symptoms. Spine 2004, 29, 1804–1808, Discussion 9. [Google Scholar] [CrossRef]
- Aboyans, V.; Criqui, M.H.; Abraham, P.; Allison, M.A.; Creager, M.A.; Diehm, C.; Fowkes, G.R.F.; Hiatt, W.R.; Jönsson, B.; Lacroix, P.; et al. Measurement and interpretation of the ankle-brachial index: A scientific statement from the American Heart Association. Circulation 2012, 126, 2890–2909. [Google Scholar] [CrossRef] [PubMed]
- Dachun, X.; Jue, L.; Liling, Z.; Yawei, X.; Dayi, H.; Pagoto, S.L.; Ma, Y. Sensitivity and specificity of the ankle--brachial index to diagnose peripheral artery disease: A structured review. Vasc. Med. 2010, 15, 361–369. [Google Scholar] [CrossRef]
- Herraiz-Adillo, A.; Cavero-Redondo, I.; Alvarez-Bueno, C.; Pozuelo-Carrascosa, D.P.; Solera-Martinez, M. The accuracy of toe brachial index and ankle brachial index in the diagnosis of lower limb peripheral arterial disease: A systematic review and meta-analysis. Atherosclerosis 2020, 315, 81–92. [Google Scholar] [CrossRef] [PubMed]
- Diehm, C.; Darius, H.; Pittrow, D.; Schwertfeger, M.; Tepohl, G.; Haberl, R.L.; Allenberg, J.R.; Burghaus, I.; Trampisch, H.J. Prognostic value of a low post-exercise ankle brachial index as assessed by primary care physicians. Atherosclerosis 2011, 214, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Gernigon, M.; Marchand, J.; Ouedraogo, N.; Leftheriotis, G.; Piquet, J.M.; Abraham, P. Proximal ischemia is a frequent cause of exercise-induced pain in patients with a normal ankle to brachial index at rest. Pain Physician 2013, 16, 57–64. [Google Scholar]
- Abraham, P.; Hersant, J.; Ramondou, P.; Picquet, J.; Feuilloy, M.; Henni, S.; SOCOS group. Comparison of exercise oximetry and ankle pressure measurements for patients with intermittent claudication: An observational study of 433 patients. Pflugers Arch. 2020, 472, 293–301. [Google Scholar] [CrossRef]
- Signolet, I.; Henni, S.; Colas-Ribas, C.; Feuilloy, M.; Picquet, J.; Abraham, P. Prevalence and Causes of Normal Exercise Oximetry in the Calf in Patients with Peripheral Artery Disease and Limiting Calf Claudication. Eur. J. Vasc. Endovasc. Surg. 2016, 51, 572–578. [Google Scholar] [CrossRef]
- Abraham, P.; Ramondou, P.; Hersant, J.; Sempore, W.Y.; Feuilloy, M.; Henni, S. Investigation of arterial claudication with transcutaneous oxygen pressure at exercise: Interests and limits. Trends Cardiovasc. Med. 2021, 31, 218–223. [Google Scholar] [CrossRef]
- Gerhard-Herman, M.D.; Gornik, H.L.; Barrett, C.; Barshes, N.R.; Corriere, M.A.; Drachman, D.E.; Fleisher, L.A.; Fowkes, F.G.R.; Hamburg, N.M.; Kinlay, S.; et al. 2016 AHA/ACC Guideline on the Management of Patients With Lower Extremity Peripheral Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 2017, 135, e726. [Google Scholar]
- Aboyans, V.; Ricco, J.B.; Bartelink, M.E.L.; Bjorck, M.; Brodmann, M.; Cohnert, T.; Collet, J.-P.; Czerny, M.; De Carlo, M.; Debus, S.; et al. 2017 ESC Guidelines on the Diagnosis and Treatment of Peripheral Arterial Diseases, in collaboration with the European Society for Vascular Surgery (ESVS): Document covering atherosclerotic disease of extracranial carotid and vertebral, mesenteric, renal, upper and lower extremity arteriesEndorsed by: The European Stroke Organization (ESO)The Task Force for the Diagnosis and Treatment of Peripheral Arterial Diseases of the European Society of Cardiology (ESC) and of the European Society for Vascular Surgery (ESVS). Eur. Heart J. 2018, 39, 763–816. [Google Scholar] [PubMed]
- Mahe, G.; Ouedraogo, N.; Marchand, J.; Vielle, B.; Picquet, J.; Leftheriotis, G.; Abraham, P. Self-reported estimation of usual walking speed improves the performance of questionnaires estimating walking capacity in patients with vascular-type claudication. J. Vasc. Surg. 2011, 54, 1360–1365. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sempore, W.Y.; Ramondou, P.; Hersant, J.; Feuilloy, M.; Guilleron, C.; Henni, S.; Abraham, P. Specific slow tests are not mandatory in patients with extremely short standard (3.2 km/hr 10% slope) test durations during exercise oximetry. Clin. Physiol. Funct. Imaging 2020, 40, 232–237. [Google Scholar] [CrossRef] [PubMed]
- Kalichman, L.; Kim, D.H.; Li, L.; Guermazi, A.; Berkin, V.; Hunter, D.J. Spondylolysis and spondylolisthesis: Prevalence and association with low back pain in the adult community-based population. Spine 2009, 34, 199–205. [Google Scholar] [CrossRef]
- Gerhardt, J.; Bette, S.; Janssen, I.; Gempt, J.; Meyer, B.; Ryang, Y.M. Is Eighty the New Sixty? Outcomes and Complications after Lumbar Decompression Surgery in Elderly Patients over 80 Years of Age. World Neurosurg. 2018, 112, e555–e560. [Google Scholar] [CrossRef]
- Fowkes, F.G.; Rudan, D.; Rudan, I.; Aboyans, V.; Denenberg, J.O.; McDermott, M.M.; Norman, P.E.; Sampson, U.K.A.; Williams, L.J.; Mensah, G.A.; et al. Comparison of global estimates of prevalence and risk factors for peripheral artery disease in 2000 and 2010: A systematic review and analysis. Lancet 2013, 382, 1329–1340. [Google Scholar] [CrossRef]
- Armstrong, D.W.; Tobin, C.; Matangi, M.F. The accuracy of the physical examination for the detection of lower extremity peripheral arterial disease. Can. J. Cardiol. 2010, 26, e346–e350. [Google Scholar] [CrossRef]
- Jeon, C.H.; Han, S.H.; Chung, N.S.; Hyun, H.S. The validity of ankle-brachial index for the differential diagnosis of peripheral arterial disease and lumbar spinal stenosis in patients with atypical claudication. Eur. Spine J. 2012, 21, 1165–1170. [Google Scholar] [CrossRef]
- Park, J.W.; Lee, J.H. Prevalence and Risk Factors of Peripheral Arterial Disease in Patients with Lumbar Spinal Stenosis and Intermittent Claudication: CT Angiography Study. J. Korean Med. Sci. 2020, 35, e87. [Google Scholar] [CrossRef]
- Han, M.H.; Lee, D.H.; Park, K.S.; Lee, Y.S.; Kim, K.T.; Sung, J.K.; Kim, H.-K.; Cho, D.-C. Risk factors and incidence for peripheral arterial disease in patients with typical lumbar spinal stenosis. Korean J. Spine 2014, 11, 183–187. [Google Scholar] [CrossRef]
- Imagama, S.; Matsuyama, Y.; Sakai, Y.; Ito, Z.; Wakao, N.; Deguchi, M.; Hachiya, Y.; Osawa, Y.; Yoshihara, H.; Kamiya, M.; et al. An arterial pulse examination is not sufficient for diagnosis of peripheral arterial disease in lumbar spinal canal stenosis: A prospective multicenter study. Spine 2011, 36, 1204–1210. [Google Scholar] [CrossRef] [PubMed]
- Abraham, P.; Picquet, J.; Vielle, B.; Sigaudo-Roussel, D.; Paisant-Thouveny, F.; Enon, B.; Saumet, J.L. Transcutaneous oxygen pressure measurements on the buttocks during exercise to detect proximal arterial ischemia: Comparison with arteriography. Circulation 2003, 107, 1896–1900. [Google Scholar] [CrossRef] [Green Version]
- Jaquinandi, V.; Picquet, J.; Bouye, P.; Saumet, J.L.; Leftheriotis, G.; Abraham, P. High prevalence of proximal claudication among patients with patent aortobifemoral bypasses. J. Vasc. Surg. 2007, 45, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Houle, M.; O’Shaughnessy, J.; Tetreau, C.; Chatillon, C.E.; Marchand, A.A.; Descarreaux, M. Comparison of walking variations during treadmill walking test between neurogenic and vascular claudication: A crossover study. Chiropr. Man. Therap. 2021, 29, 24. [Google Scholar] [CrossRef] [PubMed]
- Murakami, M.; Takahashi, K.; Sekikawa, T.; Yasuhara, K.; Yamagata, M.; Moriya, H. Effects of intravenous lipoprostaglandin E1 on neurogenic intermittent claudication. J. Spinal Disord. 1997, 10, 499–504. [Google Scholar] [CrossRef] [PubMed]
- Dezawa, A.; Unno, K.; Yamane, T.; Miki, H. Changes in the microhemodynamics of nerve root retraction in patients with lumbar spinal canal stenosis. Spine 2002, 27, 2844–2849. [Google Scholar] [CrossRef]
- Matsudaira, K.; Seichi, A.; Kunogi, J.; Yamazaki, T.; Kobayashi, A.; Anamizu, Y.; Kishimoto, J.; Hoshi, K.; Takeshita, K.; Nakamura, K. The efficacy of prostaglandin E1 derivative in patients with lumbar spinal stenosis. Spine 2009, 34, 115–120. [Google Scholar] [CrossRef]
- Han, S.H.; Jeon, C.H.; Lee, D.H.; Choo, H.S.; Chung, N.S. Clinical and radiological characteristics of concomitant peripheral arterial obstructive disease in patients with lumbar spinal stenosis. Pain Physician 2013, 16, 513–520. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| History of LSS n = 507 | No History of LSS n = 4690 | p | |
|---|---|---|---|
| Male sex | 402 (79.3) | 3688 (78.6) | 0.732 |
| Weight (kg) | 80.9 ± 15.6 | 76.0 ± 15.3 | 0.001 |
| Height (cm) | 169 ± 9 | 168 ± 8 | 0.001 |
| Age (years old) | 67.5 ± 10.3 | 63.2 ± 11.9 | 0.001 |
| Antiplatelet agent | 316 (62.3) | 3330 (71.0) | 0.001 |
| Antihypertensive drugs | 314 (61.9) | 2606 (55.6) | 0.006 |
| Cholesterol lowering drugs | 280 (55.2) | 2701 (57.6) | 0.307 |
| Active smokers | 79 (28.0) | 702 (30.9) | 0.713 |
| Pain by history on left buttock | 281 (55.4) | 1300 (27.7) | 0.001 |
| Pain by history on right buttock | 281 (55.4) | 1318 (28.1) | 0.001 |
| Pain by history on left thigh | 136 (26.8) | 769 (16.4) | 0.001 |
| Pain by history on right thigh | 134 (26.4) | 758 (16.2) | 0.001 |
| Pain by history on left calf | 262 (51.7) | 2430 (51.8) | 0.954 |
| Pain by history on right calf | 256 (50.5) | 2536 (54.1) | 0.128 |
| Time over 10 m (s) | 10.4 ± 2.7 | 9.7 ± 2.2 | 0.001 |
| History of cardiovascular disease | 230 (45.4) | 3061 (65.6) | 0.001 |
| History of lower limb revascularization | 78 (23.3) | 682 (25.5) | 0.610 |
| LEAD according to ABI (<0.90 or >1.40) | 230 (45.4) | 2237 (47.7) | 0.318 |
| Right positive ABI | 179 (35.3) | 1780 (38.0) | 0.243 |
| Left positive ABI | 165 (32.5) | 1907 (40.7) | 0.001 |
| History of LSS | No History of LSS | p | |
|---|---|---|---|
| Maximal walking time (sec) | 291 [170; 563] | 302 [180; 678] | 0.007 |
| Heart rate at rest (beats/min) | 80 ± 14 | 80 ± 15 | 0.315 |
| Heart rate at end exercise (beats/min) | 119 ± 22 | 120 ± 23 | 0.104 |
| Chest TcpO2 at rest (mm Hg) | 67 ± 12 | 67 ± 13 | 0.932 |
| Minimal chest TcpO2 (mm Hg) | 62 ± 12 | 62 ± 13 | 0.532 |
| Left buttock TcpO2 at rest (mm Hg) | 68 ± 11 | 69 ± 13 | 0.281 |
| Left calf TcpO2 at rest (mm Hg) | 70 ± 10 | 71 ± 12 | 0.031 |
| Right buttock TcpO2 at rest (mm Hg) | 68 ± 11 | 69 ± 12 | 0.216 |
| Right calf TcpO2 at rest (mm Hg) | 70 ±11 | 71 ± 13 | 0.128 |
| Left buttock DROPmin (mm Hg) | −9 [−16; −5] | −11 [−20; −6] | 0.001 |
| Left calf DROPmin (mm Hg) | −11 [−19; −6] | −15 [−26; −8] | 0.001 |
| Right buttock DROPmin (mm Hg) | −8 [−15; −5] | −11 [−19; −6] | 0.001 |
| Right calf DROPmin (mm Hg) | −10 [−17; −6] | −14 [−27; −8] | 0.001 |
| DROPmin < −15 mmHg on one or both buttocks | 173 (34.2) | 2071(44.2) | 0.001 |
| DROPmin < −15 mmHg on one or both calves | 206 (40.6) | 2874 (61.3) | 0.001 |
| Left buttock pain on treadmill | 214 (42.2) | 1199 (25.6) | 0.001 |
| Right buttock pain on treadmill | 206 (40.6) | 1208 (25.8) | 0.001 |
| Left thigh pain on treadmill | 49 (9.7) | 309 (6.6) | 0.010 |
| Right thigh pain on treadmill | 48 (9.5) | 322 (6.9) | 0.020 |
| Left calf pain on treadmill | 239 (47.1) | 2464 (52.5) | 0.021 |
| Right calf pain on treadmill | 235 (46.4) | 2428 (51.8) | 0.020 |
| Studied Parameters | Beta | SE | Normalised Beta | p | Points for the Score |
|---|---|---|---|---|---|
| ABI+ | 0.219 | 0.013 | 0.237 | <0.001 | +5 |
| Male sex | 0.217 | 0.015 | 0.192 | <0.001 | +4 |
| Antiplatelet treatment | 0.168 | 0.014 | 0.164 | <0.001 | +3 |
| BMI < 26.5 kg/m2 | 0.056 | 0.013 | 0.061 | <0.001 | +1 |
| Lower limb revascularization | 0.059 | 0.019 | 0.045 | <0.01 | +1 |
| Age ≤ 64 years old | 0.033 | 0.013 | 0.035 | 0.01 | +1 |
| Antihypertensive drugs | 0.020 | 1.391 | 0.867 | - | |
| Cholesterol lowering treatment | 0.003 | 0.172 | 0.808 | - | |
| Diabetes mellitus | 0.017 | 1.200 | 0.944 | - | |
| Active smoking | 0.000 | 0.005 | 0.959 | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lecoq, S.; Hersant, J.; Feuilloy, M.; Parent, H.-F.; Henni, S.; Abraham, P. Lower Extremity Arterial Disease and Lumbar Spinal Stenosis: A Study of Exercise-Induced Arterial Ischemia in 5197 Patients Complaining of Claudication. J. Clin. Med. 2022, 11, 5550. https://doi.org/10.3390/jcm11195550
Lecoq S, Hersant J, Feuilloy M, Parent H-F, Henni S, Abraham P. Lower Extremity Arterial Disease and Lumbar Spinal Stenosis: A Study of Exercise-Induced Arterial Ischemia in 5197 Patients Complaining of Claudication. Journal of Clinical Medicine. 2022; 11(19):5550. https://doi.org/10.3390/jcm11195550
Chicago/Turabian StyleLecoq, Simon, Jeanne Hersant, Mathieu Feuilloy, Henri-François Parent, Samir Henni, and Pierre Abraham. 2022. "Lower Extremity Arterial Disease and Lumbar Spinal Stenosis: A Study of Exercise-Induced Arterial Ischemia in 5197 Patients Complaining of Claudication" Journal of Clinical Medicine 11, no. 19: 5550. https://doi.org/10.3390/jcm11195550