
Oral Fluorescein Angiography with Ultra-Wide-Field Scanning Laser Ophthalmoscopy in Pediatric Patients Precis: Oral Fluorescein Angiography in Children

Abstract
:1. Introduction
2. Methods
3. Procedures
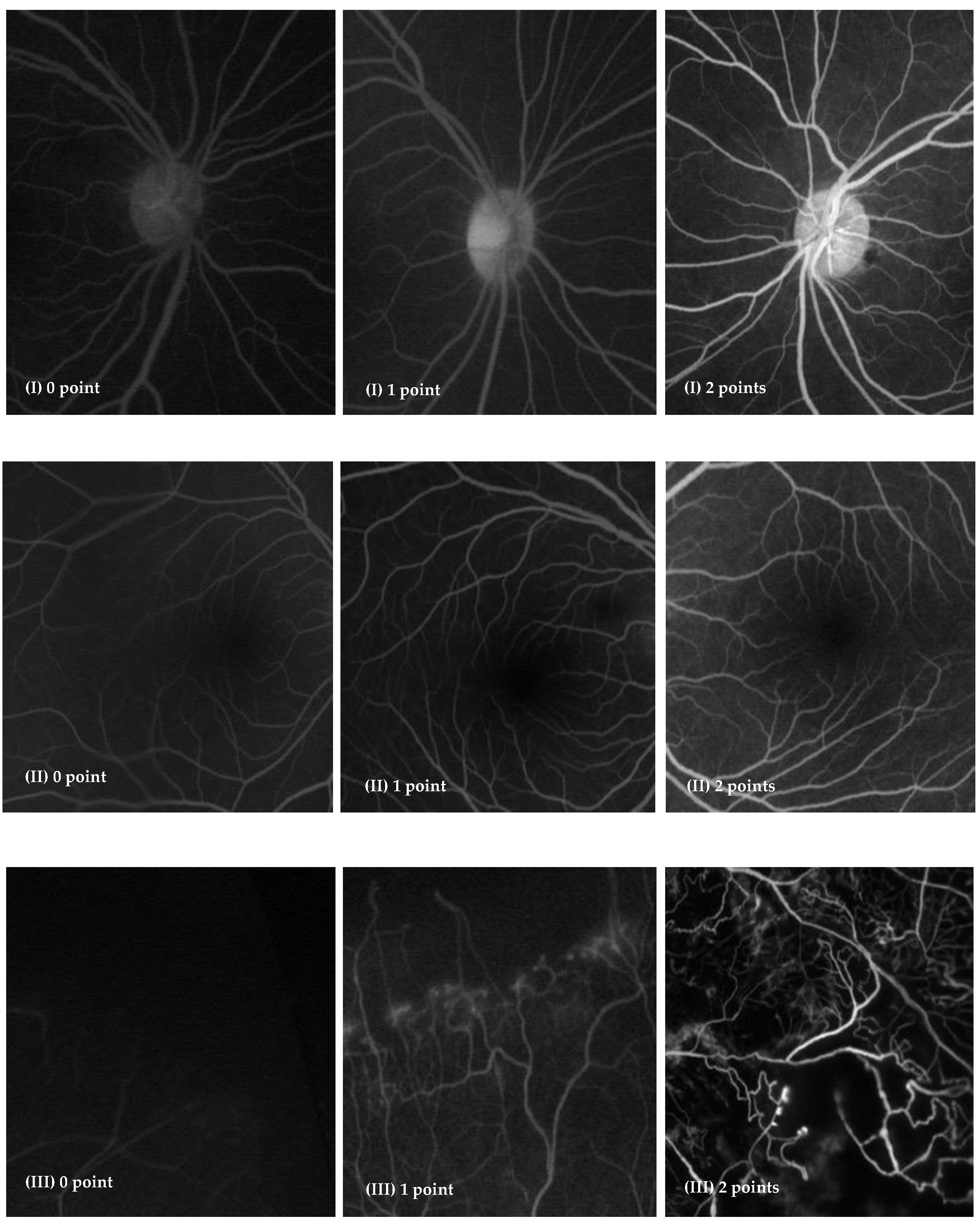
4. Image Analysis
5. Statistical Analysis
6. Results
6.1. Success Rate of Image Obtaining
6.2. Image Quality Analysis
6.3. Adverse Events
7. Discussion
8. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hayreh, S.S. Recent advances in fluorescein fundus angiography. Br. J. Ophthalmol. 1974, 58, 391–412. [Google Scholar] [CrossRef]
- Patel, S.N.; Klufas, M.A.; Ryan, M.C.; Jonas, K.E.; Ostmo, S.; Martinez-Castellanos, M.A.; Berrocal, A.M.; Chiang, M.F.; Chan, R.P. Color Fundus Photography Versus Fluorescein Angiography in Identification of the Macular Center and Zone in Retinopathy of Prematurity. Am. J. Ophthalmol. 2015, 159, 950–957.e2. [Google Scholar] [CrossRef] [PubMed]
- Hans, A.; Narang, S.; Sindhu, M.; Jain, S.; Chawla, D. Fundus fluorescein angiography in retinopathy of prematurity. Eye 2021, 36, 1604–1609. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, P.J.; Davies, N.P. An Innocuous Adverse Effect of Routine Fundus Fluorescein Angiography. JAMA Ophthalmol. 2016, 134, e153624. [Google Scholar] [CrossRef] [PubMed]
- Garcia, C.R.; E Rivero, M.; Bartsch, D.-U.; Ishiko, S.; Takamiya, A.; Fukui, K.; Hirokawa, H.; Clark, T.; Yoshida, A.; Freeman, W.R. Oral fluorescein angiography with the confocal scanning laser ophthalmoscope. Ophthalmology 1999, 106, 1114–1118. [Google Scholar] [CrossRef]
- Su, Z.; Ye, P.; Teng, Y.; Zhang, L.; Shu, X. Adverse Reaction in Patients with Drug Allergy History After Simultaneous Intravenous Fundus Fluorescein Angiography and Indocyanine Green Angiography. J. Ocul. Pharmacol. Ther. 2012, 28, 410–413. [Google Scholar] [CrossRef]
- Balogh, V.J. The use of oral fluorescein angiography in idiopathic central serous choroidopathy. J. Am. Optom. Assoc. 1986, 57, 909–913. [Google Scholar]
- Yamao, S.; Tsujioka, T.; Takada, R.; Matsumoto, F.; Kusaka, S. Utility of Oral Fluorescein Angiography with Ultra-wide-field Imaging System for Evaluation of Various Retinal Disorders. Retina 2020, 41, 1338–1345. [Google Scholar] [CrossRef]
- Sugimoto, M.; Matsubara, H.; Miyata, R.; Matsui, Y.; Ichio, A.; Kondo, M. Ultra-WideField fluorescein angiography by oral administration of fluorescein. Acta Ophthalmol. 2014, 92, e417–e418. [Google Scholar] [CrossRef]
- Kornblau, I.S.; El-Annan, J.F. Adverse reactions to fluorescein angiography: A comprehensive review of the literature. Surv. Ophthalmol. 2019, 64, 679–693. [Google Scholar] [CrossRef]
- Hara, T.; Inami, M.; Hara, T. Efficacy and safety of fluorescein angiography with orally administered sodium fluorescein. Am. J. Ophthalmol. 1998, 126, 560–564. [Google Scholar] [CrossRef]
- Kelley, J.S.; Kincaid, M. Retinal Fluorography Using Oral Fluorescein. Arch. Ophthalmol. 1979, 97, 2331–2332. [Google Scholar] [CrossRef] [PubMed]
- Squirrell, D.; Dinakaran, S.; Dhingra, S.; Mody, C.; Brand, C.; Talbot, J. Oral fluorescein angiography with the scanning laser ophthalmoscope in diabetic retinopathy: A case controlled comparison with intravenous fluorescein angiography. Eye 2004, 19, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Fung, T.H.M.; Muqit, M.M.K.; Mordant, D.J.; Smith, L.M.; Patel, C.K. Noncontact High-Resolution Ultra–Wide-Field Oral Fluorescein Angiography in Premature Infants With Retinopathy of Prematurity. JAMA Ophthalmol. 2014, 132, 108. [Google Scholar] [CrossRef]
- Ali, S.M.A.; Khan, I.; Khurram, D.; Kozak, I. Ultra-Widefield Angiography With Oral Fluorescein in Pediatric Patients With Retinal Disease. JAMA Ophthalmol. 2018, 136, 593–594. [Google Scholar] [CrossRef]
- Amador-Patarroyo, M.J.; Lin, T.; Meshi, A.; Dans, K.C.; Chen, K.; Borooah, S.; Molano-Gonzalez, N.; Díaz, J.; Freeman, W.R. Identifying the factors for improving quality of oral fluorescein angiography. Br. J. Ophthalmol. 2019, 104, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Taddio, A.; Ipp, M.; Thivakaran, S.; Jamal, A.; Parikh, C.; Smart, S.; Sovran, J.; Stephens, D.; Katz, J. Survey of the prevalence of immunization non-compliance due to needle fears in children and adults. Vaccine 2012, 30, 4807–4812. [Google Scholar] [CrossRef]
- Nir, Y.; Paz, A.; Sabo, E.; Potasman, I. Fear of injections in young adults: Prevalence and associations. Am. J. Trop. Med. Hyg. 2003, 68, 341–344. [Google Scholar] [CrossRef]
- Orenius, T.; Psych, L.; Säilä, H.; Mikola, K.; Ristolainen, L. Fear of Injections and Needle Phobia Among Children and Adolescents: An Overview of Psychological, Behavioral, and Contextual Factors. SAGE Open Nurs. 2018, 4, 2377960818759442. [Google Scholar] [CrossRef]
- Kwiterovich, K.A.; Maguire, M.G.; Murphy, R.P.; Schachat, A.P.; Bressler, N.M.; Bressler, S.B.; Fine, S.L. Frequency of Adverse Systemic Reactions after Fluorescein Angiography. Ophthalmology 1991, 98, 1139–1142. [Google Scholar] [CrossRef]
- Newsom, R.; Moate, B.; Casswell, T. Screening for diabetic retinopathy using digital colour photography and oral fluorescein angiography. Eye 2000, 14, 579–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Razvi, F.M.; Kritzinger, E.E.; Tsaloumas, M.D.; Ryder, R.E.J. Use of oral fluorescein angiography in the diagnosis of macular oedema within a diabetic retinopathy screening programme. Diabet. Med. 2001, 18, 1003–1006. [Google Scholar] [CrossRef] [PubMed]
- Bartsch, D.-U.; Elmusharaf, A.; El-Bradey, M.; Freeman, W.R. Oral Fluorescein Angiography in Patients With Choroidal Neovascularization and Macular Degeneration. Ophthalmic Surg. Lasers Imaging Retin. 2003, 34, 17–24. [Google Scholar] [CrossRef]
- Inger, H.E.; Jordan, C.O.; Yanoga, F.; Rogers, D. Equivalence of Oral Fluorescein Angiography to Intravenous Fluorescein Angiography in Evaluating Pediatric Optic Nerve Pathology. J. Pediatr. Ophthalmol. Strabismus 2019, 56, e68–e72. [Google Scholar] [CrossRef] [PubMed]
- Marmoy, O.R.; Henderson, R.H.; Ooi, K. Recommended protocol for performing oral fundus fluorescein angiography (FFA) in children. Eye 2020, 36, 234–236. [Google Scholar] [CrossRef]
- Watson, A.P.; Rosen, E.S. Oral fluorescein angiography: Reassessment of its relative safety and evaluation of optimum conditions with use of capsules. Br. J. Ophthalmol. 1990, 74, 458–461. [Google Scholar] [CrossRef]
- Barteselli, G.; Chhablani, J.; Na Lee, S.; Wang, H.; El Emam, S.; Kozak, I.; Cheng, L.; Bartsch, D.-U.; Azen, S.; Freeman, W.R. Safety and efficacy of oral fluorescein angiography in detecting macular edema in comparison with spectral-domain optical coherence tomography. Retina 2013, 33, 1574–1583. [Google Scholar] [CrossRef]
- Kwan, A.S.; Barry, C.; McAllister, I.L.; Constable, I. Fluorescein angiography and adverse drug reactions revisited: The Lions Eye experience. Clin. Exp. Ophthalmol. 2006, 34, 33–38. [Google Scholar] [CrossRef]
- Chee, R.-I.; Gupta, M.P.; Valikodath, N.G.; Cole, E.; Orlin, A.; Al-Khaled, T.; Rusu, I.; Patel, S.N.; Han, J.; Yap, V.; et al. Evaluation of Potential Systemic Adverse Events Related to Fluorescein Angiography in Pediatric Patients. Ophthalmol. Retin. 2019, 4, 595–601. [Google Scholar] [CrossRef]
- Patel, M.; Kiss, S. Ultra-wide-field fluorescein angiography in retinal disease. Curr. Opin. Ophthalmol. 2014, 25, 213–220. [Google Scholar] [CrossRef]
- Fung, T.H.; Yusuf, I.H.; Xue, K.; Smith, L.M.; Patel, C.K. Heidelberg Spectralis Ultra-Widefield Fundus Fluorescein Angiography in Infants. Am. J. Ophthalmol. 2015, 159, 78–84.e2. [Google Scholar] [CrossRef] [PubMed]
- Gunay, M.; Tugcugil, E.; Somuncu, A.M.; Kola, M.; Turk, A.; Uzlu, D.; Kose, B.; Erdol, H. The clinical use of ultra—Wide field imaging and intravenous fluorescein angiography in infants with retinopathy of prematurity. Photodiagnosis Photodyn. Ther. 2021, 37, 102658. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Case No. | Sex | Age Rangs (Years) | Weight (kg) | Diagnosis | Eyes | Images Score of Oral FFA (OD/OS) | Images Score of IV FFA (OD/OS) | p Value of Total Score |
|---|---|---|---|---|---|---|---|---|
| 1 | Male | <10 | 20 | FEVR | OU | 6/6 | 6/6 | 0.2500 |
| 2 | Male | <10 | 22 | HM | OS | Normal/6 | Normal/6 | |
| 3 | Male | 10 s | 39 | FEVR | OU | 6/6 | 6/6 | |
| 4 | Male | 10 s | 31 | FEVR | OU | 6/6 | 6/6 | |
| 5 | Male | <10 | 18 | FEVR | OU | 6/6 | 6/6 | |
| 6 | Male | <10 | 22 | FEVR | OU | 6/6 | 6/6 | |
| 7 | Female | 10 s | 31 | OT | OS | Normal/5 | Normal/6 | |
| 8 | Male | <10 | 21 | Coat’s | OS | Normal/6 | Normal/6 | |
| 9 | Male | <10 | 20 | FEVR | OS | Normal/4 | Normal/5 | |
| 10 | Female | 10 s | 33 | Coat’s | OD | 6/Normal | 6/Normal | |
| 11 | Male | <10 | 23 | Coat’s | OS | Normal/5 | Normal/6 | |
| 12 | Male | 10 s | 39 | OT | OS | Normal/4 | Normal/4 | |
| 13 | Male | 10 s | 54 | Uveitis | OS | 6/6 | 6/6 | |
| 14 | Female | <10 | 27 | FEVR | OU | 6/6 | 6/6 | |
| 15 | Female | 10 s | 50 | Uveitis | OD | 6/Normal | 6/Normal | |
| 16 | Female | <10 | 17 | Uveitis | OU | 6/6 | 6/6 | |
| 17 | Male | <10 | 32 | FEVR | OU | 4/6 | 4/6 | |
| 18 | Male | <10 | 23 | Coat’s | OS | Normal/6 | Normal/6 | |
| 19 | Female | <10 | 21 | OT | OS | Normal/6 | Normal/6 | |
| 20 | Male | <10 | 24 | Coat’s | OS | Normal/4 | Normal/4 | |
| 21 | Male | <10 | 30 | FEVR | OS | 6/4 | 6/4 | |
| 22 | Male | <10 | 27 | FEVR | OU | 6/6 | 6/6 | |
| 23 | Female | <10 | 16 | FEVR | OU | 6/6 | 6/6 | |
| 24 | Female | <10 | 15 | Uveitis | OS | Normal/6 | Normal/6 |
| Characteristics | Oral FA (n, %) | IVFA (n, %) | p Value |
|---|---|---|---|
| I. Visualization of branch retinal vessels visualization | 36(100%) | 36 (100%) | 1.000 |
| II. Visualization of foveal avascular zone | 32 (100%) | 32 (100%) | |
| III. Identification of clinically important findings | 28 (100%) | 28 (100%) | |
| Microaneurysms | 4 (100%) | 4 (100%) | |
| Neovascularization | 4 (100%) | 4 (100%) | |
| Leakage | 9 (100%) | 9 (100%) | |
| Significant nonperfusion | 11 (100%) | 11 (100%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jiang, Z.; Sun, L.; Hou, A.; Zhang, T.; Lai, Y.; Huang, L.; Ding, X. Oral Fluorescein Angiography with Ultra-Wide-Field Scanning Laser Ophthalmoscopy in Pediatric Patients Precis: Oral Fluorescein Angiography in Children. J. Clin. Med. 2022, 11, 5421. https://doi.org/10.3390/jcm11185421
Jiang Z, Sun L, Hou A, Zhang T, Lai Y, Huang L, Ding X. Oral Fluorescein Angiography with Ultra-Wide-Field Scanning Laser Ophthalmoscopy in Pediatric Patients Precis: Oral Fluorescein Angiography in Children. Journal of Clinical Medicine. 2022; 11(18):5421. https://doi.org/10.3390/jcm11185421
Chicago/Turabian StyleJiang, Zhaoxin, Limei Sun, Aohan Hou, Ting Zhang, Yanting Lai, Li Huang, and Xiaoyan Ding. 2022. "Oral Fluorescein Angiography with Ultra-Wide-Field Scanning Laser Ophthalmoscopy in Pediatric Patients Precis: Oral Fluorescein Angiography in Children" Journal of Clinical Medicine 11, no. 18: 5421. https://doi.org/10.3390/jcm11185421