
Liver Fibrosis Indices Predict the Severity of SARS-CoV-2 Infection
 , , , ,
, , , , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Participants
2.3. Baseline Evaluation and Biochemical Measurements
2.4. Statistical Analysis
3. Results
3.1. Baseline Characterization of the Study Population
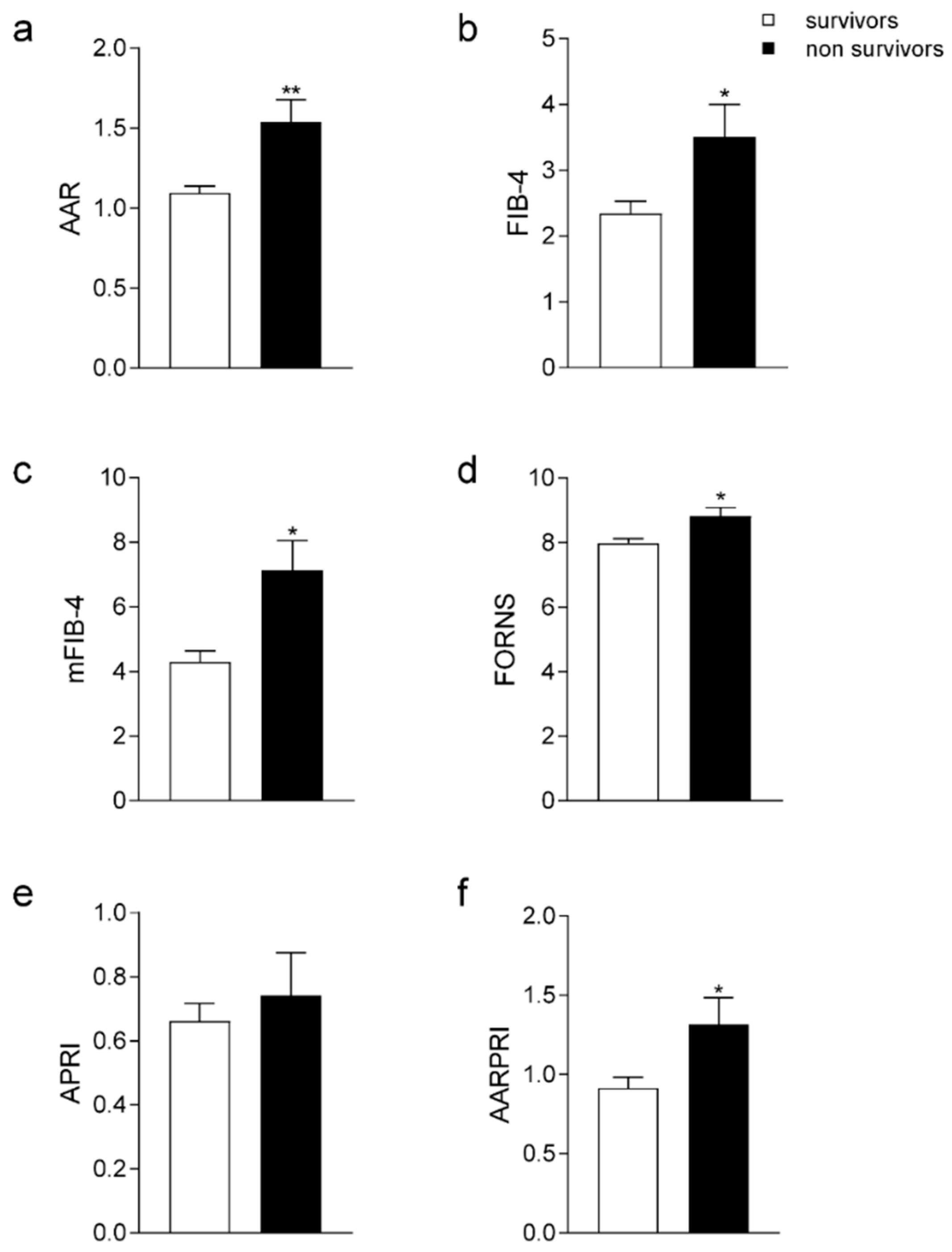
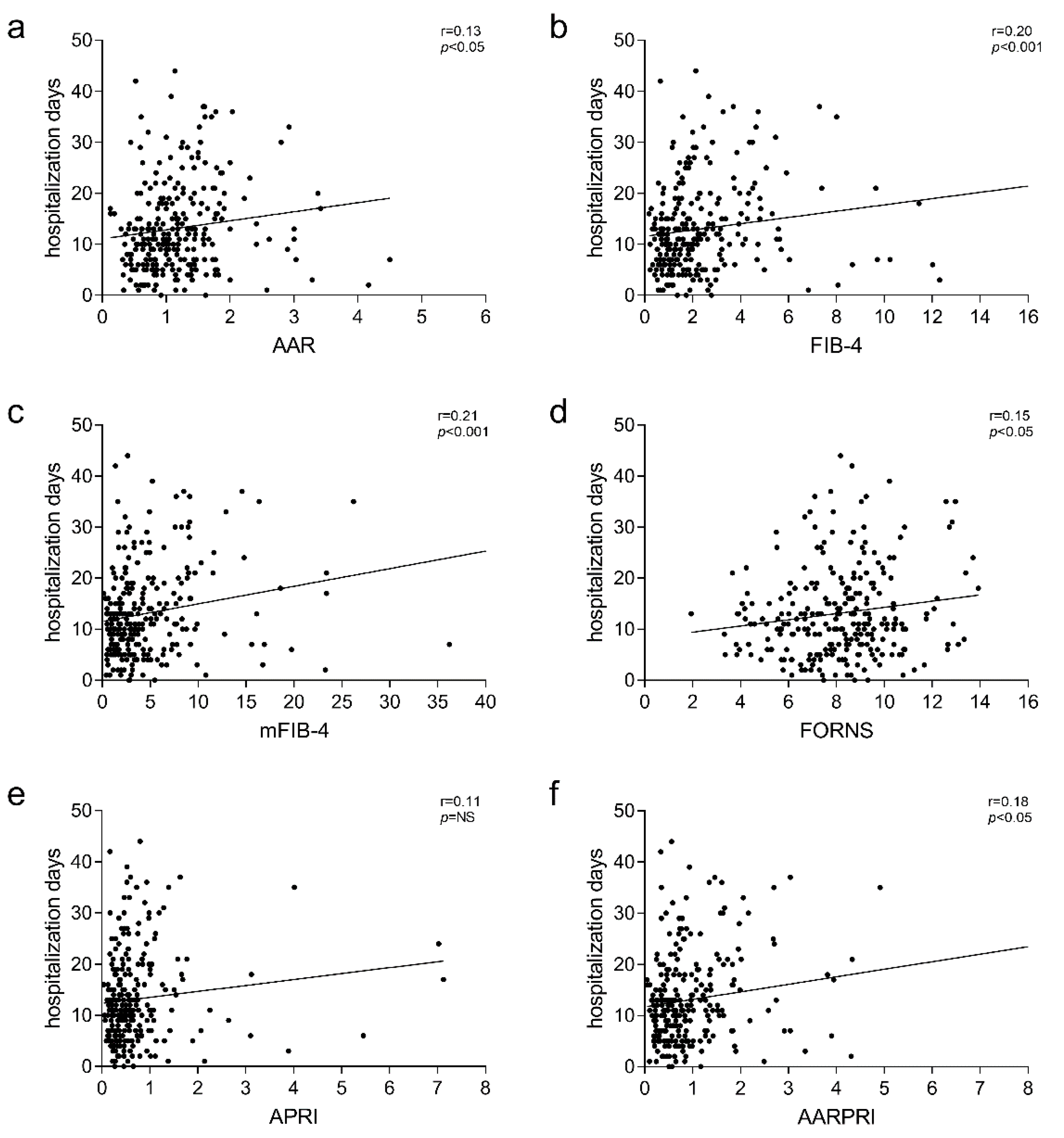
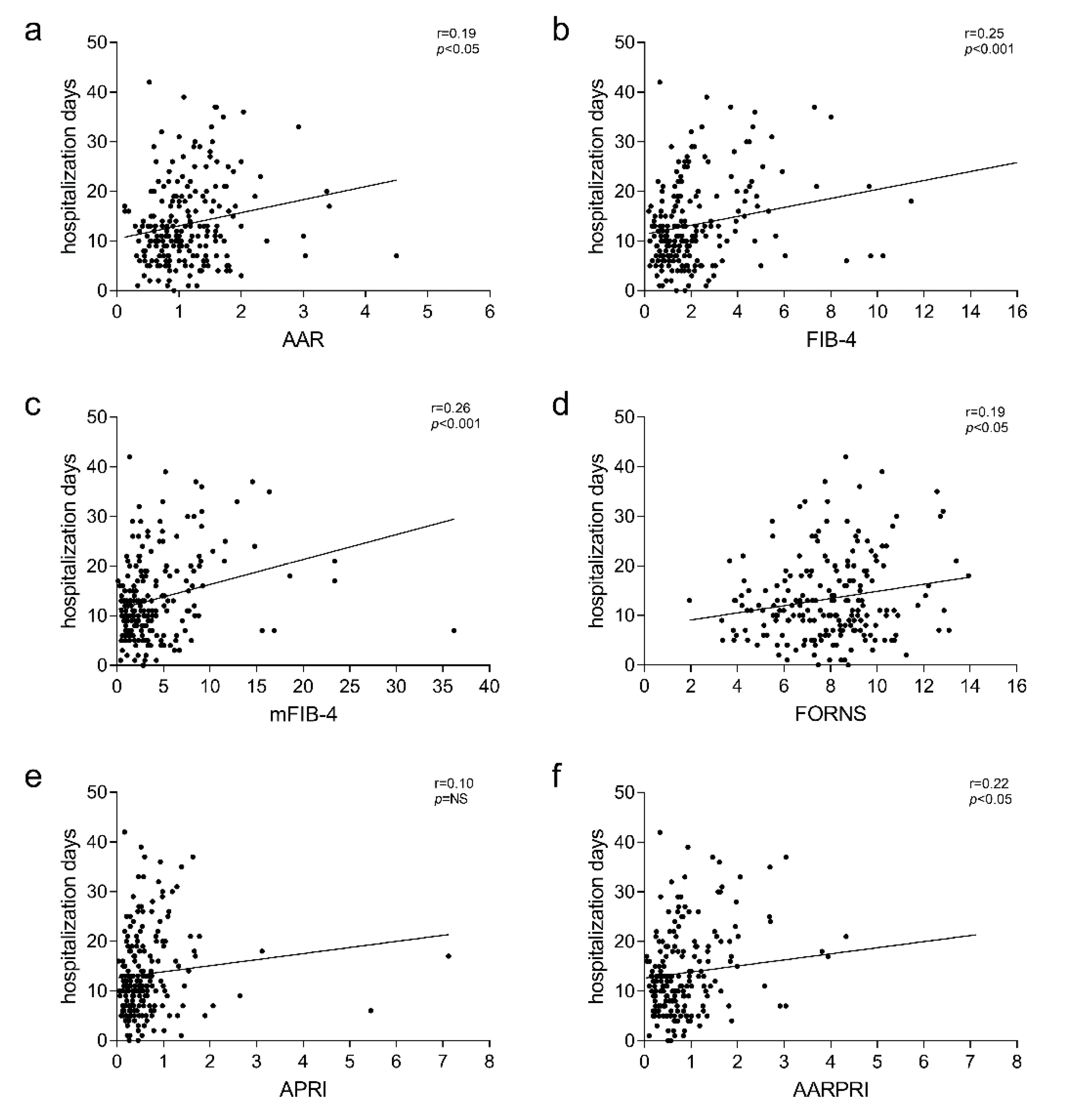
3.2. Liver Fibrosis Scores among Discharged, Admitted to Intensive Care Unit (ICU), and Non-Survivor Patients
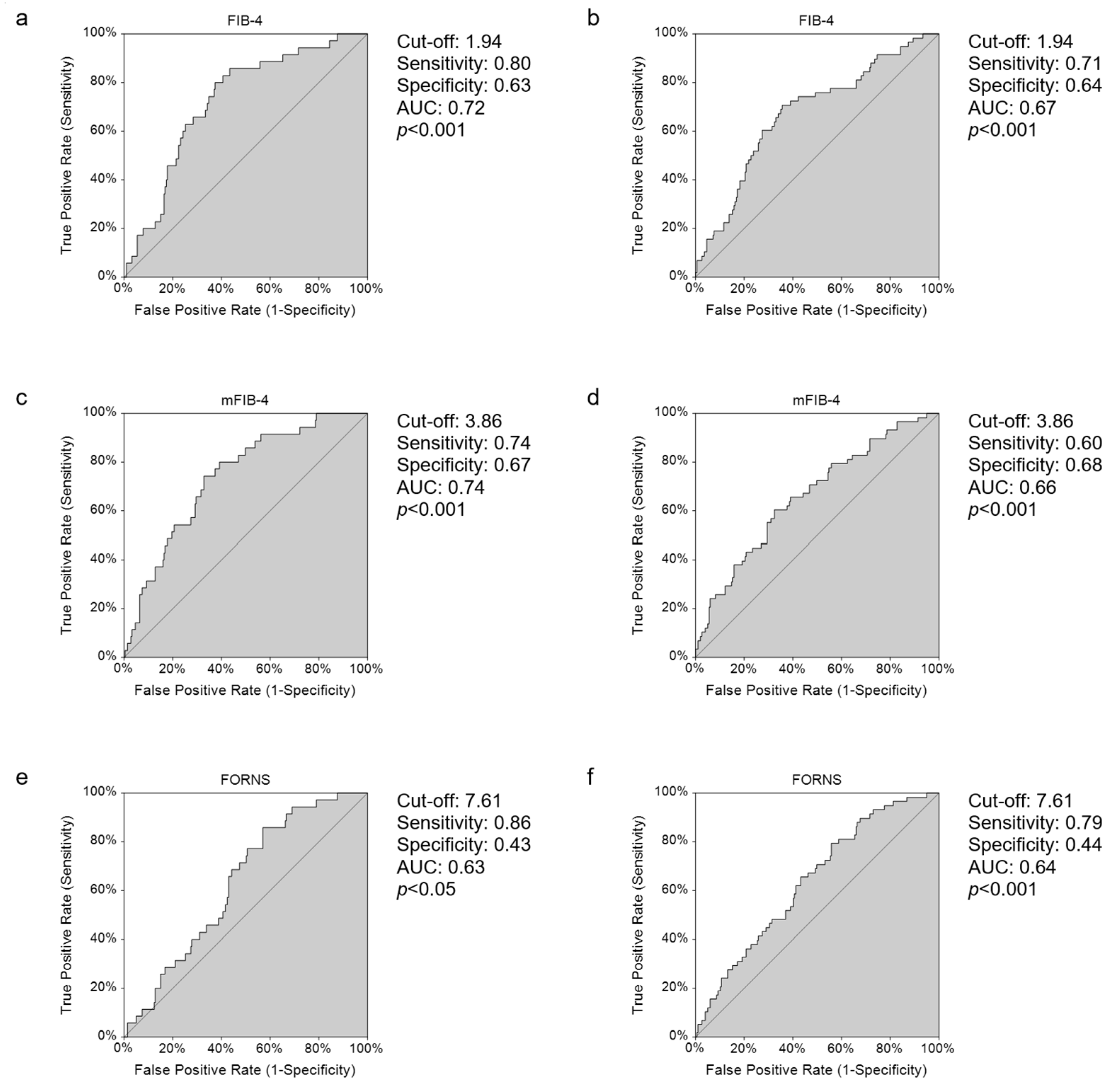
3.3. ROC Curve Analysis of Non-Invasive Scores of Liver Fibrosis to Evaluate the Best Predictor for Mortality and Severity in COVID-19
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Sun, K.; Gu, L.; Ma, L.; Duan, Y. Atlas of ACE2 Gene Expression Reveals Novel Insights into Transmission of SARS-CoV-2. Heliyon 2021, 7, e05850. [Google Scholar] [CrossRef]
- Ackermann, M.; Verleden, S.E.; Kuehnel, M.; Haverich, A.; Welte, T.; Laenger, F.; Vanstapel, A.; Werlein, C.; Stark, H.; Tzankov, A.; et al. Pulmonary Vascular Endothelialitis, Thrombosis, and Angiogenesis in Covid-19. N. Engl. J. Med. 2020, 383, 120–128. [Google Scholar] [CrossRef]
- Crudele, L.; Piccinin, E.; Moschetta, A. Visceral Adiposity and Cancer: Role in Pathogenesis and Prognosis. Nutrients 2021, 13, 2101. [Google Scholar] [CrossRef]
- Dietz, W.; Santos-Burgoa, C. Obesity and Its Implications for COVID-19 Mortality. Obesity 2020, 28, 1005. [Google Scholar] [CrossRef]
- Zammit, C.; Liddicoat, H.; Moonsie, I.; Makker, H. Obesity and Respiratory Diseases. Int. J. Gen. Med. 2010, 3, 335–343. [Google Scholar] [CrossRef]
- Koenig, S.M. Pulmonary Complications of Obesity. Am. J. Med. Sci. 2001, 321, 249–279. [Google Scholar] [CrossRef]
- Bellentani, S.; Saccoccio, G.; Masutti, F.; Crocè, L.S.; Brandi, G.; Sasso, F.; Cristanini, G.; Tiribelli, C. Prevalence of and Risk Factors for Hepatic Steatosis in Northern Italy. Ann. Intern. Med. 2000, 132, 112–117. [Google Scholar] [CrossRef]
- Dulai, P.S.; Singh, S.; Patel, J.; Soni, M.; Prokop, L.J.; Younossi, Z.; Sebastiani, G.; Ekstedt, M.; Hagstrom, H.; Nasr, P.; et al. Increased Risk of Mortality by Fibrosis Stage in Nonalcoholic Fatty Liver Disease: Systematic Review and Meta-Analysis. Hepatology 2017, 65, 1557–1565. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis—2021 Update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Giboney, P.T. Mildly Elevated Liver Transaminase Levels in the Asymptomatic Patient. Am. Fam. Physician 2005, 71, 1105–1110. [Google Scholar]
- Kim, B.K.; Kim, D.Y.; Park, J.Y.; Ahn, S.H.; Chon, C.Y.; Kim, J.K.; Paik, Y.H.; Lee, K.S.; Park, Y.N.; Han, K.H. Validation of FIB-4 and Comparison with Other Simple Noninvasive Indices for Predicting Liver Fibrosis and Cirrhosis in Hepatitis B Virus-Infected Patients. Liver Int. 2010, 30, 546–553. [Google Scholar] [CrossRef]
- McPherson, S.; Hardy, T.; Dufour, J.-F.; Petta, S.; Romero-Gomez, M.; Allison, M.; Oliveira, C.P.; Francque, S.; Van Gaal, L.; Schattenberg, J.M.; et al. Age as a Confounding Factor for the Accurate Non-Invasive Diagnosis of Advanced NAFLD Fibrosis. Am. J. Gastroenterol. 2017, 112, 740–751. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.-W.; Peng, C.-Y.; Lai, H.-C.; Su, W.-P.; Lin, C.-H.; Chuang, P.-H.; Chen, S.-H.; Chen, C.-H.; Hsu, W.-F.; Huang, G.-T. New Noninvasive Index for Predicting Liver Fibrosis in Asian Patients with Chronic Viral Hepatitis. Sci. Rep. 2017, 7, 3259. [Google Scholar] [CrossRef] [PubMed]
- Forns, X.; Ampurdanès, S.; Llovet, J.M.; Aponte, J.; Quintó, L.; Martínez-Bauer, E.; Bruguera, M.; Sánchez-Tapias, J.M.; Rodés, J. Identification of Chronic Hepatitis C Patients without Hepatic Fibrosis by a Simple Predictive Model. Hepatology 2002, 36, 986–992. [Google Scholar] [CrossRef]
- Li, Y.; Regan, J.; Fajnzylber, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Atyeo, C.; Fischinger, S.; Gillespie, E.; et al. Liver Fibrosis Index FIB-4 Is Associated with Mortality in COVID-19. Hepatol. Commun. 2021, 5, 434–445. [Google Scholar] [CrossRef] [PubMed]
- De Matteis, C.; Cariello, M.; Graziano, G.; Battaglia, S.; Suppressa, P.; Piazzolla, G.; Sabbà, C.; Moschetta, A. AST to Platelet Ratio Index (APRI) Is an Easy-to-Use Predictor Score for Cardiovascular Risk in Metabolic Subjects. Sci. Rep. 2021, 11, 14834. [Google Scholar] [CrossRef] [PubMed]
- Cifci, S.; Ekmen, N. Evaluation of Non-Invasive Fibrosis Markers in Predicting Esophageal Variceal Bleeding. Clin. Endosc. 2021, 54, 857–863. [Google Scholar] [CrossRef]
- Wang, H.; Wu, J.; Yang, X.; Liu, J.; Tao, W.; Hao, Z.; Wu, B.; Liu, M.; Zhang, S.; Wang, D. Liver Fibrosis Indices Associated with Substantial Hematoma Expansion in Chinese Patients with Primary Intracerebral Hemorrhage. BMC Neurol. 2021, 21, 478. [Google Scholar] [CrossRef]
- Campos-Murguía, A.; Román-Calleja, B.M.; Toledo-Coronado, I.V.; González-Regueiro, J.A.; Solís-Ortega, A.A.; Kúsulas-Delint, D.; Cruz-Contreras, M.; Cruz-Yedra, N.; Cubero, F.J.; Nevzorova, Y.A.; et al. Liver Fibrosis in Patients with Metabolic Associated Fatty Liver Disease Is a Risk Factor for Adverse Outcomes in COVID-19. Dig. Liver Dis. 2021, 53, 525–533. [Google Scholar] [CrossRef]
- Crisan, D.; Avram, L.; Grapa, C.; Dragan, A.; Radulescu, D.; Crisan, S.; Grosu, A.; Militaru, V.; Buzdugan, E.; Stoicescu, L.; et al. Liver Injury and Elevated FIB-4 Define a High-Risk Group in Patients with COVID-19. J. Clin. Med. 2021, 11, 153. [Google Scholar] [CrossRef]
- Van Eijk, L.E.; Binkhorst, M.; Bourgonje, A.R.; Offringa, A.K.; Mulder, D.J.; Bos, E.M.; Kolundzic, N.; Abdulle, A.E.; van der Voort, P.H.; Olde Rikkert, M.G.; et al. COVID-19: Immunopathology, Pathophysiological Mechanisms, and Treatment Options. J. Pathol. 2021, 254, 307–331. [Google Scholar] [CrossRef] [PubMed]
- Bertolini, A.; Peppel, I.P.; Bodewes, F.A.J.A.; Moshage, H.; Fantin, A.; Farinati, F.; Fiorotto, R.; Jonker, J.W.; Strazzabosco, M.; Verkade, H.J.; et al. Abnormal Liver Function Tests in Patients with COVID-19: Relevance and Potential Pathogenesis. Hepatology 2020, 72, 1864–1872. [Google Scholar] [CrossRef] [PubMed]
- Ejaz, H.; Alsrhani, A.; Zafar, A.; Javed, H.; Junaid, K.; Abdalla, A.E.; Abosalif, K.O.A.; Ahmed, Z.; Younas, S. COVID-19 and Comorbidities: Deleterious Impact on Infected Patients. J. Infect. Public Health 2020, 13, 1833–1839. [Google Scholar] [CrossRef] [PubMed]
- Elfeki, M.A.; Robles, J.; Akhtar, Z.; Ullah, F.; Ganapathiraju, I.; Tran, C.; Inman, C.; Collin, S.M.; Rosa, R. Impact of Fibrosis-4 Index Prior to COVID-19 on Outcomes in Patients at Risk of Non-Alcoholic Fatty Liver Disease. Dig. Dis. Sci. 2021, 67, 3333–3339. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Scorletti, E.; Mosca, A.; Alisi, A.; Byrne, C.D.; Targher, G. Complications, Morbidity and Mortality of Nonalcoholic Fatty Liver Disease. Metabolism 2020, 111, 154170. [Google Scholar] [CrossRef]
- Angulo, P.; Kleiner, D.E.; Dam-Larsen, S.; Adams, L.A.; Bjornsson, E.S.; Charatcharoenwitthaya, P.; Mills, P.R.; Keach, J.C.; Lafferty, H.D.; Stahler, A.; et al. Liver Fibrosis, but No Other Histologic Features, Is Associated with Long-Term Outcomes of Patients with Nonalcoholic Fatty Liver Disease. Gastroenterology 2015, 149, 389–397.e10. [Google Scholar] [CrossRef]
- Belanger, M.J.; Hill, M.A.; Angelidi, A.M.; Dalamaga, M.; Sowers, J.R.; Mantzoros, C.S. Covid-19 and Disparities in Nutrition and Obesity. N. Engl. J. Med. 2020, 383, e69. [Google Scholar] [CrossRef]
- Patel, K.P.; Patel, P.A.; Vunnam, R.R.; Hewlett, A.T.; Jain, R.; Jing, R.; Vunnam, S.R. Gastrointestinal, Hepatobiliary, and Pancreatic Manifestations of COVID-19. J. Clin. Virol. 2020, 128, 104386. [Google Scholar] [CrossRef]
- Aleem, A.; Shah, H. Gastrointestinal And Hepatic Manifestations Of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Zhang, H.; Kang, Z.; Gong, H.; Xu, D.; Wang, J.; Li, Z.; Li, Z.; Cui, X.; Xiao, J.; Zhan, J.; et al. Digestive System Is a Potential Route of COVID-19: An Analysis of Single-Cell Coexpression Pattern of Key Proteins in Viral Entry Process. Gut 2020, 69, 1010–1018. [Google Scholar] [CrossRef]
- Xiao, F.; Tang, M.; Zheng, X.; Liu, Y.; Li, X.; Shan, H. Evidence for Gastrointestinal Infection of SARS-CoV-2. Gastroenterology 2020, 158, 1831–1833.e3. [Google Scholar] [CrossRef]
- Chai, X.; Hu, L.; Zhang, Y.; Han, W.; Lu, Z.; Ke, A.; Zhou, J.; Shi, G.; Fang, N.; Fan, J.; et al. Specific ACE2 Expression in Cholangiocytes May Cause Liver Damage after 2019-NCoV Infection. biorxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Lagana, S.M.; Kudose, S.; Iuga, A.C.; Lee, M.J.; Fazlollahi, L.; Remotti, H.E.; Del Portillo, A.; De Michele, S.; de Gonzalez, A.K.; Saqi, A.; et al. Hepatic Pathology in Patients Dying of COVID-19: A Series of 40 Cases Including Clinical, Histologic, and Virologic Data. Mod. Pathol. 2020, 33, 2147–2155. [Google Scholar] [CrossRef] [PubMed]
- Bangash, M.N.; Patel, J.; Parekh, D. COVID-19 and the Liver: Little Cause for Concern. Lancet Gastroenterol. Hepatol. 2020, 5, 529–530. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Scores | Formulas |
|---|---|
| AAR | |
| FIB-4 | |
| mFIB-4 | |
| FORNS | |
| APRI | |
| AARPRI |
| Clinical Variable | Survivors | Non Survivors | p-Value |
|---|---|---|---|
| n (M:F) | 233 (130:103) | 38 (19:19) | - |
| Age (years) | 67.88 ± 1.027 | 82.68 ± 1.697 | <0.001 |
| Hemoglobin (g/dL) | 12.4 ± 0.163 | 11.9 ± 0.374 | NS |
| WBC (103/µL) | 8.46 ± 0.306 | 9.48 ± 0.798 | NS |
| Monocytes (%) | 6.35 ± 0.212 | 4.39 ± 0.445 | <0.001 |
| Lymphocytes (%) | 16.4 ± 0.75 | 9.5 ± 1.25 | <0.001 |
| Neutrophils (%) | 76.1 ± 0.875 | 85.3 ± 1.45 | <0.001 |
| NLR | 7.83 ± 0.539 | 16.7 ± 2.66 | <0.001 |
| Platelet count (103/μL) | 249 ± 7.98 | 217 ± 17.1 | NS |
| Creatinine (mg/dL) | 1.51 ± 0.262 | 1.5 ± 0.213 | NS |
| Urea (mg/dL) | 58.3 ± 3.01 | 97.8 ± 13.2 | <0.001 |
| Glucose (mg/dL) | 113 ± 3.3 | 137 ± 12 | <0.05 |
| Total Cholesterol (mg/dL) | 156 ± 4.06 | 133 ± 6.1 | <0.05 |
| HDL-c (mg/dL) | 39 ± 1.48 | 34.7 ± 2.67 | NS |
| LDL-c (mg/dL) | 86.3 ± 3.32 | 68.6 ± 5.41 | <0.05 |
| NON HDL-c (mg/dL) | 116 ± 4.31 | 98.6 ± 5.92 | NS |
| TG (mg/dL) | 146 ± 7.54 | 153 ± 13.1 | NS |
| MHR | 0.0148 ± 0.00142 | 0.0135 ± 0.00202 | NS |
| AST (U/I) | 38.8 ± 2.06 | 37.2 ± 3.32 | NS |
| ALT (U/I) | 43.7 ± 3 | 27.9 ± 2.52 | <0.05 |
| GGT (U/I) | 68.1 ± 5.35 | 61.1 ± 14.5 | NS |
| Total Bilirubin (mg/dL) | 0.684 ± 0.0502 | 0.724 ± 0.0896 | NS |
| Ferritin (ng/mL) | 709 ± 62.2 | 712 ± 102 | NS |
| Procalcitonin (ng/mL) | 0.469 ± 0.116 | 3.05 ± 2.3 | <0.05 |
| hs-CRP (mg/L) | 68.2 ± 7.39 | 98.4 ± 10.9 | NS |
| ESR (mm/h) | 65.4 ± 3.27 | 61.9 ± 9.56 | NS |
| LDH (mU/mL) | 303 ± 9.14 | 407 ± 29 | <0.001 |
| CPK (U/L) | 163 ± 32.8 | 198 ± 59.1 | NS |
| Myoglobin (μg/L) | 169 ± 19.4 | 535 ± 316 | <0.05 |
| hs-Troponin (ng/L) | 95.9 ± 29.9 | 574 ± 384 | <0.05 |
| NT-proBNP (pg/mL) | 3562 ± 932 | 6449 ± 1531 | NS |
| TSH (mUI/L) | 1.84 ± 0.355 | 1.18 ± 0.362 | NS |
| FT3 (pg/mL) | 1.63 ± 0.0559 | 1.19 ± 0.105 | <0.05 |
| FT4 (ng/dL) | 1.22 ± 0.0252 | 1.22 ± 0.0625 | NS |
| CUT-OFF Value | Sensitivity | Specificity | Sensitivity + Specificity | AUC | p-Value | |
|---|---|---|---|---|---|---|
| FIB-4_MORTALITY | ≥1.94 | 0.80 | 0.63 | 1.43 | 0.72 | p < 0.001 |
| FIB-4_SEVERITY | ≥1.94 | 0.71 | 0.64 | 1.35 | 0.67 | p < 0.001 |
| mFIB-4_MORTALITY | ≥3.86 | 0.74 | 0.67 | 1.41 | 0.74 | p < 0.001 |
| mFIB-4_SEVERITY | ≥3.86 | 0.60 | 0.68 | 1.28 | 0.66 | p < 0.001 |
| FORNS_MORTALITY | ≥7.61 | 0.86 | 0.43 | 1.29 | 0.63 | p < 0.05 |
| FORNS_SEVERITY | ≥7.61 | 0.79 | 0.44 | 1.23 | 0.64 | p < 0.001 |
| AARPRI_MORTALITY | ≥0.65 | 0.82 | 0.49 | 1.30 | 0.69 | p < 0.001 |
| AARPRI_SEVERITY | ≥1.28 | 0.38 | 0.82 | 1.20 | 0.63 | p < 0.05 |
| AAR_MORTALITY | ≥1.25 | 0.29 | 0.81 | 1.10 | 0.50 | p = NS |
| AAR_SEVERITY | ≥0.72 | 0.59 | 0.48 | 1.07 | 0.48 | p = NS |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crudele, L.; Novielli, F.; Petruzzelli, S.; Battaglia, S.; Giuliano, A.F.M.; Melodia, R.; Morano, C.M.; Dell’Aquila, P.; Moretti, R.; Castorani, L.; et al. Liver Fibrosis Indices Predict the Severity of SARS-CoV-2 Infection. J. Clin. Med. 2022, 11, 5369. https://doi.org/10.3390/jcm11185369
Crudele L, Novielli F, Petruzzelli S, Battaglia S, Giuliano AFM, Melodia R, Morano CM, Dell’Aquila P, Moretti R, Castorani L, et al. Liver Fibrosis Indices Predict the Severity of SARS-CoV-2 Infection. Journal of Clinical Medicine. 2022; 11(18):5369. https://doi.org/10.3390/jcm11185369
Chicago/Turabian StyleCrudele, Lucilla, Fabio Novielli, Stefano Petruzzelli, Stefano Battaglia, Antonio Francesco Maria Giuliano, Rosa Melodia, Chiara Maria Morano, Paola Dell’Aquila, Renata Moretti, Luigi Castorani, and et al. 2022. "Liver Fibrosis Indices Predict the Severity of SARS-CoV-2 Infection" Journal of Clinical Medicine 11, no. 18: 5369. https://doi.org/10.3390/jcm11185369