

How Does Orthodontic Mini-Implant Thread Minidesign Influence the Stability?—Systematic Review with Meta-Analysis

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
2.3. Data Extraction
2.4. Quality Assessment
2.5. Meta-Analysis
3. Results
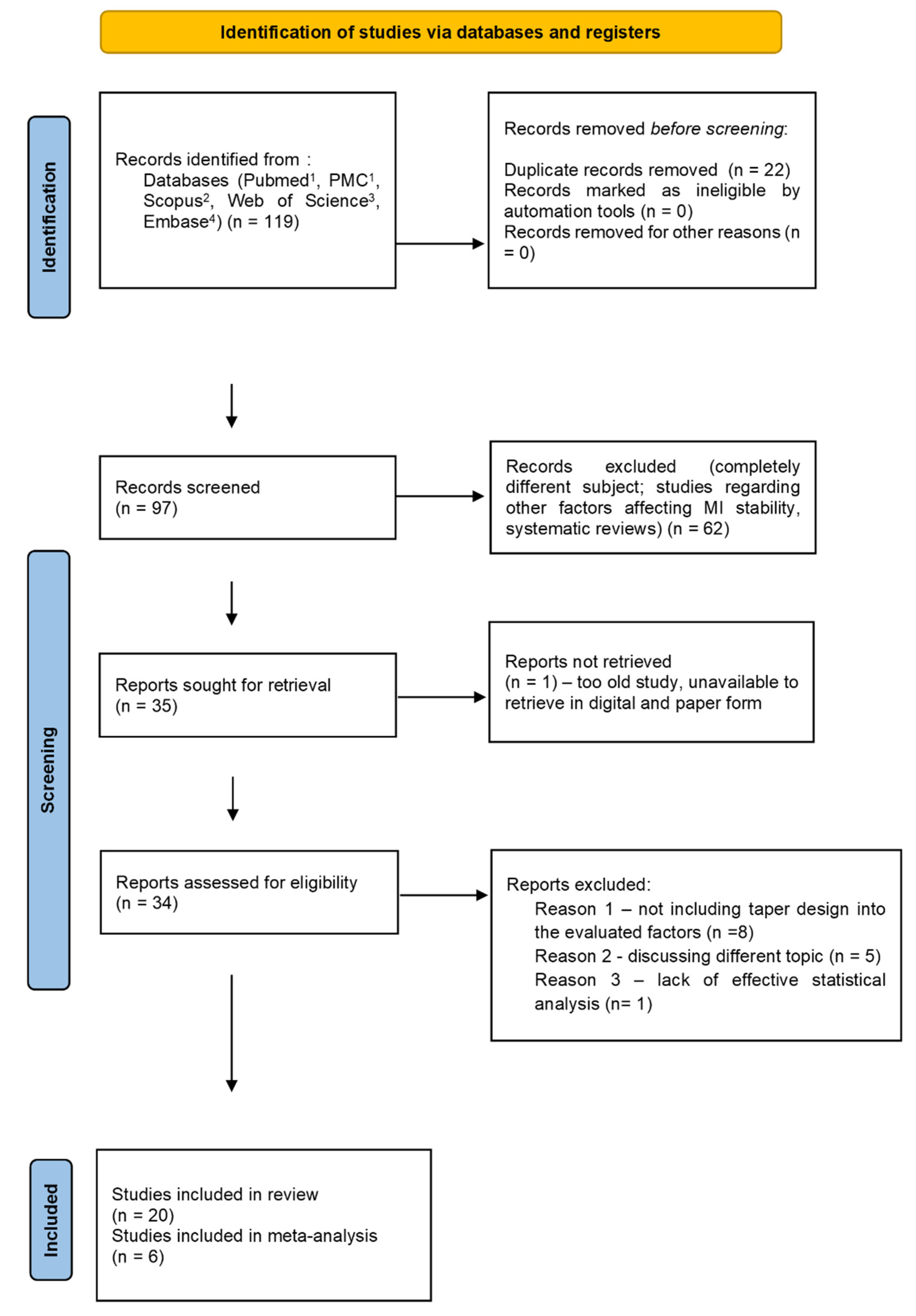
3.1. Results of the Search
3.2. Quality Assessment
3.3. Meta-Analysis
3.3.1. Meta-Analysis of In-Vitro Studies of Peak Load for Pull-Out Strength Regarding Thread Pitch Dimension
- (A)
- artificial bone model
- (B)
- animal bone model
3.3.2. Meta-Analysis of In-Vitro Studies of Peak Load for Pull-Out Strength Regarding Thread Depth
- (A)
- artificial bone model
- (B)
- animal bone model
3.3.3. Meta-Analysis of In-Vitro Studies of Peak Load for Pull-Out Strength Regarding Thread Shape Factor
- (A)
- artificial bone model
- (B)
- animal bone model
4. Discussion
5. Conclusions
- Minidesign of orthodontic mini-implant—that is characteristics such as OMI thread pitch, OMI thread depth, and OMI thread shape should be considered when choosing optimal miniscrews for orthodontic anchorage.
- Thread pitch seems to be of special importance for OMIs retention—OMIs with a more dense thread—should be preferred due to their superior stability.
- Thread depth seems to be of low importance for OMIs stability.
- There is no clear scientific evidence referring to the optimal tread shape factor.
- Studies present in the literature vary greatly in study design and way of reporting results. The results of in-vitro tests carried out on animal models are more consistent than those carried out on artificial bone models.
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Melsen, B. Northcroft Lecture: How Has the Spectrum of Orthodontics Changed over the Past Decades? J. Orthod. 2011, 38, 134–143. [Google Scholar] [CrossRef] [PubMed]
- AlMaghlouth, B.; AlMubarak, A.; Almaghlouth, I.; AlKhalifah, R.; Alsadah, A.; Hassan, A. Thank Orthodontic Intrusion Using Temporary Anchorage Devices Compared to Other Orthodontic Intrusion Methods: A Systematic Review. Clin. Cosmet. Investig. Dent. 2021, 13, 11–19. [Google Scholar] [CrossRef] [PubMed]
- Markic, G.; Katsaros, C.; Pandis, N.; Eliades, T. Temporary Anchorage Device Usage: A Survey among Swiss Orthodontists. Prog. Orthod. 2014, 15, 29. [Google Scholar] [CrossRef]
- Kuroda, S.; Tanaka, E. Application of Temporary Anchorage Devices for the Treatment of Adult Class III Malocclusions. Semin. Orthod. 2011, 17, 91–97. [Google Scholar] [CrossRef]
- Casaña-Ruiz, M.D.; Bellot-Arcís, C.; Paredes-Gallardo, V.; García-Sanz, V.; Almerich-Silla, J.M.; Montiel-Company, J.M. Risk Factors for Orthodontic Mini-Implants in Skeletal Anchorage Biological Stability: A Systematic Literature Review and Meta-Analysis. Sci. Rep. 2020, 10, 5848. [Google Scholar] [CrossRef]
- Bennardo, F.; Barone, S.; Vocaturo, C.; Nucci, L.; Antonelli, A.; Giudice, A. Usefulness of Magnetic Mallet in Oral Surgery and Implantology: A Systematic Review. J. Pers. Med. 2022, 12, 108. [Google Scholar] [CrossRef]
- de Mattos, P.M.; Gonçalves, F.M.; Basso, I.B.; Zeigelboim, B.S.; Niwa, M.F.; Stechman-Neto, J.; Santos, R.S.; de Araujo, C.M.; Guariza-Filho, O. Risk Factors Associated with the Stability of Mini-Implants and Mini-Plates: Systematic Review and Meta-Analysis. Clin. Oral Investig. 2022, 26, 65–82. [Google Scholar] [CrossRef]
- Alharbi, F.; Almuzian, M.; Bearn, D. Miniscrews Failure Rate in Orthodontics: Systematic Review and Meta-Analysis. Eur. J. Orthod. 2018, 40, 519–530. [Google Scholar] [CrossRef]
- Cunha, A.C.; da Veiga, A.M.A.; Masterson, D.; Mattos, C.T.; Nojima, L.I.; Nojima, M.C.G.; Maia, L.C. How Do Geometry-Related Parameters Influence the Clinical Performance of Orthodontic Mini-Implants? A Systematic Review and Meta-Analysis. Int. J. Oral Maxillofac. Surg. 2017, 46, 1539–1551. [Google Scholar] [CrossRef]
- Dalessandri, D.; Salgarello, S.; Dalessandri, M.; Lazzaroni, E.; Piancino, M.; Paganelli, C.; Maiorana, C.; Santoro, F. Determinants for Success Rates of Temporary Anchorage Devices in Orthodontics: A Meta-Analysis (n > 50). Eur. J. Orthod. 2014, 36, 303–313. [Google Scholar] [CrossRef] [Green Version]
- Reynders, R.; Ronchi, L.; Bipat, S. Mini-Implants in Orthodontics: A Systematic Review of the Literature. Am. J. Orthod. Dentofac. Orthop. 2009, 135, 564.e1–564.e19. [Google Scholar] [CrossRef]
- Mecenas, P.; Espinosa, D.G.; Cardoso, P.C.; Normando, D. Stainless Steel or Titanium Mini-Implants? Angle Orthod. 2020, 90, 587–597. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.; Ge, M.; Li, M.; Li, C.; Li, Y.; Li, X.; Zhao, Z. Comparison of the Success Rate between Self-Drilling and Self-Tapping Miniscrews: A Systematic Review and Meta-Analysis. Eur. J. Orthod. 2016, 39, 287–293. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 10, n71. [Google Scholar] [CrossRef] [PubMed]
- Beller, E.M.; Glasziou, P.P.; Altman, D.G.; Hopewell, S.; Bastian, H.; Chalmers, I.; Gøtzsche, P.C.; Lasserson, T.; Tovey, D.; for the PRISMA for Abstracts Group. PRISMA for Abstracts: Reporting Systematic Reviews in Journal and Conference Abstracts. PloS Med. 2013, 10, e1001419. [Google Scholar] [CrossRef]
- PRISMA-S Group; Rethlefsen, M.L.; Kirtley, S.; Waffenschmidt, S.; Ayala, A.P.; Moher, D.; Page, M.J.; Koffel, J.B. PRISMA-S: An Extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions, 1st ed.; Wiley: Hoboken, NJ, USA, 2019; ISBN 978-1-119-53662-8. [Google Scholar]
- Tacconelli, E. Systematic Reviews: CRD’s Guidance for Undertaking Reviews in Health Care. Lancet Infect. Dis. 2010, 10, 226. [Google Scholar] [CrossRef]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef]
- Wong, D.W.-C.; Chen, T.L.-W.; Peng, Y.; Lam, W.-K.; Wang, Y.; Ni, M.; Niu, W.; Zhang, M. An Instrument for Methodological Quality Assessment of Single-Subject Finite Element Analysis Used in Computational Orthopaedics. Med. Nov. Technol. Devices 2021, 11, 100067. [Google Scholar] [CrossRef]
- Sheth, V.H.; Shah, N.P.; Jain, R.; Bhanushali, N.; Bhatnagar, V. Development and Validation of a Risk-of-Bias Tool for Assessing in Vitro Studies Conducted in Dentistry: The QUIN. J. Prosthet. Dent. 2022; in press. [Google Scholar] [CrossRef]
- Del Re, A.C. A practical tutorial on conducting meta-analysis in R. Quant. Methods Psychol. 2015, 11, 37–50. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thompson, S.G. Quantifying heterogeneity in a meta-analysis. Stat. Med. 2002, 21, 1539–1558. [Google Scholar] [CrossRef] [PubMed]
- Hein, J.L. Discrete Structures, Logic, and Computability, 2nd ed.; Jones and Bartlett Publishers: Boston, MA, USA, 2001; ISBN 978-0-7637-1843-5. [Google Scholar]
- Kim, K.-H.; Chung, C.; Yoo, H.-M.; Park, D.-S.; Jang, I.-S.; Kyung, S.-H. The Comparison of Torque Values in Two Types of Miniscrews Placed in Rabbits: Tapered and Cylindrical Shapes—Preliminary Study. Korean J. Orthod. 2011, 41, 280. [Google Scholar] [CrossRef]
- Topcuoglu, T.; Bicakci, A.A.; Avunduk, M.C.; Sahin Inan, Z.D. Evaluation of the Effects of Different Surface Configurations on Stability of Miniscrews. Sci. World J. 2013, 2013, 396091. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.Z.-C.; Chen, Y.-J.; Tung, Y.-Y.; Chiang, Y.-Y.; Lai, E.H.-H.; Chen, W.-P.; Lin, C.-P. Effects of Thread Depth, Taper Shape, and Taper Length on the Mechanical Properties of Mini-Implants. Am. J. Orthod. Dentofac. Orthop. 2012, 141, 279–288. [Google Scholar] [CrossRef]
- Shen, S.; Sun, Y.; Zhang, C.; Yang, Y.; Li, Z.; Cai, X.; Duan, Y.; Li, T. Bivariate Optimization of Orthodontic Mini-Implant Thread Height and Pitch. Int. J. CARS 2015, 10, 109–116. [Google Scholar] [CrossRef]
- Dastenaei, F.; Moghimi Zand, M.; Noorolahian, S. Thread Pitch Variant in Orthodontic Mini-Screws: A 3-D Finite Element Analysis. J. Appl. Mech. 2015, 46, 257–265. [Google Scholar]
- Pouyafar, V.; Meshkabadi, R.; Sadr Haghighi, A.H.; Navid, A. Finite Element Simulation and Statistical Investigation of an Orthodontic Mini-Implant’s Stability in a Novel Screw Design. Proc. Inst. Mech. Eng. Part H J. Eng. Med. 2021, 235, 1046–1057. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Kim, Y.-J.; Yun, P.-Y.; Kim, J.-W. Effects of the Taper Shape, Dual-Thread, and Length on the Mechanical Properties of Mini-Implants. Angle Orthod. 2009, 79, 908–914. [Google Scholar] [CrossRef]
- Gracco, A.; Giagnorio, C.; Incerti Parenti, S.; Alessandri Bonetti, G.; Siciliani, G. Effects of Thread Shape on the Pullout Strength of Miniscrews. Am. J. Orthod. Dentofac. Orthop. 2012, 142, 186–190. [Google Scholar] [CrossRef]
- Migliorati, M.; Signori, A.; Biavati, A.S. Temporary Anchorage Device Stability: An Evaluation of Thread Shape Factor. Eur. J. Orthod. 2012, 34, 582–586. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Migliorati, M.; Benedicenti, S.; Signori, A.; Drago, S.; Cirillo, P.; Barberis, F.; Silvestrini Biavati, A. Thread Shape Factor: Evaluation of Three Different Orthodontic Miniscrews Stability. Eur. J. Orthod. 2013, 35, 401–405. [Google Scholar] [CrossRef] [PubMed]
- Da Cunha, A.C.; de Freitas, A.O.A.; Marquezan, M.; Nojima, L.I. Mechanical Influence of Thread Pitch on Orthodontic Mini-Implant Stability. Braz. Oral Res. 2015, 29, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Walter, A.; Winsauer, H.; Marce-Nogue, J.; Mojal, S.; Puigdollers, A. Design Characteristics, Primary Stability and Risk of Fracture of Orthodontic Mini-Implants: Pilot Scan Electron Microscope and Mechanical Studies. Med. Oral 2013, 18, e804–e810. [Google Scholar] [CrossRef]
- Cha, J.-Y.; Hwang, C.-J.; Kwon, S.H.; Jung, H.-S.; Kim, K.-M.; Yu, H.S. Strain of Bone-Implant Interface and Insertion Torque Regarding Different Miniscrew Thread Designs Using an Artificial Bone Model. Eur. J. Orthod. 2015, 37, 268–274. [Google Scholar] [CrossRef]
- Radwan, E.S.; Montasser, M.A.; Maher, A. Influence of Geometric Design Characteristics on Primary Stability of Orthodontic Miniscrews. J. Orofac. Orthop. 2018, 79, 191–203. [Google Scholar] [CrossRef]
- Katić, V.; Kamenar, E.; Blažević, D.; Špalj, S. Geometrical Design Characteristics of Orthodontic Mini-Implants Predicting Maximum Insertion Torque. Korean J. Orthod. 2014, 44, 177. [Google Scholar] [CrossRef]
- Yashwant, A.V. Does Change in Thread Shape Influence the Pull Out Strength of Mini Implants? An In Vitro Study. J. Clin. Diagn. Res. JCDR 2017, 11, ZC17. [Google Scholar] [CrossRef]
- Sana, S.; Reddy, R.; Talapaneni, A.K.; Hussain, A.; Bangi, S.L.; Fatima, A. Evaluation of Stability of Three Different Mini-Implants, Based on Thread Shape Factor and Numerical Analysis of Stress around Mini-Implants with Different Insertion Angle, with Relation to En-Masse Retraction Force. Dent. Press J. Orthod. 2020, 25, 59–68. [Google Scholar] [CrossRef]
- Watanabe, K.; Mitchell, B.; Sakamaki, T.; Hirai, Y.; Kim, D.G.; Deguchi, T.; Suzuki, M.; Ueda, K.; Tanaka, E. Mechanical stability of orthodontic miniscrew depends on a thread shape. J. Dent. Sci. 2022, 17, 1244–1252. [Google Scholar] [CrossRef]
- Budsabong, C.; Trachoo, V.; Pittayapat, P.; Chantarawaratit, P. The Association between Thread Pitch and Cortical Bone Thickness Influences the Primary Stability of Orthodontic Miniscrew Implants: A Study in Human Cadaver Palates. J. World Fed. Orthod. 2022, 11, 68–73. [Google Scholar] [CrossRef]
- Redžepagić-Vražalica, L.; Mešić, E.; Pervan, N.; Hadžiabdić, V.; Delić, M.; Glušac, M. Impact of Implant Design and Bone Properties on the Primary Stability of Orthodontic Mini-Implants. Appl. Sci. 2021, 11, 1183. [Google Scholar] [CrossRef]
- Park, H.-J.; Choi, S.-H.; Choi, Y.J.; Park, Y.-B.; Kim, K.-M.; Yu, H.-S. A Prospective, Split-Mouth, Clinical Study of Orthodontic Titanium Miniscrews with Machined and Acid-Etched Surfaces. Angle Orthod. 2019, 89, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Stanford, N. Mini-Screws Success Rates Sufficient for Orthodontic Treatment: Question: What Are the Success Rates for Mini-Screws Use in Orthodontics? Evid.-Based Dent. 2011, 12, 19. [Google Scholar] [CrossRef]
- Tatli, U.; Alraawi, M.; Toroğlu, M.S. Effects of Size and Insertion Angle of Orthodontic Mini-Implants on Skeletal Anchorage. Am. J. Orthod. Dentofac. Orthop. 2019, 156, 220–228. [Google Scholar] [CrossRef] [PubMed]
- Wilmes, B.; Su, Y.-Y.; Drescher, D. Insertion Angle Impact on Primary Stability of Orthodontic Mini-Implants. Angle Orthod. 2008, 78, 1065–1070. [Google Scholar] [CrossRef] [PubMed]
- Jedliński, M.; Janiszewska-Olszowska, J.; Mazur, M.; Ottolenghi, L.; Grocholewicz, K.; Galluccio, G. Guided Insertion of Temporary Anchorage Device in Form of Orthodontic Titanium Miniscrews with Customized 3D Templates—A Systematic Review with Meta-Analysis of Clinical Studies. Coatings 2021, 11, 1488. [Google Scholar] [CrossRef]
- Sidambe, A. Biocompatibility of Advanced Manufactured Titanium Implants—A Review. Materials 2014, 7, 8168–8188. [Google Scholar] [CrossRef]
- Vikram, N.R. Ball Headed Mini Implant. JCDR 2017, 11, ZL02. [Google Scholar] [CrossRef]
- Montemezzi, P.; Ferrini, F.; Pantaleo, G.; Gherlone, E.; Capparè, P. Dental Implants with Different Neck Design: A Prospective Clinical Comparative Study with 2-Year Follow-Up. Materials 2020, 13, 1029. [Google Scholar] [CrossRef]
- Lucchese, A.; Matarese, G.; Manuelli, M.; Ciuffreda, C.; Bassani, L.; Isola, G.; Cordasco, G.; Gherlone, E. Reliability and efficacy of palifermin in prevention and management of oral mucositis in patients with acute lymphoblastic leukemia: A randomized, double-blind controlled clinical trial. Minerva Stomatol. 2016, 65, 43–50. [Google Scholar] [PubMed]
- Jedliński, M.; Mazur, M.; Grocholewicz, K.; Janiszewska-Olszowska, J. 3D Scanners in Orthodontics—Current Knowledge and Future Perspectives—A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 1121. [Google Scholar] [CrossRef] [PubMed]
- Manazza, F.; La Rocca, S.; Nagni, M.; Chirico, L.; Cattoni, F. A simplified digital workflow for the prosthetic finishing of implant rehabilitations: A case report. J. Biol. Regul. Homeost. Agents 2021, 35 (Suppl. 1), 87–97. [Google Scholar] [CrossRef] [PubMed]














{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author and Year | Type of Article | Study Groups | Method | Outcome Measured | Results |
|---|---|---|---|---|---|
| Kim et al. 2011 [25] | Prospective randomized animal study with in-vitro analysis | 24 tapered mini-implants of 5 mm length 24 cylindrical mini-implants of 7 mm length | Insertion and removal torque test in rabbit bone | Insertion and Removal torque values [N/cm] | Despite the fact that the tapered implants were shorter, they presented higher torque values than cylindrical at each time of the test. |
| Topcuoglu et al. 2013 [26] | Prospective randomized animal study with in-vitro analysis | 4 groups of 20 immediately loaded Ti6Al4V OMIs with interpitch distance of I—0.694 mmm, II—0.721 mm, III—0.693 mm and IV—0.702 mm inserted into rabbit fibula 4 groups of 20 unloaded Ti6Al4V OMIs with interpitch distance of I—0.694 mmm, II—0.721 mm, III—0.693 mm and IV—0.702 mm inserted into rabbit fibula | Removal torque test, SEM, and histomorphometric analyses in rabbit bone | Removal torque values [N/cm] | More frequent thread pitch had a positive effect on stability in every group studied. I—8.50 (2.41–10.05) 8.10 (4.94–9.35) II—6.92 (2.76–8.48) 4.63 (3.53–8.59) III—6.27 (3.99–9.87) 4.59 (2.26–5.57) IV—5.78 (4.17–7.95) 4.10 (2.59–5.53) |
| Chang et al. 2012 [27] | 3D finite element analysis | Four types of titanium grade V OMIs with different design parameters Screw type 1 had a 0.4-mm thread depth and a 7 tapered core at the 5 uppermost threads. Screw type 2 had a 0.4-mm thread depth and a 0 tapered core (cylindrical core). Screw type 3 had a 0.4-mm thread depth and a 7 tapered core at the 3 uppermost threads. Screw type 4 had a 0.32-mm thread depth and a 7 tapered core at the 3 uppermost threads. To evaluate the effect of thread depth on primary stability, the thread depths of the mini-implants were set at 0.16, 0.24, 0.32, 0.40, and 0.48 mm; | Assessment of possible mini-implant insertion torque stress and of displacement within the trabecular bone | Maximum insertion torque [Ncm], Pullout strength (N), Displacement before failure (mm), Stiffness (N/mm) | Mini-implants with greater thread depths, smaller tapers, and shorter taper lengths generated higher maximum stresses on the bone and thread elements. These mini-implants had larger relative displacements, as well. Pullout resistance increased as thread depth increased from 0.16 to 0.32 mm. However, the pullout resistance decreased as thread depth exceeded 0.32 mm. Pullout resistance also decreased as taper degrees and taper lengths decreased. High stresses were distributed on the uppermost threads at the neck of the mini-implants close to the bone margin in all conditions. Maximum insertion torque was observed in the first and the third OMIs. |
| Shen et al. 2014 [28] | 3D finite element analysis | 9 samples of titanium grade V mini-implants of thread heigh of 0.1 mm, 0.25 mm and 0.4 mm height and thread pitch of 0.5 mm, 1.20 mm, and 2 mm. | 3D finite element analysis of type III bone according to the Lekholm & Zarb classification (maxillary posterior region) | Maximum equivalent stresses | Increased thread height with a thread pitch of 1.20 mm was superior for the maxillary posterior region. Thread height proved more important for reducing maxillary stress and enhancing orthodontic mini-implant stability than the thread pitch. |
| Dastenaei et al. 2015 [29] | 3D finite element analysis | Titanium grade V OMI of diameter 1.6 mm, length 8 mm, thread pitch of 0.75 mm, thread depth of 0.25 mm and thread height of 0.331, tip angle 63° | Assessment of stress points within the implant inserted to trabecular bone | Maximum equivalent stresses | Stress concentration usually occured at the first thread of the implant. Stress decreased when screw pitch decreased from 1 to 0.5 mm; it was concentrated at the apex of the threads. The stress increased when the screw pitch became less than 0.45 mm and the stress distribution pattern was sparse. It seems appropriate to create a new dual miniscrew design that can provide ergonomic aims, with bigger thread pitch at the apex and smaller on threads neck. |
| Pouyafar et al. 2021 [30] | 3D finite element analysis | Series of test leading to optimal design of OMI | Assessment of possible mini-implant displacement within the trabecular bone | The lateral displacement measurement [µm] | The conical section improved the initial stability by creating compressive stress and additional friction in the surrounding bone. With increasing each millimeter and each degree in the conical section’s length and angle, the lateral displacement decreased by 2.3 and 1.8mm, respectively. The length and angle of the non-threaded part does not significantly control the lateral displacement. The higher the pitch of the mini-implant, the higher the lateral displacement (increases by 1.3– 2.2mm). It is necessary to consider the minimum possible value for the pitch according to the threads’ shape. |
| Kim et al. 2009 [31] | In-vitro study | Titanium grade V (10 of each group) 6 mm cylindrical, 8 mm cylindrical, 6 mm taper, 8 mm taper, 6 mm dual-thread and taper and 8 mm dual-thread and taper | Mechanical assessment of toque in artificial bone block from polyurethane foam block | Insertion torque (MIT), maximum removal torque (MRT), torque ratio (TR; MRT/MIT), insertion angular momentum (IAM), removal angular momentum (RAM) | The removal torque of the taper shape was lower than the removal of torque of the dual-thread shape. The dual-thread shape showed a low insertion torque and a gentle increase of insertion torque. The dual-thread shape also showed a higher removal torque on the broad range than the cylindrical and taper shapes. Long mini-implants need higher insertion torque than short mini-implants. Dual-thread shape may need improvement for reducing the long insertion time to decrease the stress to the surrounding tissue. |
| Gracco et al. 2012 [32] | In-vitro study | 35 OMIs (7 in each group) five different designs in thread shape (reverse buttress, buttress, 75° joint profile with flutes, trapezoidal and rounded) | Pull out strength form artificial bone block from polyurethane foam block | Pull out strength [N] | The thread shape influenced the resistance to pullout and, therefore, the primary stability of miniscrews. The buttress reverse thread shape (about 192.8 N) had consistently higher pullout strength values than the other designs. They fared worse in turn rounded, trapezoidal, 75° joint profile design and buttress profile) |
| Migliorati et al. 2012 [33] | In-vitro study | Three types of OMIs—one stainless steel, two titanium grade V of thread depth of 0.1735 mm, 0.1926 mm, 0.2757 mm and thread pitch of 0.9172 mm, 0.8255 mm and 0.1043 mm | Mechanical assessment of toque and screw mobility in artificial bone block with different densities from polyurethane foam | Peak load at the pull out tests [KN] | Increased thread shape factor (depth/pitch) is positively correlated with resistance to extraction. |
| Migliorati et al. 2013 [34] | In-vitro study | 30 titanium grade V OMIs in 3 groups: (10 in each group) of thread depth of 0.345, 0.216, 0.114mm and thread pitch of 0.826, 0.894, 0.574 | Mechanical assessment of toque and screw mobility in artificial bone block with different densities from polyurethane foam | Maximum insertion torque [Ncm], peak load at the pull out tests [KN] | There is a direct positive correlation between the increase in TSF (depth/pitch), the miniscrew pull-out strength and maximum insertion torque |
| Da Cunha et al. 2015 [35] | In-vitro study | 20 titanium grade V OMIs in 2 groups (10 in each group) G1 of thread pitch 30 × 0.6 mm and G2 45 × 0.8 mm | Mechanical assessment of torque and screw mobility in artificial bone block with different densities of polyurethane foam | Maximum insertion torque, removal torque, loss of torque [Ncm], implant stability [x] | The mini-implants with a shorter pitch distance and an insertion angle of 30° presented a better primary stability (torque) in artificial bone of a higher density. The mini-implants with a longer pitch distance and an insertion angle of 45° were found to be more stable in artificial bone of lower density, when performing evaluation with the Periotest. |
| Walter et al. 2013 [36] | In-vitro study | 240 self-drilling titanium Titanium Grade V OMIs of 12 types from 8 manufacturers The authors did not provide exact geometrical characteristics for every type od the screw—only correlations | Mechanical tests of pull-out strength, torsional fracture and insertion torque in artificial bone block of polyurethane foam, SEM inspection | Maximum insertion torque, Torsional Fracture [Ncm], pull-out strength [N] | Within the medium diameter OMI group, conical screws had higher insertion torque and torsional fracture values than cylindrical OMIs. Greater thread depth was related to higher pull-out strength values, although OMIs with similar pull-out strength values may have different insertion torque values. Thread depth and pitch had some impact on pull-out strenght. Torsional fracture depended mainly on the OMI inner and outer diameters. A thread depth to outer diameter ratio close to 40% increased torsion fracture risk. |
| Cha et al. 2015 [37] | In-vitro study | Titanium grade V OMIs with single-thread (thread pitch 0.7) and dual-thread design (lower part pitch 0.7 and 0.35 upper pitch part) | Insertion torque test and strain of bone-implant interface in artificial bone block from polyurethane foam block | Strain in [µstrains] and Insertion torque in [Nm] | The strain between the single-thread and dual-thread type miniscrews was similar at a cortical bone thickness of 1.0mm, but the discrepancy between miniscrew types widened to >10,000 μstrain with increasing cortical bone thicknesses. Self-drilling dual-thread miniscrews provide better initial mechanical stability, but their design may cause excessive strain that is over the physiological bone remodeling level (>1mm cortical bone) at the bone-implant interface of thick cortical bone layers. |
| Radwan et al. 2017 [38] | In-vitro study | 40 orthodontic miniscrews of same diameter and length and different taper designs randomly inserted into pilot holes | Mechanical assessment of pull-out test and periotest in 10 embalmed human maxillae | Pull-out strength estimation [N], implant stability [x] | Larger pitch width, flank, thread angle, apical face angle, and/or lead angle led to a higher primary stability, while a smaller thread shape factor (depth/width) improved primary stability. |
| Katić et al. 2017 [39] | In-vitro study | In each tested group there were 10 cylindrical self-drilling titanium grade 5 Ortho Easy® (FORESTADENT®, Pforzheim, Germany), 1.7 × 6 mm and 1.7 × 8 mm; Aarhus Anchorage System (MEDICON eG, Tuttlingen, Germany), 1.5 × 6 mm and 1.5 × 8 mm; and Jeil Dual Top™ Anchor System (Jeil Medical Corp., Seoul, Korea), 1.4 × 6 mm, 1.6 × 6 mm, 2.0 × 6 mm, 1.4 × 8 mm, 1.6 × 8 mm, and 2.0 × 8 mm | Maximum insertion torque test in rabbit bone | Maximum insertion torque [Nmm], Vertical Force [N], Torsion [Nmm] | The multiple linear regression model showed that significant predictors for higher maximum insertion torque were: a larger implant diameter, a higher insertion angle, and thicker cortical bone. Manufacturers should consider increasing the insertion angle of the implant to improve the implant design and achieve a better primary stability in cases where the operator cannot use a larger implant diameter. |
| Yashwant et al. 2017 [40] | In-vitro study | 50 OMIs (10 in each group) of five different designs in thread shape (reverse buttress, buttress, 75° joint profile with flutes, trapezoidal and trapezoidal fluted) | Pull out strength in artificial bone block from polyurethane foam block | Pull out strength [N] | Trapezoidal fluted mini implants showed twice as higher pull out strength then mini implants of other thread designs used in this study (about 61N), followed by reverse buttress (about 27N), (buttress, 75° joint profile with flutes) which showed similar values (about 26N). A trapezoidal design presented the lowest value (13N). |
| Sana et al. 2020 [41] | In-vitro study | 3 Titanium grade V OMIs— ORTHOImplant (3M Unitek, Monrovia, CA, USA): 1.8-mm diameter and 8-mm length, TOMAS (Dentaurum): 1.6-mm diameter and 8-mm length, VECTOR TAS (Ormco): 1.4-mm diameter and 8-mm length. | Pull out strength in artificial bone block from polyurethane foam block | Pull out strength [N] | Orthoimplant type with a larger diameter, smaller pitch and shorter taper length has a better primary stability, and lower stresses within the mini-implants and surrounding comparing to other groups tested. The favorable insertion angulation found was 90°, as it provides better primary stability and low stresses in the mini-implant and surrounding bone under orthodontic loading. |
| Watanbe et al. 2022 [42] | In-vitro study | Cylindrical vs. classic thread shape vs. novel thread shape Titanium grade V OMIs The authors did not provide exact geometrical characteristics for every type od the screw—only correlations | Mechanical assessment of toque, screw mobility and stiffness in artificial bone block from polyurethane foam | Values of maximum insertion torque, removal torque, torque ratio, [Ncm} screw mobility, [mm] static stiffness, dynamic stiffness [N/mm} and energy dissipation | Compared to miniscrews of a regular thread shape, the novel miniscrew of a different thread shape showed a higher torque ratio, a lower stiffness and screw mobility. These features seem important for the initial stability. |
| Budasbong et al. 2022 [43] | In-vitro study | 60 custom made titanium Grade V OMIs | Mechanical assessment of toque in 10 embalmed human maxillae | Maximum insertion torque [Nm], implant stability [x] | The maximum insertion torque and implant stability tests demonstrated a pitch-dependent decrease. The pitch had a strong negative correlation with maximum insertion torque and implant stability, while the cortical bone thickness had a strong positive correlation with these outcomes. |
| Redžepagić-Vražalica et al. 2022 [44] | In-vitro study | 40 Titanium grade V OMIs of which 20 | Mechanical assessment of toque in 40 pork ribs | Maximum insertion torque [Nm], Pull out strength [N] | The design of the mini-implant affects the insertion torque and pulling force. The bone quality at the implant insertion point is important for primary stability; thus, the increase in the cortical bone thickness significantly increases the pulling force. |
| Item | Type of Bias | Domain | Kim et al. 2011 [25] | Topcuoglu et al. 2013 [26] |
|---|---|---|---|---|
| 1 | Selection bias | Sequence generation | - | + |
| 2 | Selection bias | Baseline characteristics | + | + |
| 3 | Selection bias | Allocation concealment | ? | + |
| 4 | Performance bias | Random housing | ? | ? |
| 5 | Performance bias | Blinding | - | ? |
| 6 | Detection bias | Random outcome assessment | - | + |
| 7 | Detection bias | Blinding | - | ? |
| 8 | Attrition bias | Incomplete outcome data | + | + |
| 9 | Reporting bias | Selective outcome reporting | + | + |
| 10 | Other | Other sources of bias | ? | ? |
| Question | Chang et al. 2012 [27] | Shen et al. 2014 [28] | Dastenaei et al. 2015 [29] | Pouyafar et al. 2021 [30] | |
|---|---|---|---|---|---|
| Study Design and Presentation of Findings | |||||
| 1 | Was the hypothesis/aim/objective of the study clearly described? | Yes | Yes | Yes | Yes |
| 2 | Were all analyses planned at the outset of study? Answer NO for unplanned analysis/sub-analysis, unable to determine. | Yes | Yes | Yes | Yes |
| 3 | If data dredging (establish objectives, hypothesis and endpoint parameters without scientific reason) was used, was the spectrum of the data justified by any concepts? Answer YES if no data dredging, NO if unable to determine | Yes | Yes | Yes | Yes |
| 4 | Were ALL the outcome measures and parameters (including all data reduction methods or derived parameters) clearly described and defined in the Objectives or Methods section? Answer NO if they are only defined in results or discussion | Yes | Yes | No | No |
| 5 | Were the time points or period for ALL the outcome measures clearly described? Answer YES if not applicable | Yes | No | No | Yes |
| 6 | Were the main outcome measures appropriate to describe the targeted conditions? Answer NO if unable to determine | Yes | Yes | Yes | Yes |
| 7 | Were the key findings described clearly? | Yes | Yes | Yes | Yes |
| 8 | Were ALL the contour plots that were used for comparison presented with the same colour scale? | Yes | Yes | Yes | Yes |
| Subject Recruitment | |||||
| 9 | Were the characteristics of the model subject clearly described? | Yes—implants with features invented by researchers | Yes—specific implant available for purchase | Yes—specific implant available for purchase | Yes—specific implant available for purchase |
| 10 | Were the principal confounders of the model subject clearly described? (Age, sex, or body weight, and height) | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features |
| 11 | Was the model subject participated in the study representative of the population with the targeted clinical conditions or demographic features? (e.g., answer NO if simulating a pathology by modifying a normal subject model; or scaling an adult model to a child model) | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features |
| 12 | Were the targeted intervention or clinical condition clearly described? (with details in the severity, class, design/dimensions of implants, or details in surgical surgery) | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features | Yes—standard artificial bone features |
| Model Reconstruction and Configuration | |||||
| 13 | Was the model reconstruction modality for the body parts and ALL other items, such as implants, clearly described (e.g., MRI, 3D-scanning, CAD)? | Yes | Yes | Yes | Yes |
| 14 | Were ALL important technical specifications (e.g., resolution) for the reconstruction modality clearly described? | Yes | Yes | Yes | Yes |
| 15 | Was the posture or position of the body parts controlled during the acquisition process (e.g., MRI, CT) of the model reconstruction? | Yes/No | Yes | Yes | Yes |
| 16 | Were the model reconstruction methods for ALL components clearly described including those requiring additional procedures (e.g., connecting points for drawing ligaments from MRI)? | Yes/No | Yes | Yes | Yes |
| 17 | Were the orientation or relative position among the components of the model assembly (where appropriate) clearly described? Answer YES if not applicable | Yes | Yes | Yes | Yes |
| 18 | Was the type of mesh for ALL components, including the order of magnitude of the elements, clearly described? | No | No | No | Yes |
| 19 | Were the material properties for ALL components clearly described and justified? (e.g., with reference) | Yes | Yes | No | Yes |
| 20 | Were ALL the contact or interaction behaviours in the model clearly described and justified? | Yes/No | Yes/No | No | No |
| Boundary and Loading Condition (Simulation) | |||||
| 21 | Were the boundary and loading conditions clearly described? | Yes | Yes | Yes | Yes |
| 22 | Was the boundary and loading condition sufficiently simulating the common activity/scenario of the conditions? (e.g., if the research or inference is targeted to ambulation or daily activities, simulations of balanced standing or pre-set compressive load are insufficient) | Yes | Yes | Yes | Yes |
| 23 | Was the model driven by the boundary condition acquired from the same model subject? | Yes | Yes | Yes | Yes |
| 24 | Was loading condition on the scenario sufficiently and appropriately considered in the simulation? (e.g., muscle force, boundary force, inertia force) | Yes | Yes | Yes | Yes |
| 25 | Was the loading condition acquired from the same model subject? | Yes | Yes | Yes | Yes |
| 26 | Were the software (e.g., Abaqus, Ansys), type of analysis (e.g., quasi-static, dynamic), AND solver (e.g., standard, explicit) clearly described? (solver can be regarded as clearly described if it is obvious to the type of analysis) | Yes | Yes | Yes | Yes |
| Model Verification and Validation | |||||
| 27 | Were the methods of mesh convergence or other verification tests conducted and clearly described? | No | Yes | No | Yes |
| 28 | Were the model verification conducted and results presented clearly; and that the model was justified acceptable? | No | Yes | No | No—just mentioned about carrying them out |
| 29 | Were direct model validation (with experiment) conducted and described clearly? Answer YES if the authors had direct model validation previously with reference. | No | Yes | No | Yes |
| 30 | Were the model validation conducted and results presented clearly; and that the model was justified acceptable? | No | Yes | No | Yes |
| 31 | Were the model prediction or validation findings compared to relevant studies? | No | Yes | Yes | No |
| Model Assumption and Validity | |||||
| 32 | Were the model assumptions or simplifications on model reconstruction/configuration AND material properties discussed? | No | Yes | No | Yes |
| 33 | Were the model assumptions or simplifications on the boundary and loading conditions discussed? | Yes/No | Yes | Yes/No | Yes |
| 34 | Were the limitations of model validation discussed? (e.g., differences in case scenario; differences between validation metric and primary outcome) | Yes | No | No | No |
| 35 | Was the limitation on external validity, single-subject, and subject-specific design discussed? | No | Yes | No | Yes |
| 36 | Were there any attempts to improve or discuss internal validity (such as mesh convergence test), uncertainty and variability in the study? | No | Yes | Yes | Yes |
| 37 | Was there any discussion, highlights or content on the implications or translation potential of the research findings? Answer NO if there are only bold claims without making use of the result findings or key concepts | No | Yes | No | Yes |
| Sum: | 26 | 34.5 | 23.5 | 33 | |
| Criteria No. | Criteria | Kim et al. 2009 [31] | Gracco et al. 2012 [32] | Migliorati et al. 2012 [33] | Migliorati et al. 2013 [34] | Da Cunha et al. 2015 [35] | Walter et al. 2013 [36] | Cha et al. 2015 [37] |
|---|---|---|---|---|---|---|---|---|
| 1 | Clearly stated aims/objectives | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 2 | Detailed explanation of sample size calculation | 0 | 0 | 0 | 0 | 2 | 0 | 0 |
| 3 | Detailed explanation of sampling technique | 2 | 2 | 2 | 2 | 1 | 2 | 2 |
| 4 | Details of comparison group | 2 | 2 | 1 | 2 | 2 | 2 | 2 |
| 5 | Detailed explanation of methodology | 2 | 1 | 1 | 1 | 2 | 2 | 2 |
| 6 | Operator details | 0 | 0 | 1 | 2 | 2 | 2 | 2 |
| 7 | Randomization | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 | Method of measurement of outcome | 2 | 1 | 2 | 2 | 2 | 1 | 2 |
| 9 | Outcome assessor details | 1 | 2 | 2 | 2 | 1 | 1 | 1 |
| 10 | Blinding | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 11 | Statistical analysis | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 12 | Presentation of results | 2 | 2 | 1 | 2 | 1 | 1 | 2 |
| Criteria No. | Criteria | Radwan et al. 2017 [38] | Katić et al. 2017 [39] | Yashwant et al. 2017 [40] | Sana et al. 2020 [41] | Watanbe et al. 2021 [42] | Budasbong et al. 2022 [43] | Redžepagić-Vražalica et al. 2022 [44] |
| 1 | Clearly stated aims/objectives | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 2 | Detailed explanation of sample size calculation | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 3 | Detailed explanation of sampling technique | 1 | 2 | 1 | 2 | 2 | 2 | 2 |
| 4 | Details of comparison group | 1 | 2 | 1 | 2 | 2 | 2 | 2 |
| 5 | Detailed explanation of methodology | 1 | 2 | 1 | 1 | 2 | 2 | 1 |
| 6 | Operator details | 1 | 2 | 1 | 2 | 2 | 2 | 0 |
| 7 | Randomization | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 8 | Method of measurement of outcome | 2 | 2 | 1 | 2 | 1 | 1 | 2 |
| 9 | Outcome assessor details | 2 | 2 | 1 | 2 | 2 | 1 | 0 |
| 10 | Blinding | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 11 | Statistical analysis | 2 | 2 | 2 | 2 | 2 | 2 | 2 |
| 12 | Presentation of results | 1 | 2 | 1 | 2 *—additonally performed FEA does not bring any sigificant information to the study | 1 | 2 | 2 |
| Author | Number of Implants with Reduced Thread Pitch (Number of Threads-Observations) | Dimension of Thread Pitch [mm] | Pull-Out Strength [KN] | Number of Implants with Greater Thread pitch (Number of Threads-Observations) | Dimension of Thread Pitch [mm] | Pull-Out Strength [KN] |
|---|---|---|---|---|---|---|
| Migliorati et al. 2012 [33] | 1 (9) | 0.8255 ± 0.0282 | 0.34 ± 0.07 | 1 (6) | 0.9172 ± 0.0655 | 0.32 ± 0.05 |
| Migliorati et al. 2012 [33] | 1 (9) | 0.8255 ± 0.0282 | 0.34 ± 0.07 | 1 (10) | 1.043 ± 0.0306 | 0.43 ± 0.09 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.574 ± 0.006 | 0.34 ± 0.07 | 1 (7) | 0.826 ± 0.014 | 0.69 ± 0.12 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.574 ± 0.006 | 0.34 ± 0.07 | 1 (7) | 0.894 ± 0.006 | 0.58 ± 0.12 |
| Sana et al. 2020 [41] | 1 (12) | 0.507 ± 0.010 | 0.138 ± 0.025 | 1 (7) | 0.849 ± 0.024 | 0.142 ± 0.030 |
| Sana et al. 2020 [41] | 1 (12) | 0.507 ± 0.010 | 0.138 ± 0.025 | 1 (11) | 0.088 ± 0.049 | 0.181 ± 0.018 |
| Meta-analysis of in-vitro studies of peak load for pull-out strength—animal bone model | ||||||
| Radwan et al. 2017 [38] | 10 (80) | 0.70 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.83 ± 0.0 | 0.43699 ± 0.16779 |
| Radwan et al. 2017 [38] | 10 (80) | 0.70 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.71 ± 0.0 | 0.25713 ± 0.07902 |
| Radwan et al. 2017 [38] | 10 (80) | 0.70 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.89 ± 0.04 | 0.45062 ± 0.10022 |
| Redžepagić-Vražalica et al. 2022 [44] | 10 (80) | 0.8 ± 0.006 | 0.16160 ± 0.566 | 20 (140) | 0.890 ± 0.011 | 0.216.90 ± 0.568 |
| Redžepagić-Vražalica et al. 2022 [44] | 10 (80) | 0.799 ± 0.006 | 0.16440 ± 0.5247 | 20 (140) | 0.890 ± 0.011 | 0.216.90 ± 0.568 |
| Meta-analysis of in-vitro studies of peak load for pull-out strength—artificial bone model | ||||||
| Author | Number of implants with reduced thread depth (number of threads-observations) | Dimension of thread depth [mm] | Pull-out strength [KN] | Number of implants with greater thread depth (number of threads-observations) | Dimension of thread depth [mm] | Pull-out strength [KN |
| Migliorati et al. 2012 [33] | 1 (6) | 0.1735 ± 0.085 | 0.32 ± 0.05 | 1 (9) | 0.01926 ± 0.0172 | 0.34 ± 0.07 |
| Migliorati et al. 2012 [33] | 1 (6) | 0.1735 ± 0.085 | 0.32 ± 0.05 | 1 (10) | 0.02757 ± 0.0093 | 0.43 ± 0.09 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.114 ± 0.01 | 0.34 ± 0.07 | 1 (7) | 0.216 ± 0.013 | 0.58 ± 0.12 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.114 ± 0.01 | 0.34 ± 0.07 | 1 (7) | 0.345 ± 0.029 | 0.69 ± 0.12 |
| Sana et al. [41] | 1 (11) | 0.088 ± 0.019 | 0.181 ± 0.018 | 1 (12) | 0.097 ± 0.027 | 0.138 ± 0.025 |
| Sana et al. [41] | 1 (11) | 0.088 ± 0.019 | 0.181 ± 0.018 | 1 (7) | 0.217 ± 0.046 | 0.142 ± 0.030 |
| Meta-analysis of in-vitro studies of peak load for pull-out strength—animal bone model | ||||||
| Radwan et al. 2017 [38] | 10 (80) | 0.22 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.22 ± 0.01 | 0.45062 ± 0.10022 |
| Radwan et al. 2017 [38] | 10 (80) | 0.22 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.26 ± 0.0 | 0.43699 ± 0.16779 |
| Radwan et al. 2017 [38] | 10 (80) | 0.22 ± 0.0 | 0.19411 ± 0.7392 | 10 (70) | 0.33 ± 0.01 | 0.25713 ± 0.7902 |
| Redžepagić-Vražalica et al. 2022 [44] | 20 (140) | 0.238 ± 0.017 | 0.216.90 ± 0.568 | 10 (80) | 0.303 ± 0.005 | 0.16440 ± 0.5247 |
| Redžepagić-Vražalica et al. 2022 [44] | 20 (140) | 0.238 ± 0.017 | 0.216.90 ± 0.568 | 10 (80) | 0.272 ± 0.016 | 0.1616 ± 0.05663 |
| Meta-analysis of in-vitro studies of peak load for pull-out strength—artificial bone model | ||||||
| Author | Number of implants with reduced thread shape factor (number of threads -observations) | Value of thread shape factor | Pull-out strength [KN] | Number of implants with greater thread shape factor (number of threads -observations) | Value of thread shape factor | Pull-out strength [KN] |
| Migliorati et al. 2012 [33] | 1 (6) | 0.19 ± 0.01 | 0.32 ± 0.05 | 1 (9) | 0.23 ± 0.02 | 0.34 ± 0.07 |
| Migliorati et al. 2012 [33] | 1 (6) | 0.19 ± 0.01 | 0.32 ± 0.05 | 1 (10) | 0.27 ± 0.01 | 0.43 ± 0.09 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.198 ± 0.018 | 0.34 ± 0.07 | 1 (7) | 0.242 ± 0.015 | 0.58 ± 0.12 |
| Migliorati et al. 2013 [34] | 1 (11) | 0.198 ± 0.018 | 0.34 ± 0.07 | 1 (7) | 0.417 ± 0.038 | 0.69 ± 0.12 |
| Sana et al. [41] | 1 (12) | 0.191 ± 0.05277 | 0.138 ± 0.025 | 1 (11) | 0.20667 ± 0.04894 | 0.181 ± 0.018 |
| Sana et al. [41] | 1(12) | 0.191 ± 0.05277 | 0.138 ± 0.025 | 1 (7) | 0.25483 ± 0.04967 | 0.142 ± 0.030 |
| Meta-analysis of in-vitro studies of peak load for pull-out strength—animal bone model | ||||||
| Radwan et al. 2017 [38] | 10 (70) | 0.25 ± 0.02 | 0.45062 ± 0.10022 | 10 (80) | 0.31 ± 0.01 | 0.19411 ± 0.7392 |
| Radwan et al. 2017 [38] | 10 (70) | 0.25 ± 0.02 | 0.450.62 ± 0.10022 | 10 (70) | 0.32 ± 0.01 | 0.43699 ± 0.16779 |
| Radwan et al. 2017 [39] | 10 (70) | 0.25 ± 0.02 | 0.450.62 ± 0.10022 | 10 (70) | 0.47 ± 0.01 | 0.25713 ± 0.7902 |
| Redžepagić-Vražalica et al. 2022 [44] | 20 (140) | 0.270 ± 0.025 | 0.216.90 ± 0.568 | 10 (80) | 0.340 ± 0.021 | 0.1616 ± 0.05663 |
| Redžepagić-Vražalica et al. 2022 [44] | 20 (140) | 0.270 ± 0.025 | 0.216.90 ± 0.568 | 10 (80) | 0.380 ± 0.006 | 0.16440 ± 0.05247 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jedliński, M.; Janiszewska-Olszowska, J.; Mazur, M.; Grocholewicz, K.; Suárez Suquía, P.; Suárez Quintanilla, D. How Does Orthodontic Mini-Implant Thread Minidesign Influence the Stability?—Systematic Review with Meta-Analysis. J. Clin. Med. 2022, 11, 5304. https://doi.org/10.3390/jcm11185304
Jedliński M, Janiszewska-Olszowska J, Mazur M, Grocholewicz K, Suárez Suquía P, Suárez Quintanilla D. How Does Orthodontic Mini-Implant Thread Minidesign Influence the Stability?—Systematic Review with Meta-Analysis. Journal of Clinical Medicine. 2022; 11(18):5304. https://doi.org/10.3390/jcm11185304
Chicago/Turabian StyleJedliński, Maciej, Joanna Janiszewska-Olszowska, Marta Mazur, Katarzyna Grocholewicz, Pedro Suárez Suquía, and David Suárez Quintanilla. 2022. "How Does Orthodontic Mini-Implant Thread Minidesign Influence the Stability?—Systematic Review with Meta-Analysis" Journal of Clinical Medicine 11, no. 18: 5304. https://doi.org/10.3390/jcm11185304