
Middle Cerebral Artery M2 Thrombectomy: Safety and Technical Considerations in the German Stroke Registry (GSR)

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definition of Middle Cerebral Artery M2 Segment
2.3. Image Acquisition and Analysis
2.4. Treatment
2.5. Outcome and Safety
2.6. Statistical Analysis and Outcome Model Description
3. Results
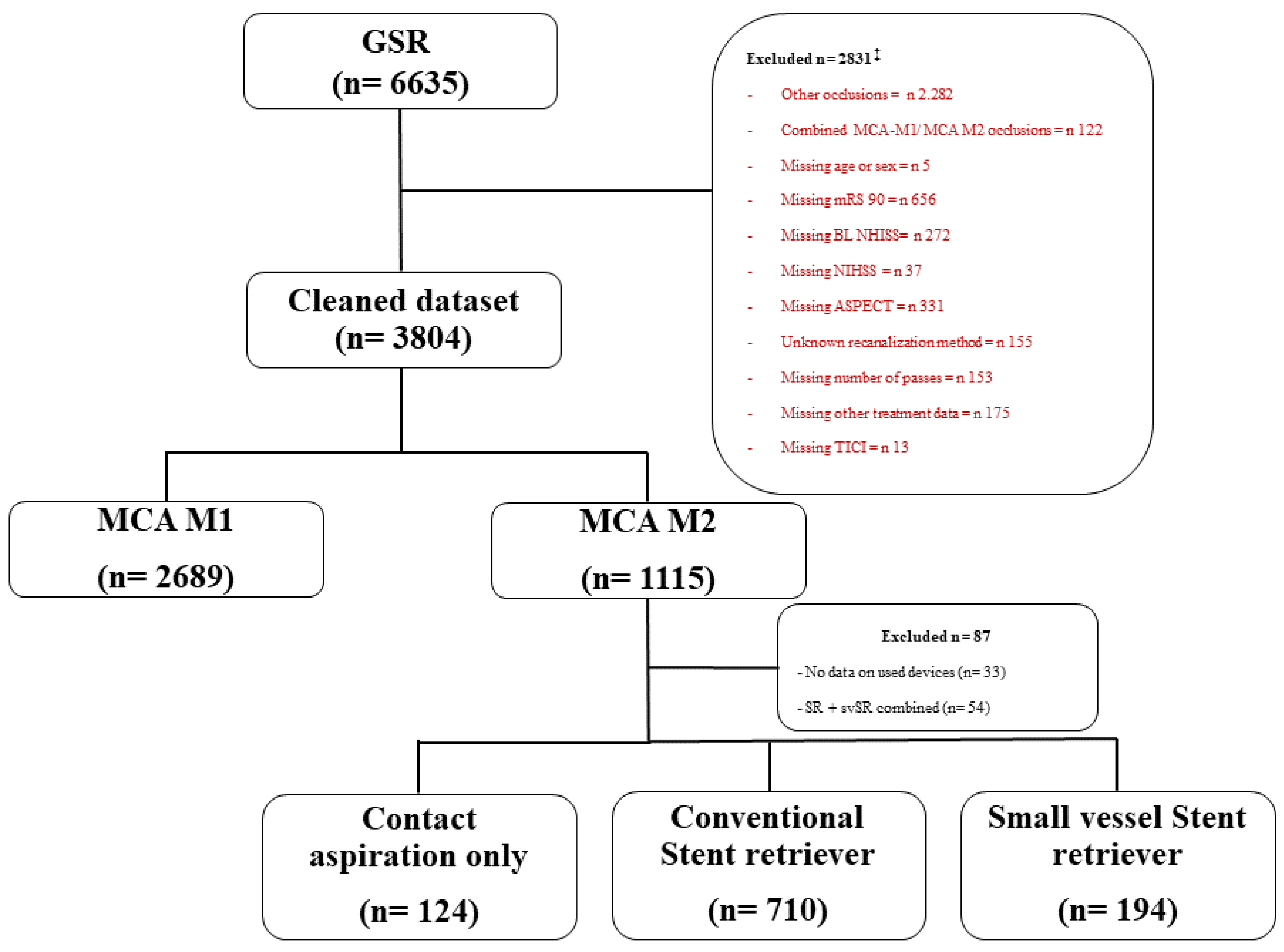
3.1. Patient Selection
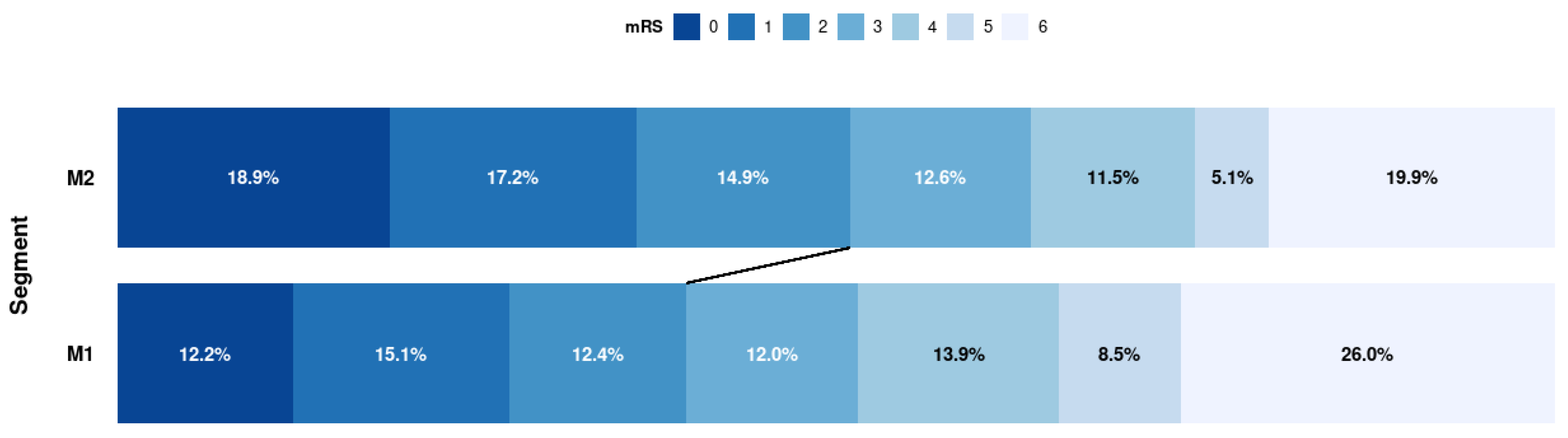
3.2. Baseline Characteristics, Clinical Outcome, and Safety M1 vs. M2
3.3. Subgroup Analysis of the M2 Cohort Regarding Treatment Strategies
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Name | Degree | Organization | Role | Contribution |
|---|---|---|---|---|
| Tobias Boeckh-Behrens | MD | Klinikum r.d.Isar, Munich, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Silke Wunderlich | MD | Klinikum r.d.Isar, Munich, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Arno Reich | MD | Uniklinik RWTH Aachen, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Anastasios Mpotsaris | MD | Uniklinik RWTH Aachen, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Martin Wiesmann | MD | Uniklinik RWTH Aachen, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Ulrike Ernemann | MD | Tübingen University Hospital, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Till-Karsten Hauser | MD | Tübingen University Hospital, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Christian H Nolte | MD | Charite Campus Benjamin Franklin | Site Investigator | German Stroke Registry—Steering Committee |
| Eberhard Siebert | MD | Charité – Campus Benjamin Franklin und Campus Charité Mitte, Berlin, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Sarah Zweynert | MD | Charité—Campus Virchow Klinikum, Berlin, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Georg Bohner | MD | Charité—Campus Virchow Klinikum, Berlin, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Alexander Ludolph | MD | Sana Klinikum Offenbach, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Karl-Heinz Henn | MD | Sana Klinikum Offenbach, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Waltraud Pfeilschifter | MD | Uniklinik Frankfurt/ Main, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Marlis Wagner | MD | Uniklinik Frankfurt/ Main, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Joachim Röther | MD | Asklepios Klinik Altona, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Bernd Eckert | MD | Asklepios Klinik Altona, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Jörg Berrouschot | MD | Klinikum Altenburger Land, Altenburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Albrecht Bormann | MD | Klinikum Altenburger Land, Altenburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Anna Alegiani | MD | University Medical Center Hamburg-Eppendorf, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Jens Fiehler | MD | University Medical Center Hamburg-Eppendorf, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Fabian Flottmann | MD | University Medical Center Hamburg-Eppendorf, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Christian Gerloff | MD | University Medical Center Hamburg-Eppendorf, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Götz Thomalla | MD | University Medical Center Hamburg-Eppendorf, Hamburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Elke Hattingen | MD | University Hospital Bonn, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Gabor Petzold | MD | University Hospital Bonn, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Sven Thonke | MD | Klinikum Hanau, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Christopher Bangard | MD | Klinikum Hanau, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Christoffer Kraemer | MD | Klinikum Lüneburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Martin Dichgans | MD | Ludwig Maximilian University of Munich, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Marios Psychogios | MD | Georg-August-Universität Göttingen, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Jan Liman | MD | Georg-August-Universität Göttingen, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Martina Petersen | MD | Klinikum Osnabrück, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Florian Stögbauer | MD | Klinikum Osnabrück, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Peter Kraft | MD | University Hospital Würzburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Mirko Pham | MD | University Hospital Würzburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Michael Braun | MD | Bezirkskrankenhaus Günzburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Gerhard F. Hamann | MD | Bezirkskrankenhaus Günzburg, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Andreas Kastrup | MD | Klinikum Bremen Mitte, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Christian Roth | MD | Klinikum Bremen Mitte, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Klaus Gröschel | MD | University Medical Center Mainz, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Timo Uphaus | MD | University Medical Center Mainz, Germany | Site Investigator | German Stroke Registry—Steering Committee |
| Volker Limmroth | MD | Kliniken Köln, Germany | Site Investigator | German Stroke Registry—Steering Committee |
References
- Goyal, M.; Menon, B.K.; van Zwam, W.H.; Dippel, D.W.J.; Mitchell, P.J.; Demchuk, A.M.; Dávalos, A.; Majoie, C.B.L.M.; van der Lugt, A.; de Miquel, M.A.; et al. Endovascular thrombectomy after large-vessel ischaemic stroke: A meta-analysis of individual patient data from five randomised trials. Lancet 2016, 387, 1723–1731. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients with Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef] [PubMed]
- Lima, F.O.; Furie, K.L.; Silva, G.S.; Lev, M.H.; Camargo, E.C.S.; Singhal, A.B.; Harris, G.J.; Halpern, E.F.; Koroshetz, W.J.; Smith, W.S.; et al. Prognosis of untreated strokes due to anterior circulation proximal intracranial arterial occlusions detected by use of computed tomography angiography. JAMA Neurol. 2014, 71, 151–157. [Google Scholar] [CrossRef] [PubMed]
- Rahme, R.; Abruzzo, T.A.; Martin, R.H.; Tomsick, T.A.; Ringer, A.J.; Furlan, A.J.; Carrozzella, J.A.; Khatri, P. Is intra-arterial thrombolysis beneficial for M2 occlusions? Subgroup analysis of the PROACT-II trial. Stroke 2013, 44, 240–242. [Google Scholar] [CrossRef] [Green Version]
- Campbell, B.C.V.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [Green Version]
- Menon, B.K.; Hill, M.D.; Davalos, A.; Roos, Y.B.W.E.M.; Campbell, B.C.V.; Dippel, D.W.J.; Guillemin, F.; Saver, J.L.; van der Lugt, A.; Demchuk, A.M.; et al. Efficacy of endovascular thrombectomy in patients with M2 segment middle cerebral artery occlusions: Meta-analysis of data from the HERMES Collaboration. J. Neurointerv. Surg. 2019, 11, 1065–1069. [Google Scholar] [CrossRef]
- Lemmens, R.; Hamilton, S.A.; Liebeskind, D.S.; Tomsick, T.A.; Demchuk, A.M.; Nogueira, R.G.; Marks, M.P.; Jahan, R.; Gralla, J.; Yoo, A.J.; et al. Effect of endovascular reperfusion in relation to site of arterial occlusion. Neurology 2016, 86, 762–770. [Google Scholar] [CrossRef] [Green Version]
- de Havenon, A.; Narata, A.P.; Amelot, A.; Saver, J.L.; Bozorgchami, H.; Mattle, H.P.; Ribo, M.; Andersson, T.; Zaidat, O.O. Benefit of endovascular thrombectomy for M2 middle cerebral artery occlusion in the ARISE II study. J. Neurointerv. Surg. 2021, 13, 779–783. [Google Scholar] [CrossRef] [PubMed]
- Jumaa, M.A.; Castonguay, A.C.; Salahuddin, H.; Jadhav, A.P.; Limaye, K.; Farooqui, M.; Zaidi, S.F.; Mueller-Kronast, N.; Liebeskind, D.S.; Zaidat, O.O.; et al. Middle Cerebral Artery M2 Thrombectomy in the STRATIS Registry. Stroke 2021, 52, 3490–3496. [Google Scholar] [CrossRef]
- Khunte, M.; Wu, X.; Koo, A.; Payabvash, S.; Matouk, C.; Heit, J.J.; Wintermark, M.; Gregory, A.W.; Sanelli, P.C.; Gandhi, D.; et al. Cost-effectiveness of thrombectomy in patients with minor stroke and large vessel occlusion: Effect of thrombus location on cost-effectiveness and outcomes. J. Neurointerv. Surg. 2022. [Google Scholar] [CrossRef]
- Saver, J.L.; Chapot, R.; Agid, R.; Hassan, A.; Jadhav, A.P.; Liebeskind, D.S.; Lobotesis, K.; Meila, D.; Meyer, L.; Raphaeli, G.; et al. Thrombectomy for Distal, Medium Vessel Occlusions: A Consensus Statement on Present Knowledge and Promising Directions. Stroke 2020, 51, 2872–2884. [Google Scholar] [CrossRef]
- Maïer, B.; Finitsis, S.; Bourcier, R.; Papanagiotou, P.; Richard, S.; Marnat, G.; Sibon, I.; Dargazanli, C.; Arquizan, C.; Blanc, R.; et al. First-line thrombectomy strategy for anterior large vessel occlusions: Results of the prospective ETIS egistry. J. Neurointerv. Surg. 2021, 14, 450–456. [Google Scholar] [CrossRef] [PubMed]
- Kurre, W.; Aguilar-Pérez, M.; Martinez-Moreno, R.; Schmid, E.; Bäzner, H.; Henkes, H. Stent Retriever Thrombectomy of Small Caliber Intracranial Vessels Using pREset LITE: Safety and Efficacy. Clin. Neuroradiol. 2017, 27, 351–360. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navia, P.; Schramm, P.; Fiehler, J. ADAPT technique in ischemic stroke treatment of M2 middle cerebral artery occlusions in comparison to M1 occlusions: Post hoc analysis of the PROMISE study. Interv. Neuroradiol. 2020, 26, 178–186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grieb, D.; Schlunz-Hendann, M.; Brinjikji, W.; Melber, K.; Greling, B.; Lanfermann, H.; Brassel, F.; Meila, D. Mechanical thrombectomy of M2 occlusions with distal access catheters using ADAPT. J. Neuroradiol. 2019, 46, 231–237. [Google Scholar] [CrossRef] [PubMed]
- Haussen, D.C.; Lima, A.; Nogueira, R.G. The Trevo XP 3×20 mm retriever (‘Baby Trevo’) for the treatment of distal intracranial occlusions. J. Neurointerv. Surg. 2016, 8, 295–299. [Google Scholar] [CrossRef] [PubMed]
- Alegiani, A.C.; Dorn, F.; Herzberg, M.; Wollenweber, F.A.; Kellert, L.; Siebert, E.; Nolte, C.H.; von Rennenberg, R.; Hattingen, E.; Petzold, G.C.; et al. Systematic evaluation of stroke thrombectomy in clinical practice: The German Stroke Registry Endovascular Treatment. Int. J. Stroke 2018, 4, 372–380. [Google Scholar] [CrossRef]
- Wollenweber, F.A.; Tiedt, S.; Alegiani, A.; Alber, B.; Bangard, C.; Berrouschot, J.; Bode, F.J.; Boeckh-Behrens, T.; Bohner, G.; Bormann, A.; et al. Functional Outcome Following Stroke Thrombectomy in Clinical Practice. Stroke 2019, 50, 2500–2506. [Google Scholar] [CrossRef]
- Goyal, M.; Menon, B.K.; Krings, T.; Patil, S.; Qazi, E.; McTaggart, R.A.; Almekhlafi, M.A.; Jehan, R.; Saver, J.; Jayaraman, M.V. What constitutes the M1 segment of the middle cerebral artery? J. Neurointerv. Surg. 2016, 8, 1273–1277. [Google Scholar] [CrossRef]
- Hill, M.D.; Demchuk, A.M.; Goyal, M.; Jovin, T.G.; Foster, L.D.; Tomsick, T.A.; von Kummer, R.; Yeatts, S.D.; Palesch, Y.Y.; Broderick, J.P. Alberta Stroke Program early computed tomography score to select patients for endovascular treatment: Interventional Management of Stroke (IMS)-III Trial. Stroke 2014, 45, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.-F.M.; et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar] [CrossRef] [Green Version]
- Kim, C.H.; Kim, S.-E.; Jeon, J.P. Meta-Analysis of Endovascular Treatment for Acute M2 Occlusion. J. Korean Neurosurg. Soc. 2019, 62, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saber, H.; Narayanan, S.; Palla, M.; Saver, J.L.; Nogueira, R.G.; Yoo, A.J.; Sheth, S.A. Mechanical thrombectomy for acute ischemic stroke with occlusion of the M2 segment of the middle cerebral artery: A meta-analysis. J. Neurointerv. Surg. 2018, 10, 620–624. [Google Scholar] [CrossRef]
- Muszynski, P.; Anadani, M.; Richard, S.; Marnat, G.; Bourcier, R.; Sibon, I.; Dargazanli, C.; Arquizan, C.; Maïer, B.; Blanc, R.; et al. Endovascular reperfusion of M2 occlusions in acute ischemic stroke reduced disability and mortality: ETIS Registry results. J. Neurointerv. Surg. 2021, 14, 444–449. [Google Scholar] [CrossRef] [PubMed]
- Nakano, T.; Shigeta, K.; Ota, T.; Amano, T.; Ueda, M.; Matsumaru, Y.; Shiokawa, Y.; Hirano, T. Efficacy and Safety of Mechanical Thrombectomy for Occlusion of the Second Segment of the Middle Cerebral Artery: Retrospective Analysis of the Tama-REgistry of Acute endovascular Thrombectomy (TREAT). Clin. Neuroradiol. 2020, 30, 481–487. [Google Scholar] [CrossRef]
- Ospel, J.M.; Goyal, M. A review of endovascular treatment for medium vessel occlusion stroke. J. Neurointerv. Surg. 2021, 13, 623–630. [Google Scholar] [CrossRef] [PubMed]
- Alexander, C.; Caras, A.; Miller, W.K.; Tahir, R.; Mansour, T.R.; Medhkour, A.; Marin, H. M2 segment thrombectomy is not associated with increased complication risk compared to M1 segment: A meta-analysis of recent literature. J. Stroke Cerebrovasc. Dis. 2020, 29, 105018. [Google Scholar] [CrossRef] [PubMed]
- Raychev, R.; Saber, H.; Saver, J.L.; Hinman, J.D.; Brown, S.; Vinuela, F.; Duckwiler, G.; Jahan, R.; Tateshima, S.; Szeder, V.; et al. Impact of eloquent motor cortex-tissue reperfusion beyond the traditional thrombolysis in cerebral infarction (TICI) scoring after thrombectomy. J. Neurointerv. Surg. 2021, 13, 990–994. [Google Scholar] [CrossRef] [PubMed]
- Kurmann, C.C.; Mujanovic, A.; Piechowiak, E.I.; Dobrocky, T.; Zibold, F.; Beyeler, M.; Vynckier, J.; Seiffge, D.; Meinel, T.R.; Mordasini, P.; et al. Heterogeneity of the Relative Benefits of TICI 2c/3 over TICI 2b50/2b67: Are there Patients who are less Likely to Benefit? Clin. Neuroradiol. 2022; Online ahead of print. [Google Scholar] [CrossRef]
- de Havenon, A.; Mlynash, M.; Kim-Tenser, M.A.; Lansberg, M.G.; Leslie-Mazwi, T.; Christensen, S.; McTaggart, R.A.; Alexander, M.; Albers, G.; Broderick, J.; et al. Results from DEFUSE 3 -Good Collaterals Are Associated with Reduced Ischemic Core Growth but Not Neurologic Outcome. Stroke 2019, 50, 632–638. [Google Scholar] [CrossRef]
- Compagne, K.C.J.; van der Sluijs, P.M.; van den Wijngaard, I.R.; Roozenbeek, B.; Mulder, M.J.H.L.; van Zwam, W.H.; Emmer, B.J.; Majoie, C.B.L.M.; Yoo, A.J.; Lycklama à Nijeholt, G.J.; et al. Endovascular Treatment: The Role of Dominant Caliber M2 Segment Occlusion in Ischemic Stroke. Stroke 2019, 50, 419–427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kappelhof, M.; Ospel, J.; Kashani, N.; Cimflova, P.; Singh, N.; Almekhlafi, M.A.; Menon, B.K.; Fiehler, J.; Chen, M.; Sakai, N.; et al. Influence of intravenous alteplase on endovascular treatment decision-making in acute ischemic stroke due to primary medium-vessel occlusion: A case-based survey study. J. Neurointerv. Surg. 2021, 14, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Cimflova, P.; Kappelhof, M.; Singh, N.; Kashani, N.; Ospel, J.M.; McDonough, R.; Demchuk, A.M.; Menon, B.K.; Sakai, N.; Chen, M.; et al. Factors influencing thrombectomy decision making for primary medium vessel occlusion stroke. J. Neurointerv. Surg. 2021, 14, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Sarraj, A.; Sangha, N.; Hussain, M.S.; Wisco, D.; Vora, N.; Elijovich, L.; Goyal, N.; Abraham, M.; Mittal, M.; Feng, L.; et al. Endovascular Therapy for Acute Ischemic Stroke with Occlusion of the Middle Cerebral Artery M2 Segment. JAMA Neurol. 2016, 73, 1291–1296. [Google Scholar] [CrossRef] [PubMed]
- Boyanpally, A.; Nardi, M.; Patel, V.G.; Jacob, M. Isolated M2 Segment Occlusions: Should These Patients Receive Endovascular Therapy? (P4.209). Neurology 2018, 90. [Google Scholar]
- Gory, B. Contact Aspiration Versus Stent Retriever in Patients with Acute Ischemic Stroke with M2 Occlusion in the ASTER Randomized Trial (Contact Aspiration Versus Stent Retriever for Successful Revascularization). Available online: https://www.ahajournals.org/doi/10.1161/STROKEAHA.117.019598?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed (accessed on 12 June 2022).


| MCA-M1 (n = 2689) | MCA-M2 (n = 1115) | p Value | |
|---|---|---|---|
| Age—years, median (IQR) | 76.00 [65.00–82.00] | 77.00 [66.00–83.00] | 0.41 |
| Sex—female, n (%) | 1449 (53.9) | 550 (49.5) | 0.14 |
| Clinical characteristics at admission | |||
| Baseline NIHSS at ADM, median (IQR) | 15.00 [10.00–18.00] | 11.00 [6.25–16.00] | <0.001 |
| Time intervals (minutes) | |||
| Symptom onset to groin | 195.00 [140.00–265.50] | 190.00 [139.00–270.00] | 0.99 |
| Last seen well to groin | 490.00 [301.00–814.50] | 520.50 [307.25–811.75] | 0.89 |
| IVT treatment, n (%) | 1335 (50.0) | 609 (54.8) | 0.80 |
| ASPECTS, median (IQR) | 9.00 [7.00–10.00] | 9.00 [8.00–10.00]s | <0.001 |
| Type of anesthesia | 0.15 | ||
| Conscious sedation, n (%) | 792 (30.9) | 283 (26.2) | |
| General anesthesia, n (%) | 1685 (65.7) | 762 (70.6) | |
| Conversion, n (%) | 89 (3.5) | 35 (3.2) |
| MCA-M1 (n = 2689) | MCA-M2 (n = 1115) | p Value | |
|---|---|---|---|
| Outcome | |||
| Good functional outcome (mRS 0–2), n (%) | 1348 (38.9) | 607 (46.5) | <0.001 |
| Mortality (mRS 6), n (%) | 590 (26.9) | 218 (22.9) | 0.23 |
| Improvement of clinical symptomatic, n (%) | 1359 (62.5) | 600 (61.4) | 0.57 |
| mTICI, n (%) | 0.30 | ||
| 0 | 183 (6.9) | 90 (8.2) | |
| 1 | 28 (1.0) | 20 (1.8) | |
| 2a | 136 (5.1) | 75 (6.8) | |
| 2b | 889 (33.3) | 393 (35.6) | |
| 3 | 1431 (53.7) | 525 (47.6) | |
| Procedural results | <0.001 | ||
| Aspiration catheter only, n (%) | 401 (14.9) | 124 (11.1) | |
| Conventional stent retriever ± aspiration, n (%) | 2062 (76.7) | 710 (63.7) | |
| Small vessel stent retriever ± aspiration, n (%) | 80 (3.0) | 194 (17.4) | |
| Small vessel+ conventional stent retriever ± aspiration, n = (%) | 39 (1.5) | 15 (1.3) | |
| Number of passages, median (IQR) | 2.00 [2.00–8.00] | 2.00 [2.00–7.00] | 0.10 |
| First pass mTICI 2b/3 | 34 (1.3) | 29 (2.7) | 0.50 |
| Treatment completed, n (%) | 2505 (94.2) | 1010 (91.6) | 0.40 |
| Treatment extracranial ICA (NASCET > 70%), n (%) | 326 (12.1) | 96 (8.6) | 0.20 |
| Treatment extracranial ICA with stent, n (%) | 237 (8.8) | 74 (6.6) | 0.30 |
| Safety outcome | |||
| Periprocedural complications, n (%) | 385 (14.4) | 202 (18.1) | 0.63 |
| Allergic | 4 (0.1) | 2 (0.2) | |
| Reanimation | 6 (0.2) | 1 (0.1) | |
| Periprocedural rethrombosis | 12 (0.4) | 4 (0.4) | |
| SAH, n (%) | 43 (1.6) | 29 (2.6) | 0.53 |
| Vasospasm, n (%) | 96 (3.6) | 49 (4.4) | 0.26 |
| Recurrent stroke 24, n (%) | 91 (3.4) | 44 (3.9) | 0.44 |
| ICH 24 h, n (%) | 298 (11.1) | 124 (11.1) | 1.0 |
| Hemorrhagic transformation 24 h, n (%) | 91 (3.4) | 44 (3.9) | 0.45 |
| Aspiration Only (CA) (n = 124) | Conventional Stent Retriever ± Aspiration (n = 710) | Small Vessel Stent Retriever ± Aspiration (n = 194) | p Value | |
|---|---|---|---|---|
| Age—years, median (IQR) | 76.00 [63.75–84.00] | 77.00 [67.00–83.00] | 77.00 [68.00–82.00] | 0.75 |
| Sex—female, n (%) | 54 (43.5) | 361 (51.1) | 95 (49.0) | 0.29 |
| Clinical characteristics at admission | ||||
| Baseline NIHSS at ADM, median (IQR) | 11.00 [7.00–15.25] | 11.00 [6.00–16.00] | 10.00 [6.00–16.00] | 0.83 |
| Time intervals (minutes) | ||||
| Symptom onset to groin | 159.00 [135.00–217.25] | 195.00 [139.50–276.50] | 186.50 [134.00–267.00] | 0.14 |
| Last seen well to groin | 446.00 [370.00–761.50] | 538.50 [304.75–837.00] | 525.00 [275.00–853.50] | 0.97 |
| IVT treatment, n (%) | 80 (64.5) | 361 (51.0) | 114 (59.1) | 0.60 |
| ASPECTS, median (IQR) | 9.00 [8.00–10.00] | 9.00 [8.00–10.00] | 9.00 [8.00–10.00] | 0.34 |
| Aspiration Only (CA) (n = 124) | Conventional Stent Retriever ± Aspiration (n = 710) | Small Vessel Stent Retriever ± Aspiration (n = 194) | p Value | |
|---|---|---|---|---|
| Outcome | ||||
| Good functional outcome (mRS 0-2), n (%) | 71 (50.5) | 385 (45.7) | 115 (51.8) | 0.65 |
| Mortality (mRS 6), n (%) | 23 (21.5) | 140 (23.4) | 34 (20.7) | 0.74 |
| Improvement of clinical symptomatic, n (%) | 75 (71.4) | 369 (60.5) | 110 (60.8) | 0.98 |
| mTICI, n (%) | ||||
| 0 | 12 (9.8) | 31 (4.4) | 22 (11.4) | 1.0 |
| 1 | 5 (4.1) | 8 (1.1) | 3 (1.6) | 0.52 |
| 2a | 10 (8.2) | 44 (6.2) | 10 (5.2) | 0.56 |
| 2b | 49 (40.2) | 241 (34.2) | 77 (39.9) | 0.21 |
| 3 | 46 (37.7) | 380 (54.0) | 81 (42.0) | <0.001 |
| Procedural results | ||||
| Number of passages, median (IQR) | 2.00 [2.00–2.00] | 7.00 [2.00–8.00] | 2.00 [2.00. 7.00] | <0.001 |
| First pass mTICI 2b/3 | 5 (4.2) | 1 (0.1) | 0 (0.0) | <0.001 |
| Treatment completed, n (%) | 116 (93.5) | 683 (97.2) | 182 (95.3) | 0.96 |
| Treatment extracranial ICA (NASCET > 70%), n (%) | 9 (7.3) | 61 (8.6) | 16 (8.2) | 0.88 |
| Treatment extracranial ICA with stent, n (%) | 8 (6.5) | 52 (7.3) | 10 (5.2) | 0.56 |
| Safety outcome | ||||
| Periprocedural complications, n (%) | 18 (14.5) | 128 (18.1) | 42 (21.6) | 0.20 |
| SAH, n (%) | 1 (0.8) | 20 (2.8) | 8 (4.1) | 0.22 |
| Vasospasm, n (%) | 4 (3.2) | 39 (5.5) | 5 (2.6) | 0.17 |
| Recurrent stroke 24 h, n (%) | 1 (0.8) | 3 (0.4) | 0 (0.0) | 0.62 |
| ICH 24 h, n (%) | 9 (7.3) | 79 (11.1) | 22 (11.3) | 0.42 |
| Hemorrhagic transformation 24 h, n (%) | 2 (1.6) | 10 (1.4) | 1 (0.5) | 0.57 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Herzberg, M.; Dorn, F.; Trumm, C.; Kellert, L.; Tiedt, S.; Feil, K.; Küpper, C.; Wollenweber, F.; Liebig, T.; Zimmermann, H. Middle Cerebral Artery M2 Thrombectomy: Safety and Technical Considerations in the German Stroke Registry (GSR). J. Clin. Med. 2022, 11, 4619. https://doi.org/10.3390/jcm11154619
Herzberg M, Dorn F, Trumm C, Kellert L, Tiedt S, Feil K, Küpper C, Wollenweber F, Liebig T, Zimmermann H. Middle Cerebral Artery M2 Thrombectomy: Safety and Technical Considerations in the German Stroke Registry (GSR). Journal of Clinical Medicine. 2022; 11(15):4619. https://doi.org/10.3390/jcm11154619
Chicago/Turabian StyleHerzberg, Moriz, Franziska Dorn, Christoph Trumm, Lars Kellert, Steffen Tiedt, Katharina Feil, Clemens Küpper, Frank Wollenweber, Thomas Liebig, and Hanna Zimmermann. 2022. "Middle Cerebral Artery M2 Thrombectomy: Safety and Technical Considerations in the German Stroke Registry (GSR)" Journal of Clinical Medicine 11, no. 15: 4619. https://doi.org/10.3390/jcm11154619