
Evaluation of Cough Medication Use Patterns in Ambulatory Care Settings in the United States: 2003–2018

 ,
,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Study Cohort
2.3. Medications
2.4. Patient, Visit, and Practice Characteristics
2.5. Statistical Analysis
2.6. Secondary and Sensitivity Analyses
3. Results
3.1. NAMCS Analysis: 2003–2018
3.1.1. Patient, Visit, and Practice Characteristics
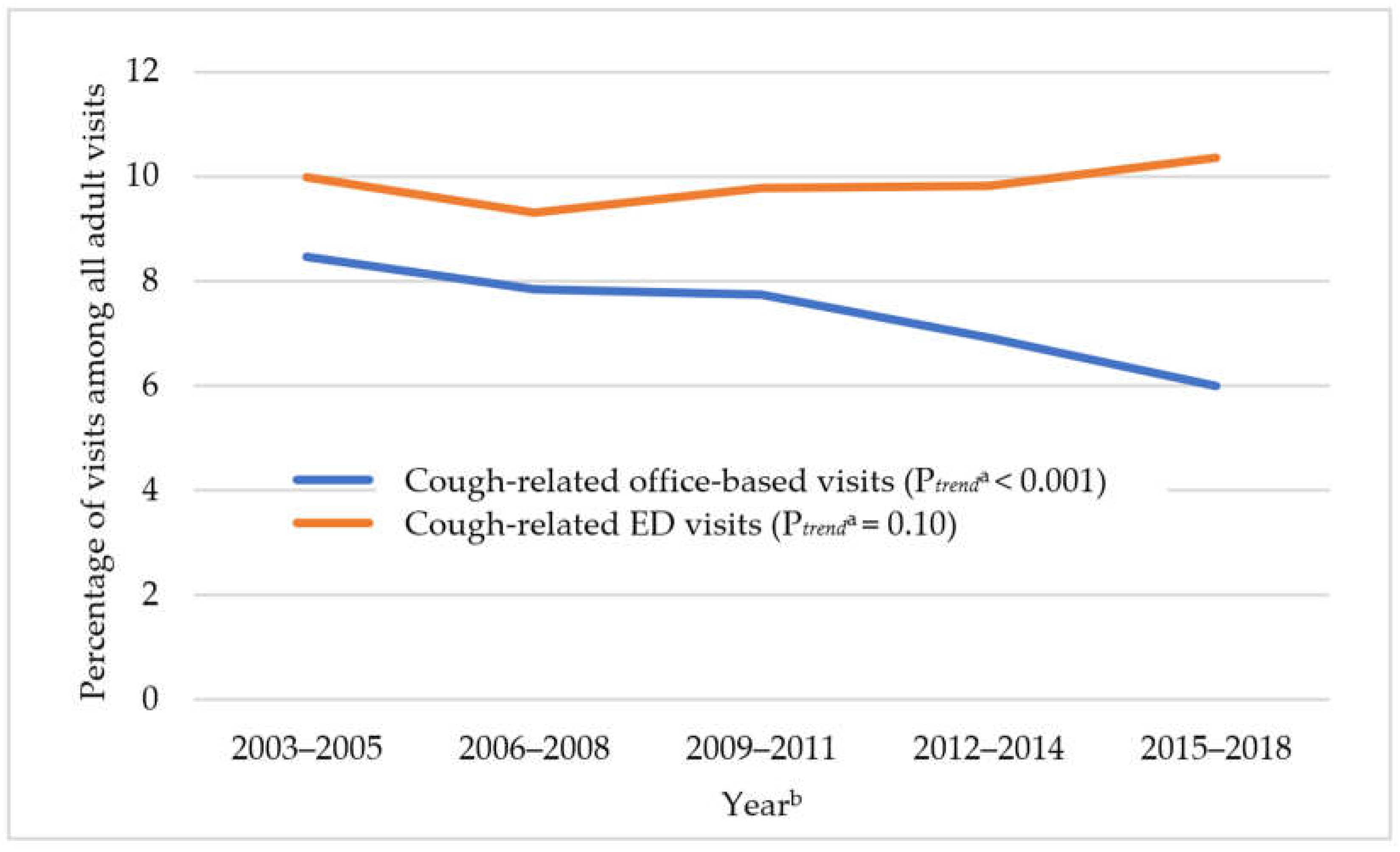
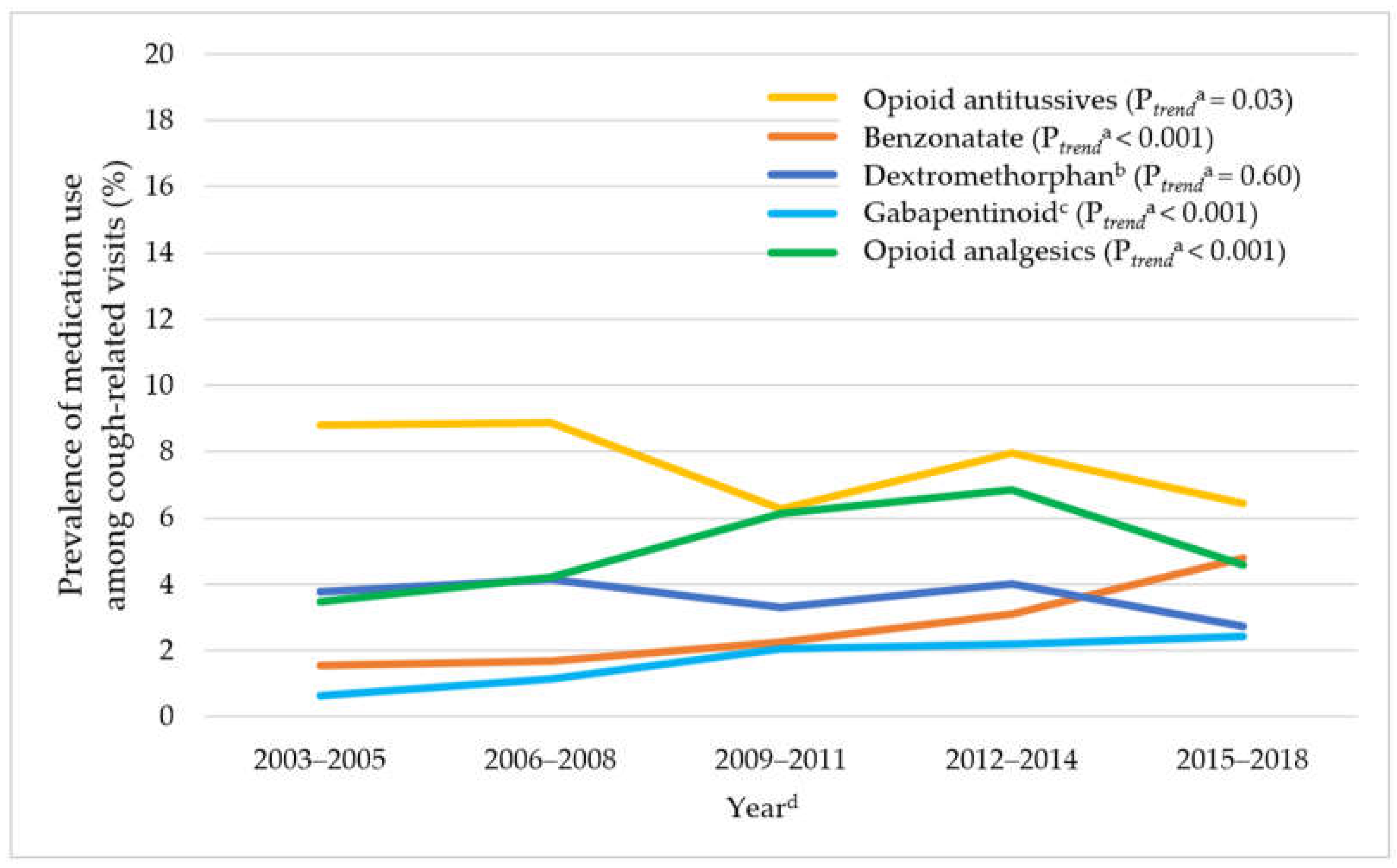
3.1.2. Trends in Cough-Related Office-Based Visits and Medication Use
3.2. NHAMCS Analysis: 2003–2018
3.2.1. Patient, Visit, and Practice Characteristics
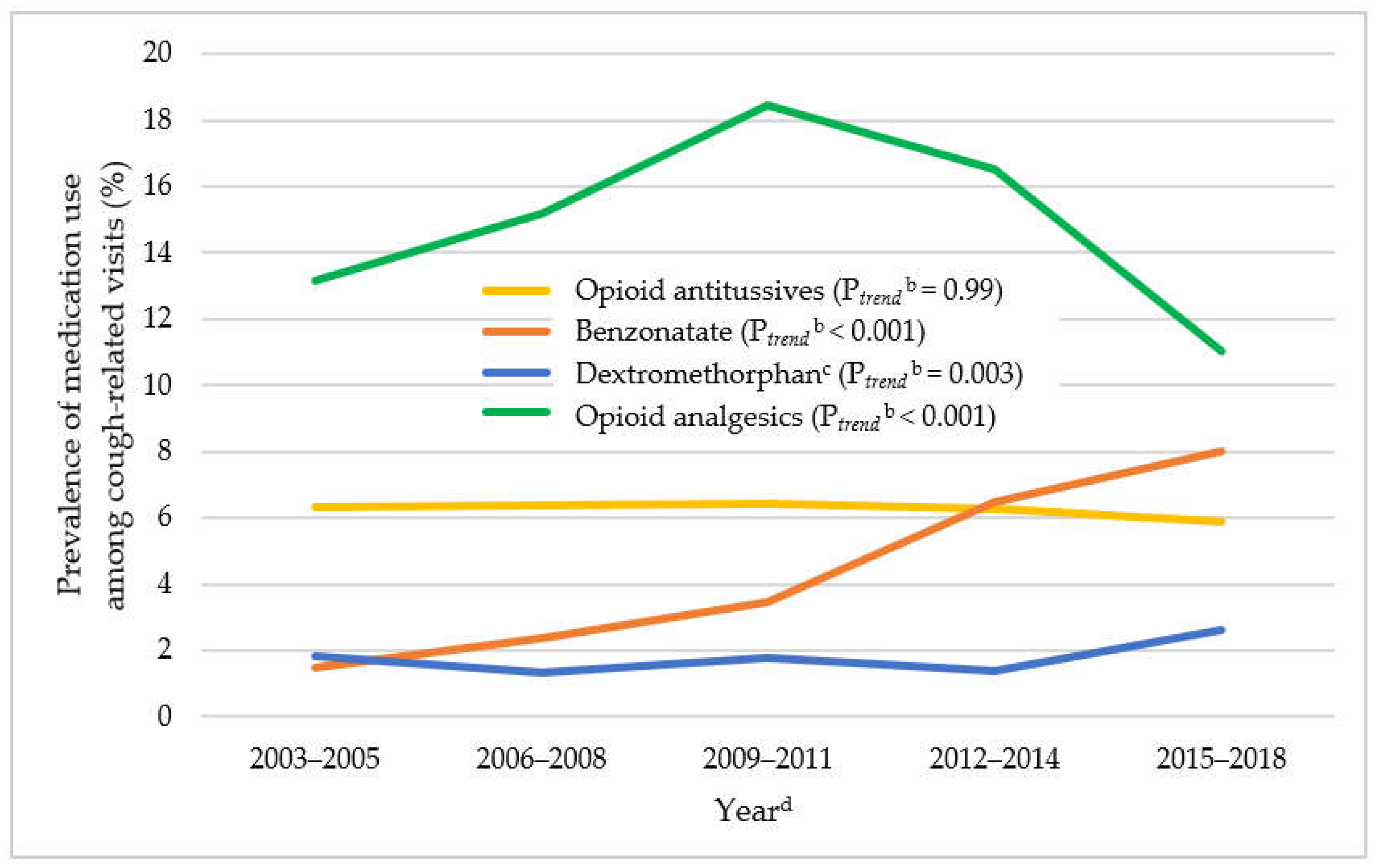
3.2.2. Trends in Cough-Related ED Visits and Medication Use
3.3. Secondary and Sensitivity Analyses
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Center for Disease Control and Prevention. National Center for Health Statistics. National Ambulatory Medical Care Survey: 2018 National Summary Tables. Available online: https://www.cdc.gov/nchs/data/ahcd/namcs_summary/2018-namcs-web-tables-508.pdf (accessed on 22 June 2022).
- Center for Disease Control and Prevention. National Center for Health Statistics. National Hospital Ambulatory Medical Care Survey: 2018 Emergency Department Summary Tables. Available online: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2018-ed-web-tables-508.pdf (accessed on 22 June 2022).
- Song, W.J.; Chang, Y.S.; Faruqi, S.; Kim, J.Y.; Kang, M.G.; Kim, S.; Jo, E.J.; Kim, M.H.; Plevkova, J.; Park, H.W.; et al. The global epidemiology of chronic cough in adults: A systematic review and meta-analysis. Eur. Respir. J. 2015, 45, 1479–1481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, R.S.; Baumann, M.H.; Bolser, D.C.; Boulet, L.P.; Braman, S.S.; Brightling, C.E.; Brown, K.K.; Canning, B.J.; Chang, A.B.; Dicpinigaitis, P.V.; et al. Diagnosis and management of cough executive summary: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 1S–23S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Irwin, R.S.; French, C.L.; Chang, A.B.; Altman, K.W.; Panel, C.E.C. Classification of Cough as a Symptom in Adults and Management Algorithms: CHEST Guideline and Expert Panel Report. Chest 2018, 153, 196–209. [Google Scholar] [CrossRef] [Green Version]
- Gibson, P.; Wang, G.; McGarvey, L.; Vertigan, A.E.; Altman, K.W.; Birring, S.S.; Panel, C.E.C. Treatment of Unexplained Chronic Cough: CHEST Guideline and Expert Panel Report. Chest 2016, 149, 27–44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pratter, M.R. Overview of common causes of chronic cough: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 59S–62S. [Google Scholar] [CrossRef] [PubMed]
- McGarvey, L.; Gibson, P.G. What Is Chronic Cough? Terminology. J. Allergy Clin. Immunol. Pract. 2019, 7, 1711–1714. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weinberger, M.; Hendeles, L. Nonprescription medications for respiratory symptoms: Facts and marketing fictions. Allergy Asthma Proc. 2018, 39, 169–176. [Google Scholar] [CrossRef] [PubMed]
- The Medical Letter. Drugs for cough. Med. Lett. Drugs Ther. 2018, 60, 206–208. [Google Scholar]
- Eddy, N.B. Codeine and its alternates for pain and cough relief. Ann. Intern. Med. 1969, 71, 1209–1212. [Google Scholar] [CrossRef] [PubMed]
- Molassiotis, A.; Smith, J.A.; Mazzone, P.; Blackhall, F.; Irwin, R.S.; Panel, C.E.C. Symptomatic Treatment of Cough Among Adult Patients with Lung Cancer: CHEST Guideline and Expert Panel Report. Chest 2017, 151, 861–874. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Eccles, R.; Morris, S.; Jawad, M. Lack of effect of codeine in the treatment of cough associated with acute upper respiratory tract infection. J. Clin. Pharm. Ther. 1992, 17, 175–180. [Google Scholar] [CrossRef]
- Freestone, C.; Eccles, R. Assessment of the antitussive efficacy of codeine in cough associated with common cold. J. Pharm. Pharmacol. 1997, 49, 1045–1049. [Google Scholar] [CrossRef] [PubMed]
- Eccles, R. Codeine, cough and upper respiratory infection. Pulm. Pharmacol. 1996, 9, 293–297. [Google Scholar] [CrossRef] [PubMed]
- Morice, A.H. The cough hypersensitivity syndrome: A novel paradigm for understanding cough. Lung 2010, 188 (Suppl. S1), 87–90. [Google Scholar] [CrossRef] [PubMed]
- Ryan, N.M.; Birring, S.S.; Gibson, P.G. Gabapentin for refractory chronic cough: A randomised, double-blind, placebo-controlled trial. Lancet 2012, 380, 1583–1589. [Google Scholar] [CrossRef]
- Vertigan, A.E.; Kapela, S.L.; Ryan, N.M.; Birring, S.S.; McElduff, P.; Gibson, P.G. Pregabalin and Speech Pathology Combination Therapy for Refractory Chronic Cough: A Randomized Controlled Trial. Chest 2016, 149, 639–648. [Google Scholar] [CrossRef]
- Radley, D.C.; Finkelstein, S.N.; Stafford, R.S. Off-label prescribing among office-based physicians. Arch. Intern. Med. 2006, 166, 1021–1026. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.V.; Lofwall, M.R.; Havens, J.R. Abuse and diversion of gabapentin among nonmedical prescription opioid users in Appalachian Kentucky. Am. J. Psychiatry 2015, 172, 487–488. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smith, R.V.; Havens, J.R.; Walsh, S.L. Gabapentin misuse, abuse and diversion: A systematic review. Addiction 2016, 111, 1160–1174. [Google Scholar] [CrossRef] [PubMed]
- Buttram, M.E.; Kurtz, S.P.; Dart, R.C.; Margolin, Z.R. Law enforcement-derived data on gabapentin diversion and misuse, 2002-2015: Diversion rates and qualitative research findings. Pharmacoepidemiol. Drug Saf. 2017, 26, 1083–1086. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, U.; Scherbaum, N. How addictive are gabapentin and pregabalin? A systematic review. Eur. Neuropsychopharmacol. 2017, 27, 1185–1215. [Google Scholar] [CrossRef] [PubMed]
- Meara, E.; Horwitz, J.R.; Powell, W.; McClelland, L.; Zhou, W.; O’Malley, A.J.; Morden, N.E. State Legal Restrictions and Prescription-Opioid Use among Disabled Adults. N. Engl. J. Med. 2016, 375, 44–53. [Google Scholar] [CrossRef] [PubMed]
- Center for Disease Control and Prevention. National Center for Health Statistics. About the Ambulatory Health Care Surveys. 2019. Available online: https://www.cdc.gov/nchs/ahcd/about_ahcd.htm (accessed on 18 October 2021).
- Center for Disease Control and Prevention. National Center for Health Statistics. Scope and Sample Design. 2015. Available online: https://www.cdc.gov/nchs/ahcd/ahcd_scope.htm (accessed on 18 October 2021).
- National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS). ICD-9-CM Official Guidelines for Coding and Reporting, Effective October 1, 2011. Available online: https://www.cdc.gov/nchs/data/icd/icd9cm_guidelines_2011.pdf (accessed on 11 February 2021).
- National Center for Health Statistics (NCHS) and the Centers for Medicare and Medicaid Services (CMS). ICD-10-CM Official Guidelines for Coding and Reporting, FY 2021—Updated January 1, 2021. Available online: https://www.cms.gov/files/document/2021-coding-guidelines-updated-12162020.pdf (accessed on 11 February 2021).
- Zhou, L.; Bhattacharjee, S.; Kwoh, C.K.; Tighe, P.J.; Malone, D.C.; Slack, M.; Wilson, D.L.; Brown, J.D.; Lo-Ciganic, W.H. Trends, Patient and Prescriber Characteristics in Gabapentinoid Use in a Sample of United States Ambulatory Care Visits from 2003 to 2016. J. Clin. Med. 2019, 9, 83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Center for Disease Control and Prevention. National Center for Health Statistics. Reliability of Estimates. 2015. Available online: https://www.cdc.gov/nchs/ahcd/ahcd_estimation_reliability.htm (accessed on 18 October 2021).
- Austin, P.C. An Introduction to Propensity Score Methods for Reducing the Effects of Confounding in Observational Studies. Multivariate Behav. Res. 2011, 46, 399–424. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Connor, R.; O’Doherty, J.; O’Regan, A.; Dunne, C. Antibiotic use for acute respiratory tract infections (ARTI) in primary care; what factors affect prescribing and why is it important? A narrative review. Ir. J. Med. Sci. 2018, 187, 969–986. [Google Scholar] [CrossRef] [Green Version]
- Lane, B.H.; Mallow, P.J.; Hooker, M.B.; Hooker, E. Trends in United States emergency department visits and associated charges from 2010 to 2016. Am. J. Emerg. Med. 2020, 38, 1576–1581. [Google Scholar] [CrossRef] [PubMed]
- Poon, S.J.; Schuur, J.D.; Mehrotra, A. Trends in Visits to Acute Care Venues for Treatment of Low-Acuity Conditions in the United States From 2008 to 2015. JAMA Intern. Med. 2018, 178, 1342–1349. [Google Scholar] [CrossRef] [PubMed]
- Rui, P.; Santo, L.; Ashman, J.J. Trends in Opioids Prescribed at Discharge from Emergency Departments Among Adults: United States, 2006–2017. Natl. Health Stat. Rep. 2020, 135, 1–12. [Google Scholar]
- Ryan, N.M.; Gibson, P.G.; Birring, S.S. Arnold’s nerve cough reflex: Evidence for chronic cough as a sensory vagal neuropathy. J. Thorac. Dis. 2014, 6, S748–S752. [Google Scholar] [CrossRef]
- Li, J.; Ye, L. Effect of pregabalin for the treatment of chronic refractory cough: A case report. Medicine 2019, 98, e15916. [Google Scholar] [CrossRef]
- Bastian, Z.J.; Bastian, R.W. The use of neuralgia medications to treat sensory neuropathic cough: Our experience in a retrospective cohort of thirty-two patients. PeerJ 2015, 3, e816. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.K.; Mintz, S. Chronic cough as a sign of laryngeal sensory neuropathy: Diagnosis and treatment. Ann. Otol. Rhinol. Laryngol. 2006, 115, 871. [Google Scholar] [CrossRef] [PubMed]
- Mintz, S.; Lee, J.K. Gabapentin in the treatment of intractable idiopathic chronic cough: Case reports. Am. J. Med. 2006, 119, e13–e15. [Google Scholar] [CrossRef] [PubMed]
- Van de Kerkhove, C.; Goeminne, P.C.; Van Bleyenbergh, P.; Dupont, L.J. A cohort description and analysis of the effect of gabapentin on idiopathic cough. Cough 2012, 8, 9. [Google Scholar] [CrossRef] [Green Version]
- Halum, S.L.; Sycamore, D.L.; McRae, B.R. A new treatment option for laryngeal sensory neuropathy. Laryngoscope 2009, 119, 1844–1847. [Google Scholar] [CrossRef]
- Chung, K.F.; McGarvey, L.; Mazzone, S. Chronic cough and cough hypersensitivity syndrome. Lancet. Respir. Med. 2016, 4, 934–935. [Google Scholar] [CrossRef]
- Dicpinigaitis, P. Understanding the foundations of chronic cough. Am. J. Manag. Care 2020, 26, S232–S238. [Google Scholar] [CrossRef]
- Johansen, M.E. Gabapentinoid Use in the United States 2002 Through 2015. JAMA Intern. Med. 2018, 178, 292–294. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | Opioid Antitussives | Benzonatate | Dextromethorphan a | Gabapentinoids | Opioid Analgesics | Mean ASD b |
|---|---|---|---|---|---|---|
| 63.3 Million (7.7%) | 20.9 Million (2.5%) | 29.7 Million (3.6%) | 13.3 Million (1.6%) | 41.1 Million (5.0%) | ||
| Weighted % | Weighted % | Weighted % | Weighted % | Weighted % | ||
| Patient Characteristics | ||||||
| Age ≥ 65 years | 23.5 | 25.7 | 21.5 | 41.2 | 24.7 | 0.21 |
| Female | 64.8 | 71.3 | 62.6 | 62.9 | 61.6 | 0.09 |
| Race | 0.10 | |||||
| White | 81.0 | 84.1 | 78.9 | 87.5 | 83.1 | |
| Non-White | 19.0 | 15.9 | 21.1 | 12.5 | 16.9 | |
| Smoking status c | 0.16 | |||||
| Current | 15.3 | 12.9 | 14.8 | 19.7 | 24.6 | |
| Non-current | 81.5 | 83.0 | 81.3 | 78.0 | 72.0 | |
| Visit Characteristics | ||||||
| Payment source d | 0.33 | |||||
| Governmental | 27.7 | 30.4 | 31.7 | 53.2 | 44.6 | |
| Commercial | 62.7 | 60.1 | 54.9 | 37.3 | 45.5 | |
| Others | 7.5 | 6.3 | 11.4 | 5.0 | 7.7 | |
| Chronicity of principal reason-for-visit e | 12.9 | 15.5 | 12.0 | 37.8 | 34.1 | 0.37 |
| ≥2 Chronic conditions f | 39.7 | 41.1 | 30.7 | 64.8 | 45.5 | 0.29 |
| Top 3 major reasons-for-visit | ||||||
| Cough 65.1 | Cough 64.0 | Cough 55.3 | Cough 38.3 | Cough 39.8 | ||
| Nasal congestion 21.4 | Nasal congestion 18.3 | Throat symptom 26.0 | Nasal congestion 12.5 | Throat symptom 14.5 | ||
| Throat symptom 19.0 | Throat symptom 16.7 | Nasal congestion 22.9 | Throat symptom 11.1 | Nasal congestion 10.7 | ||
| Top 3 major diagnoses | ||||||
| Bronchitis 39.1 | Acute URTI 39.8 | Acute URTI 53.4 | Bronchitis 22.6 | Acute URTI 30.8 | ||
| Acute URTI 36.8 | Cough 30.0 | Bronchitis 27.0 | Acute URTI 21.9 | Bronchitis 25.8 | ||
| Cough 15.8 | Bronchitis 26.1 | Cough 14.9 | Chronic URTD 17.7 | Chronic URTD 16.4 | ||
| Practice characteristics | ||||||
| Prescriber specialty | 0.37 | |||||
| Primary care | 88.7 | 89.0 | 88.6 | 76.7 | 80.1 | |
| Others | 11.3 | 11.0 | 11.4 | 23.3 | 19.9 | |
| Geographic region g | 0.22 | |||||
| Northeast | 12.4 | 11.1 | 21.7 | 12.4 | 10.9 | |
| Midwest | 19.5 | 16.2 | 14.4 | 22.4 | 20.9 | |
| South | 44.6 | 53.8 | 42.0 | 43.1 | 41.4 | |
| West | 23.5 | 19.0 | 21.8 | 22.1 | 26.9 | |
| Metropolitan area | 86.7 | 90.9 | 88.5 | 76.4 | 83.6 | 0.14 |
| Characteristics | Opioid Antitussives | Benzonatate | Dextromethorphan a | Opioid Analgesics | Mean ASD b |
|---|---|---|---|---|---|
| 9.7 Million (6.2%) | 7.5 Million (4.8%) | 2.9 Million (1.9%) | 22.7 Million (14.6%) | ||
| Weighted% | Weighted% | Weighted% | Weighted% | ||
| Patient Characteristics | |||||
| Age ≥ 65 years | 10.6 | 10.8 | 10.5 | 15.4 | 0.07 |
| Female | 63.2 | 65.8 | 62.1 | 63.0 | 0.03 |
| Race | 0.13 | ||||
| White | 71.3 | 68.0 | 59.1 | 72.7 | |
| Non-White | 28.7 | 32.0 | 40.9 | 27.3 | |
| Visit Characteristics | |||||
| Payment source c | 0.10 | ||||
| Governmental | 37.8 | 40.2 | 40.7 | 46.1 | |
| Commercial | 31.9 | 31.5 | 26.6 | 27.8 | |
| Others | 28.6 | 27.7 | 31.5 | 24.5 | |
| ≥2 Chronic Conditions d | 24.9 | 26.5 | 27.8 | 31.9 | 0.08 |
| Top 3 major reasons-for-visit | |||||
| Cough 66.5 | Cough 68.3 | Cough 61.0 | Cough 35.3 | ||
| Throat symptoms 17.8 | Throat symptoms 18.1 | Throat symptoms 21.3 | Throat symptoms 16.8 | ||
| Fever 15.9 | Nasal congestion 17.7 | Nasal congestion 20.7 | Shortness of breath 15.0 | ||
| Top 3 major diagnoses | |||||
| Bronchitis 44.6 | Bronchitis 40.9 | Acute URTI 37.0 | Acute URTI 28.4 | ||
| Acute URTI 28.8 | Acute URTI 33.3 | Bronchitis 34.5 | Bronchitis 24.7 | ||
| Cough 14.4 | Cough 23.1 | Cough 16.3 | Pneumonia 18.6 | ||
| Practice Characteristics | |||||
| Geographic region | 0.21 | ||||
| Northeast | 12.8 | 16.0 | 9.5 | 10.0 | |
| Midwest | 20.0 | 23.0 | 19.8 | 22.6 | |
| South | 51.3 | 47.8 | 54.3 | 42.2 | |
| West | 15.9 | 13.2 | 16.4 | 25.2 | |
| Metropolitan area e | 77.8 | 83.2 | 78.2 | 86.2 | 0.13 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, S.; Hincapie-Castillo, J.M.; Ke, X.; Schelfhout, J.; Ding, H.; Sher, M.R.; Zhou, L.; Chang, C.-Y.; Wilson, D.L.; Lo-Ciganic, W.-H. Evaluation of Cough Medication Use Patterns in Ambulatory Care Settings in the United States: 2003–2018. J. Clin. Med. 2022, 11, 3671. https://doi.org/10.3390/jcm11133671
Yang S, Hincapie-Castillo JM, Ke X, Schelfhout J, Ding H, Sher MR, Zhou L, Chang C-Y, Wilson DL, Lo-Ciganic W-H. Evaluation of Cough Medication Use Patterns in Ambulatory Care Settings in the United States: 2003–2018. Journal of Clinical Medicine. 2022; 11(13):3671. https://doi.org/10.3390/jcm11133671
Chicago/Turabian StyleYang, Seonkyeong, Juan M. Hincapie-Castillo, Xuehua Ke, Jonathan Schelfhout, Helen Ding, Mandel R. Sher, Lili Zhou, Ching-Yuan Chang, Debbie L. Wilson, and Wei-Hsuan Lo-Ciganic. 2022. "Evaluation of Cough Medication Use Patterns in Ambulatory Care Settings in the United States: 2003–2018" Journal of Clinical Medicine 11, no. 13: 3671. https://doi.org/10.3390/jcm11133671