
Exploring Retinal Blood Vessel Diameters as Biomarkers in Multiple Sclerosis

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Oximetry Imaging and Measurements
2.2. Statistics
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Walton, C.; King, R.; Rechtman, L.; Kaye, W.; Leray, E.; Marrie, R.A.; Robertson, N.; la Rocca, N.; Uitdehaag, B.; van der Mei, I.; et al. Rising prevalence of multiple sclerosis worldwide: Insights from the Atlas of MS, third edition. Mult. Scler. 2020, 26, 1816–1821. [Google Scholar] [CrossRef] [PubMed]
- Costello, F. The afferent visual pathway: Designing a structural-functional paradigm of multiple sclerosis. ISRN Neurol. 2013, 2013, 134858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costello, K. Multiple sclerosis research: Diagnostics, disease-modifying treatments, and emerging therapies. J. Neurosci. Nurs. 2013, 45 (Suppl. S1), S14–S23. [Google Scholar] [CrossRef] [PubMed]
- Graham, S.L.; Klistorner, A. Afferent visual pathways in multiple sclerosis: A review. Clin. Exp. Ophthalmol. 2017, 45, 62–72. [Google Scholar] [CrossRef] [Green Version]
- Reulen, J.P.; Sanders, E.A.; Hogenhuis, L.A. Eye movement disorders in multiple sclerosis and optic neuritis. Brain 1983, 106 Pt 1, 121–140. [Google Scholar] [CrossRef]
- Fuest, M.; Rößler, G.; Walter, P.; Plange, N. Retinal vasculitis as manifestation of multiple sclerosis. Ophthalmologe 2014, 111, 871–875. [Google Scholar] [CrossRef]
- Pedraza-Concha, A.; Brandauer, K.; Tello, A.; Rangel, C.M.; Scheib, C. Bilateral Anterior and Intermediate Uveitis with Occlusive Vasculitis as Sole Manifestation of Relapse in Multiple Sclerosis. Case Rep. Ophthalmol. Med. 2019, 2019, 8239205. [Google Scholar] [CrossRef] [Green Version]
- Schmitt, C.; Strazielle, N.; Ghersi-Egea, J.F. Brain leukocyte infiltration initiated by peripheral inflammation or experimental autoimmune encephalomyelitis occurs through pathways connected to the CSF-filled compartments of the forebrain and midbrain. J. Neuroinflamm. 2012, 9, 1–15. [Google Scholar] [CrossRef]
- Petzold, A.; de Boer, J.F.; Schippling, S.; Vermersch, P.; Kardon, R.; Green, A.; Calabresi, P.A.; Polman, C. Optical coherence tomography in multiple sclerosis: A systematic review and meta-analysis. Lancet Neurol. 2010, 9, 921–932. [Google Scholar] [CrossRef] [Green Version]
- Trapp, B.D.; Peterson, J.; Ransohoff, R.M.; Rudick, R.; Mörk, S.; Bö, L. Axonal transection in the lesions of multiple sclerosis. N. Engl. J. Med. 1998, 338, 278–285. [Google Scholar] [CrossRef]
- Balcer, L.J. Clinical trials to clinical use: Using vision as a model for multiple sclerosis and beyond. J. Neuroophthalmol. 2014, 34, S18–S23. [Google Scholar] [CrossRef] [PubMed]
- Kolinko, Y.; Krakorova, K.; Cendelin, J.; Kralickova, Z.T.M. Microcirculation of the brain: Morphological assessment in degenerative diseases and restoration processes. Rev. Neurosci. 2015, 26, 75–93. [Google Scholar] [CrossRef] [PubMed]
- Sepulcre, J.; Murie-Fernandez, M.; Salinas-Alaman, A.; García-Layana, A.; Bejarano, B.; Villoslada, P. Diagnostic accuracy of retinal abnormalities in predicting disease activity in MS. Neurology 2007, 68, 1488–1494. [Google Scholar] [CrossRef] [PubMed]
- Engell, T. Neurological disease activity in multiple sclerosis patients with periphlebitis retinae. Acta Neurol. Scand. 1986, 73, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Kerrison, J.B.; Flynn, T.; Green, W.R. Retinal pathologic changes in multiple sclerosis. Retina 1994, 14, 445–451. [Google Scholar] [CrossRef] [PubMed]
- Harris, A.; Ciulla, T.A.; Chung, H.S.; Martin, B. Regulation of retinal and optic nerve blood flow. Arch. Ophthalmol. 1998, 116, 1491–1495. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Russo, A.; Costagliola, C.; Rizzoni, D.; Ghilardi, N.; Turano, R.; Semeraro, F. Arteriolar Diameters in Glaucomatous Eyes with Single-Hemifield Damage. Optom. Vis. Sci. 2016, 93, 504–509. [Google Scholar] [CrossRef]
- Bhaduri, B.; Nolan, R.M.; Shelton, R.L.; Pilutti, L.A.; Motl, R.W.; Moss, H.E.; Pula, J.H.; Boppart, S.A. Detection of retinal blood vessel changes in multiple sclerosis with optical coherence tomography. Biomed. Opt. Express. 2016, 7, 2321–2330. [Google Scholar] [CrossRef] [Green Version]
- Balcer, L.J.; Raynowska, J.; Nolan, R.; Galetta, S.L.; Kapoor, R.; Benedict, R.; Phillips, G.; LaRocca, N.; Lynn, H.; Richard, R.; et al. Validity of low-contrast letter acuity as a visual performance outcome measure for multiple sclerosis. Mult. Scler. 2017, 23, 734–747. [Google Scholar] [CrossRef]
- Einarsdottir, A.B.; Olafsdottir, O.B.; Hjaltason, H.; Hardarson, S.H. Retinal oximetry is affected in multiple sclerosis. Acta. Ophthalmol. 2018, 96, 528–530. [Google Scholar] [CrossRef] [Green Version]
- McDonald, W.I.; Compston, A.; Edan, G.; Goodkin, D.; Hartung, H.-P.; Lublin, F.D.; McFarland, H.F.; Paty, D.W.; Polman, C.H.; Reingold, S.C.; et al. Recommended diagnostic criteria for multiple sclerosis: Guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann. Neurol. 2001, 50, 121–127. [Google Scholar] [CrossRef] [PubMed]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kurtzke, J.F. Rating neurologic impairment in multiple sclerosis: An expanded disability status scale (EDSS). Neurology 1983, 33, 1444–1452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stulting, R.D.; Dupps, W.J., Jr.; Kohnen, T.; Mamalis, N.; Rosen, E.S.; Koch, D.D.; Obstbaum, S.A.; Waring, G.O., III; Reinstein, D.Z. Standardized graphs and terms for refractive surgery results. Cornea 2011, 30, 945–947. [Google Scholar] [CrossRef]
- Hardarson, S.H.; Harris, A.; Karlsson, R.A.; Halldorsson, G.H.; Kagemann, L.; Rechtman, E.; Zoega, G.M.; Eysteinsson, T.; Benediktsson, J.A.; Thorsteinsson, A.; et al. Automatic retinal oximetry. Invest. Ophthalmol. Vis. Sci. 2006, 47, 5011–5016. [Google Scholar] [CrossRef]
- Veiby, N.C.B.B.; Simeunovic, A.; Heier, M.; Brunborg, C.; Saddique, N.; Moe, M.C.; Dahl-Jørgensen, K.; Margeirsdottir, H.D.; Petrovski, G. Venular oxygen saturation is increased in young patients with type 1 diabetes and mild nonproliferative diabetic retinopathy. Acta. Ophthalmol. 2020, 98, 800–807. [Google Scholar] [CrossRef]
- Geirsdottir, A.; Palsson, O.; Hardarson, S.H.; Olafsdottir, O.B.; Kristjansdottir, J.V.; Stefánsson, E. Retinal vessel oxygen saturation in healthy individuals. Invest. Ophthalmol. Vis. Sci. 2012, 53, 5433–5442. [Google Scholar] [CrossRef] [Green Version]
- Blondal, R.; Sturludottir, M.K.; Hardarson, S.H.; Halldorsson, G.H.; Stefánsson, E. Reliability of vessel diameter measurements with a retinal oximeter. Graefes. Arch. Clin. Exp. Ophthalmol. 2011, 249, 1311–1317. [Google Scholar] [CrossRef] [Green Version]
- Wang, X.; Jia, Y.; Spain, R.; Potsaid, B.; Liu, J.J.; Baumann, B.; Hornegger, J.; Fujimoto4, J.G.; Wu, Q.; Huang, D. Optical coherence tomography angiography of optic nerve head and parafovea in multiple sclerosis. Br. J. Ophthalmol. 2014, 98, 1368–1373. [Google Scholar] [CrossRef] [Green Version]
- Christiansen, C.F. Risk of vascular disease in patients with multiple sclerosis: A review. Neurol. Res. 2012, 34, 746–753. [Google Scholar] [CrossRef]
- Geraldes, R.; Esiri, M.M.; Perera, R.; Yee, S.A.; Jenkins, D.; Palace, J.; DeLuca, G.C. Vascular disease and multiple sclerosis: A post-mortem study exploring their relationships. Brain 2020, 143, 2998–3012. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.J.; Liew, G.; Klein, R.; Rochtchina, E.; Knudtson, M.D.; Klein, B.E.K.; Wong, T.Y.; Burlutsky, G.; Mitchell, P. Retinal vessel diameter and cardiovascular mortality: Pooled data analysis from two older populations. Eur. Heart J. 2007, 28, 1984–1992. [Google Scholar] [CrossRef] [PubMed]
- Moss, H.E. Retinal vascular changes are a marker for cerebral vascular diseases. Curr. Neurol. Neurosci. Rep. 2015, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bek, T. Diameter changes of retinal vessels in diabetic retinopathy. Curr. Diab. Rep. 2017, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Healthy Controls | People with MS | |
|---|---|---|
| Eyes, n (Patients, n) | 45 (23) | 44 (23) |
| Mean Age, years (SD) | 34.8 (8.1) | 32.2 (7.5) |
| Female sex, n (%) | 13 (56.5) | 13 (56.5) |
| Time since diagnosis, weeks (SD) | - | 2 (SD) |
| Optic Neuritis, n (Patients, n) | 0 (0) | 2 (2) |
| EDSS, n (Patients, n): 0; 1.0; 1.5; 2,0; 2.5; 3.0 | - | 3; 6; 6; 3, 4, 1 |
| Variable | Healthy Controls (n = 23) | People with MS (n = 23) | p-Value |
|---|---|---|---|
| Retinal arteriolar diameter (µm) Mean (±SD) 95% CI | 120.6 (11.5) 115.4–126–0 | 112.6 (10.7) 108.1–11.0 | 0.0013 |
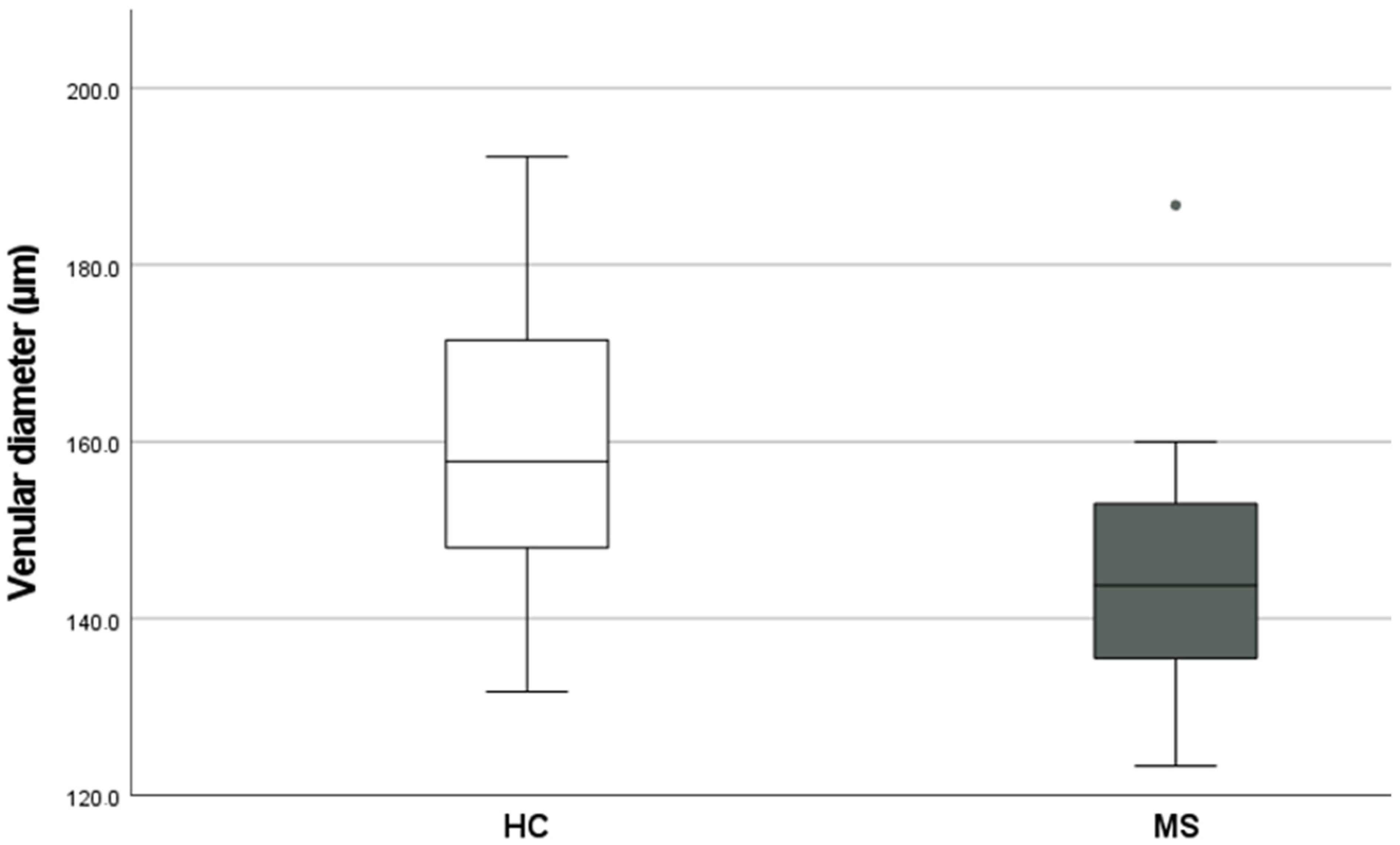
| Retinal venular diameter (µm) Median, Range (IQR) | 157.8 (148.0–171.5) | 143.8 (123.3–186.8) | 0.0089 |
| A-V difference in % Mean (SD) 95% CI | 38.3 (14.8) 31.5–45.0 | 31.8 (12.0) 27.0–37.0 | 0.0527 |
| Arteriolar O2 saturation (%) Mean (±SD) 95% CI | 91.5 (7.3) 88.2–95.0 | 93.7 (4.2) 92.0–95.5 | 0.8934 |
| Venular O2 saturation in% Mean (±SD) 95% CI | 59.3 (9.5) 55.0–64.0 | 60.0 (4.6) 92.0–95.5 | 0.5980 |
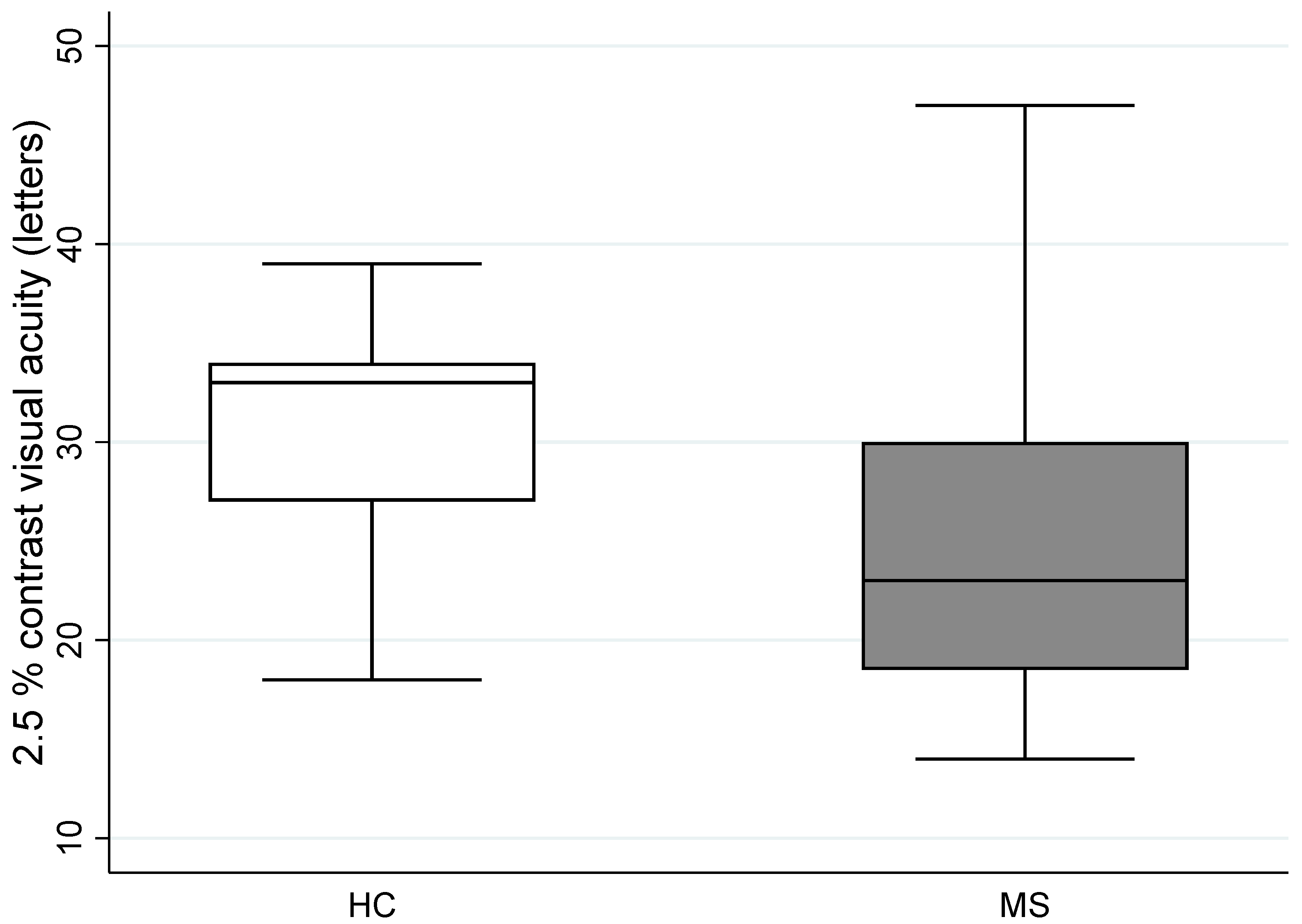
| 2.5% contrast visual acuity, number of letters Left eye Median, Range (IQR) | 31 (27.0–34.0) | 23 (18.5–30.0) | 0.0143 |
| High contrast visual acuity Right eye /Left eye Mean (±SD) 95% CI | 0.43 (0.09) 0.38–0.47/ 0.44 (0.12) 0.38–0.50 | 0.35 (0.23) 0.25–0.45/ 0.43 (0.24) 0.33–0.53 | 0.0722 0.04022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Drobnjak Nes, D.; Berg-Hansen, P.; de Rodez Benavent, S.A.; Høgestøl, E.A.; Beyer, M.K.; Rinker, D.A.; Veiby, N.; Karabeg, M.; Petrovski, B.É.; Celius, E.G.; et al. Exploring Retinal Blood Vessel Diameters as Biomarkers in Multiple Sclerosis. J. Clin. Med. 2022, 11, 3109. https://doi.org/10.3390/jcm11113109
Drobnjak Nes D, Berg-Hansen P, de Rodez Benavent SA, Høgestøl EA, Beyer MK, Rinker DA, Veiby N, Karabeg M, Petrovski BÉ, Celius EG, et al. Exploring Retinal Blood Vessel Diameters as Biomarkers in Multiple Sclerosis. Journal of Clinical Medicine. 2022; 11(11):3109. https://doi.org/10.3390/jcm11113109
Chicago/Turabian StyleDrobnjak Nes, Dragana, Pål Berg-Hansen, Sigrid A. de Rodez Benavent, Einar A. Høgestøl, Mona K. Beyer, Daniel A. Rinker, Nina Veiby, Mia Karabeg, Beáta Éva Petrovski, Elisabeth G. Celius, and et al. 2022. "Exploring Retinal Blood Vessel Diameters as Biomarkers in Multiple Sclerosis" Journal of Clinical Medicine 11, no. 11: 3109. https://doi.org/10.3390/jcm11113109