
Elevated Thyroxine Concentration and Lithium Intoxication—An Analysis Based on the LiSIE Retrospective Cohort Study

 , , ,
, , ,
Abstract
:1. Introduction
Aims
- Hyperthyroxinaemia is commonly associated with lithium intoxication.
- Hyperthyroxinaemia leads to increased tubular reabsorption of lithium, which increases the risk of lithium intoxication.
2. Materials and Methods
2.1. Study Design
2.2. Lithium—Study into Effects and Side Effects Participants
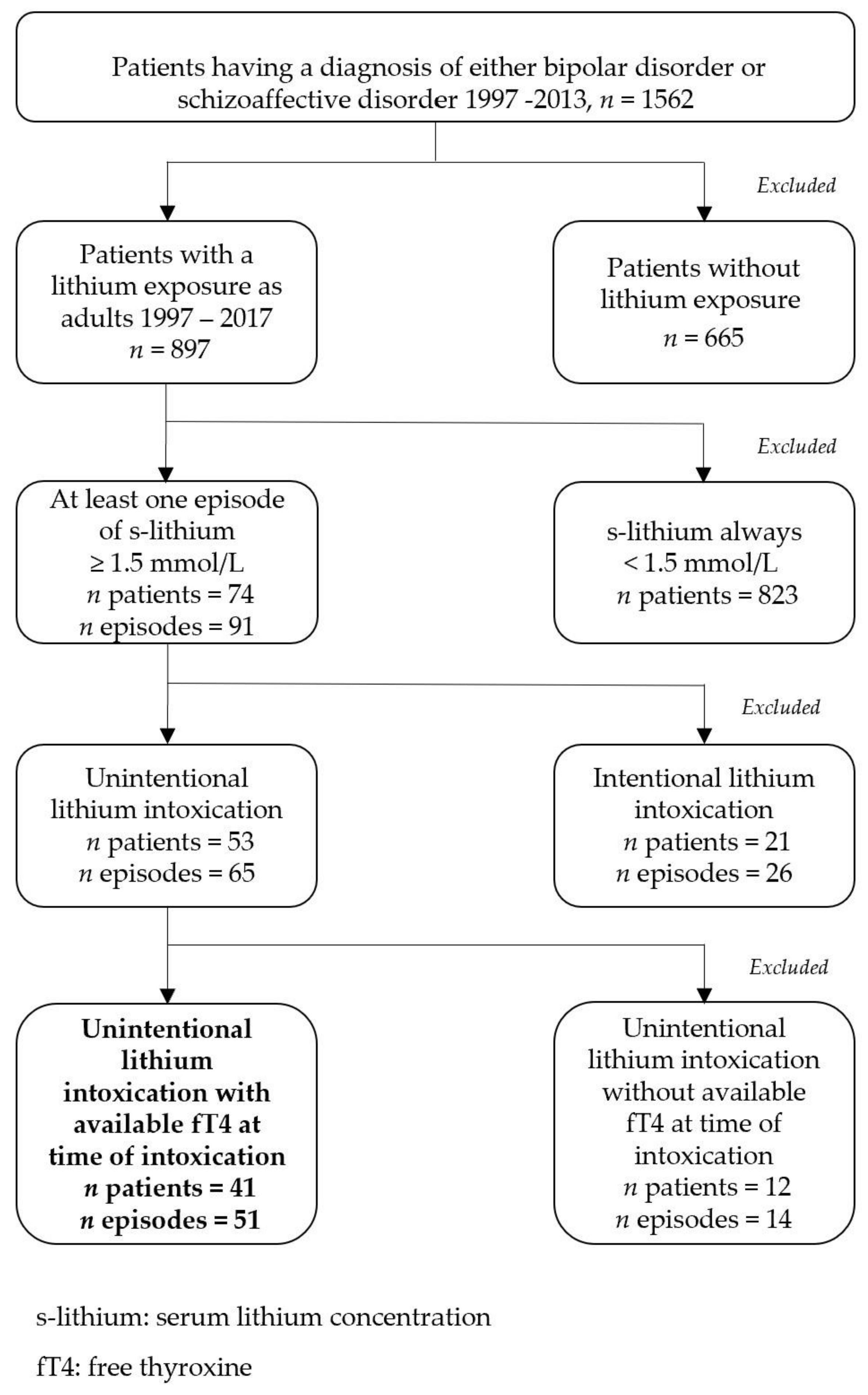
2.3. Patient Selection and Inclusion Criteria
2.4. Exclusion Criteria
2.5. Outcome Definition
2.6. Exposure Parameters
2.6.1. Lithium Exposure
2.6.2. Hyperthyroxinaemia
2.6.3. Renal Function
2.6.4. Other Variables
2.7. Chart Review, Analysis, and Validation
2.8. Control for Bias and Missing Data
2.9. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Hypothesis 1: Hyperthyroxinaemia Is Commonly Associated with Lithium Intoxication
3.3. Hypothesis 2: Hyperthyroxinaemia Leads to Increased Tubular Reabsorption of Lithium, Which Increases the Risk of Lithium Intoxication
4. Discussion
4.1. Strengths
4.2. Weaknesses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bocchetta, A.; Cocco, F.; Velluzzi, F.; Del Zompo, M.; Mariotti, S.; Loviselli, A. Fifteen-year follow-up of thyroid function in lithium patients. J. Endocrinol. Invest. 2007, 30, 363–366. [Google Scholar] [CrossRef]
- Fairbrother, F.; Petzl, N.; Scott, J.G.; Kisely, S. Lithium can cause hyperthyroidism as well as hypothyroidism: A systematic review of an under-recognised association. Aust. N. Z. J. Psychiatry 2019, 53, 384–402. [Google Scholar] [CrossRef] [PubMed]
- Hayes, J.F.; Marston, L.; Walters, K.; Geddes, J.R.; King, M.; Osborn, D.P. Adverse Renal, Endocrine, Hepatic, and Metabolic Events during Maintenance Mood Stabilizer Treatment for Bipolar Disorder: A Population-Based Cohort Study. PLoS Med. 2016, 13, e1002058. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.W.; Dawson, A.H.; Whyte, I.M. Lithium: Thyroid effects and altered renal handling. J. Toxicol. Clin. Toxicol. 2000, 38, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Bandyopadhyay, D.; Nielsen, C. Lithium-induced hyperthyroidism, thyrotoxicosis and mania: A case report. QJM 2012, 105, 83–85. [Google Scholar] [CrossRef] [Green Version]
- Sato, Y.; Taki, K.; Honda, Y.; Takahashi, S.; Yoshimura, A. Lithium toxicity precipitated by thyrotoxicosis due to silent thyroiditis: Cardiac arrest, quadriplegia, and coma. Thyroid 2013, 23, 766–770. [Google Scholar] [CrossRef]
- Miller, K.K.; Daniels, G.H. Association between lithium use and thyrotoxicosis caused by silent thyroiditis. Clin. Endocrinol. 2001, 55, 501–508. [Google Scholar] [CrossRef]
- Ng, Y.W.; Tiu, S.C.; Choi, K.L.; Chan, F.K.; Choi, C.H.; Kong, P.S.; Ng, C.M.; Shek, C.C. Use of lithium in the treatment of thyrotoxicosis. Hong Kong Med. J. 2006, 12, 254–259. [Google Scholar]
- Gupta, Y.; Singh, S.; Ammini, A.C. Development of Graves’ disease after long-standing hypothyroidism on treatment, with acute toxicity to thionamides and lithium. BMJ Case Rep. 2012, 2012, bcr2012006433. [Google Scholar] [CrossRef] [Green Version]
- Gavin, L.A.; Rosenthal, M.; Cavalieri, R.R. The diagnostic dilemma of isolated hyperthyroxinemia in acute illness. JAMA 1979, 242, 251–253. [Google Scholar] [CrossRef]
- Spratt, D.I.; Pont, A.; Miller, M.B.; McDougall, I.R.; Bayer, M.F.; McLaughlin, W.T. Hyperthyroxinemia in patients with acute psychiatric disorders. Am. J. Med. 1982, 73, 41–48. [Google Scholar] [CrossRef]
- Lieber, I.; Ott, M.; Öhlund, L.; Lundqvist, R.; Eliasson, M.; Sandlund, M.; Werneke, U. Lithium-associated hypothyroidism and potential for reversibility after lithium discontinuation: Findings from the LiSIE retrospective cohort study. J. Psychopharmacol. 2020, 34, 293–303. [Google Scholar] [CrossRef]
- Ott, M.; Stegmayr, B.; Salander Renberg, E.; Werneke, U. Lithium intoxication: Incidence, clinical course and renal function—A population-based retrospective cohort study. J. Psychopharmacol. 2016, 30, 1008–1019. [Google Scholar] [CrossRef] [Green Version]
- Chen, K.P.; Shen, W.W.; Lu, M.L. Implication of serum concentration monitoring in patients with lithium intoxication. Psychiatry Clin. Neurosci. 2004, 58, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Council for International Organizations of Medical Sciences. Guidelines for Preparing Core Clinical-Safety Information on Drugs. Essential Drugs Monitor; World Health Organization: Geneva, Switzerland, 1996; Volume 22, p. 18. [Google Scholar]
- Levey, A.S.; Stevens, L.A.; Schmid, C.H.; Zhang, Y.L.; Castro, A.F., 3rd; Feldman, H.I.; Kusek, J.W.; Eggers, P.; Van Lente, F.; Greene, T.; et al. A new equation to estimate glomerular filtration rate. Ann. Intern. Med. 2009, 150, 604–612. [Google Scholar] [CrossRef]
- Koomans, H.A.; Boer, W.H.; Dorhout Mees, E.J. Evaluation of lithium clearance as a marker of proximal tubule sodium handling. Kidney Int. 1989, 36, 2–12. [Google Scholar] [CrossRef] [Green Version]
- Barclay, M.L.; Brownlie, B.E.; Turner, J.G.; Wells, J.E. Lithium associated thyrotoxicosis: A report of 14 cases, with statistical analysis of incidence. Clin. Endocrinol. 1994, 40, 759–764. [Google Scholar] [CrossRef]
- Kirov, G.; Tredget, J.; John, R.; Owen, M.J.; Lazarus, J.H. A cross-sectional and a prospective study of thyroid disorders in lithium-treated patients. J. Affect. Disord. 2005, 87, 313–317. [Google Scholar] [CrossRef]
- Dickerman, A.L.; Barnhill, J.W. Abnormal thyroid function tests in psychiatric patients: A red herring? Am. J. Psychiatry 2012, 169, 127–133. [Google Scholar] [CrossRef]
- Carney, M.W.; Macleod, S.; Sheffield, B.F. Thyroid function screening in psychiatric in-patients. Br. J. Psychiatry 1981, 138, 154–156. [Google Scholar] [CrossRef]
- Timmons, J.G.; Mukhopadhyay, B. Hyperthyroxinemia with a non-suppressed TSH: How to confidently reach a diagnosis in this clinical conundrum. Hormones 2020, 19, 311–315. [Google Scholar] [CrossRef] [Green Version]
- Styra, R.; Joffe, R.; Singer, W. Hyperthyroxinemia in major affective disorders. Acta Psychiatr. Scand. 1991, 83, 61–63. [Google Scholar] [CrossRef]
- Kinsella, J.; Sacktor, B. Thyroid hormones increase Na+-H+ exchange activity in renal brush border membranes. Proc. Natl. Acad. Sci. USA 1985, 82, 3606–3610. [Google Scholar] [CrossRef] [Green Version]
- Owada, A.; Tomita, K.; Ujiie, K.; Akiba, T.; Marumo, F. Decreased lithium clearance in patients with hyperthyroidism. Nephron 1993, 64, 37–41. [Google Scholar] [CrossRef]
- Schairer, B.; Jungreithmayr, V.; Schuster, M.; Reiter, T.; Herkner, H.; Gessl, A.; Sengolge, G.; Winnicki, W. Effect of Thyroid Hormones on Kidney Function in Patients after Kidney Transplantation. Sci. Rep. 2020, 10, 2156. [Google Scholar] [CrossRef] [Green Version]
- den Hollander, J.G.; Wulkan, R.W.; Mantel, M.J.; Berghout, A. Correlation between severity of thyroid dysfunction and renal function. Clin. Endocrinol. 2005, 62, 423–427. [Google Scholar] [CrossRef]
- Mariani, L.H.; Berns, J.S. The renal manifestations of thyroid disease. J. Am. Soc. Nephrol. 2012, 23, 22–26. [Google Scholar] [CrossRef] [Green Version]
- Tsuda, A.; Inaba, M.; Ichii, M.; Ochi, A.; Ohno, Y.; Nakatani, S.; Yamada, S.; Mori, K.; Tahara, H.; Ishimura, E. Relationship between serum TSH levels and intrarenal hemodynamic parameters in euthyroid subjects. Eur. J. Endocrinol. 2013, 169, 45–50. [Google Scholar] [CrossRef] [Green Version]
- Iglesias, P.; Bajo, M.A.; Selgas, R.; Diez, J.J. Thyroid dysfunction and kidney disease: An update. Rev. Endocr. Metab. Disord. 2017, 18, 131–144. [Google Scholar] [CrossRef]
- Vargas, F.; Rodriguez-Gomez, I.; Vargas-Tendero, P.; Jimenez, E.; Montiel, M. The renin-angiotensin system in thyroid disorders and its role in cardiovascular and renal manifestations. J. Endocrinol. 2012, 213, 25–36. [Google Scholar] [CrossRef] [Green Version]
- Ritchie, M.; Yeap, B.B. Thyroid hormone: Influences on mood and cognition in adults. Maturitas 2015, 81, 266–275. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Very Common | ≥1/10 | ≥10% |
|---|---|---|
| Common (Frequent) | ≥1/100 and <1/10 | ≥1% and <10% |
| Uncommon (Infrequent) | ≥1/1000 and <1/100 | ≥0.1% and <1% |
| Rare | ≥1/10,000 and <1/1000 | ≥0.01% and <0.1% |
| Very Rare | <1/10,000 | <0.01% |
| Patients Exposed to Lithium, n | 897 |
|---|---|
| Sex, n (%) Male Female | 357 (39.8) 540 (60.2) |
| Age (years) at study start Mean (SD) Median (min–max) | 45.0 (15.2) 45.0 (18–92) |
| Type of diagnosis, n (%) Bipolar disorder Schizoaffective disorder | 768 (85.6) 129 (14.4) |
| Time of lithium exposure (person–years) Total Mean (SD) Median (min–max) | 6684 7.5 (6.5) 5.7 (0–21) |
| Episode a | fT4 (pmol/L) b | fT3 (pmol/L) c | eGFR (mL/min/1.73m2) | s-Lithium (mmol/L) | NDI | Presumed Main Cause of Lithium Intoxication | |||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Before | During | Before | During | Before | During | Before | During | ↑ tubular reabsorption attributable to ↑ fT4 | Alternative explanation: | ||
| 1 | 22.3 | 84.1 | NA | 17.3 | 51 | 22 | 0.66 | 1.61 | No | Unlikely | Addition of ARB and spironolactone 4 weeks before intoxication leading to ↓ GFR |
| 2 | 16.1 | 30.1 | 3.1 | 5.7 | 85 | 64 | 0.82 | 1.74 | No | Unlikely | ↓ GFR, reason unclear |
| 3 | 19.3 | 28.1 | 3.9 | NA | 67 | 15 | 0.81 | 4.20 | No | Unlikely | Infection/pyelonephritis leading to ↓ GFR |
| 4 | 19.5 | 24.7 | NA | NA | 37 | 6 | 0.83 | 1.50 | No | Unlikely | Postrenal AKI leading to ↓ GFR |
| 5 | NA | 24.7 | NA | NA | 64 | 42 | 0.62 | 2.59 | No | Unlikely | ACEI and thiazide 11 weeks before leading to ↓ GFR |
| 6 | 18.9 | 24.1 | 3.9 | 2.7 | 89 | 41 | 0.67 | 1.57 | No | Unlikely | Dehydration and colitis leading to ↓ GFR |
| 7 | 14.8 | 23.4 | 3.5 | 2.0 | 72 | 62 | 0.62 | 1.56 | Yes | Unlikely | NDI and dehydration leading to ↓ GFR |
| 8 | 13.7 | 22.6 | 3.4 | 4.9 | 54 | 26 | 0.69 | 2.02 | No | Unlikely | Treatment with amiloride/hydrochlorothiazide 2 weeks before leading to ↓ GFR |
| 9 | 20.8 | 22.4 | 5.2 | NA | 46 | 5 | 0.31 | 1.81 | No | Unlikely | Sepsis and prerenal AKI leading to ↓ GFR |
| Case | Study | Sex | Age (years) | Limax mmol/L | fT4intox pmol/L (Upper Normal Reference) | Creatinine µmol/L (Upper Normal Reference) eGFR a | Presumed Cause of Lithium Intoxication b | |
|---|---|---|---|---|---|---|---|---|
| Elevation fT4 Mediated (Dehydration/Tubular) | Alternative Explanation | |||||||
| Lithium Used as Treatment for an Affective Disorder | ||||||||
| 1 | [4] | F | 34 | 3.27 | 72.4 (25.0) | 387 (100) 13 | Unlikely | Nephrogenic diabetes insipidus leading to dehydration leading to AKI and ↓ GFR Thioridazine interaction with lithium. Hyperthyroidism mediated dehydration possible |
| 2 | [6] | F | 64 | 3.81 | 57.3 (19.1) | 226 (71) 20 | Unlikely | Hyperthyroidism mediated dehydration possible AKI due to another reason leading to ↓ GFR cannot be excluded |
| 3 | [5] | F | 46 | 3.6 | 38.6 (23.2) | Normal | Possible | No |
| 4 | [7] | F | 36 | 1.6 | FT4I 21.6 (4–12ng/L) c | Not known | Not enough information to rate | |
| Lithium Used as a Treatment for Hyperthyroidism | ||||||||
| 5 | [8] | F | 37 | 3.40 | 103 (23.2) | Normal | Possible | No |
| 6 | [9] | F | 66 | 1.54 | 31.8 (21.9) | Normal | Possible | No |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lieber, I.; Ott, M.; Lundqvist, R.; Eliasson, M.; Sandlund, M.; Werneke, U. Elevated Thyroxine Concentration and Lithium Intoxication—An Analysis Based on the LiSIE Retrospective Cohort Study. J. Clin. Med. 2022, 11, 3041. https://doi.org/10.3390/jcm11113041
Lieber I, Ott M, Lundqvist R, Eliasson M, Sandlund M, Werneke U. Elevated Thyroxine Concentration and Lithium Intoxication—An Analysis Based on the LiSIE Retrospective Cohort Study. Journal of Clinical Medicine. 2022; 11(11):3041. https://doi.org/10.3390/jcm11113041
Chicago/Turabian StyleLieber, Ingrid, Michael Ott, Robert Lundqvist, Mats Eliasson, Mikael Sandlund, and Ursula Werneke. 2022. "Elevated Thyroxine Concentration and Lithium Intoxication—An Analysis Based on the LiSIE Retrospective Cohort Study" Journal of Clinical Medicine 11, no. 11: 3041. https://doi.org/10.3390/jcm11113041