
Long-Term Maintenance of Sinus Rhythm Is Associated with Favorable Echocardiographic Remodeling and Improved Clinical Outcomes after Transcatheter Aortic Valve Replacement

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Definitions and Outcomes
2.3. AF Management and Follow-Up
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics
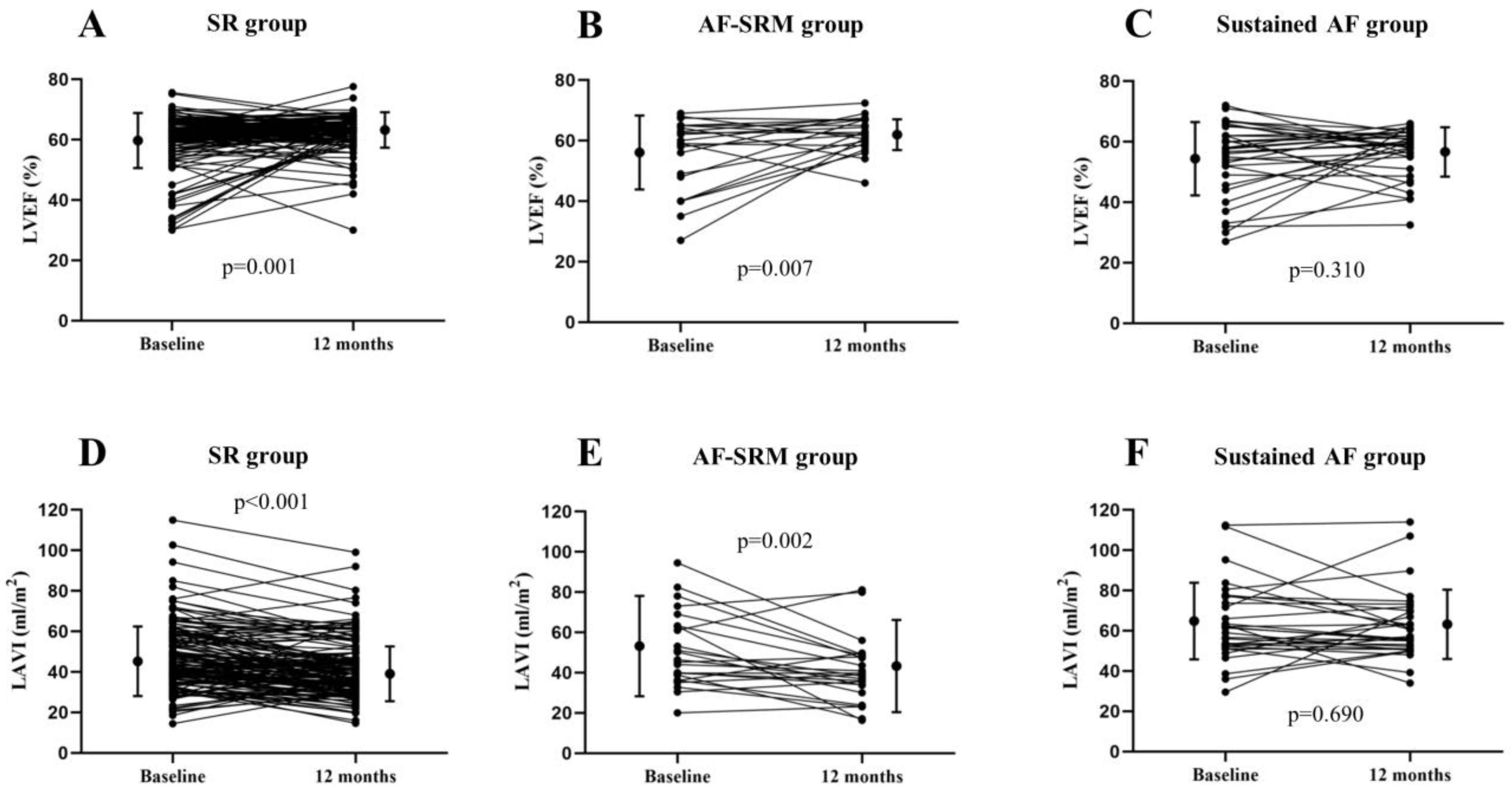
3.2. Echocardiographic Improvement
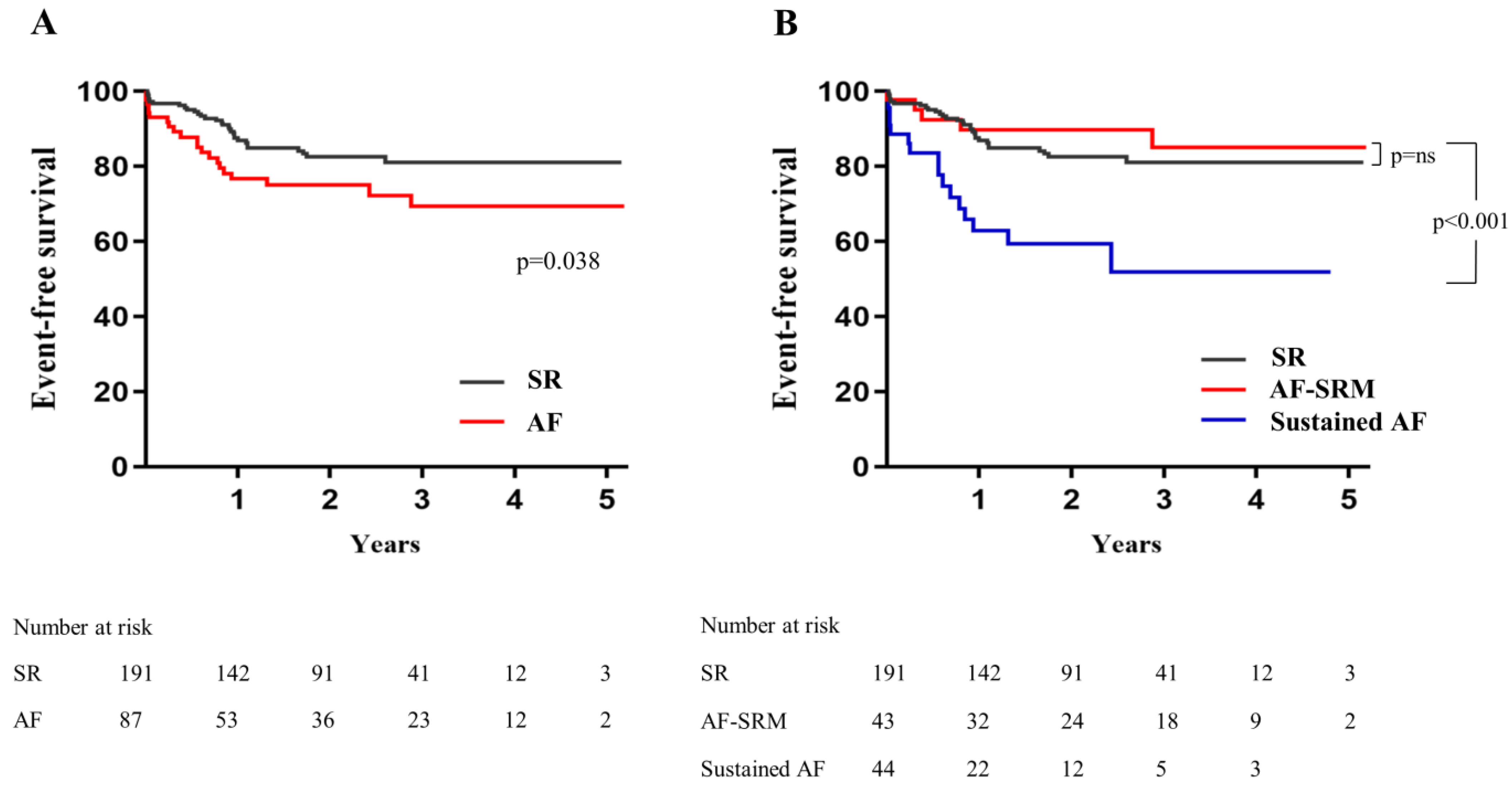
3.3. Clinical Outcomes
3.4. Impact of SR Maintenance in Pre-Existing AF and NOAF
3.5. Predictors for SR Maintenance
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kannel, W.B.; Abbott, R.D.; Savage, D.D.; McNamara, P.M. Epidemiologic features of chronic atrial fibrillation. N. Engl. J. Med. 1982, 306, 1018–1022. [Google Scholar] [CrossRef] [PubMed]
- Sannino, A.; Gargiulo, G.; Schiattarella, G.G.; Perrino, C.; Stabile, E.; Losi, M.A.; Galderisi, M.; Izzo, R.; de Simone, G.; Trimarco, B.; et al. A meta-analysis of the impact of pre-existing and new-onset atrial fibrillation on clinical outcomes in patients undergoing transcatheter aortic valve implantation. EuroIntervention 2016, 12, e1047–e1056. [Google Scholar] [CrossRef] [PubMed]
- Mack, M.J.; Leon, M.B.; Thourani, V.H.; Makkar, R.; Kodali, S.K.; Russo, M.; Kapadia, S.R.; Malaisrie, S.C.; Cohen, D.J.; Pibarot, P.; et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1695–1705. [Google Scholar] [CrossRef] [PubMed]
- Popma, J.J.; Deeb, G.M.; Yakubov, S.J.; Mumtaz, M.; Gada, H.; O’Hair, D.; Bajwa, T.; Heiser, J.C.; Merhi, W.; Kleiman, N.S.; et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N. Engl. J. Med. 2019, 380, 1706–1715. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Mojoli, M.; Urena, M.; Vahanian, A. Atrial fibrillation in patients undergoing transcatheter aortic valve implantation: Epidemiology, timing, predictors, and outcome. Eur. Heart J. 2017, 38, 1285–1293. [Google Scholar] [CrossRef] [PubMed]
- Mojoli, M.; Gersh, B.J.; Barioli, A.; Masiero, G.; Tellaroli, P.; D’Amico, G.; Tarantini, G. Impact of atrial fibrillation on outcomes of patients treated by transcatheter aortic valve implantation: A systematic review and meta-analysis. Am. Heart J. 2017, 192, 64–75. [Google Scholar] [CrossRef]
- Barbash, I.M.; Minha, S.; Ben-Dor, I.; Dvir, D.; Torguson, R.; Aly, M.; Bond, E.; Satler, L.F.; Pichard, A.D.; Waksman, R. Predictors and clinical implications of atrial fibrillation in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2015, 85, 468–477. [Google Scholar] [CrossRef]
- Biviano, A.B.; Nazif, T.; Dizon, J.; Garan, H.; Fleitman, J.; Hassan, D.; Kapadia, S.; Babaliaros, V.; Xu, K.; Parvataneni, R.; et al. Atrial fibrillation is associated with increased mortality in patients undergoing transcatheter aortic valve replacement: Insights from the placement of aortic transcatheter valve (partner) trial. Circ. Cardiovasc. Interv. 2016, 9, e002766. [Google Scholar] [CrossRef] [Green Version]
- Chopard, R.; Teiger, E.; Meneveau, N.; Chocron, S.; Gilard, M.; Laskar, M.; Eltchaninoff, H.; Iung, B.; Leprince, P.; Chevreul, K.; et al. Baseline characteristics and prognostic implications of pre-existing and new-onset atrial fibrillation after transcatheter aortic valve implantation: Results from the france-2 registry. JACC Cardiovas. Interv. 2015, 8, 1346–1355. [Google Scholar] [CrossRef] [Green Version]
- Nombela-Franco, L.; Webb, J.G.; de Jaegere, P.P.; Toggweiler, S.; Nuis, R.J.; Dager, A.E.; Amat-Santos, I.J.; Cheung, A.; Ye, J.; Binder, R.K.; et al. Timing, predictive factors, and prognostic value of cerebrovascular events in a large cohort of patients undergoing transcatheter aortic valve implantation. Circulation 2012, 126, 3041–3053. [Google Scholar] [CrossRef]
- Sannino, A.; Stoler, R.C.; Lima, B.; Szerlip, M.; Henry, A.C.; Vallabhan, R.; Kowal, R.C.; Brown, D.L.; Mack, M.J.; Grayburn, P.A. Frequency of and prognostic significance of atrial fibrillation in patients undergoing transcatheter aortic valve implantation. Am. J. Cardiol. 2016, 118, 1527–1532. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Mojoli, M.; Windecker, S.; Wendler, O.; Lefevre, T.; Saia, F.; Walther, T.; Rubino, P.; Bartorelli, A.L.; Napodano, M.; et al. Prevalence and impact of atrial fibrillation in patients with severe aortic stenosis undergoing transcatheter aortic valve replacement: An analysis from the source xt prospective multicenter registry. JACC Cardiovasc. Interv. 2016, 9, 937–946. [Google Scholar] [CrossRef] [PubMed]
- Yankelson, L.; Steinvil, A.; Gershovitz, L.; Leshem-Rubinow, E.; Furer, A.; Viskin, S.; Keren, G.; Banai, S.; Finkelstein, A. Atrial fibrillation, stroke, and mortality rates after transcatheter aortic valve implantation. Am. J. Cardiol. 2014, 114, 1861–1866. [Google Scholar] [CrossRef] [PubMed]
- Sherman, D.G.; Kim, S.G.; Boop, B.S.; Corley, S.D.; Dimarco, J.P.; Hart, R.G.; Haywood, L.J.; Hoyte, K.; Kaufman, E.S.; Kim, M.H.; et al. Occurrence and characteristics of stroke events in the atrial fibrillation follow-up investigation of sinus rhythm management (affirm) study. Arch. Intern. Med. 2005, 165, 1185–1191. [Google Scholar] [CrossRef] [Green Version]
- Corley, S.D.; Epstein, A.E.; DiMarco, J.P.; Domanski, M.J.; Geller, N.; Greene, H.L.; Josephson, R.A.; Kellen, J.C.; Klein, R.C.; Krahn, A.D.; et al. Relationships between sinus rhythm, treatment, and survival in the atrial fibrillation follow-up investigation of rhythm management (affirm) study. Circulation 2004, 109, 1509–1513. [Google Scholar]
- Marrouche, N.F.; Brachmann, J.; Andresen, D.; Siebels, J.; Boersma, L.; Jordaens, L.; Merkely, B.; Pokushalov, E.; Sanders, P.; Proff, J.; et al. Catheter ablation for atrial fibrillation with heart failure. N. Engl. J. Med. 2018, 378, 417–427. [Google Scholar] [CrossRef]
- Lee, J.K.; Klein, G.J.; Krahn, A.D.; Yee, R.; Zarnke, K.; Simpson, C.; Skanes, A.; Spindler, B. Rate-control versus conversion strategy in postoperative atrial fibrillation: A prospective, randomized pilot study. Am. Heart J. 2000, 140, 871–877. [Google Scholar] [CrossRef]
- Ferguson, T.B., Jr.; Dziuban, S.W., Jr.; Edwards, F.H.; Eiken, M.C.; Shroyer, A.L.; Pairolero, P.C.; Anderson, R.P.; Grover, F.L. The sts national database: Current changes and challenges for the new millennium. Committee to establish a national database in cardiothoracic surgery, the society of thoracic surgeons. Ann. Thorac. Surg. 2000, 69, 680–691. [Google Scholar] [CrossRef]
- Nashef, S.A.; Roques, F.; Michel, P.; Gauducheau, E.; Lemeshow, S.; Salamon, R. European system for cardiac operative risk evaluation (euroscore). Eur. J. Cardiothorac. Surg. 1999, 16, 9–13. [Google Scholar] [CrossRef]
- Schulman, S.; Kearon, C.; The Subcommittee on Control of Anticoagulation of the Scientific; Standardization Committee of the International Society on Thrombosis and Haemostasis. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef]
- Dunnett, C.W. A multiple comparisons procedure for comparing several treatments with a control. J. Am. Stat. Assoc. 1955, 50, 1096–1121. [Google Scholar] [CrossRef]
- Geisler, D.; Rudzinski, P.N.; Hasan, W.; Andreas, M.; Hasimbegovic, E.; Adlbrecht, C.; Winkler, B.; Weiss, G.; Strouhal, A.; Dell-Karth, G.; et al. Identifying patients without a survival benefit following transfemoral and transapical transcatheter aortic valve replacement. J. Clin. Med. 2021, 10, 4911. [Google Scholar] [CrossRef]
- Khan, M.Z.; Zahid, S.; Khan, M.U.; Kichloo, A.; Jamal, S.; Minhas, A.M.K.; Ullah, W.; Sattar, Y.; Mir, T.; Balla, S.; et al. Outcomes of transcatheter aortic valve replacement in patiens with and without atrial fibrillation: Insights from national inpatient sample. Expert. Rev. Cardiovasc. Ther. 2021, 19, 939–946. [Google Scholar] [CrossRef] [PubMed]
- Lip, G.Y.; Windecker, S.; Huber, K.; Kirchhof, P.; Marin, F.; Ten Berg, J.M.; Haeusler, K.G.; Boriani, G.; Capodanno, D.; Gilard, M.; et al. Management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous coronary or valve interventions: A joint consensus document of the european society of cardiology working group on thrombosis, european heart rhythm association (ehra), european association of percutaneous cardiovascular interventions (eapci) and european association of acute cardiac care (acca) endorsed by the heart rhythm society (hrs) and asia-pacific heart rhythm society (aphrs). Eur. Heart J. 2014, 35, 3155–3179. [Google Scholar] [PubMed] [Green Version]
- Vora, A.N.; Dai, D.; Matsuoka, R.; Harrison, J.K.; Hughes, G.C.T.; Sherwood, M.W.; Piccini, J.P.; Bhardwaj, B.; Lopes, R.D.; Cohen, D.; et al. Incidence, management, and associated clinical outcomes of new-onset atrial fibrillation following transcatheter aortic valve replacement: An analysis from the sts/acc tvt registry. JACC Cardiovasc. Interv. 2018, 11, 1746–1756. [Google Scholar] [CrossRef]
- Seeger, J.; Gonska, B.; Rodewald, C.; Rottbauer, W.; Wohrle, J. Apixaban in patients with atrial fibrillation after transfemoral aortic valve replacement. JACC Cardiovasc. Interv. 2017, 10, 66–74. [Google Scholar] [CrossRef]
- Van Mieghem, N.M.; Unverdorben, M.; Hengstenberg, C.; Mollmann, H.; Mehran, R.; Lopez-Otero, D.; Nombela-Franco, L.; Moreno, R.; Nordbeck, P.; Thiele, H.; et al. Edoxaban versus vitamin K antagonist for atrial fibrillation after TAVR. N. Engl. J. Med. 2021, 385, 2150–2160. [Google Scholar] [CrossRef]
- Megaly, M.; Garcia, S.; Anzia, L.E.; Morley, P.; Garberich, R.; Gornick, C.C.; Lesser, J.; Sorajja, P.; Gossl, M.; Sengupta, J. Detection of atrial fibrillation and atrial flutter by pacemaker device interrogation after transcatheter aortic valve replacement (tavr): Implications for management. J. Invasive Cardiol. 2019, 31, E177–E183. [Google Scholar]
- Wyse, D.G.; Waldo, A.L.; DiMarco, J.P.; Domanski, M.J.; Rosenberg, Y.; Schron, E.B.; Kellen, J.C.; Greene, H.L.; Mickel, M.C.; Dalquist, J.E.; et al. A comparison of rate control and rhythm control in patients with atrial fibrillation. N. Engl. J. Med. 2002, 347, 1825–1833. [Google Scholar]
- Packer, D.L.; Mark, D.B.; Robb, R.A.; Monahan, K.H.; Bahnson, T.D.; Poole, J.E.; Noseworthy, P.A.; Rosenberg, Y.D.; Jeffries, N.; Mitchell, L.B.; et al. Effect of catheter ablation vs antiarrhythmic drug therapy on mortality, stroke, bleeding, and cardiac arrest among patients with atrial fibrillation: The cabana randomized clinical trial. JAMA 2019, 321, 1261–1274. [Google Scholar] [CrossRef]
- Kelly, J.P.; DeVore, A.D.; Wu, J.; Hammill, B.G.; Sharma, A.; Cooper, L.B.; Felker, G.M.; Piccini, J.P.; Allen, L.A.; Heidenreich, P.A.; et al. Rhythm control versus rate control in patients with atrial fibrillation and heart failure with preserved ejection fraction: Insights from get with the guidelines-heart failure. J. Am. Heart Assoc. 2019, 8, e011560. [Google Scholar] [CrossRef] [PubMed]
- Shahim, B.; Malaisrie, S.C.; George, I.; Thourani, V.H.; Biviano, A.B.; Russo, M.; Brown, D.L.; Babaliaros, V.; Guyton, R.A.; Kodali, S.K.; et al. Postoperative atrial fibrillation or flutter following transcatheter or surgical aortic valve replacement. JACC Cardiovasc. Interv. 2021, 14, 1565–1574. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| SR (n = 191) | AF-SRM (n = 43) | Sustained AF (n = 44) | p | |
|---|---|---|---|---|
| Age, years | 78.4 ± 6.9 | 80.1 ± 5.9 | 79.3 ± 6.5 | 0.249 |
| Male sex | 89 (46.5%) | 21 (48.8%) | 18 (40.9%) | 0.731 |
| BMI, kg/m2 | 24.4 ± 3.9 | 24.3 ± 4.1 | 24.2 ± 3.9 | 0.707 |
| Prosthetic valve type | 0.024 | |||
| Self-expandable | 76 (39.8%) | 24 (55.8%) | 12 (27.3%) | |
| Balloon-expandable | 115 (60.2%) | 19 (44.2%) | 32 (72.7%) | |
| Comorbidities, n (%) | ||||
| Hypertension | 133 (69.6%) | 32 (74.4%) | 34 (77.3%) | 0.541 |
| Diabetes | 58 (30.3%) | 15 (34.9%) | 13 (29.5%) | 0.826 |
| COPD | 56 (29.3%) | 12 (27.9%) | 17 (36.4%) | 0.616 |
| Prior stroke | 24 (12.5%) | 8 (18.6%) | 9 (20.5%) | 0.305 |
| PAD | 32 (16.7%) | 6 (14.0%) | 9 (20.5%) | 0.717 |
| Prior MI | 11 (5.8%) | 6 (14.0%) | 7 (15.9%) | 0.039 |
| Obstructive CAD | 74 (38.7%) | 19 (44.2%) | 21 (47.7%) | 0.495 |
| CKD | 21 (10.9%) | 8 (18.6%) | 13 (29.5%) | 0.006 |
| Creatinine, mg/dL | 1.3 ± 1.7 | 1.3 ± 0.9 | 1.5 ± 1.3 | 0.638 |
| CHA2DS2-Vasc score | 4.0 ± 1.3 | 4.4 ± 1.6 | 4.5 ± 1.6 | 0.018 |
| AVA, cm2 | 0.73 ± 0.17 | 0.69 ± 0.19 | 0.70 ± 0.19 | 0.356 |
| AV Vmax, m/s | 4.6 ± 0.6 | 4.8 ± 0.7 | 4.4 ± 0.7 | 0.093 |
| LA diameter, mm | 43.4 ± 5.4 | 45.3 ± 6.9 | 49.2 ± 6.9 | <0.001 |
| LAVI, mL/m2 | 46.3 ± 17.4 | 52.1 ± 24.6 | 65.4 ± 18.9 | <0.001 |
| LVEF, % | 60.9 ± 9.9 | 57.1 ± 13.0 | 55.4 ± 11.9 | 0.001 |
| STS score | 8.1 ± 6.5 | 9.7 ± 8.9 | 9.3 ± 6.4 | 0.171 |
| DC cardioversion, n (%) | 3 (7.0%) | 4 (9.1%) | 0.901 | |
| Medications after TAVR, n (%) | ||||
| Single antiplatelet | 12 (6.3%) | 1 (2.3%) | 0 | 0.150 |
| Dual antiplatelet | 150 (78.5%) | 18 (41.9%) | 5 (11.4%) | <0.001 |
| Single OAC | 23 (12.0%) | 19 (44.2%) | 25 (56.8%) | <0.001 |
| Antiplatelet + OAC | 2 (1.0%) | 5 (11.6%) | 12 (27.3%) | <0.001 |
| Beta-blocker | 53 (27.7%) | 7 (16.3%) | 10 (22.7%) | 0.270 |
| RAS blocker | 84 (44.0%) | 15 (34.9%) | 17 (38.6%) | 0.529 |
| Antiarrhythmic drug | 16 (37.2%) | 13 (29.5%) | 0.364 |
| SR (n = 132) | AF-SRM (n = 33) | Sustained AF (n = 34) | p | |
|---|---|---|---|---|
| LVEF, % | 62.6 ± 5.9 | 62.0 ± 5.2 | 56.1 ± 8.3 | <0.001 |
| ∆LVEF, % | 2.6 ± 9.2 | 6.1 ± 11.8 | 2.0 ± 11.6 | 0.381 |
| LAVI, mL/m2 | 39.4 ± 13.6 | 43.4 ± 23.2 | 62.6 ± 17.1 | <0.001 |
| ∆LAVI, mL/m2 | −6.3 ± 11.7 | −10.1 ± 16.0 | −1.2 ± 16.6 | 0.233 |
| RVSP, mmHg | 30.7 ± 8.8 | 28.7 ± 7.3 | 38.0 ± 15.3 | 0.004 |
| ∆RVSP, mmHg | −4.2 ± 11.8 | −9.6 ± 12.3 | −5.8 ± 14.2 | 0.221 |
| AV Vmax, m/s | 2.4 ± 0.4 | 2.5 ± 0.7 | 2.3 ± 0.5 | 0.511 |
| AVA, cm2 | 1.6 ± 0.4 | 1.7 ± 0.5 | 1.6 ± 0.5 | 0.694 |
| ≥Moderate PVL, n (%) | 11 (8.3%) | 3 (9.4%) | 0 | 0.205 |
| SR | AF-SRM | Sustained AF | HR * | 95% CI | p | |
|---|---|---|---|---|---|---|
| Death, stroke or rehospitalization | 30 (15.7%) | 5 (11.6%) | 16 (36.4%) | 4.449 | 1.614–12.270 | 0.004 |
| All-cause death | 20 (10.5%) | 4 (9.3%) | 7 (15.9%) | 1.918 | 0.561–6.561 | 0.299 |
| Cardiovascular death | 5 (2.6%) | 2 (4.7%) | 5 (11.4%) | 2.615 | 0.506–13.490 | 0.251 |
| HF rehospitalization | 11 (5.8%) | 0 | 10 (22.7%) | <0.001 | ||
| Stroke | 4 (2.1%) | 1 (2.3%) | 0 | 0.616 | ||
| Major bleeding | 12 (6.3%) | 2 (4.7%) | 5 (11.4%) | 3.095 | 0.592–16.17 | 0.181 |
| Variable | Crude HR | 95% CI | p | Adjusted HR | 95% CI | p |
|---|---|---|---|---|---|---|
| Age | 1.073 | 1.031–1.122 | 0.002 | 1.098 | 1.041–1.158 | <0.001 |
| Male sex | 1.205 | 0.693–2.071 | 0.525 | 1.124 | 0.545–2.317 | 0.750 |
| LVEF < 50% | 1.613 | 0.814–3.221 | 0.175 | 1.701 | 0.704–4.108 | 0.237 |
| LAVI | 1.021 | 1.012–1.034 | 0.002 | 1.011 | 0.996–1.027 | 0.142 |
| Hypertension | 2.162 | 1.014–4.596 | 0.046 | 1.811 | 0.717–4.575 | 0.208 |
| Diabetes | 1.834 | 0.922–3.661 | 0.086 | |||
| Stroke | 0.851 | 0.386–1.885 | 0.685 | |||
| Obstructive CAD | 1.819 | 1.054–3.171 | 0.033 | 1.589 | 0.805–3.135 | 0.181 |
| CKD | 3.642 | 2.016–6.595 | <0.001 | 3.873 | 1.759–8.530 | <0.001 |
| Prior MI | 1.568 | 0.671–3.684 | 0.300 | 0.749 | 0.239–2.342 | 0.619 |
| CHA2DS2-Vasc score | 1.154 | 0.963–1.382 | 0.141 | |||
| Use of balloon-expandable device | 1.033 | 0.591–1.817 | 0.917 | 0.962 | 0.471–1.965 | 0.916 |
| Anticoagulation | 1.021 | 0.565–1.838 | 0.960 | 0.381 | 0.107–1.347 | 0.134 |
| Any AF | 1.809 | 1.032–3.163 | 0.038 | 0.343 | 0.088–1.341 | 0.124 |
| SR maintenance | 0.292 | 0.162–0.523 | <0.001 | 0.081 | 0.018–0.368 | 0.001 |
| Variable | Crude HR | 95% CI | p | Adjusted HR | 95% CI | p |
|---|---|---|---|---|---|---|
| Age | 1.044 | 0.975–1.117 | 0.312 | 1.078 | 0.988–1.176 | 0.090 |
| Male sex | 1.442 | 0.611–3.393 | 0.407 | 1.913 | 0.593–6.163 | 0.277 |
| LVEF < 50% | 1.303 | 0.504–3.376 | 0.593 | 1.275 | 0.302–5.378 | 0.739 |
| LAVI | 1.013 | 0.991–1.032 | 0.360 | 1.000 | 0.971–1.029 | 0.981 |
| Hypertension | 3.166 | 0.735–13.606 | 0.123 | |||
| Diabetes | 1.202 | 0.472–3.114 | 0.702 | |||
| Stroke | 0.740 | 0.221–2.513 | 0.625 | |||
| Obstructive CAD | 1.425 | 0.623–3.497 | 0.383 | |||
| CKD | 1.951 | 0.780–4.864 | 0.151 | 1.543 | 0.410–5.802 | 0.520 |
| Prior MI | 1.764 | 0.642–4.806 | 0.271 | 1.102 | 0.238–5.092 | 0.900 |
| CHA2DS2-Vasc score | 1.101 | 0.851–1.423 | 0.474 | |||
| Use of balloon-expandable device | 0.828 | 0.359–1.941 | 0.654 | 1.128 | 0.324–3.920 | 0.849 |
| Anticoagulation | 0.685 | 0.284–1.650 | 0.395 | 0.104 | 0.015–0.720 | 0.021 |
| Persistent AF | 1.392 | 0.571–3.413 | 0.466 | 0.390 | 0.086–1.760 | 0.221 |
| Pre-existing AF* | 0.893 | 0.375–2.118 | 0.792 | 1.909 | 0.434–8.389 | 0.391 |
| SR maintenance | 0.220 | 0.081–0.626 | 0.004 | 0.023 | 0.003–0.183 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Choi, Y.; Hwang, B.-H.; Oh, G.-C.; Kim, J.J.; Choo, E.; Kim, M.-C.; Kim, J.; Jung, H.O.; Youn, H.-J.; Chung, W.-S.; et al. Long-Term Maintenance of Sinus Rhythm Is Associated with Favorable Echocardiographic Remodeling and Improved Clinical Outcomes after Transcatheter Aortic Valve Replacement. J. Clin. Med. 2022, 11, 1330. https://doi.org/10.3390/jcm11051330
Choi Y, Hwang B-H, Oh G-C, Kim JJ, Choo E, Kim M-C, Kim J, Jung HO, Youn H-J, Chung W-S, et al. Long-Term Maintenance of Sinus Rhythm Is Associated with Favorable Echocardiographic Remodeling and Improved Clinical Outcomes after Transcatheter Aortic Valve Replacement. Journal of Clinical Medicine. 2022; 11(5):1330. https://doi.org/10.3390/jcm11051330
Chicago/Turabian StyleChoi, Young, Byung-Hee Hwang, Gyu-Chul Oh, Jin Jin Kim, Eunho Choo, Min-Chul Kim, Juhan Kim, Hae Ok Jung, Ho-Joong Youn, Wook-Sung Chung, and et al. 2022. "Long-Term Maintenance of Sinus Rhythm Is Associated with Favorable Echocardiographic Remodeling and Improved Clinical Outcomes after Transcatheter Aortic Valve Replacement" Journal of Clinical Medicine 11, no. 5: 1330. https://doi.org/10.3390/jcm11051330