
Is Oxidative Stress an Emerging Player in the Thrombosis of Patients with Anti-Phosphatidylethanolamine Autoantibodies?

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. aPE Detection
2.2.1. In-House ELISA with PE-Only Coating
2.2.2. Commercial aPE ELISA with PE and B2GPI Coating
2.3. Adsorption Experiments on B2GPI Coated Plate
2.4. TBARs Dosage
2.5. Statistical Analysis
3. Results
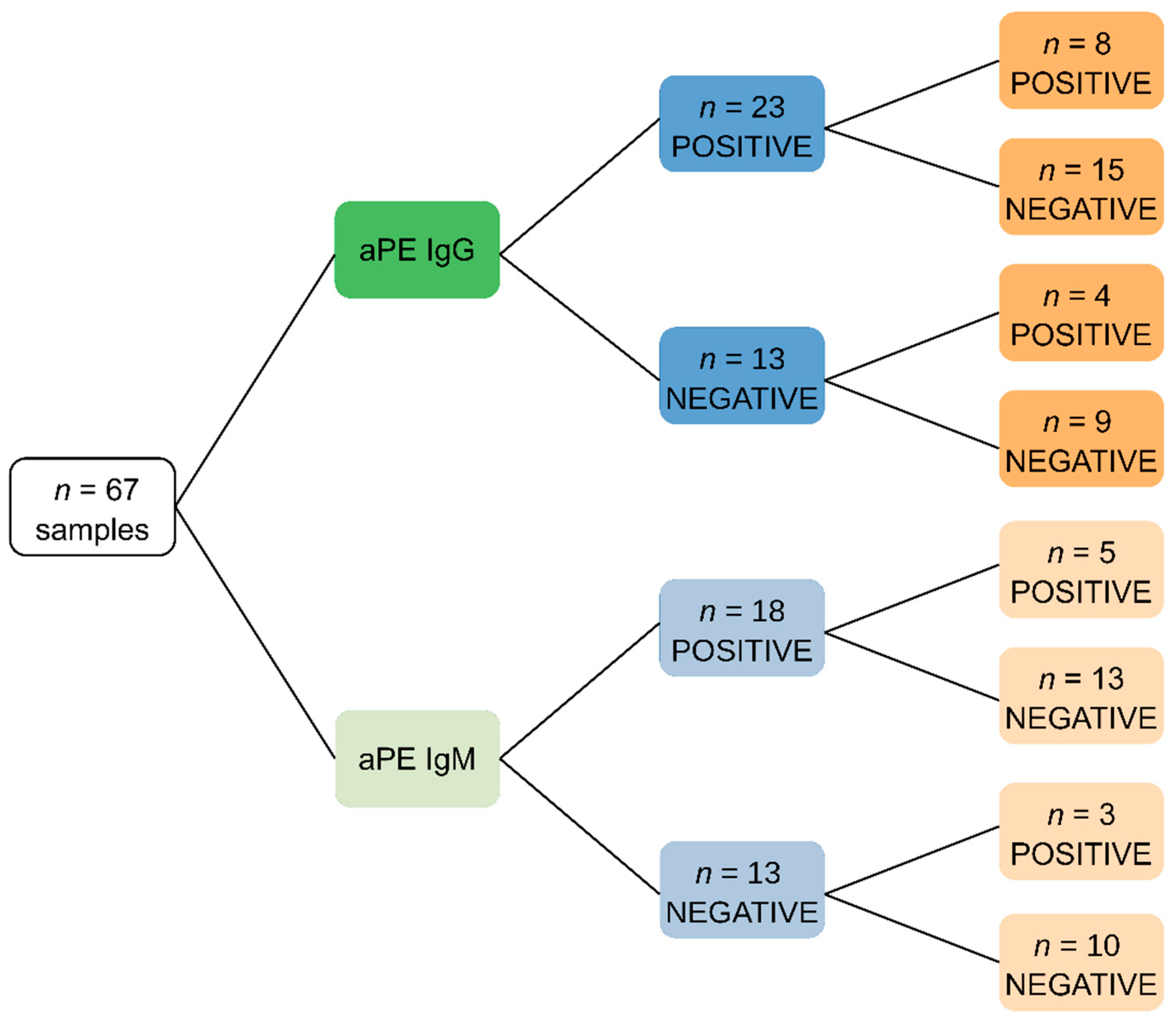
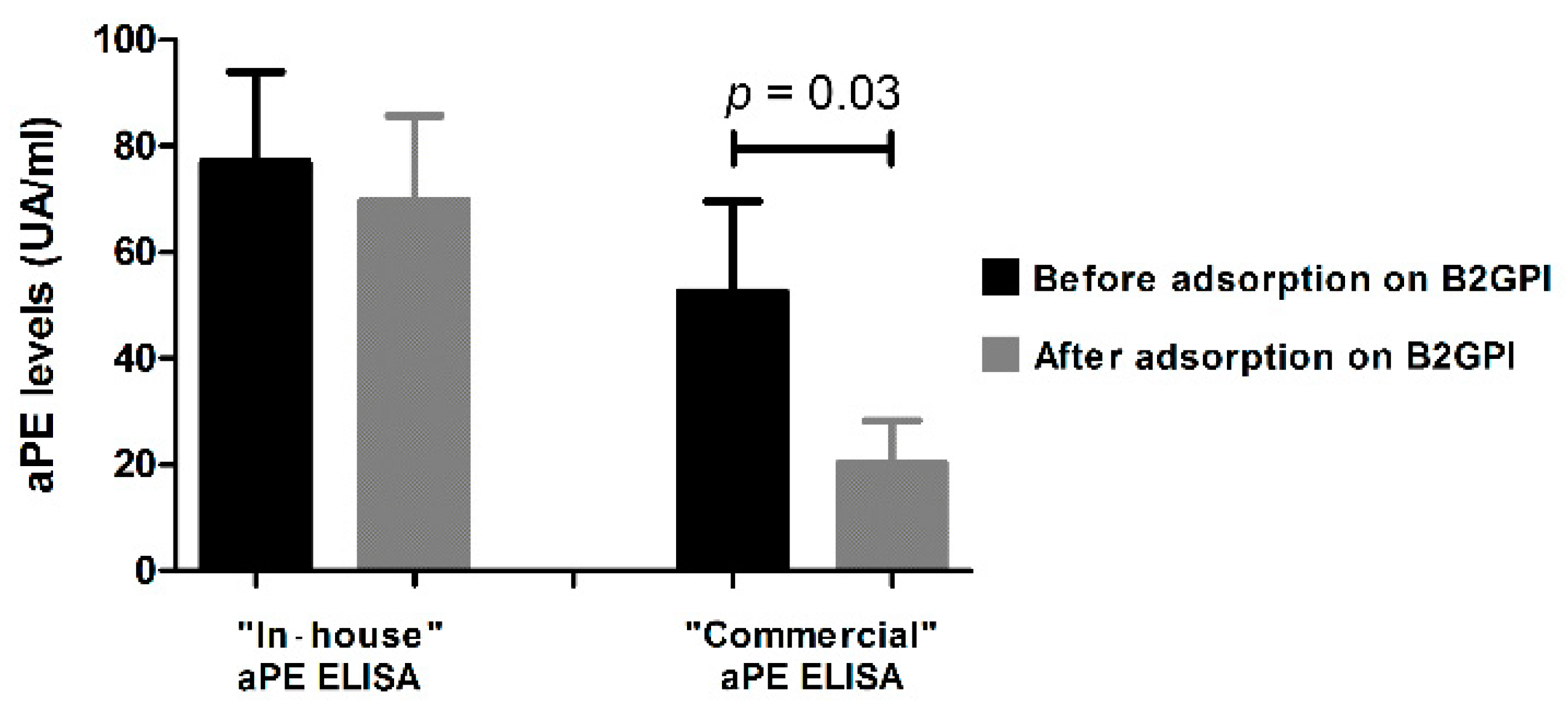
3.1. Specific Detection of aPE
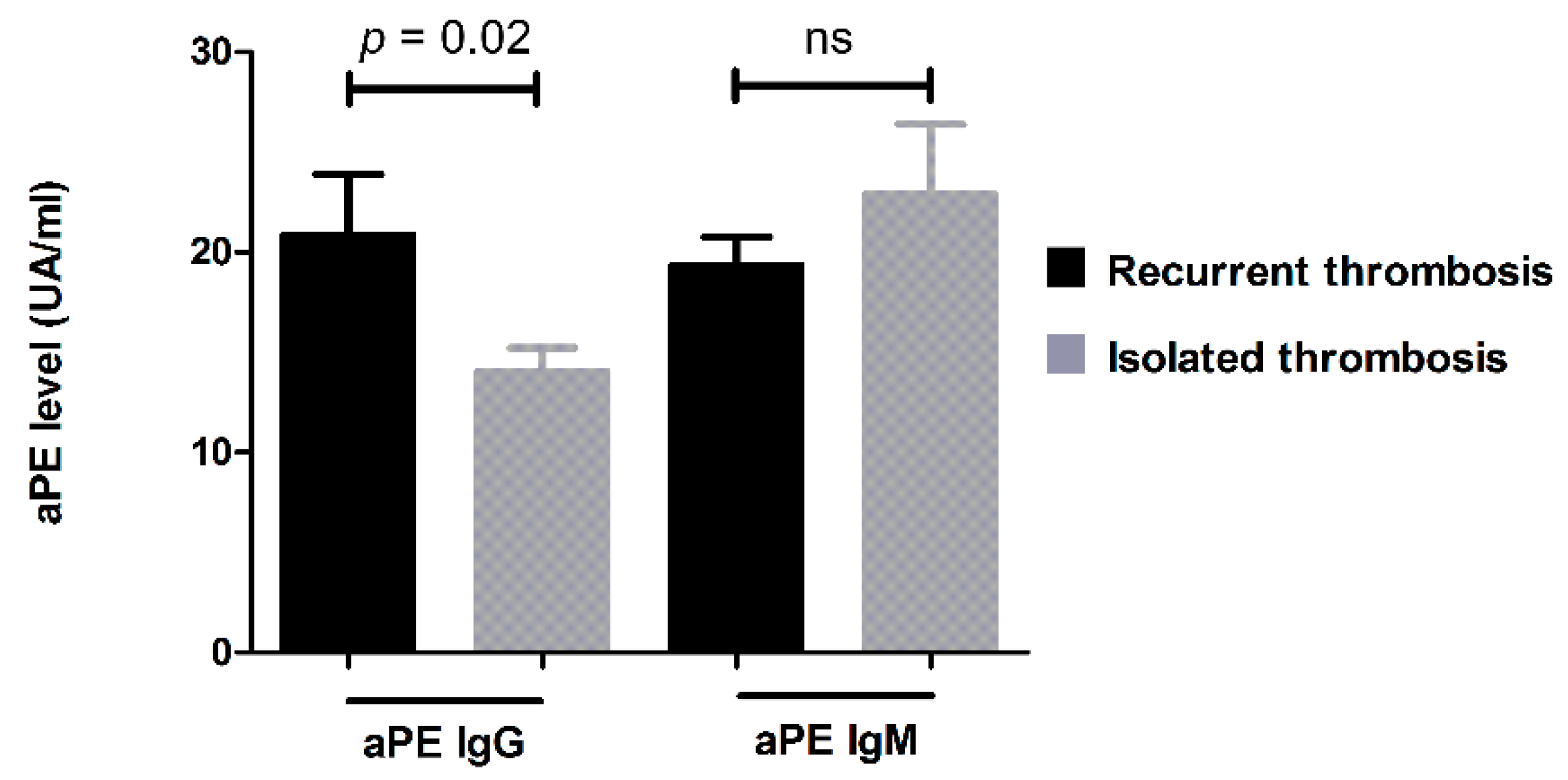
3.2. Retrospective Clinical Study
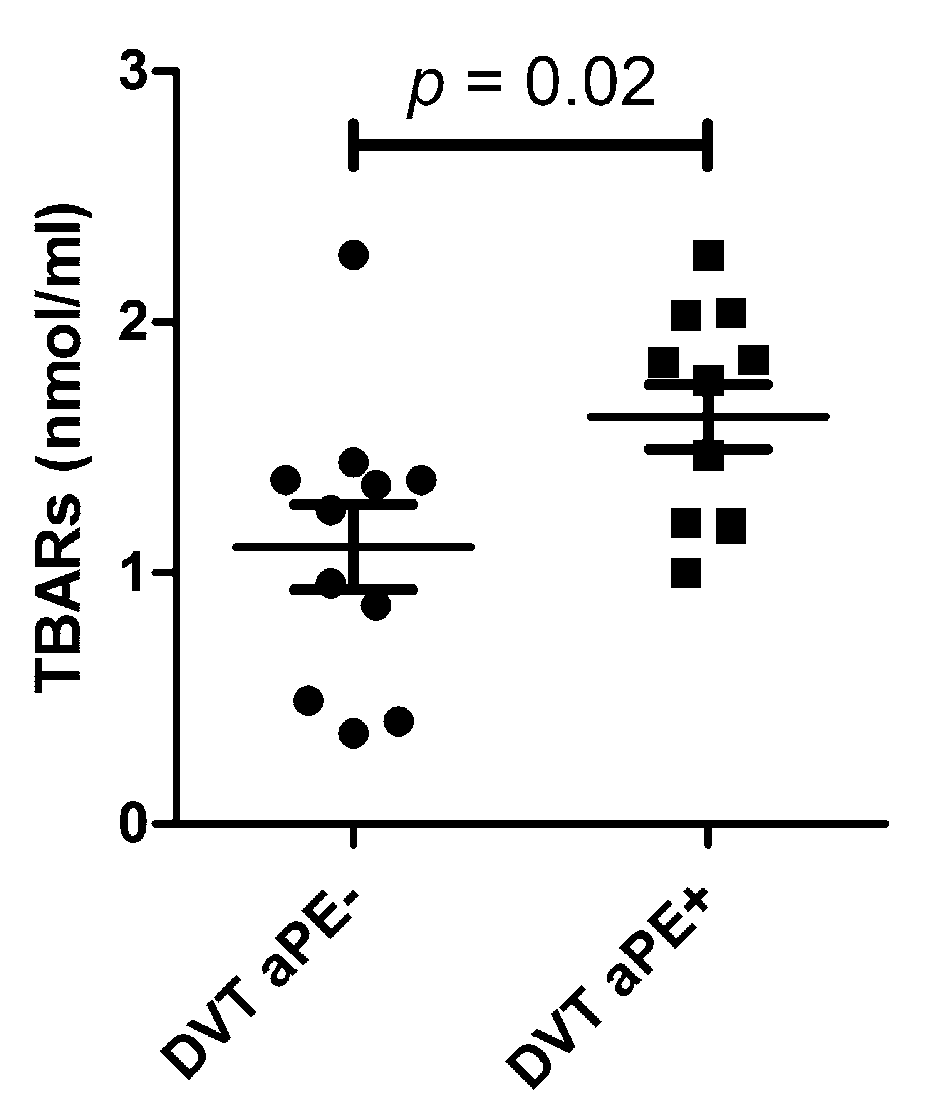
3.3. Association between aPEs and Oxidative Stress in Patients with Unexplained DVT
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Langley, K.E.; Kennedy, E.P. Energetics of rapid transmembrane movement and of compositional asymmetry of phosphatidylethanolamine in membranes of Bacillus megaterium. Proc. Natl. Acad. Sci. USA 1979, 76, 6245–6249. [Google Scholar] [CrossRef] [Green Version]
- Li, Z.; Wells, C.W.; North, P.E.; Kumar, S.; Duris, C.B.; McIntyre, J.A.; Zhao, M. Phosphatidylethanolamine at the Luminal Endothelial Surface—Implications for Hemostasis and Thrombotic Autoimmunity. Clin. Appl. Thromb. Hemost 2011, 17, 158–163. [Google Scholar] [CrossRef] [Green Version]
- Zachowski, A. Phospholipids in animal eukaryotic membranes: Transverse asymmetry and movement. Biochem. J. 1993, 294 Pt 1, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zwaal, R.F.; Roelofsen, B.; Comfurius, P.; van Deenen, L. Organization of phospholipids in human red cell membranes as detected by the action of various purified phospholipases. Biochim. Biophys. Acta 1975, 406, 83–96. [Google Scholar] [CrossRef] [Green Version]
- Deeba, F.; Tahseen, H.N.; Sharad, K.S.; Ahmad, N.; Akhtar, S.; Saleemuddin, M.; Mohammad, O. Phospholipid diversity: Correlation with membrane–membrane fusion events. Biochim. Biophys. Acta 2005, 1669, 170–181. [Google Scholar] [CrossRef] [Green Version]
- Verkleij, A.J.; Leunissen-Bijvelt, J.; de Kruijff, B.; Hope, M.; Cullis, P.R. Non-Bilayer Structures in Membrane Fusion. Ciba Found. Symp. 1984, 103, 45–59. [Google Scholar] [CrossRef] [PubMed]
- Emoto, K.; Kobayashi, T.; Yamaji, A.; Aizawa, H.; Yahara, I.; Inoue, K.; Umeda, M. Redistribution of phosphatidylethanolamine at the cleavage furrow of dividing cells during cytokinesis. Proc. Natl. Acad. Sci. USA 1996, 93, 12867–12872. [Google Scholar] [CrossRef] [Green Version]
- Hailey, D.W.; Rambold, A.S.; Satpute-Krishnan, P.; Mitra, K.; Sougrat, R.; Kim, P.K.; Lippincott-Schwartz, J. Mitochondria Supply Membranes for Autophagosome Biogenesis during Starvation. Cell 2010, 141, 656–667. [Google Scholar] [CrossRef] [Green Version]
- Nebauer, R.; Rosenberger, S.; Daum, G. Phosphatidylethanolamine, a Limiting Factor of Autophagy in Yeast Strains Bearing a Defect in the Carboxypeptidase Y Pathway of Vacuolar Targeting. J. Biol. Chem. 2007, 282, 16736–16743. [Google Scholar] [CrossRef] [Green Version]
- Sanmarco, M.; Alessi, M.-C.; Harle, J.R.; Sapin, C.; Aillaud, M.-F.; Gentile, S.; Juhan-Vague, I.; Weiller, P.-J. Antibodies to phosphatidylethanolamine as the only antiphospholipid antibodies found in patients with unexplained thromboses. Thromb. Haemost. 2001, 85, 800–805. [Google Scholar] [CrossRef]
- Sanmarco, M.; Gayet, S.; Alessi, M.-C.; Audrain, M.; de Maistre, E.; Gris, J.-C.; de Groot, P.G.; Hachulla, E.; Harlé, J.-R.; Sié, P.; et al. Antiphosphatidylethanolamine antibodies are associated with an increased odds ratio for thrombosis. A Multicenter Study with the Participation of the European Forum on Antiphospholipid Antibodies. Thromb. Haemost. 2007, 97, 949–954. [Google Scholar] [CrossRef] [PubMed]
- Hou, S.; Fölsch, H.; Ke, K.; Mills, J.C.; Ramsey-Goldman, R.; Zhao, M. Early endosome as a pathogenic target for antiphosphatidylethanolamine antibodies. Proc. Natl. Acad. Sci. USA 2017, 114, 13798–13803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Qiao, J.; Arthur, J.F.; Gardiner, E.E.; Andrews, R.K.; Zeng, L.; Xu, K. Regulation of platelet activation and thrombus formation by reactive oxygen species. Redox Biol. 2018, 14, 126–130. [Google Scholar] [CrossRef]
- Gutmann, C.; Siow, R.; Gwozdz, A.M.; Saha, P.; Smith, A. Reactive Oxygen Species in Venous Thrombosis. Int. J. Mol. Sci. 2020, 21, 1918. [Google Scholar] [CrossRef] [Green Version]
- Mihara, M.; Uchiyama, M. Effects of antioxidants on the TBA reaction of various rat liver homogenates. Biochem. Med. 1983, 30, 131–134. [Google Scholar] [CrossRef]
- Yoshikawa, T.; Tanaka, H.; Kondo, M. The increase of lipid peroxidation in rat adjuvant arthritis and its inhibition by superoxide dismutase. Biochem. Med. 1985, 33, 320–326. [Google Scholar] [CrossRef]
- Jammes, Y.; Steinberg, J.G.; Mambrini, O.; Brégeon, F.; Delliaux, S. Chronic fatigue syndrome: Assessment of increased oxidative stress and altered muscle excitability in response to incremental exercise. J. Intern. Med. 2005, 257, 299–310. [Google Scholar] [CrossRef]
- Gris, J.C.; Quéré, I.; Sanmarco, M.; Boutiere, B.; Mercier, E.; Amiral, J.; Hubert, A.M.; Ripart-Neveu, S.; Hoffet, M.; Tailland, M.L.; et al. Antiphospholipid and antiprotein syndromes in non-thrombotic, non-autoimmune women with unexplained recurrent primary early foetal loss. The Nîmes Obstetricians and Haematologists Study--NOHA. Thromb. Haemost. 2000, 84, 228–236. [Google Scholar] [PubMed]
- Sanmarco, M.; Bardin, N.; Camoin, L.; Beziane, A.; Gamerre, M.; Porcu, G.; Dignat-George, F. Antigenic Profile, Prevalence, and Clinical Significance of Antiphospholipid Antibodies in Women Referred for in Vitro Fertilization. Ann. N. Y. Acad. Sci. 2007, 1108, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Esmon, N.L.; Safa, O.; Smirnov, M.D.; Esmon, C.T. Antiphospholipid Antibodies and the Protein C Pathway. J. Autoimmun. 2000, 15, 221–225. [Google Scholar] [CrossRef] [PubMed]
- Smirnov, M.D.; Safa, O.; Regan, L.; Mather, T.; Stearns-Kurosawa, D.J.; Kurosawa, S.; Rezaie, A.R.; Esmon, N.L.; Esmon, C.T. A Chimeric Protein C Containing the Prothrombin Gla Domain Exhibits Increased Anticoagulant Activity and Altered Phospholipid Specificity. J. Biol. Chem. 1998, 273, 9031–9040. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Smirnov, M.D.; Esmon, C.T. Phosphatidylethanolamine incorporation into vesicles selectively enhances factor Va inactivation by activated protein C. J. Biol. Chem. 1994, 269, 816–819. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical or Biological Parameters | Number of Positive Patient for Each Parameter | Size of Population (Nb of Patients) | Prevalence |
|---|---|---|---|
| Clinical events | |||
| -Thrombosis: | 291 | 1131 | 0.257 |
| -Arterial thrombosis | 143 | 291 | 0.491 |
| -Venous thrombosis | 181 | 291 | 0.622 |
| -Cerebral stroke | 92 | 291 | 0.316 |
| -Pulmonary embolism | 76 | 291 | 0.261 |
| -Myocardial infarction | 12 | 291 | 0.041 |
| -Recurrent fetal losses | 178 | 848 | 0.21 |
| -Obstetrical complications | 30 | 848 | 0.035 |
| -Infertility | 25 | 848 | 0.029 |
| Biological data | |||
| aPE IgG and/or IgM | 234 | 1131 | 0.207 |
| aPE IgG | 209 | 1131 | 0.185 |
| aPE IgM | 38 | 1131 | 0.034 |
| aB2GPI IgG | 44 | 1131 | 0.039 |
| aB2GPI IgM | 41 | 1131 | 0.036 |
| aCL IgG | 60 | 1131 | 0.053 |
| aCL IgM | 84 | 1131 | 0.074 |
| LA | 66 | 968 | 0.068 |
| aPE IgG and/or IgM | aPE IgG | aPE IgM | |||||||
|---|---|---|---|---|---|---|---|---|---|
| − Nb (%) | + Nb (%) | p value | − Nb (%) | + Nb (%) | p value | − Nb (%) | + Nb (%) | p value | |
| Thrombosis | 220 (24.5%) | 71 (30.3%) | 0.06 | 226 (24.5%) | 65 (31.1%) | 0.04 | 281 (25.7%) | 10 (26.3%) | 0.93 |
| Recurrent pregnancy loss | 139 (20.8%) | 39 (21.6%) | 0.83 | 146 (21.2%) | 32 (20.1%) | 0.76 | 169 (20.7%) | 9 (28.1%) | 0.31 |
| Obstetrical complications | 27 (4.1%) | 3 (1.7%) | 0.12 | 27 (3.9%) | 3 (1.9%) | 0.21 | 30 (3.7%) | 0 (0%) | 0.62 |
| Infertility | 16 (2.4%) | 9 (5.0%) | 0.06 | 17 (2.5%) | 8 (5.0%) | 0.11 | 23 (2.8%) | 2 (6.3%) | 0.24 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Heim, X.; Bertin, D.; Resseguier, N.; Beziane, A.; Metral, A.; Brodovitch, A.; Guieu, R.; Steinberg, J.-G.; Blot-Chabaud, M.; Morange, P.-E.; et al. Is Oxidative Stress an Emerging Player in the Thrombosis of Patients with Anti-Phosphatidylethanolamine Autoantibodies? J. Clin. Med. 2022, 11, 1297. https://doi.org/10.3390/jcm11051297
Heim X, Bertin D, Resseguier N, Beziane A, Metral A, Brodovitch A, Guieu R, Steinberg J-G, Blot-Chabaud M, Morange P-E, et al. Is Oxidative Stress an Emerging Player in the Thrombosis of Patients with Anti-Phosphatidylethanolamine Autoantibodies? Journal of Clinical Medicine. 2022; 11(5):1297. https://doi.org/10.3390/jcm11051297
Chicago/Turabian StyleHeim, Xavier, Daniel Bertin, Noémie Resseguier, Abdelouahab Beziane, Audrey Metral, Alexandre Brodovitch, Régis Guieu, Jean-Guillaume Steinberg, Marcel Blot-Chabaud, Pierre-Emmanuel Morange, and et al. 2022. "Is Oxidative Stress an Emerging Player in the Thrombosis of Patients with Anti-Phosphatidylethanolamine Autoantibodies?" Journal of Clinical Medicine 11, no. 5: 1297. https://doi.org/10.3390/jcm11051297