
The Combination of Lymph Node Transfer and Excisional Procedures in Bilateral Lower Extremity Lymphedema: Clinical Outcomes and Quality of Life Assessment with Long-Term Follow-Up

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
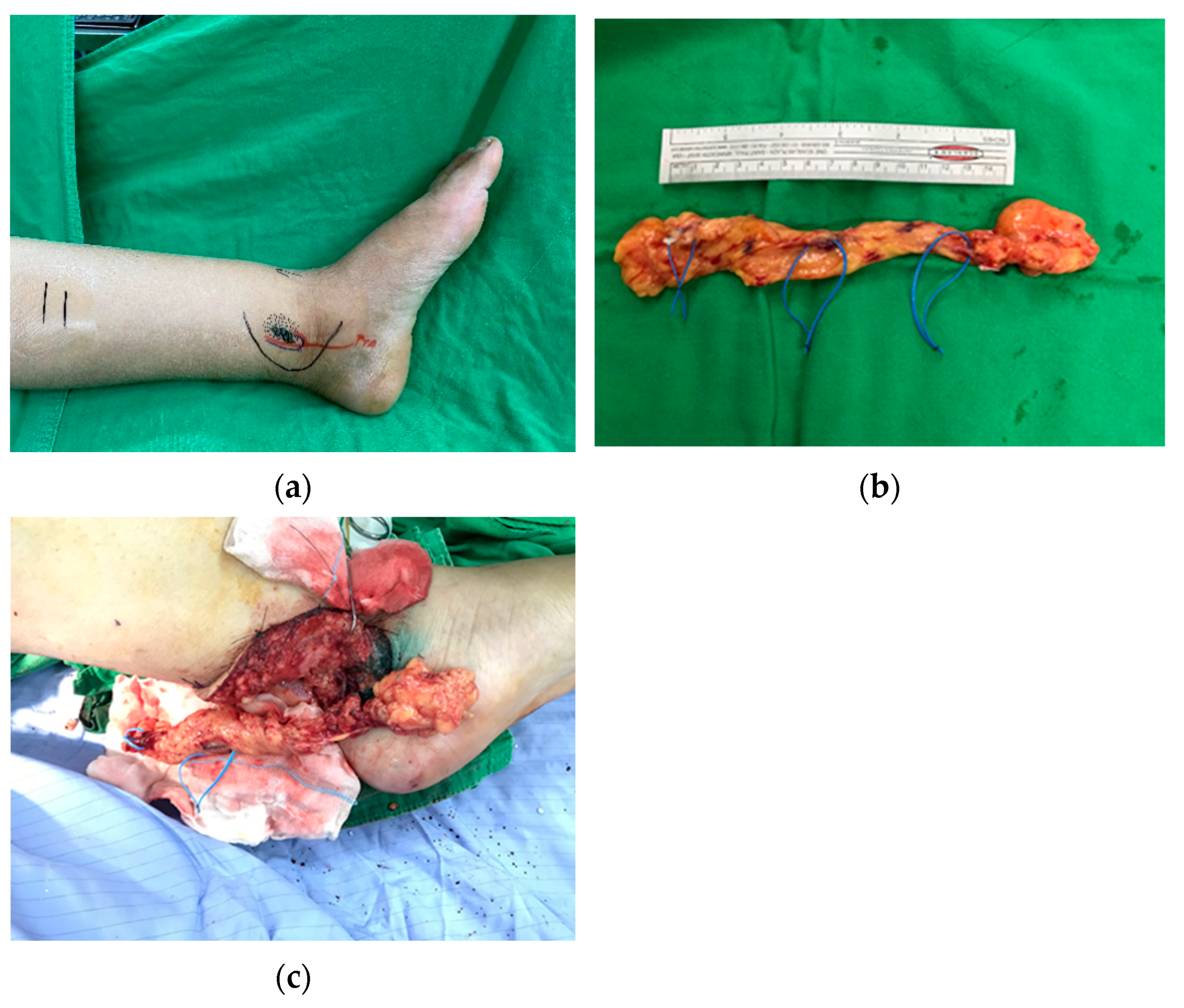
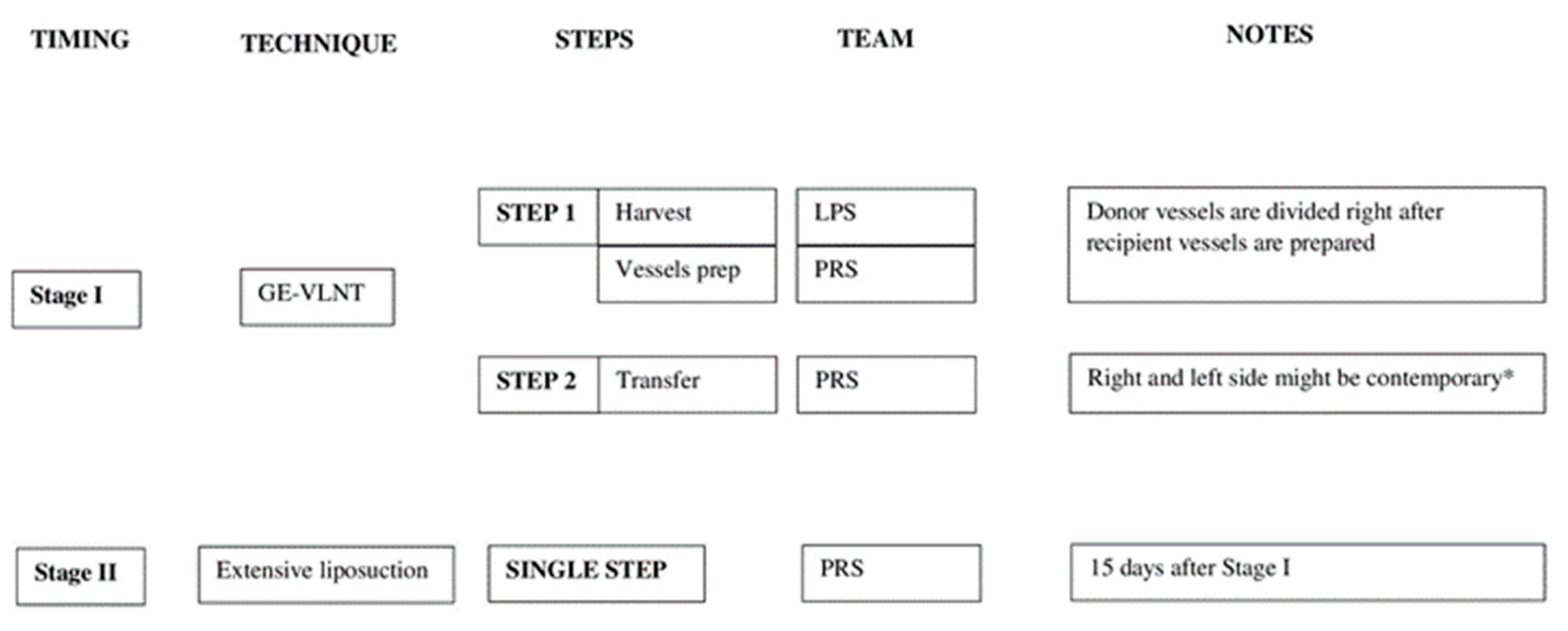
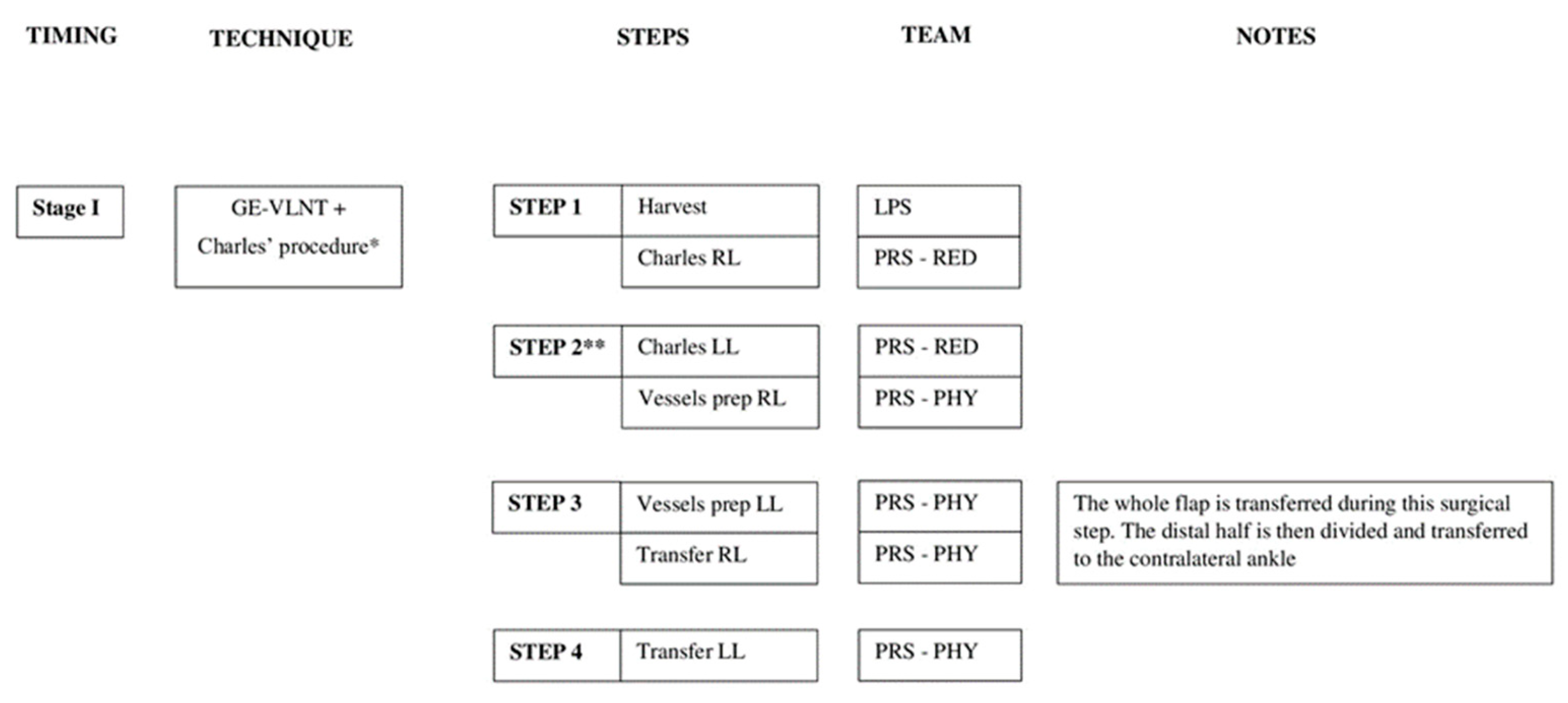
2.1. Surgical Techniques
2.2. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lee, T.S.; Morris, C.M.; Czerniec, S.A.; Mangion, A.J. Does lymphedema severity affect quality of life? Simple question. Challenging answers. Lymphat. Res. Biol. 2018, 16, 85–91. [Google Scholar] [CrossRef]
- Cigna, E.; Pierazzi, D.M.; Sereni, S.; Marcasciano, M.; Losco, L.; Bolletta, A. Lymphatico-venous anastomosis in chronic ulcer with venous insufficiency: A case report. Microsurgery 2021, 41, 574–578. [Google Scholar] [CrossRef]
- Lo Torto, F.; Kaciulyte, J.; Mori, F.L.; Frattaroli, J.M.; Marcasciano, M.; Casella, D.; Cigna, E.; Losco, L.; Manrique, O.J.; Nicoli, F.; et al. Microsurgical lymphedema treatment: An objective evaluation of the quality of online information. J. Plast. Reconstr. Aesthet. Surg. 2021, 74, 637–640. [Google Scholar] [CrossRef]
- de Sire, A.; Losco, L.; Cigna, E.; Lippi, L.; Gimigliano, F.; Gennari, A.; Cisari, C.; Chen, H.C.; Fusco, N.; Invernizzi, M. Three-dimensional laser scanning as a reliable and reproducible diagnostic tool in breast cancer related lymphedema rehabilitation: A proof-of-principle study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 4476–4485. [Google Scholar]
- de Sire, A.; Inzitari, M.T.; Moggio, L.; Pinto, M.; de Sire, G.; Supervia, M.; Petraroli, A.; Rubino, M.; Carbotti, D.; Succurro, E.; et al. Effects of Intermittent Pneumatic Compression on Lower Limb Lymphedema in Patients with Type 2 Diabetes Mellitus: A Pilot Randomized Controlled Trial. Medicina 2021, 57, 1018. [Google Scholar] [CrossRef]
- Rockson, S.G. The unique biology of lymphatic edema. Lymphat. Res. Biol. 2009, 7, 97–100. [Google Scholar] [CrossRef]
- Tashiro, K.; Arikawa, M.; Kagaya, Y.; Kobayashi, E.; Kawai, A.; Miyamoto, S. Flap reconstruction after groin and medial thigh sarcoma resection reduces the risk of lower-extremity lymphedema. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 685–710. [Google Scholar] [CrossRef]
- Feola, A.; Marino, V.; Marsella, L.T. Medical Liability: The Current State of Italian Legislation. Eur. J. Health Law 2015, 22, 347–358. [Google Scholar] [CrossRef]
- Feola, A.; Minotti, C.; Marchetti, D.; Caricato, M.; Capolupo, G.T.; Marsella, L.T.; La Monaca, G. A Five-Year Survey for Plastic Surgery Malpractice Claims in Rome, Italy. Medicina 2021, 57, 571. [Google Scholar] [CrossRef]
- Losco, L.; Roxo, A.C.; Roxo, C.W.; de Sire, A.; Bolletta, A.; Cuomo, R.; Grimaldi, L.; Cigna, E.; Roxo, C.D.P. Helix Thigh Lift. A Novel Approach to Severe Deformities in Massive Weight Loss Patients. J. Investig. Surg. 2021, 24, 1–7. [Google Scholar] [CrossRef]
- Verhulst, A.C.; Wesselius, T.S.; Glas, H.H.; Vreeken, R.D.; Ulrich, D.; Maal, T. Accuracy and reproducibility of a newly developed tool for volume measurements of the arm using 3D stereophotogrammetry. J. Plast. Reconstr. Aesthet. Surg. 2017, 12, 1753–1759. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Invernizzi, M.; Lippi, L.; Cisari, C.; Özçakar, L.; Franchignoni, F. Blurred lines between axillary web syndrome and Mondor’s disease after breast cancer surgery: A case report. Ann. Phys. Rehabil. Med. 2020, 63, 365–367. [Google Scholar] [CrossRef] [PubMed]
- Cheville, A.L.; McGarvey, C.L.; Petrek, J.A.; Russo, S.A.; Taylor, M.E.; Thiadens, S.R. Lymphedema management. Semin. Radiat. Oncol. 2003, 13, 290–301. [Google Scholar] [CrossRef]
- Ciudad, P.; Chen, H.C.; Bustos, S.S.; Manrique, O.J.; Bolletta, A.; Forte, A.J.; Huayllani, M.T.; Agko, M.; Urbina, J.A.; Date, S.; et al. The deep inferior epigastric lymphatic cable flap connected to gastroepiploic lymph node flap for treatment of refractory chylous ascites: Report of two cases. Microsurgery 2021, 41, 376–383. [Google Scholar] [CrossRef] [PubMed]
- de Sire, A.; Losco, L.; Cisari, C.; Gennari, A.; Boldorini, R.; Fusco, N.; Cigna, E.; Invernizzi, M. Axillary web syndrome in women after breast cancer surgery referred to an Oncological Rehabilitation Unit: Which are the main risk factors? A retrospective case-control study. Eur. Rev. Med. Pharmacol. Sci. 2020, 24, 8028–8035. [Google Scholar]
- Qiu, S.S.; Chen, H.Y.; Cheng, M.H. Vascularized lymph node flap transfer and lymphovenous anastomosis for klippel-trenaunay syndrome with congenital lymphedema. Plast. Reconstr. Surg. Glob. Open 2014, 2, e167. [Google Scholar] [CrossRef]
- Bolletta, A.; Di Taranto, G.; Chen, S.H.; Elia, R.; Amorosi, V.; Chan, J.C.; Chen, H.C. Surgical treatment of Milroy disease. J. Surg. Oncol. 2020, 121, 175–181. [Google Scholar] [CrossRef] [Green Version]
- The diagnosis and treatment of peripheral lymphedema: 2016 consensus document of the international society of Lymphology. Lymphology 2016, 49, 170–184.
- Keeley, V.; Crooks, S.; Locke, J.; Veigas, D.; Riches, K.; Hilliam, R. A quality of life measure for limb lymphoedema (LYMQOL). J. Lymphoedema 2010, 5, 1. [Google Scholar]
- Ciudad, P.; Manrique, O.J.; Date, S.; Agko, M.; Perez Coca, J.J.; Chang, W.L.; Lo Torto, F.; Nicoli, F.; Maruccia, M.; López Mendoza, J.; et al. Double gastroepiploic vascularized lymph node tranfers to middle and distal limb for the treatment of lymphedema. Microsurgery 2017, 37, 771–779. [Google Scholar] [CrossRef]
- Schaverien, M.V.; Munnoch, D.A.; Brorson, H. Liposuction treatment of lymphedema. Semin. Plast. Surg. 2018, 32, 42–47. [Google Scholar] [CrossRef]
- Karri, V.; Yang, M.C.; Lee, I.J.; Chen, S.H.; Hong, J.P.; Xu, E.S.; Cruz-Vargas, J.; Chen, H.C. Optimizing outcome of charles’ procedure for chronic lower extremity lymphoedema. Ann. Plast. Surg. 2011, 66, 393–402. [Google Scholar] [CrossRef] [PubMed]
- Salgado, C.J.; Mardini, S.; Spanio, S.; Tang, W.R.; Sassu, P.; Chen, H.C. Radical reduction of lymphedema with preservation of perforators. Ann. Plast. Surg. 2007, 59, 173–179. [Google Scholar] [CrossRef]
- Agko, M.; Ciudad, P.; Chen, H.-C. Staged surgical treatment of extremity lymphedema with dual gastroepiploic vascularized lymph node transfers followed by suction-assisted lipectomy—A prospective study. J. Surg. Oncol. 2018, 117, 1148–1156. [Google Scholar] [CrossRef] [PubMed]
- Di Taranto, G.; Bolletta, A.; Chen, S.H.; Losco, L.; Elia, R.; Cigna, E.; Rubino, C.; Ribuffo, D.; Chen, H.C. A prospective study on combined lymphedema surgery: Gastroepiploic vascularized lymph nodes transfer and lymphaticovenous anastomosis followed by suction lipectomy. Microsurgery 2021, 41, 34–43. [Google Scholar] [CrossRef] [PubMed]
- Yildirim, M.E.C.; Chen, S.H.; Mousavi, S.A.; Chen, H.C. Treatment of toes as an integrated part of infection control for advanced lower limb lymphedema. J. Plast. Reconstr. Aesthet. Surg. 2020, 21, 30371–30375. [Google Scholar] [CrossRef] [PubMed]
- Bolletta, A.; di Taranto, G.; Losco, L.; Elia, R.; Sert, G.; Ribuffo, D.; Cigna, E.; Chen, H.C. Combined lymph node transfer and suction-assisted lipectomy in lymphedema treatment: A prospective study. Microsurgery 2022. [Google Scholar] [CrossRef]
- Loh, C.Y.Y.; Wu, J.C.-W.; Nguyen, A.; Dayan, J.; Smith, M.; Masia, J.; Chang, D.; Koshima, I.; Cheng, M.H. The 5th world symposium for lymphedema surgery-Recent updates in lymphedema surgery and setting up of a global knowledge exchange platform. J. Surg. Oncol. 2017, 115, 6–12. [Google Scholar] [CrossRef]
- Di Taranto, G.; Chen, S.H.; Elia, R.; Bolletta, A.; Amorosi, V.; Sitpahul, N.; Chan, J.C.; Ribuffo, D.; Chen, H.C. Free gastroepiploic lymph nodes and omentum flap for treatment of lower limb ulcers in severe lymphedema: Killing two birds with one stone. J. Surg. Oncol. 2020, 121, 168–174. [Google Scholar] [CrossRef] [Green Version]
- Scaglioni, M.F.; Arvanitakis, M.; Chen, Y.C.; Giovanoli, P.; Chia-Shen Yang, J.; Chang, E.I. Comprehensive review of vascularized lymph node transfers for lymphedema: Outcomes and complications. Microsurgery 2016, 38, 222–229. [Google Scholar] [CrossRef]
- Zampell, J.C.; Aschen, S.; Weitman, E.S.; Yan, A.; Elhadad, S.; De Brot Andrade, M.; Mehrara, B. Regulation of adipogenesis by lymphatic fluid stasis: Part I. Adipogenesis, fibrosis, and inflammation. Plast. Reconstr. Surg. 2012, 129, 825–834. [Google Scholar] [CrossRef] [Green Version]
- Olszewski, W.L.; Engeset, A.; Romaniuk, A.; Grzelak, I.; Ziolkowska, A. Immune cells in peripheral lymph and skin of patients with obstructive lymphedema. Lymphology 1990, 23, 23–33. [Google Scholar] [PubMed]
- Brorson, H.; Svensson, H. Skin blood flow of the lymphedematous arm before and after liposuction. Lymphology 1997, 30, 165–172. [Google Scholar] [PubMed]
- Tashiro, K.; Feng, J.; Wu, S.H.; Mashiko, T.; Kanayama, K.; Narushima, M.; Uda, H.; Miyamoto, S.; Koshima, I.; Yoshimura, K. Pathological changes of adipose tissue in secondary lymphedema. Br. J. Dermatol. 2017, 177, 158–167. [Google Scholar] [CrossRef] [PubMed]
- Ciudad, P.; Manrique, O.J.; Adabi, K.; Huang, T.C.; Agko, M.; Trignano, E.; Chang, W.L.; Chen, T.W.; Salgado, C.J.; Chen, H.C. Combined double vascularized lymph node transfers and modified radical reduction with preservation of perforators for advanced stages of lymphedema. J. Surg. Oncol. 2019, 119, 439–448. [Google Scholar] [CrossRef] [PubMed]
- Sapountzis, S.; Ciudad, P.; Lim, S.Y.; Chilgar, R.M.; Kiranantawat, K.; Nicoli, F.; Constantinides, J.; Wei, M.Y.; Sönmez, T.T.; Singhal, D.; et al. Modified Charles procedure and lymph node flap transfer for advanced lower extremity lymphedema. Microsurgery 2014, 34, 439–447. [Google Scholar] [CrossRef] [PubMed]
- Kaciulyte, J.; Garutti, L.; Spadoni, D.; Velazquez-Mujica, J.; Losco, L.; Ciudad, P.; Marcasciano, M.; Lo Torto, F.; Casella, D.; Ribuffo, D.; et al. Genital Lymphedema and How to Deal with It: Pearls and Pitfalls from over 38 Years of Experience with Unusual Lymphatic System Impairment. Medicina 2021, 57, 1175. [Google Scholar] [CrossRef]
- Machol, J.A., 4th; Langenstroer, P.; Sanger, J.R. Surgical reduction of scrotal massive localized lymphedema (MLL) in obesity. J. Plast. Reconstr. Aesthet. Surg. 2014, 67, 1719–1725. [Google Scholar] [CrossRef]
- Losco, L.; Roxo, A.C.; Roxo, C.W.; Lo Torto, F.; Bolletta, A.; de Sire, A.; Aksoyler, D.; Ribuffo, D.; Cigna, E.; Roxo, C.P. Lower Body Lift After Bariatric Surgery: 323 Consecutive Cases Over 10-Year Experience. Aesthetic Plast. Surg. 2020, 44, 421–432. [Google Scholar] [CrossRef]
- O’Neill, A.C.; Sebastiampillai, S.; Zhong, T.; Hofer, S.O.P. Increasing body mass index increases complications but not failure rates in microvascular breast reconstruction: A retrospective cohort study. J. Plast. Reconstr. Aesthet. Surg. 2019, 72, 1518–1524. [Google Scholar] [CrossRef]
- Cheng, M.H.; Loh, C.Y.Y.; Lin, C.Y. Outcomes of vascularized lymph node transfer and lymphovenous anastomosis for treatment of primary lymphedema. Plast. Reconstr. Surg. Glob. Open 2018, 6, e2056. [Google Scholar] [CrossRef]
- Manrique, O.J.; Sabbagh, M.D. Primary lymphedema and lymphedema associated with vascular malformations: Diagnosis and management. In Lymphedema: Surgical Approach and Specific Topics; Chen, H.C., Ciudad, P., Tang, Y.B., Chen, S.H., Eds.; Elsevier LLC: Taiwan, 2017; pp. 39–55. [Google Scholar]
- Sakuma, H.; Watanabe, S.; Kono, H. A Novel Surgical Approach for Refractory Secondary Lymphedema of the Lower Extremity Accompanying Micro-Arteriovenous Fistula. Ann. Vasc. Surg. 2020, 65, 284.e13–284.e18. [Google Scholar] [CrossRef] [PubMed]
- Paul, M.A.; Opyrchał, J.; Knakiewicz, M.; Jaremków, P.; Duda-Barcik, Ł.; Ibrahim, A.; Lin, S.J. The long-term effect of body contouring procedures on the quality of life in morbidly obese patients after bariatric surgery. PLoS ONE 2020, 15, e0229138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, A.J.M.; Kool, M.; Keuter, X.H.A.; Heuts, E.M.; Piatkowski de Grzymala, A.A.; van der Hulst, R.; Qiu, S.S. Quality of Life Questionnaires in Breast Cancer-Related Lymphedema Patients: Review of the Literature. Lymphat. Res. Biol. 2018, 16, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Domenici, L.; Caputo, G.G.; Losco, L.; Di Taranto, G.; Lo Torto, F.; Pierazzi, D.M.; Governa, M.; Benedetti Panici, P.; Ribuffo, D.; Cigna, E. Muscle-Sparing Skin-Reducing Breast Reconstruction with Pre-Pectoral Implants in Breast Cancer Patients: Long-Term Assessment of Patients’ Satisfaction and Quality of Life. J. Investig. Surg. 2021, 20, 1–7. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Value (Rate) |
|---|---|
| Patients | 29 |
| Age—years | |
| Mean ± SD | 51 ± 17.1 |
| Range | 15–75 |
| Gender | |
| Female | 18 (62%) |
| BMI—kg/m2 | |
| Mean ± SD | 25.5 ± 2.8 |
| Range | 22–36.5 |
| Etiology | |
| Primary | 9 (31%) |
| Secondary | 20 (69%) |
| Duration of symptoms—months | |
| Mean ± SD | 32.5 ± 24.7 |
| Range | 20–158 |
| Circumference improvement—cm | |
| Mean ± SD | 4.2 ± 3.3 |
| mid-thigh | 5.1 ± 1.1 |
| mid-calf | 6.9 ± 5 |
| ankle | 2.9 ± 0.7 |
| mid-foot | 1.7 ± 0.5 |
| Follow-up—months | 38.4 ± 11.8 |
| Postoperative Cellulitis | No Postoperative Cellulitis | p-Value | |
|---|---|---|---|
| Duration of symptoms (months) | 39.1 ± 34.2 | 26.3 ± 4.9 | 0.020 |
| Body mass index (kg/m2) | 26.5 ± 3.4 | 24.3 ± 1.4 | 0.006 |
| Complications | Value (Rate) |
|---|---|
| Overall complications | 9 (31%) |
| Recurrent infections | 3 (10%) |
| Partial skin graft loss | 1 (3%) |
| Persistent erythema | 1 (3%) |
| Persistent numbness (unilateral) | 1 (3%) |
| Hypertrophic scarring | 5 (17%) |
| Revisional surgery | |
| Skin grafting | 6 (20%) |
| Crypt excision | 5 (17%) |
| Toe amputation | 1 (3%) |
| Re-Operations * | 3 (10%) |
| Features | Preoperative LYMQoL | Postoperative LYMQoL | Improvement | p-Value |
|---|---|---|---|---|
| Group A * (overall) | 3.7 ± 0.6 | 6.3 ± 0.8 | 2.6 ± 0.5 | <0.001 |
| Function | 28.2 ± 1.1 | 24.2 ± 1.3 | 4 ± 0.7 | |
| Appearance | 25.3 ± 1 | 18.9 ± 1.5 | 6.3 ±1.3 | |
| Symptoms | 15.8 ± 1.2 | 12.1 ± 1.3 | 3.7 ± 0.9 | |
| Mood | 19.3 ± 1 | 11.7 ± 1.4 | 7.5 ± 1.3 | |
| Group B * (overall) | 2.6 ± 1 | 6 ± 0.8 | 3.4 ± 0.5 | <0.001 |
| Function | 30.6 ± 1.2 | 24 ± 2.4 | 6.6 ± 1.8 | |
| Appearance | 26.9 ± 1.3 | 21.6 ± 2.8 | 5.3 ± 2 | |
| Symptoms | 18.3 ± 1.1 | 12.2 ± 2.6 | 6.1 ± 1.9 | |
| Mood | 22.7 ± 1.1 | 18.3 ± 2.6 | 4.4 ± 1.9 | |
| Total (overall) | 3.4 ± 0.9 | 6.2 ± 0.8 | 2.8 ± 0.6 | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Losco, L.; Bolletta, A.; de Sire, A.; Chen, S.-H.; Sert, G.; Aksoyler, D.; Velazquez-Mujica, J.; Invernizzi, M.; Cigna, E.; Chen, H.-C. The Combination of Lymph Node Transfer and Excisional Procedures in Bilateral Lower Extremity Lymphedema: Clinical Outcomes and Quality of Life Assessment with Long-Term Follow-Up. J. Clin. Med. 2022, 11, 570. https://doi.org/10.3390/jcm11030570
Losco L, Bolletta A, de Sire A, Chen S-H, Sert G, Aksoyler D, Velazquez-Mujica J, Invernizzi M, Cigna E, Chen H-C. The Combination of Lymph Node Transfer and Excisional Procedures in Bilateral Lower Extremity Lymphedema: Clinical Outcomes and Quality of Life Assessment with Long-Term Follow-Up. Journal of Clinical Medicine. 2022; 11(3):570. https://doi.org/10.3390/jcm11030570
Chicago/Turabian StyleLosco, Luigi, Alberto Bolletta, Alessandro de Sire, Shih-Heng Chen, Gokhan Sert, Dicle Aksoyler, Jonathan Velazquez-Mujica, Marco Invernizzi, Emanuele Cigna, and Hung-Chi Chen. 2022. "The Combination of Lymph Node Transfer and Excisional Procedures in Bilateral Lower Extremity Lymphedema: Clinical Outcomes and Quality of Life Assessment with Long-Term Follow-Up" Journal of Clinical Medicine 11, no. 3: 570. https://doi.org/10.3390/jcm11030570