
Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
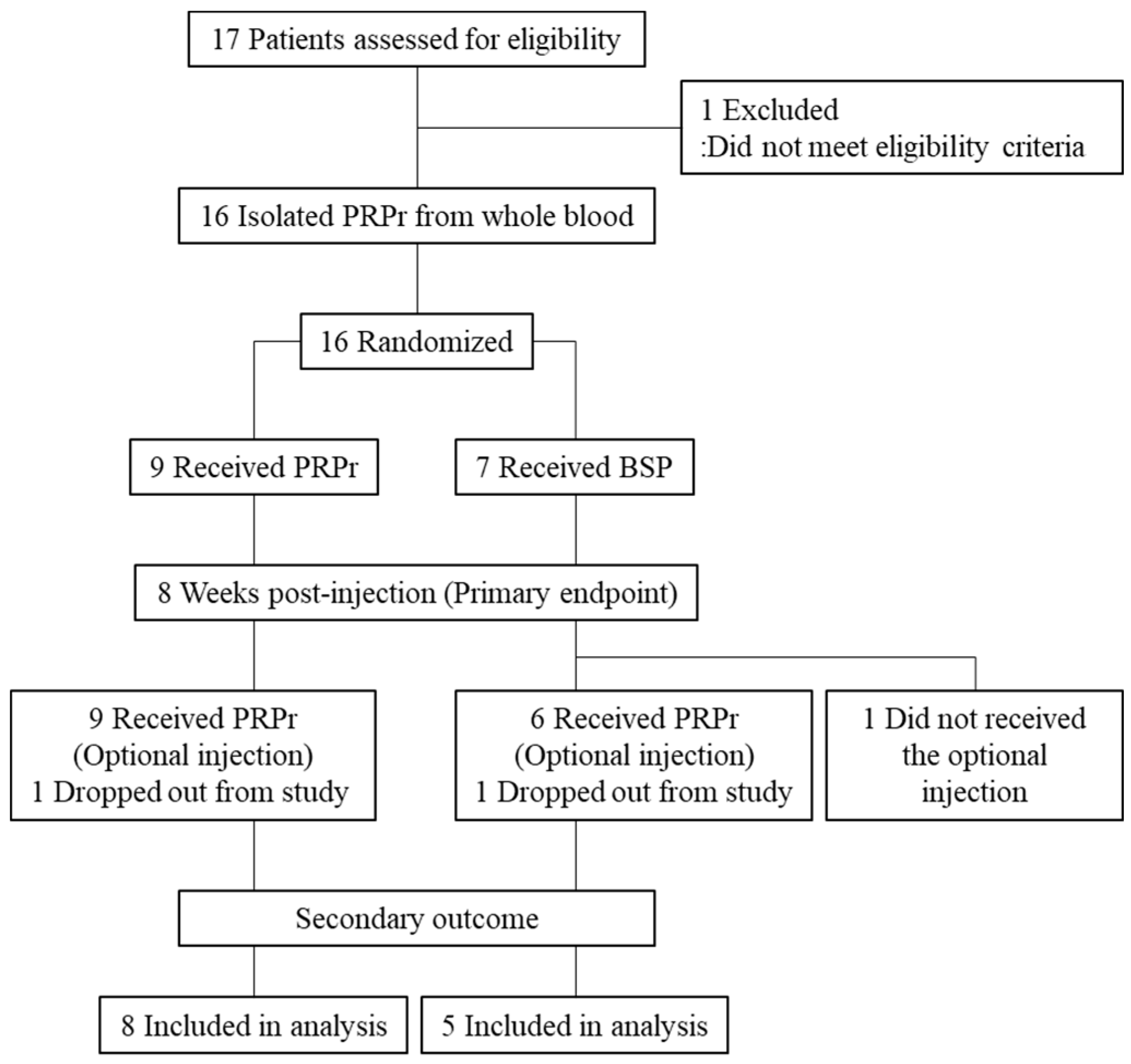
2.1. Study Design
2.2. Participants
2.3. Randomization
2.4. PRP Releasate (PRPr) Preparation and Fluoroscopy-Guided Injection
2.5. Outcome Measures
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Quality Assessment of Platelet-Rich Plasma (PRP)
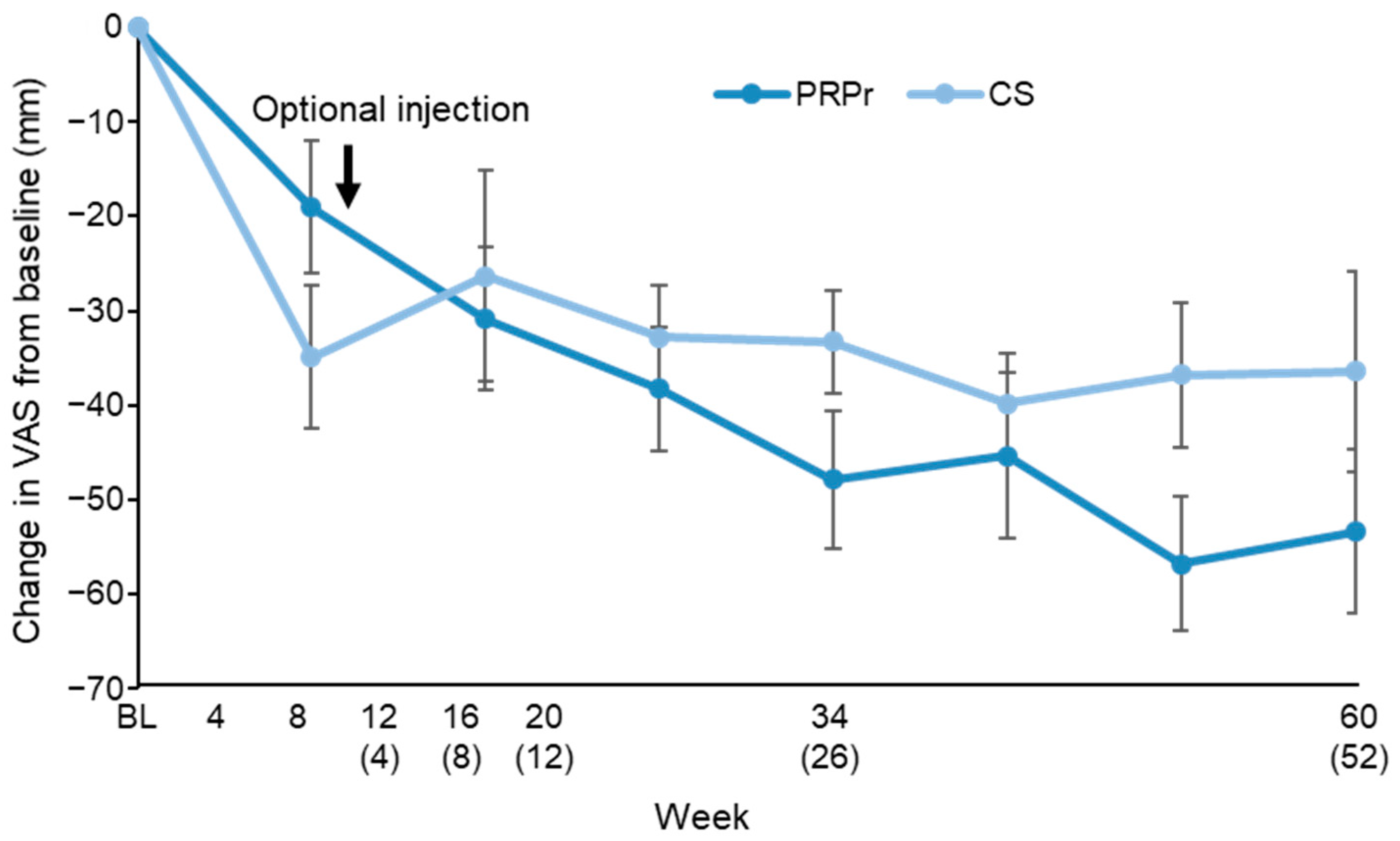
3.3. Primary Outcome of Efficacy
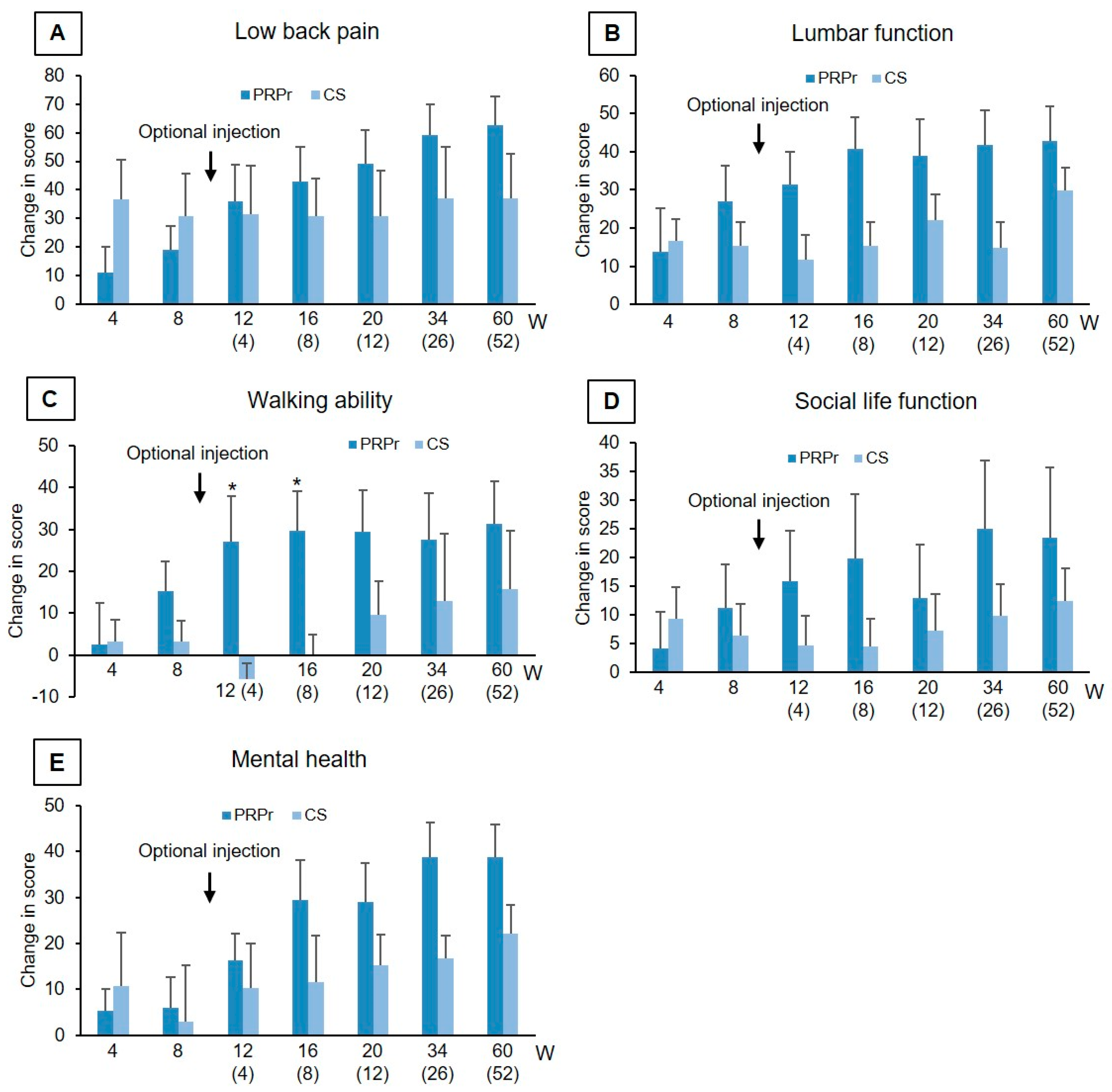
3.4. Secondary Outcomes of Efficacy
3.4.1. Outcomes of the Optional Injection (n = 15)
3.4.2. Outcomes of Single Injection (n = 1)
3.5. Safety
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Knezevic, N.N.; Candido, K.D.; Vlaeyen, J.W.S.; Van Zundert, J.; Cohen, S.P. Low back pain. Lancet 2021, 398, 78–92. [Google Scholar] [CrossRef]
- Zhang, S.; Hu, B.; Liu, W.; Wang, P.; Lv, X.; Chen, S.; Shao, Z. The role of structure and function changes of sensory nervous system in intervertebral disc-related low back pain. Osteoarthr. Cartil. 2021, 29, 17–27. [Google Scholar] [CrossRef]
- Vo, N.V.; Hartman, R.A.; Patil, P.R.; Risbud, M.V.; Kletsas, D.; Iatridis, J.C.; Hoyland, J.A.; Le Maitre, C.L.; Sowa, G.A.; Kang, J.D. Molecular mechanisms of biological aging in intervertebral discs. J. Orthop. Res. 2016, 34, 1289–1306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akeda, K.; An, H.S.; Pichika, R.; Attawia, M.; Thonar, E.J.; Lenz, M.E.; Uchida, A.; Masuda, K. Platelet-rich plasma (PRP) stimulates the extracellular matrix metabolism of porcine nucleus pulposus and anulus fibrosus cells cultured in alginate beads. Spine (Phila Pa 1976) 2006, 31, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Chujo, T.; An, H.S.; Akeda, K.; Miyamoto, K.; Muehleman, C.; Attawia, M.; Andersson, G.; Masuda, K. Effects of growth differentiation factor-5 on the intervertebral disc--in vitro bovine study and in vivo rabbit disc degeneration model study. Spine (Phila Pa 1976) 2006, 31, 2909–2917. [Google Scholar] [CrossRef] [PubMed]
- Masuda, K.; Imai, Y.; Okuma, M.; Muehleman, C.; Nakagawa, K.; Akeda, K.; Thonar, E.; Andersson, G.; An, H.S. Osteogenic protein-1 injection into a degenerated disc induces the restoration of disc height and structural changes in the rabbit anular puncture model. Spine (Phila Pa 1976) 2006, 31, 742–754. [Google Scholar] [CrossRef]
- Kato, K.; Akeda, K.; Miyazaki, S.; Yamada, J.; Muehleman, C.; Miyamoto, K.; Asanuma, Y.A.; Asanuma, K.; Fujiwara, T.; Lenz, M.E.; et al. NF-kB decoy oligodeoxynucleotide preserves disc height in a rabbit anular-puncture model and reduces pain induction in a rat xenograft-radiculopathy model. Eur. Cell. Mater. 2021, 41, 90–109. [Google Scholar] [CrossRef]
- An, H.S.; Masuda, K.; Cs-Szabo, G.; Zhang, Y.; Chee, A.; Andersson, G.B.; Im, H.J.; Thonar, E.J.; Kwon, Y.M. Biologic repair and regeneration of the intervertebral disk. J. Am. Acad. Orthop. Surg. 2011, 19, 450–452. [Google Scholar] [CrossRef]
- Masuda, K.; An, H.S. Prevention of disc degeneration with growth factors. Eur. Spine J. 2006, 15 (Suppl. 3), S422–S432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akeda, K.; Yamada, J.; Linn, E.T.; Sudo, A.; Masuda, K. Platelet-rich plasma in the management of chronic low back pain: A critical review. J. Pain Res. 2019, 12, 753–767. [Google Scholar] [CrossRef] [Green Version]
- Nurden, A.T. Platelets, inflammation and tissue regeneration. Thromb. Haemost. 2011, 105 (Suppl. 1), S13–S33. [Google Scholar] [CrossRef]
- Everts, P.; Onishi, K.; Jayaram, P.; Lana, J.F.; Mautner, K. Platelet-Rich Plasma: New Performance Understandings and Therapeutic Considerations in 2020. Int. J. Mol. Sci 2020, 21, 7794. [Google Scholar] [CrossRef] [PubMed]
- Mariani, E.; Roffi, A.; Cattini, L.; Pulsatelli, L.; Assirelli, E.; Krishnakumar, G.S.; Cenacchi, A.; Kon, E.; Filardo, G. Release kinetic of pro- and anti-inflammatory biomolecules from platelet-rich plasma and functional study on osteoarthritis synovial fibroblasts. Cytotherapy 2020, 22, 344–353. [Google Scholar] [CrossRef] [PubMed]
- Nie, L.Y.; Zhao, K.; Ruan, J.; Xue, J. Effectiveness of Platelet-Rich Plasma in the Treatment of Knee Osteoarthritis: A Meta-analysis of Randomized Controlled Clinical Trials. Orthop J. Sports Med. 2021, 9, 2325967120973284. [Google Scholar] [CrossRef]
- Muthu, S.; Jeyaraman, M.; Chellamuthu, G.; Jeyaraman, N.; Jain, R.; Khanna, M. Does the Intradiscal Injection of Platelet Rich Plasma Have Any Beneficial Role in the Management of Lumbar Disc Disease? Glob. Spine J. 2021, 2192568221998367. [Google Scholar] [CrossRef]
- Tuakli-Wosornu, Y.A.; Terry, A.; Boachie-Adjei, K.; Harrison, J.R.; Gribbin, C.K.; LaSalle, E.E.; Nguyen, J.T.; Solomon, J.L.; Lutz, G.E. Lumbar Intradiskal Platelet-Rich Plasma (PRP) Injections: A Prospective, Double-Blind, Randomized Controlled Study. PMR 2016, 8, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Akeda, K.; Ohishi, K.; Masuda, K.; Bae, W.C.; Takegami, N.; Yamada, J.; Nakamura, T.; Sakakibara, T.; Kasai, Y.; Sudo, A. Intradiscal Injection of Autologous Platelet-Rich Plasma Releasate to Treat Discogenic Low Back Pain: A Preliminary Clinical Trial. Asian Spine J. 2017, 11, 380–389. [Google Scholar] [CrossRef]
- Pfirrmann, C.W.; Metzdorf, A.; Zanetti, M.; Hodler, J.; Boos, N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2001, 26, 1873–1878. [Google Scholar] [CrossRef]
- Koslosky, E.; Gendelberg, D. Classification in Brief: The Meyerding Classification System of Spondylolisthesis. Clin. Orthop. Relat. Res. 2020, 478, 1125–1130. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Sekiguchi, M.; Otani, K.; Mashiko, H.; Shioda, H.; Wakita, T.; Niwa, S.; Kikuchi, S.; Konno, S. Computational psychological study of the Brief Scale for Psychiatric Problems in Orthopaedic Patients (BS-POP) for patients with chronic low back pain: Verification of responsiveness. J. Orthop. Sci. 2015, 20, 469–474. [Google Scholar] [CrossRef] [PubMed]
- Collins, T.; Alexander, D.; Barkatali, B. Platelet-rich plasma: A narrative review. EFORT Open Rev. 2021, 6, 225–235. [Google Scholar] [CrossRef] [PubMed]
- Ostelo, R.W.; Deyo, R.A.; Stratford, P.; Waddell, G.; Croft, P.; Von Korff, M.; Bouter, L.M.; de Vet, H.C. Interpreting change scores for pain and functional status in low back pain: Towards international consensus regarding minimal important change. Spine (Phila Pa 1976) 2008, 33, 90–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roach, K.E.; Brown, M.D.; Dunigan, K.M.; Kusek, C.L.; Walas, M. Test-retest reliability of patient reports of low back pain. J. Orthop. Sports Phys. 1997, 26, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Shafshak, T.S.; Elnemr, R. The Visual Analogue Scale Versus Numerical Rating Scale in Measuring Pain Severity and Predicting Disability in Low Back Pain. J. Clin. Rheumatol. 2021, 27, 282–285. [Google Scholar] [CrossRef]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry Disability Index. Spine (Phila Pa 1976) 2000, 25, 2940–2952; discussion 2952. [Google Scholar] [CrossRef]
- Roland, M.; Fairbank, J. The Roland-Morris Disability Questionnaire and the Oswestry Disability Questionnaire. Spine (Phila Pa 1976) 2000, 25, 3115–3124. [Google Scholar] [CrossRef] [Green Version]
- Suzukamo, Y.; Fukuhara, S.; Kikuchi, S.; Konno, S.; Roland, M.; Iwamoto, Y.; Nakamura, T.; Committee on Science Project, J.O.A. Validation of the Japanese version of the Roland-Morris Disability Questionnaire. J. Orthop. Sci. 2003, 8, 543–548. [Google Scholar] [CrossRef]
- Clinical Outcomes Committee of the Japanese Orthopaedic Association, Subcommittee on Evaluation of Back Pain and Cervical Myelopathy; Subcommittee on Low Back Pain; Cervical Myelopathy Evaluation of the Clinical Outcome Committe of the Japanese Orthopaedic Association; Fukui, M.; Chiba, K.; Kawakami, M.; Kikuchi, S.; Konno, S.; Miyamoto, M.; Seichi, A.; et al. JOA back pain evaluation questionnaire: Initial report. J. Orthop. Sci. 2007, 12, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Fukui, M.; Chiba, K.; Kawakami, M.; Kikuchi, S.; Konno, S.; Miyamoto, M.; Seichi, A.; Shimamura, T.; Shirado, O.; Taguchi, T.; et al. Japanese Orthopaedic Association Back Pain Evaluation Questionnaire. Part 2. Verification of its reliability: The Subcommittee on Low Back Pain and Cervical Myelopathy Evaluation of the Clinical Outcome Committee of the Japanese Orthopaedic Association. J. Orthop. Sci. 2007, 12, 526–532. [Google Scholar] [CrossRef] [Green Version]
- Fukui, M.; Chiba, K.; Kawakami, M.; Kikuchi, S.; Konno, S.; Miyamoto, M.; Seichi, A.; Shimamura, T.; Shirado, O.; Taguchi, T.; et al. JOA Back Pain Evaluation Questionnaire (JOABPEQ)/JOA Cervical Myelopathy Evaluation Questionnaire (JOACMEQ). The report on the development of revised versions. April 16, 2007. The Subcommittee of the Clinical Outcome Committee of the Japanese Orthopaedic Association on Low Back Pain and Cervical Myelopathy Evaluation. J. Orthop. Sci. 2009, 14, 348–365. [Google Scholar] [CrossRef] [PubMed]
- Griffith, J.F.; Wang, Y.X.; Antonio, G.E.; Choi, K.C.; Yu, A.; Ahuja, A.T.; Leung, P.C. Modified Pfirrmann grading system for lumbar intervertebral disc degeneration. Spine (Phila Pa 1976) 2007, 32, E708–E712. [Google Scholar] [CrossRef]
- Levi, D.; Horn, S.; Tyszko, S.; Levin, J.; Hecht-Leavitt, C.; Walko, E. Intradiscal Platelet-Rich Plasma Injection for Chronic Discogenic Low Back Pain: Preliminary Results from a Prospective Trial. Pain Med. 2016, 17, 1010–1022. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, P.; Jiang, L.; Zhuang, C.; Yang, Y.; Zhang, Z.; Chen, W.; Zheng, T. Intradiscal injection therapy for degenerative chronic discogenic low back pain with end plate Modic changes. Spine J. 2011, 11, 100–106. [Google Scholar] [CrossRef]
- Lu, Y.; Guzman, J.Z.; Purmessur, D.; Iatridis, J.C.; Hecht, A.C.; Qureshi, S.A.; Cho, S.K. Nonoperative management of discogenic back pain: A systematic review. Spine (Phila Pa 1976) 2014, 39, 1314–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khot, A.; Bowditch, M.; Powell, J.; Sharp, D. The use of intradiscal steroid therapy for lumbar spinal discogenic pain: A randomized controlled trial. Spine (Phila Pa 1976) 2004, 29, 833–836; discussion 837. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria |
| Patients aged more than 18 years old were included if they had: |
| 1. Low back pain for at least 3 months. |
| 2. Low back pain visual analogue scare (VAS) score more than 40 mm. |
| 3. ODI score (%) more than 20% at bassline. |
| 4. Painful degenerative disc disease at least one lumbar level from L3/L4 to L5/S1 confirmed by radiographic findings and provocative discography. |
| (A) Disc degeneration evaluated by MRI (more than grade II by Pfirrmann grading [19]). |
| (B) Less than a 50% decrease of disc height measurement by lumbar radiograph. |
| (C) Discogenic pain evaluated by provocative discography. |
| 5. Provided written informed consent. |
| Exclusion Criteria |
| Patients were excluded if they had: |
| 1. Remarkable neurological symptoms including cauda equine and neuropathy in the lower extremities. |
| 2. Any systematic or spinal infections. |
| 3. Undergone any lumbar surgeries. |
| 4. Undergone any interventional intervertebral disc therapies. |
| 5. Intervertebral instability evaluated by lumbar radiograph. |
| 6. Spondylolisthesis (more than grade I by Meyerding classification [20]). |
| 7. A history of neuro-muscular diseases, cerebral diseases, malignant tumor, and blood coagulation disorders. |
| 8. Any diseases that were high risk for infections after the injection treatment. |
| 9. Anti-coagulant or anti-platelet drugs at the time of treatment. |
| 10. Reported that they were pregnant or lactating. |
| 11. Difficulty in participating over the evaluation period. |
| 12. More than 10-points in doctor version of brief scale for evaluation of psychiatric problems in orthopedic patients (BS-POP) and more than 15-points in patient version of BS-POS [21]. |
| 13. Any contraindication for MRI examination. |
| 14. Been judged as inappropriate for clinical study by the principal investigator or co-investigators. |
| PRPr (n = 9) | CS (n = 7) | p-Value | |
|---|---|---|---|
| Age | 35.1 (8.7) | 27.9 (5.2) | 0.09 |
| Gender (male: n, %) | 6 (66.7%) | 5 (71.4%) | 0.78 |
| Target disc level (n, %) | 0.16 | ||
| L3/L4 | 1 (9.0%) | 3 (30%) | |
| L4/L5 | 5 (45.5%) | 6 (60%) | |
| L5/S1 | 5 (45.5%) | 1 (10%) | |
| Number of the target disc | 0.78 | ||
| One disc | 7 | 4 | |
| Two discs | 2 | 3 | |
| VAS | 68.3 ± 13.3 | 59.4 ± 12.4 | 0.19 |
| ODI (%) | 36.0 ± 11.8 | 33.3 ± 11.6 | 0.66 |
| RDQ | 8.6 ± 4.8 | 9.3 ± 4.7 | 0.77 |
| JOABPEQ | |||
| Low back pain | 22.0 ± 21.5 | 12.1 ± 9.9 | 0.28 |
| Lumbar function | 51.8 ± 23.7 | 59.6 ± 28.6 | 0.56 |
| Walking ability | 65.0 ± 28.1 | 66.3 ± 34.5 | 0.94 |
| Social function | 48.6 ± 15.2 | 43.7 ± 16.0 | 0.55 |
| Mental health | 42.2 ± 21.8 | 47.6 ± 17.6 | 0.61 |
| Pfirrmann classification | N.A. | ||
| Grade 4 | 11 | 10 | |
| Modified Pfirrmann classification | N.A. | ||
| Grade 4 | 8 | 5 | |
| Grade 5 | 0 | 3 | |
| Grade 6 | 3 | 2 | |
| Blood cell count of whole blood | |||
| Platelet (×103/µL) | 262.2 ± 45.7 | 250.3 ± 37.1 | 0.57 |
| WBC (×103/µL) | 7.1 ± 1.8 | 5.7 ± 0.7 | 0.08 |
| Blood cell count of PRP | |||
| Platelet (×103/µL) | 1054.1 ± 350.3 | 1148.0 ± 399.8 | 0.63 |
| WBC (×103/µL) | 0.1 ± 0.1 | 0.1 ± 0.2 | 0.99 |
| Change | % Change | |||||
|---|---|---|---|---|---|---|
| Week | PRPr | CS | p-Value | PRPr | CS | p-Value |
| VAS | ||||||
| 4 | −19.0 ± 21.3 | −34.9 ± 20.1 | 0.15 | −29.4 ± 37.0 | −57.6 ± 31.2 | 0.13 |
| 8 | −30.9 ± 22.7 | −26.3 ± 29.8 | 0.73 | −48.2 ± 34.9 | −41.7 ± 54.5 | 0.78 |
| 12 (4) | −38.3 ± 19.6 | −32.8 ± 13.4 | 0.56 | −60.1 ± 31.9 | −56.4 ± 22.0 | 0.81 |
| 16 (8) | −47.9 ± 21.2 | −33.3 ± 13.4 | 0.18 | −74.2 ± 33.5 | −57.3 ± 22.5 | 0.30 |
| 20 (12) | −45.4 ± 26.3 | −29.8 ± 12.8 | 0.64 | −67.5 ± 37.3 | −68.7 ± 20.3 | 0.94 |
| 32 (26) | −56.8 ± 20.2 | −36.8 ± 17.1 | 0.10 | −84.2 ± 23.8 | −66.6 ± 28.6 | 0.25 |
| 60 (52) | −53.4 ± 24.7 | −36.4 ± 23.7 | 0.25 | −78.2 ± 33.2 | −61.0 ± 37.9 | 0.41 |
| ODI (%) | ||||||
| 4 | −8.2 ± 9.5 | −7.2 ± 8.4 | 0.83 | −20.4 ± 27.1 | −28.5 ± 38.0 | 0.63 |
| 8 | −14.5 ± 11.6 | −7.7 ± 8.9 | 0.22 | −37.7 ± 31.9 | −31.0 ± 41.1 | 0.72 |
| 12 (4) | −17.9 ± 13.2 | −11.2 ± 7.8 | 0.30 | −46.5 ± 33.4 | −37.1 ± 34.4 | 0.61 |
| 16 (8) | −23.6 ± 14.9 | −11.9 ± 7.3 | 0.10 | −62.1 ± 30.6 | −39.0 ± 32.2 | 0.19 |
| 20 (12) | −21.9 ± 13.4 | −12.7 ± 6.1 | 0.14 | −58.9 ± 31.1 | −43.4 ± 32.1 | 0.37 |
| 32 (26) | −26.9 ± 13.1 | −14.5 ± 10.8 | 0.14 | −74.8 ± 27.9 | −45.9 ± 41.1 | 0.18 |
| 60 (52) | −26.6 ± 14.8 | −13.9 ± 9.7 | 0.12 | −76.0 ± 37.6 | −42.4 ± 31.5 | 0.13 |
| RDQ | ||||||
| 4 | −2.2 ± 5.9 | −2.3 ± 4.2 | 0.95 | −25.6 ± 97.1 | −38.0 ± 58.4 | 0.27 |
| 8 | −3.4 ± 6.7 | −1.7 ± 4.2 | 0.58 | −39.5 ± 85.8 | −32.8 ± 58.5 | 0.54 |
| 12 (4) | −6.9 ± 6.4 | −1.6 ± 3.6 | 0.13 | −54.8 ± 67.5 | −31.0 ± 47.8 | 0.51 |
| 16 (8) | −6.6 ± 6.1 | −1.7 ± 2.9 | 0.10 | −56.7 ± 63.7 | −25.6 ± 43.2 | 0.32 |
| 20 (12) | −6.7 ± 6.2 | −2.3 ± 4.6 | 0.17 | −65.7 ± 35.4 | −32.8 ± 56.1 | 0.18 |
| 32 (26) | −8.5 ± 5.3 | −3.4 ± 4.0 | 0.09 | −88.0 ± 23.5 | −42.1 ± 45.1 | 0.03 * |
| 60 (52) | −8.8 ± 5.0 | −4.2 ± 4.5 | 0.13 | −92.8 ± 14.1 | −49.6 ± 44.4 | 0.10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akeda, K.; Ohishi, K.; Takegami, N.; Sudo, T.; Yamada, J.; Fujiwara, T.; Niimi, R.; Matsumoto, T.; Nishimura, Y.; Ogura, T.; et al. Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial. J. Clin. Med. 2022, 11, 304. https://doi.org/10.3390/jcm11020304
Akeda K, Ohishi K, Takegami N, Sudo T, Yamada J, Fujiwara T, Niimi R, Matsumoto T, Nishimura Y, Ogura T, et al. Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial. Journal of Clinical Medicine. 2022; 11(2):304. https://doi.org/10.3390/jcm11020304
Chicago/Turabian StyleAkeda, Koji, Kohshi Ohishi, Norihiko Takegami, Takao Sudo, Junichi Yamada, Tatsuhiko Fujiwara, Rui Niimi, Takeshi Matsumoto, Yuki Nishimura, Toru Ogura, and et al. 2022. "Platelet-Rich Plasma Releasate versus Corticosteroid for the Treatment of Discogenic Low Back Pain: A Double-Blind Randomized Controlled Trial" Journal of Clinical Medicine 11, no. 2: 304. https://doi.org/10.3390/jcm11020304