
Restoration of Fertility in Patients with Spontaneous Premature Ovarian Insufficiency: New Techniques under the Microscope

 ,
,  ,
, 
Abstract
:1. Introduction
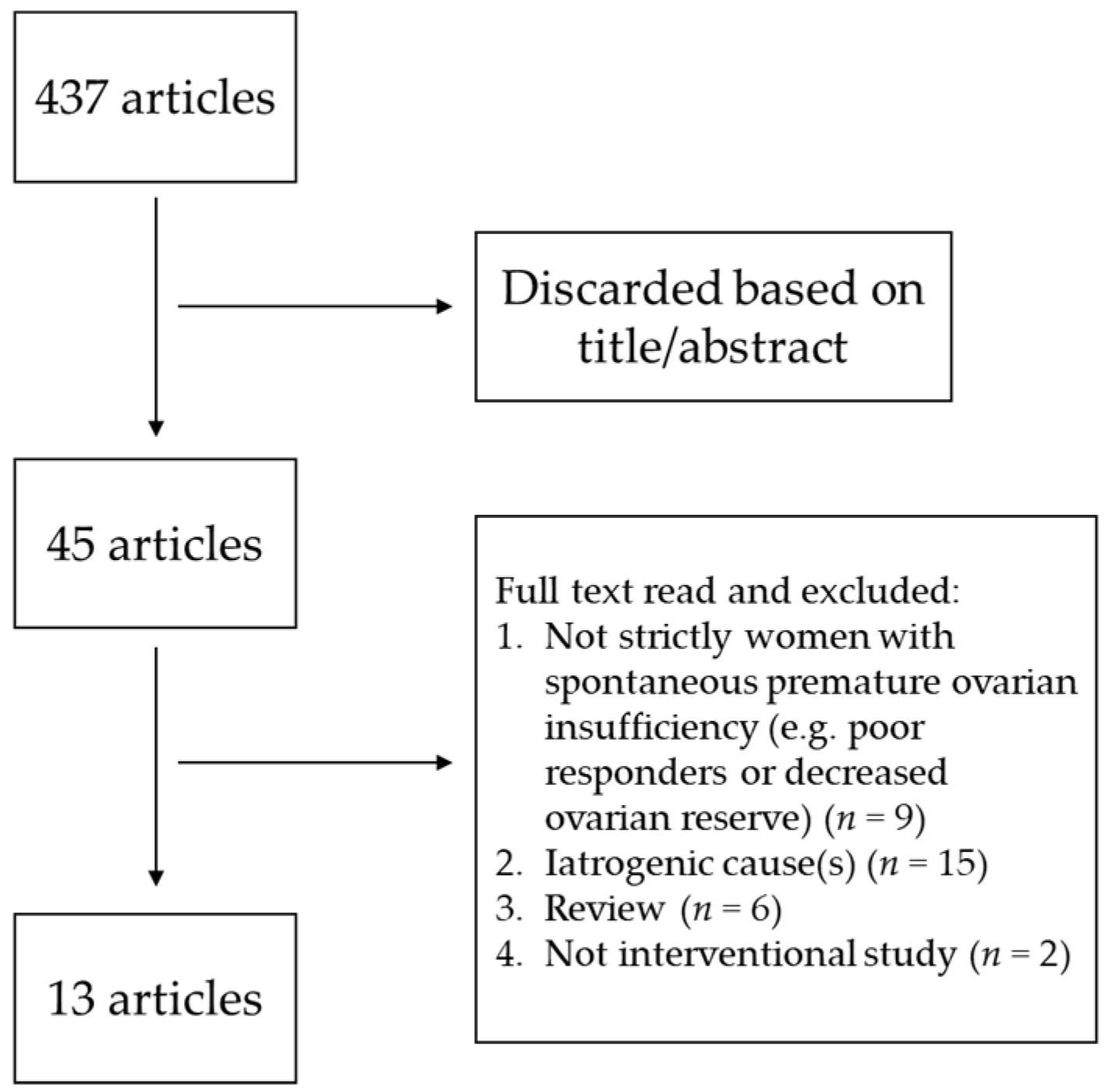
2. Materials and Methods
3. Results
3.1. Autologous Platelet-Rich Plasma Intraovarian Injection
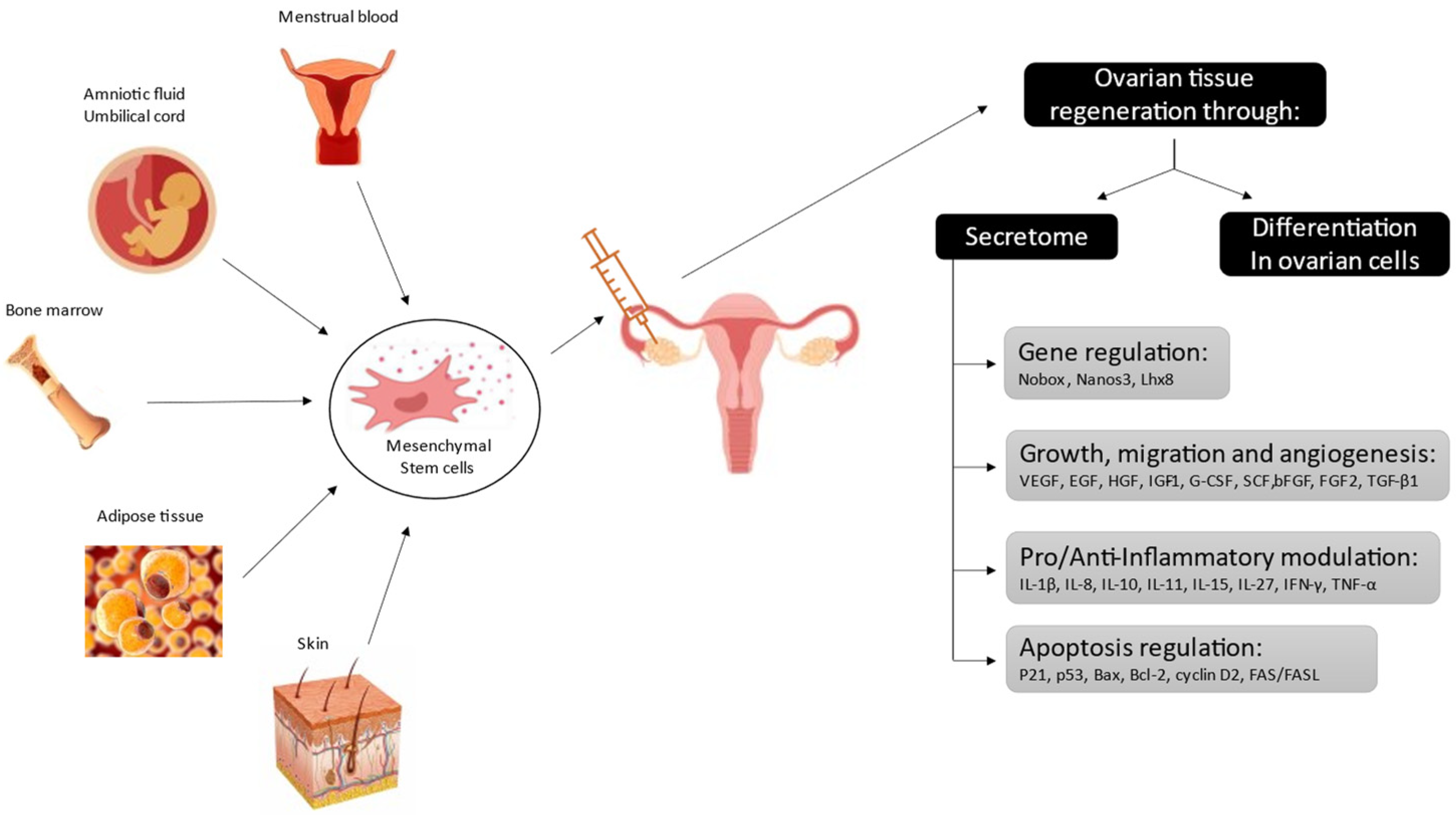
3.2. Human Mesenchymal Stem Cells
3.3. In Vitro Activation of Dormant Follicles
3.4. Mechanical Activation of Dormant Follicles
3.5. Immunomodulation in Autoimmune Forms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Webber, L.; Davies, M.; Anderson, R.; Bartlett, J.; Braat, D.; Cartwright, B.; Cifkova, R.; de Muinck Keizer-Schrama, S.; Hogervorst, E.; Janse, F.; et al. ESHRE Guideline: Management of women with premature ovarian insufficiency. Hum. Reprod. 2016, 31, 926–937. [Google Scholar] [CrossRef] [Green Version]
- Dolmans, M.M.; Donnez, J. Fertility preservation in women for medical and social reasons: Oocytes vs. ovarian tissue. Best Pract. Res. Clin. Obstet. Gynaecol. 2021, 70, 63–80. [Google Scholar] [CrossRef] [PubMed]
- Fertility&Sterility. IFFS Surveillance 07. Fertil. Steril. 2007, 87, 69. [Google Scholar]
- Ford, E.A.; Beckett, E.L.; Roman, S.D.; McLaughlin, E.A.; Sutherland, J.M. Advances in human primordial follicle activation and premature ovarian insufficiency. Reproduction 2020, 159, R15–R29. [Google Scholar] [CrossRef] [Green Version]
- Kawamura, K.; Kawamura, N.; Hsueh, A.J. Activation of dormant follicles: A new treatment for premature ovarian failure? Curr. Opin. Obstet. Gynecol. 2016, 28, 217–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharara, F.I.; Lelea, L.L.; Rahman, S.; Klebanoff, J.S.; Moawad, G.N. A narrative review of platelet-rich plasma (PRP) in reproductive medicine. J. Assist. Reprod. Genet. 2021, 38, 1003–1012. [Google Scholar] [CrossRef]
- Dos Santos, R.G.; Santos, G.S.; Alkass, N.; Chiesa, T.L.; Azzini, G.O.; da Fonseca, L.F.; Dos Santos, A.F.; Rodrigues, B.L.; Mosaner, T.; Lana, J.F. The regenerative mechanisms of platelet-rich plasma: A review. Cytokine 2021, 144, 155560. [Google Scholar] [CrossRef]
- Sfakianoudis, K.; Simopoulou, M.; Nitsos, N.; Rapani, A.; Pappas, A.; Pantou, A.; Chronopoulou, M.; Deligeoroglou, E.; Koutsilieris, M.; Pantos, K. Autologous Platelet-Rich Plasma Treatment Enables Pregnancy for a Woman in Premature Menopause. J. Clin. Med. 2018, 8, 1. [Google Scholar] [CrossRef] [Green Version]
- Pantos, K.; Simopoulou, M.; Pantou, A.; Rapani, A.; Tsioulou, P.; Nitsos, N.; Syrkos, S.; Pappas, A.; Koutsilieris, M.; Sfakianoudis, K. A Case Series on Natural Conceptions Resulting in Ongoing Pregnancies in Menopausal and Prematurely Menopausal Women Following Platelet-Rich Plasma Treatment. Cell Transplant. 2019, 28, 1333–1340. [Google Scholar] [CrossRef] [Green Version]
- Sfakianoudis, K.; Simopoulou, M.; Grigoriadis, S.; Pantou, A.; Tsioulou, P.; Maziotis, E.; Rapani, A.; Giannelou, P.; Nitsos, N.; Kokkali, G.; et al. Reactivating Ovarian Function through Autologous Platelet-Rich Plasma Intraovarian Infusion: Pilot Data on Premature Ovarian Insufficiency, Perimenopausal, Menopausal, and Poor Responder Women. J. Clin. Med. 2020, 9, 1809. [Google Scholar] [CrossRef]
- Cakiroglu, Y.; Saltik, A.; Yuceturk, A.; Karaosmanoglu, O.; Kopuk, S.Y.; Scott, R.T.; Tiras, B.; Seli, E. Effects of intraovarian injection of autologous platelet rich plasma on ovarian reserve and IVF outcome parameters in women with primary ovarian insufficiency. Aging 2020, 12, 10211–10222. [Google Scholar] [CrossRef]
- Ahmadian, S.; Mahdipour, M.; Pazhang, M.; Sheshpari, S.; Mobarak, H.; Bedate, A.M.; Rahbarghazi, R.; Nouri, M. Effectiveness of Stem Cell Therapy in the Treatment of Ovarian Disorders and Female Infertility: A Systematic Review. Curr. Stem Cell Res. Ther. 2020, 15, 173–186. [Google Scholar] [CrossRef]
- Sagaradze, G.; Grigorieva, O.; Nimiritsky, P.; Basalova, N.; Kalinina, N.; Akopyan, Z.; Efimenko, A. Conditioned Medium from Human Mesenchymal Stromal Cells: Towards the Clinical Translation. Int. J. Mol. Sci. 2019, 20, 1656. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Igboeli, P.; El Andaloussi, A.; Sheikh, U.; Takala, H.; ElSharoud, A.; McHugh, A.; Gavrilova-Jordan, L.; Levy, S.; Al-Hendy, A. Intraovarian injection of autologous human mesenchymal stem cells increases estrogen production and reduces menopausal symptoms in women with premature ovarian failure: Two case reports and a review of the literature. J. Med. Case Rep. 2020, 14, 108. [Google Scholar] [CrossRef] [PubMed]
- Takehara, Y.; Yabuuchi, A.; Ezoe, K.; Kuroda, T.; Yamadera, R.; Sano, C.; Murata, N.; Aida, T.; Nakama, K.; Aono, F.; et al. The restorative effects of adipose-derived mesenchymal stem cells on damaged ovarian function. Lab. Investig. 2013, 93, 181–193. [Google Scholar] [CrossRef] [Green Version]
- Grady, S.T.; Watts, A.E.; Thompson, J.A.; Penedo, M.C.T.; Konganti, K.; Hinrichs, K. Effect of intra-ovarian injection of mesenchymal stem cells in aged mares. J. Assist Reprod. Genet. 2019, 36, 543–556. [Google Scholar] [CrossRef] [PubMed]
- Edessy, M. Autologous stem cells therapy, the first baby of idiopathic primary ovarian failure. Acta Med. Int. 2016, 3, 19–23. [Google Scholar] [CrossRef]
- Gabr, H.; Abo Elkheir, W.; El-Gazzar, A. Autologous stem cell transplantation in patients with idiopathic premature ovarian failure. J. Tissue Sci. Eng. 2016, 7, 27. [Google Scholar]
- Ding, L.; Yan, G.; Wang, B.; Xu, L.; Gu, Y.; Ru, T.; Cui, X.; Lei, L.; Liu, J.; Sheng, X.; et al. Transplantation of UC-MSCs on collagen scaffold activates follicles in dormant ovaries of POF patients with long history of infertility. Sci. China Life Sci. 2018, 61, 1554–1565. [Google Scholar] [CrossRef]
- Mashayekhi, M.; Mirzadeh, E.; Chekini, Z.; Ahmadi, F.; Eftekhari-Yazdi, P.; Vesali, S.; Madani, T.; Aghdami, N. Evaluation of safety, feasibility and efficacy of intra-ovarian transplantation of autologous adipose derived mesenchymal stromal cells in idiopathic premature ovarian failure patients: Non-randomized clinical trial, phase I, first in human. J. Ovarian Res. 2021, 14, 5. [Google Scholar] [CrossRef]
- Yan, L.; Wu, Y.; Li, L.; Wu, J.; Zhao, F.; Gao, Z.; Liu, W.; Li, T.; Fan, Y.; Hao, J.; et al. Clinical analysis of human umbilical cord mesenchymal stem cell allotransplantation in patients with premature ovarian insufficiency. Cell Prolif. 2020, 53, e12938. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Kawamura, K.; Cheng, Y.; Liu, S.; Klein, C.; Duan, E.K.; Hsueh, A.J. Activation of dormant ovarian follicles to generate mature eggs. Proc. Natl. Acad. Sci. USA 2010, 107, 10280–10284. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamura, K.; Cheng, Y.; Suzuki, N.; Deguchi, M.; Sato, Y.; Takae, S.; Ho, C.H.; Kawamura, N.; Tamura, M.; Hashimoto, S.; et al. Hippo signaling disruption and Akt stimulation of ovarian follicles for infertility treatment. Proc. Natl. Acad. Sci. USA 2013, 110, 17474–17479. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, N.; Yoshioka, N.; Takae, S.; Sugishita, Y.; Tamura, M.; Hashimoto, S.; Morimoto, Y.; Kawamura, K. Successful fertility preservation following ovarian tissue vitrification in patients with primary ovarian insufficiency. Hum. Reprod. 2015, 30, 608–615. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Han, T.; Yan, L.; Jiao, X.; Qin, Y.; Chen, Z.J. Resumption of Ovarian Function After Ovarian Biopsy/Scratch in Patients With Premature Ovarian Insufficiency. Reprod. Sci. 2019, 26, 207–213. [Google Scholar] [CrossRef]
- Kirshenbaum, M.; Orvieto, R. Premature ovarian insufficiency (POI) and autoimmunity—An update appraisal. J. Assist Reprod. Genet 2019, 36, 2207–2215. [Google Scholar] [CrossRef] [PubMed]
- Nelson, L.M.; Anasti, J.N.; Kimzey, L.M.; Defensor, R.A.; Lipetz, K.J.; White, B.J.; Shawker, T.H.; Merino, M.J. Development of luteinized graafian follicles in patients with karyotypically normal spontaneous premature ovarian failure. J. Clin. Endocrinol. Metab. 1994, 79, 1470–1475. [Google Scholar] [CrossRef]
- Musiał-Wysocka, A.; Kot, M.; Majka, M. The Pros and Cons of Mesenchymal Stem Cell-Based Therapies. Cell Transpl. 2019, 28, 801–812. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Reference | Sfakianoudis K. et al., 2020 | Cakiroglu Y. et al., 2020 | |||||
|---|---|---|---|---|---|---|---|
| Number of patients Mean age (years) | n = 30 * | n = 311 34.8 ± 4.3 | |||||
| Success group (n = 18, 60.0%) 35.11 ± 1.57 | Failure group (n = 12, 40.0%) 35.92 ± 1.93 | ||||||
| Baseline | 3 months after intraovarian injection of PRP | Baseline | 3 months after intraovarian injection of PRP | Baseline | After intraovarian injection of PRP | ||
| Mean duration of amenorrhea (months) | 10.06 ± 2.62 | Return of menstruation | 10.17 ± 4.76 | No return of menstruation | >4 | NA | |
| Hypothalamic– pituitary–ovarian axis parameters (means) | FSH (UI/mL) | 40.61 ± 6.05 | 20.67 ± 3.58 | 63.65 ± 6.41 | 59.40 ± 9.47 | 41.9 ± 24.7 | 41.6 ± 24.7 |
| LH (UI/mL) | 25.14 ± 3.10 | 19.31 ± 1.93 | 24.33 ± 3.04 | 23.50 ± 4.37 | NA | NA | |
| E2 (pg/mL) | 17.13 ± 2.22 | 48.08 ± 6.28 | 17.38 ± 2.61 | 20.86 ± 7.11 | NA | NA | |
| Ovarian reserve parameters (means) | AMH (ng/mL) | 0.18 ± 0.04 | 0.75 ± 0.06 | 0.15 ± 0.04 | 0.30 ± 0.05 | 0.13 ± 0.16 | 0.18 ± 0.18 |
| AFC | 0 | 2.33 ± 0.49 | 0 | 0 | 0.5 ± 0.5 | 1.7 ± 1.4 | |
| Pregnancy rate | Spontaneous | 16.7% (3/18) | 0% (0/12) | 7.4% (23/311) | |||
| After IVF | Not part of the study protocol | 4.5% (13/288) | |||||
| Total for the study | 10% (3/18) | 11.6% (36/311) | |||||
| Reference | Sample Size | Study Design | Stem Cells Source | Method | Main Outcomes |
|---|---|---|---|---|---|
| Edessy M. et al., 2016 | n = 10 | Single-arm study | Autologous bone marrow-derived mesenchymal stem cells | Laparoscopic injection in both ovaries |
|
| Gabr H. et al., 2016 | n = 30 | Single-arm study | Autologous bone-marrow-derived mesenchymal stem cells | Laparoscopic injection in one ovary and one ovarian artery |
|
| Ding L. et al., 2018 | n = 14 | Randomized, controlled, 2-arm study | Group 1 (n = 6): umbilical cord mesenchymal stem cells Group 2 (n = 8): umbilical cord mesenchymal stem cells on a collagen scaffold | Transvaginal injection guided by ultrasonography in one ovary | 2/14 (14.3%): pregnancy (one in each group):
|
| Yan L. et al., 2020 | n = 61 | Single-arm study | Umbilical cord mesenchymal stem cells | Transvaginal injection guided by ultrasonography in both ovaries |
|
| Mashayekhi M. et al., 2021 | n = 9 | Nonrandomized, controlled, open-label, 3-arm study | Autologous adipose-derived stromal cells; the subjects were divided in 3 groups (n = 3 per group) receiving 5, 10 or 15 × 106 cells | Transvaginal injection guided by ultrasonography in one ovary | 4/9 (44.4%) had menses restoration:
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mawet, M.; Perrier d’Hauterive, S.; Henry, L.; Potorac, I.; Kridelka, F.; Nisolle, M.; Pintiaux, A. Restoration of Fertility in Patients with Spontaneous Premature Ovarian Insufficiency: New Techniques under the Microscope. J. Clin. Med. 2021, 10, 5647. https://doi.org/10.3390/jcm10235647
Mawet M, Perrier d’Hauterive S, Henry L, Potorac I, Kridelka F, Nisolle M, Pintiaux A. Restoration of Fertility in Patients with Spontaneous Premature Ovarian Insufficiency: New Techniques under the Microscope. Journal of Clinical Medicine. 2021; 10(23):5647. https://doi.org/10.3390/jcm10235647
Chicago/Turabian StyleMawet, Marie, Sophie Perrier d’Hauterive, Laurie Henry, Iulia Potorac, Frédéric Kridelka, Michelle Nisolle, and Axelle Pintiaux. 2021. "Restoration of Fertility in Patients with Spontaneous Premature Ovarian Insufficiency: New Techniques under the Microscope" Journal of Clinical Medicine 10, no. 23: 5647. https://doi.org/10.3390/jcm10235647