
Long-Term Symptoms among Hospitalized COVID-19 Patients 48 Weeks after Discharge—A Prospective Cohort Study

 , , ,
, , ,  and
and
Abstract
:1. Introduction
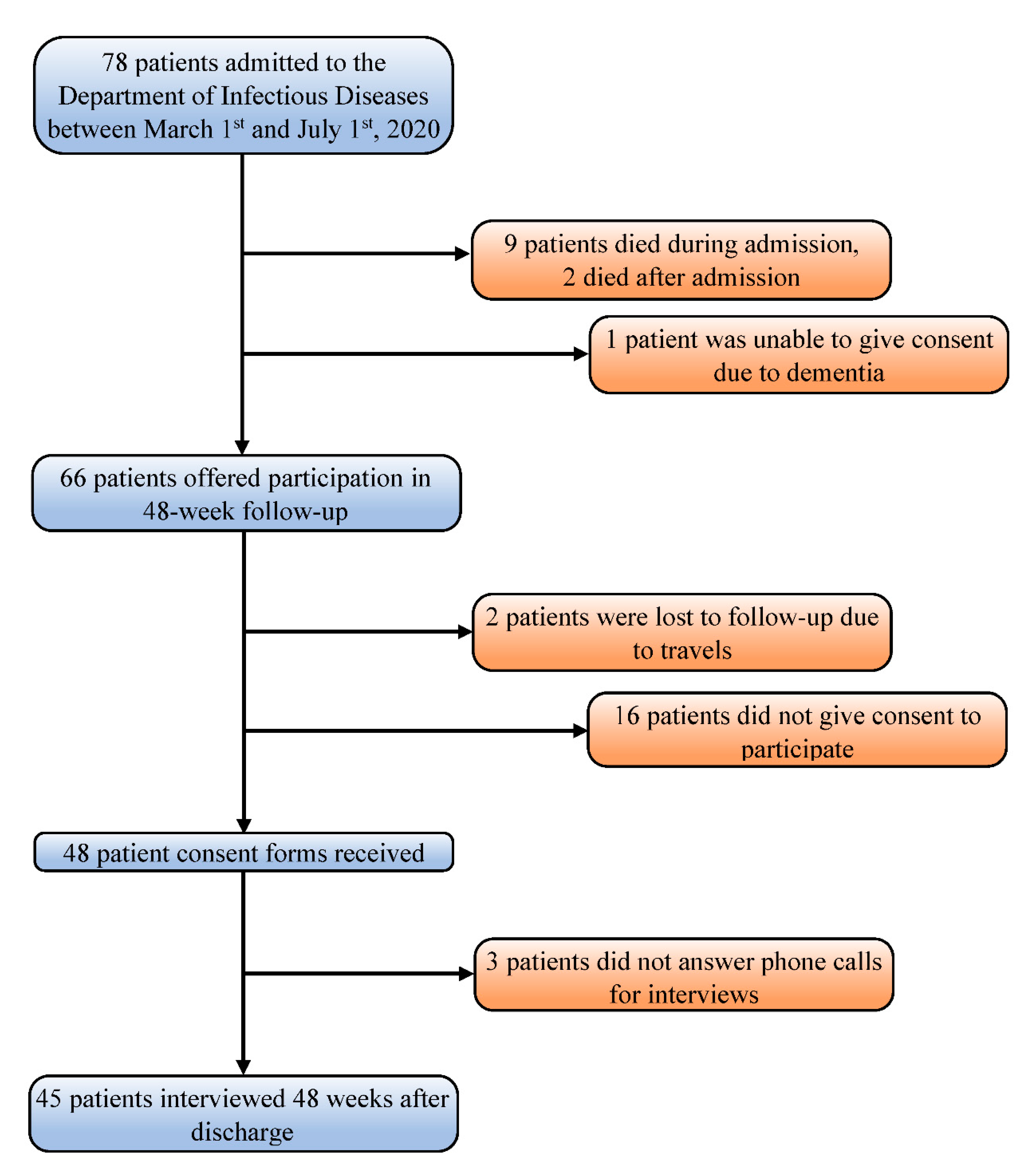
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
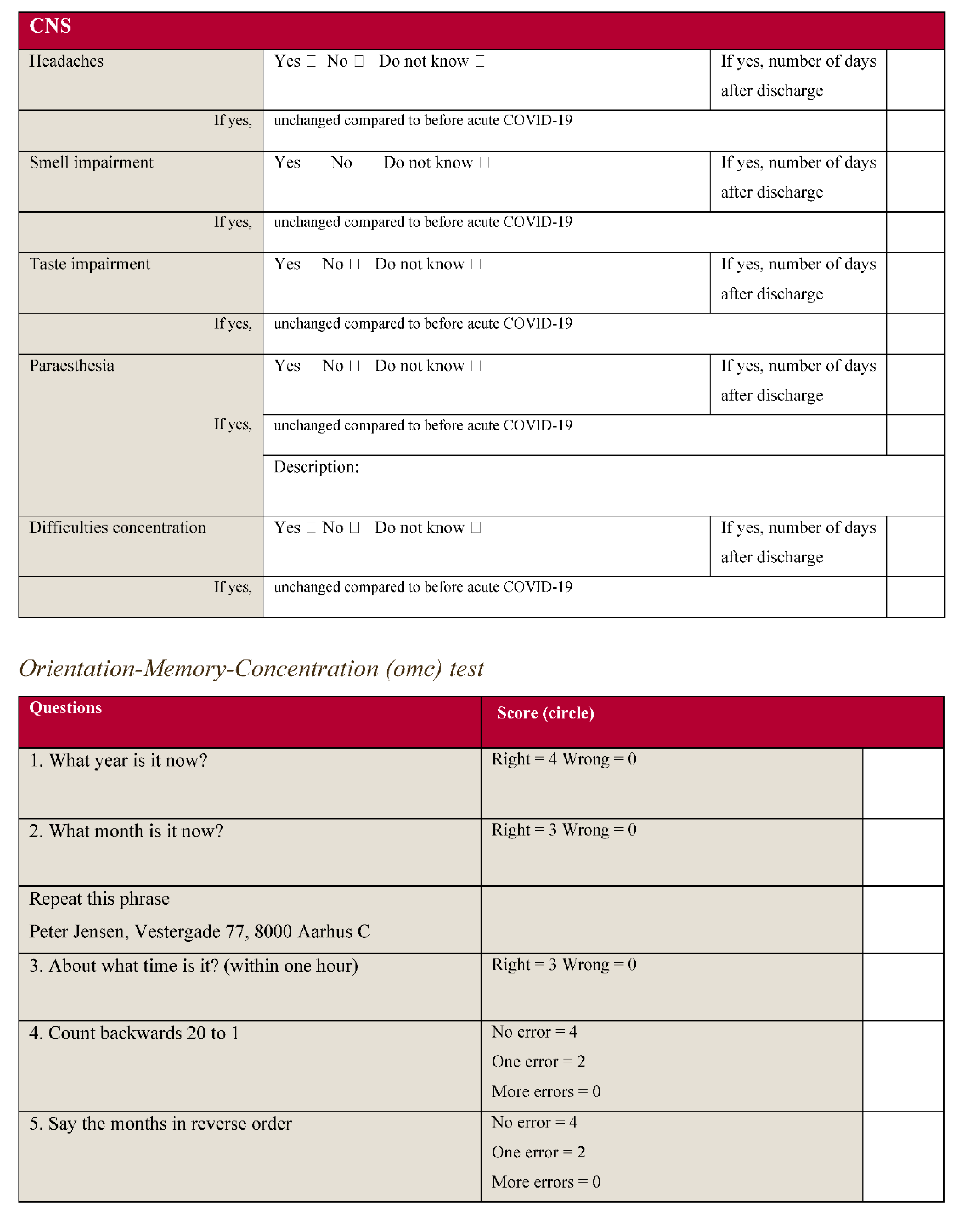
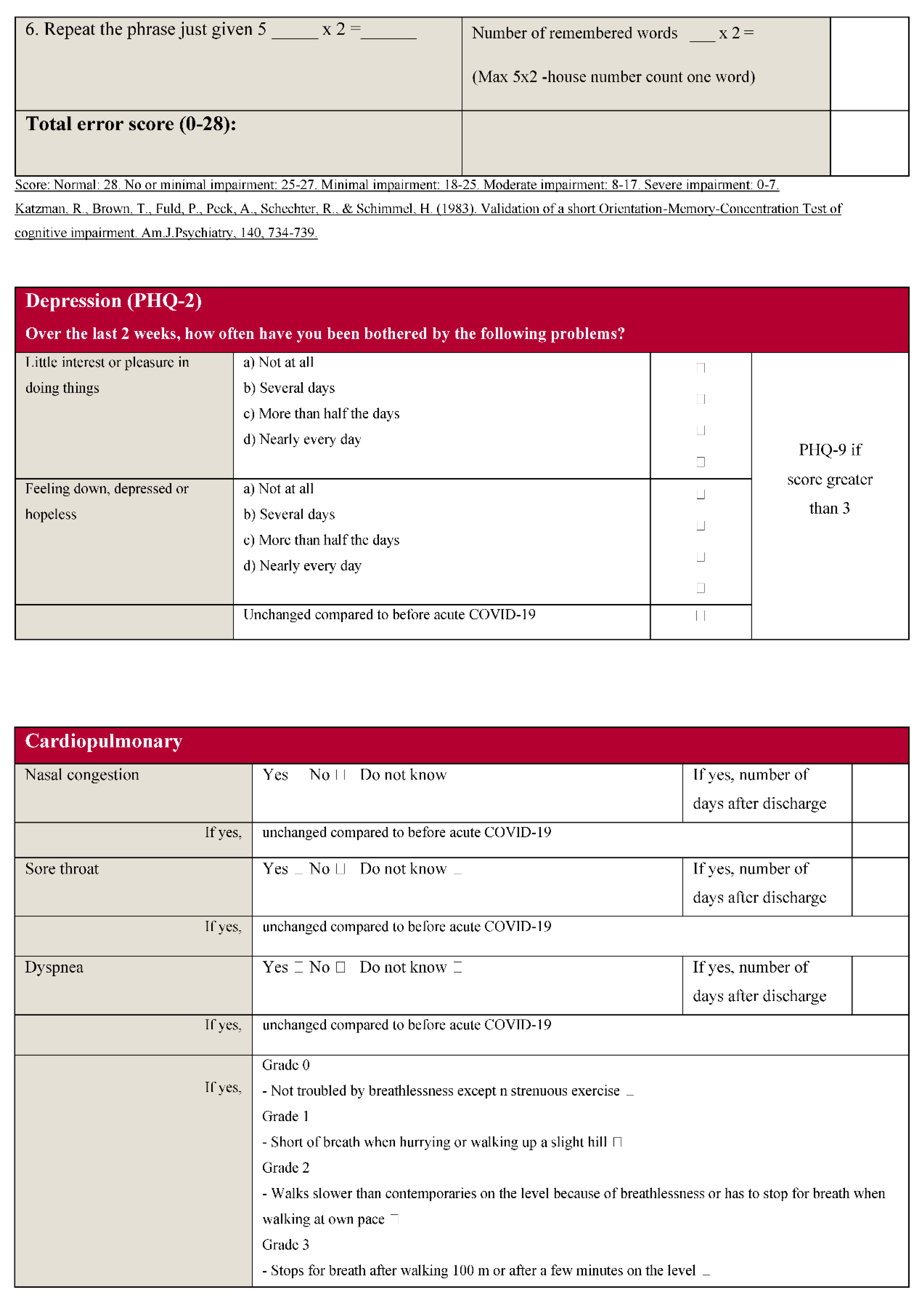
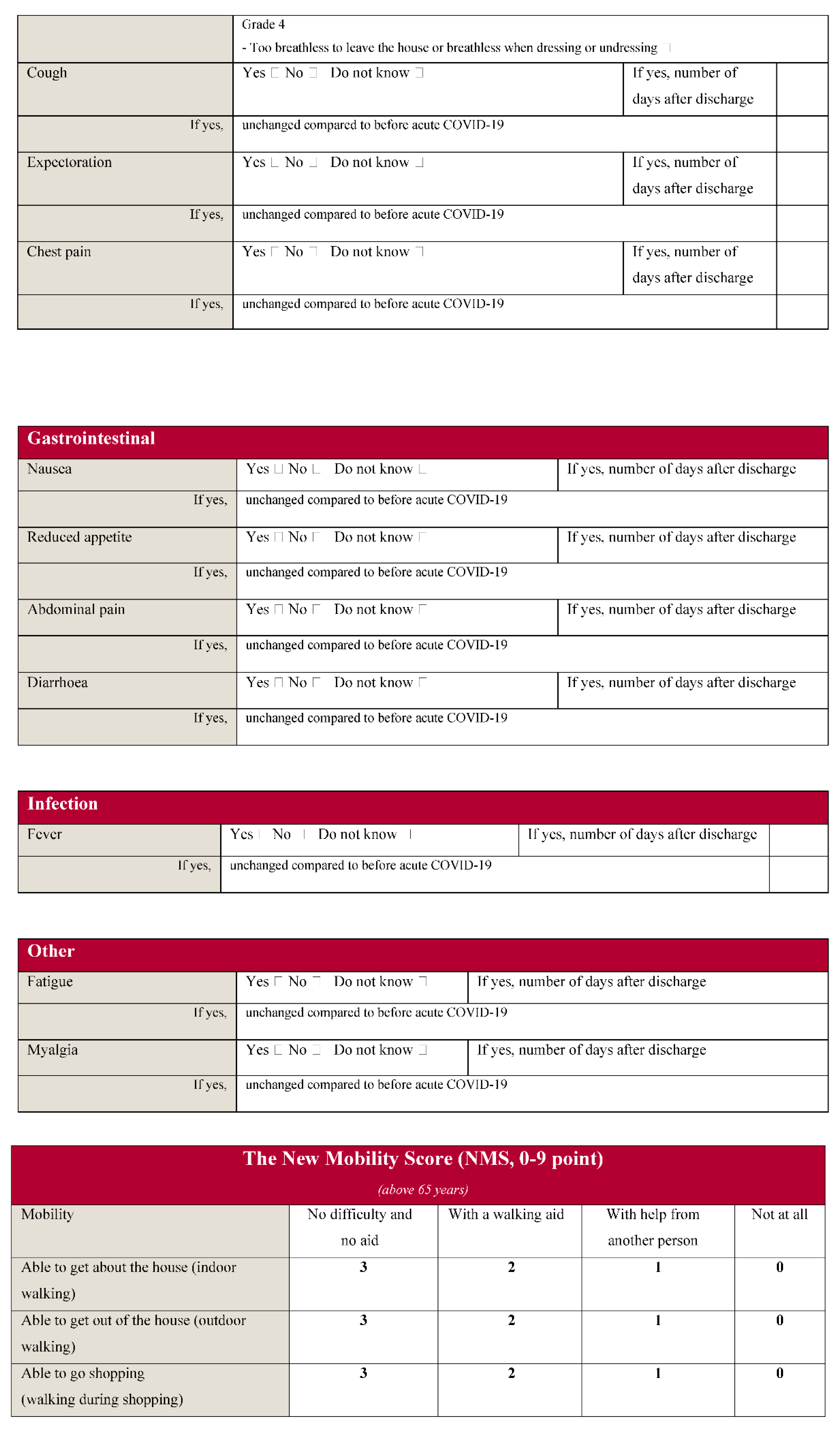
Appendix A





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Total (n = 45) | |
|---|---|
| Age, years (Median (IQR)) | 57 (51–70) |
| Sex (No (%)) | |
| Men | 21 (47) |
| Women | 24 (53) |
| BMI (Median (IQR)) | 28.10 (24.8–32.6) |
| Ethnicity (No (%)) | |
| Caucasian | 39 (87) |
| African | 4 (9) |
| Middle Eastern | 2 (4) |
| Smoking status (No (%)) | |
| Never-smoker | 27 (60) |
| Previous smoker | 14 (31) |
| Active smoker | 4 (9) |
| Received oxygen therapy during admission (No (%)) | 33 (73) |
| Received steroid medicine during admission (No (%)) 1 | 8 (18) |
| Comorbidities (No (%)) | |
| Any | 28 (62) |
| Hypertension | 13 (29) |
| Asthma | 4 (9) |
| Coronary heart disease | 4 (9) |
| Malignancy | 4 (9) |
| Chronic obstructive pulmonary disease | 3 (7) |
| Transplanted | 1 (2) |
| Other | 12 (31) |
| Inflammatory diseases | 6 |
| Hypercholesterolemia | 3 |
| Arthritis urica | 1 |
| Psoriasis | 1 |
| Hypothyroidism | 1 |
| Length of hospital stay, days (Median (IQR)) | 7 (3–12) |
| ICU admission (No (%)) | 8 (18) |
| Time from symptom onset to admission, days (Median (IQR)) | 8 (5–10) |
| Time from discharge to 48-week follow-up (Median (IQR)) | 350 (341–380) |
| 1 Steroid treatment was given on other indications than COVID-19 | |
| COVID-19 related symptoms at 48 weeks | Symptoms lasting 48 weeks or more after discharge |
| No. of patients (%) | |
| Total | 45 |
| Cognitive assessment | |
| Concentrating difficulties | 18 (40) |
| Impaired OMC test | 11 (24) |
| Central- and peripheral nervous system (C-/PNS) | |
| Headache | 10 (22) |
| Paresthesia | 12 (27) |
| Smell impairment | 11 (24) |
| Taste impairment | 11 (24) |
| ≥1 symptom(s) from the C-/PNS | 14 (31) |
| Cardiopulmonary system (CPS) | |
| Dyspnea | 18 (40) |
| Severe dyspnea | 5 (28 *) |
| Cough | 13 (29) |
| Expectoration | 9 (20) |
| Chest pain | 4 (9) |
| Nasal congestion | 3 (7) |
| Sore throat | 8 (18) |
| ≥1 symptom(s) from the CPS | 28 (62) |
| Gastrointestinal system (GIS) | |
| Reduced appetite | 7 (16) |
| Nausea | 7 (16) |
| Abdominal pain | 4 (9) |
| Altered bowel habits | 6 (13) |
| ≥1 symptom(s) from the GIS | 12 (27) |
| Other | |
| Fatigue | 27 (60) |
| Myalgia | 12 (27) |
| Joint pain | 10 (22) |
| Fever episode since discharge | 7 (16) |
| All | |
| ≥1 of any kind of symptom(s) | 39 (87) |
| Test of Risk Factors for Symptoms Reported after 48 Weeks | ||||
| Fatigue | Odds Ratio | p-value | 95% confidence interval | |
| Female sex | 3.66 | 0.084 | 0.84 | 15.92 |
| Other ethnicity than Caucasian | 0.061 | 0.027 | 0.0051 | 0.72 |
| Age ≥60 years | 0.87 | 0.867 | 0.18 | 4.23 |
| BMI ≥25 kg/m2 | 2.19 | 0.337 | 0.44 | 10.87 |
| Having a comorbidity | 0.73 | 0.71 | 0.14 | 3.78 |
| Receiving oxygen therapy | 0.80 | 0.74 | 0.13 | 4.88 |
| Dyspnea | Odds Ratio | p-value | 95% confidence interval | |
| Female sex | 1.33 | 0.67 | 0.43 | 6.24 |
| Other ethnicity than Caucasian | 0.88 | 0.89 | 0.14 | 8.12 |
| Age >60 years | 1.92 | 0.81 | 0.22 | 4.45 |
| BMI >25 kg/m2 | 2.30 | 0.30 | 0.37 | 8.20 |
| Having a comorbidity | 1.38 | 0.67 | 0.41 | 9.97 |
| Receiving oxygen therapy | 4.13 | 0.12 | 0.68 | 25.02 |
| Difficulties concentrating | Odds Ratio | p-value | 95% confidence interval | |
| Female sex | 4.06 | 0.07 | 0.89 | 18.47 |
| Other ethnicity than Caucasian | 0.15 | 0.15 | 0.011 | 2.00 |
| Age >60 years | 0.55 | 0.50 | 0.097 | 3.14 |
| BMI >25 kg/m2 | 0.45 | 0.37 | 0.078 | 2.62 |
| Having a comorbidity | 0.22 | 0.075 | 0.043 | 1.16 |
| Receiving oxygen therapy | 1.57 | 0.63 | 0.08 | 9.79 |
References
- Mølhave, M. Clinical Management of COVID-19 Patients—An Update. Semin. Nucl. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Yao, Q.; Gu, X.; Wang, Q.; Ren, L.; Wang, Y.; Hu, P.; Guo, L.; Liu, M.; Xu, J.; et al. 1-year outcomes in hospital survivors with COVID-19: A longitudinal cohort study. Lancet 2021, 398, 747–758. [Google Scholar] [CrossRef]
- Augustin, M.; Schommers, P.; Stecher, M. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health—Eur. 2021, 6, 100122. [Google Scholar] [CrossRef]
- Xiong, Q.; Xu, M.; Li, J.; Liu, Y.; Zhang, J.; Xu, Y.; Dong, W. Clinical sequelae of COVID-19 survivors in Wuhan, China: A single-centre longitudinal study. Clin. Microbiol. Infect. 2020, 27, 89–95. [Google Scholar] [CrossRef] [PubMed]
- García-Abellán, J.; Padilla, S.; Fernández-González, M. Antibody Response to SARS-CoV-2 is Associated with Long-term Clinical Outcome in Patients with COVID-19: A Longitudinal Study. J. Clin. Immunol. 2021, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Townsend, L.; Dyer, A.H.; Jones, K.; Dunne, J.; Mooney, A.; Gaffney, F.; O’Connor, L.; Leavy, D.; O’Brien, K.; Dowds, J.; et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS ONE 2020, 15, e0240784. [Google Scholar] [CrossRef] [PubMed]
- Moreno-Pérez, O.; Merino, E.; Leon-Ramirez, J.-M.; Andres, M.; Ramos, J.M.; Arenas-Jiménez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef] [PubMed]
- Leth, S.; Gunst, J.D.; Mathiasen, V.; Hansen, K.; Søgaard, O.; Østergaard, L.; Jensen-Fangel, S.; Storgaard, M.; Agergaard, J. Persistent Symptoms in Patients Recovering From COVID-19 in Denmark. Open Forum Infect. Dis. 2021, 8, ofab042. [Google Scholar] [CrossRef] [PubMed]
- Bourgonje, A.R.; Abdulle, A.E.; Timens, W.; Hillebrands, J.; Navis, G.J.; Gordijn, S.J.; Bolling, M.C.; Dijkstra, G.; Voors, A.A.; Osterhaus, A.D.M.E.; et al. Angiotensin-converting enzyme 2 (ACE2), SARS-CoV-2 and the pathophysiology of coronavirus disease 2019 (COVID-19). J. Pathol. 2020, 251, 228–248. [Google Scholar] [CrossRef] [PubMed]
- Logue, J.K.; Franko, N.M.; McCulloch, D.J.; McDonald, D.; Magedson, A.; Wolf, C.R.; Chu, H.Y. Sequelae in Adults at 6 Months After COVID-19 Infection. JAMA Netw. Open 2021, 4, e210830. [Google Scholar] [CrossRef] [PubMed]
- Agergaard, J.; Th, P.; Pedersen, T.; Harbo, T.; Blicher, J.; Karlsson, P.; Østergaard, L.; Andersen, H.; Tankisi, H. Myopathic changes in patients with long-term fatigue after COVID-19. Clin. Neurophysiol. 2021, 132, 1974–1981. [Google Scholar] [CrossRef] [PubMed]
- Ayoubkhani, D.; Bosworth, M. Prevalence of Ongoing Symptoms Following Coronavirus (COVID-19) Infection in the UK—Office for National Statistics. Available online: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/prevalenceofongoingsymptomsfollowingcoronaviruscovid19infectionintheuk/4november2021 (accessed on 14 November 2021).
- Yomogida, K.; Zhu, S.; Rubino, F.; Figueroa, W.; Balanji, N.; Holman, E. Post-Acute Sequelae of SARS-CoV-2 Infection Among Adults Aged ≥ 18 Years—Long Beach, California, 1 April–10 December 2020. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1274–1277. [Google Scholar] [CrossRef] [PubMed]
- Barsky, A.J.; Peekna, H.M.; Borus, J.F. Somatic symptom reporting in women and men. J. Gen. Intern. Med. 2001, 16, 266–275. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takahashi, T.; Ellingson, M.K.; Wong, P.; Israelow, B.; Lucas, C.; Klein, J.; Silva, J.; Mao, T.; Oh, J.E.; Tokuyama, M.; et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature 2020, 588, 315–320. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mølhave, M.; Leth, S.; Gunst, J.D.; Jensen-Fangel, S.; Østergaard, L.; Wejse, C.; Agergaard, J. Long-Term Symptoms among Hospitalized COVID-19 Patients 48 Weeks after Discharge—A Prospective Cohort Study. J. Clin. Med. 2021, 10, 5298. https://doi.org/10.3390/jcm10225298
Mølhave M, Leth S, Gunst JD, Jensen-Fangel S, Østergaard L, Wejse C, Agergaard J. Long-Term Symptoms among Hospitalized COVID-19 Patients 48 Weeks after Discharge—A Prospective Cohort Study. Journal of Clinical Medicine. 2021; 10(22):5298. https://doi.org/10.3390/jcm10225298
Chicago/Turabian StyleMølhave, Martin, Steffen Leth, Jesper Damsgaard Gunst, Søren Jensen-Fangel, Lars Østergaard, Christian Wejse, and Jane Agergaard. 2021. "Long-Term Symptoms among Hospitalized COVID-19 Patients 48 Weeks after Discharge—A Prospective Cohort Study" Journal of Clinical Medicine 10, no. 22: 5298. https://doi.org/10.3390/jcm10225298