
The Role of Multimodality Imaging in Athlete’s Heart Diagnosis: Current Status and Future Directions

 , , , ,
, , , ,  , , and
, , and
Abstract
:1. Introduction
2. Clinical and Electrocardiographic Evaluation
3. Echocardiography
3.1. Exercise Stress Echocardiography
3.2. New Echocardiographic Technologies
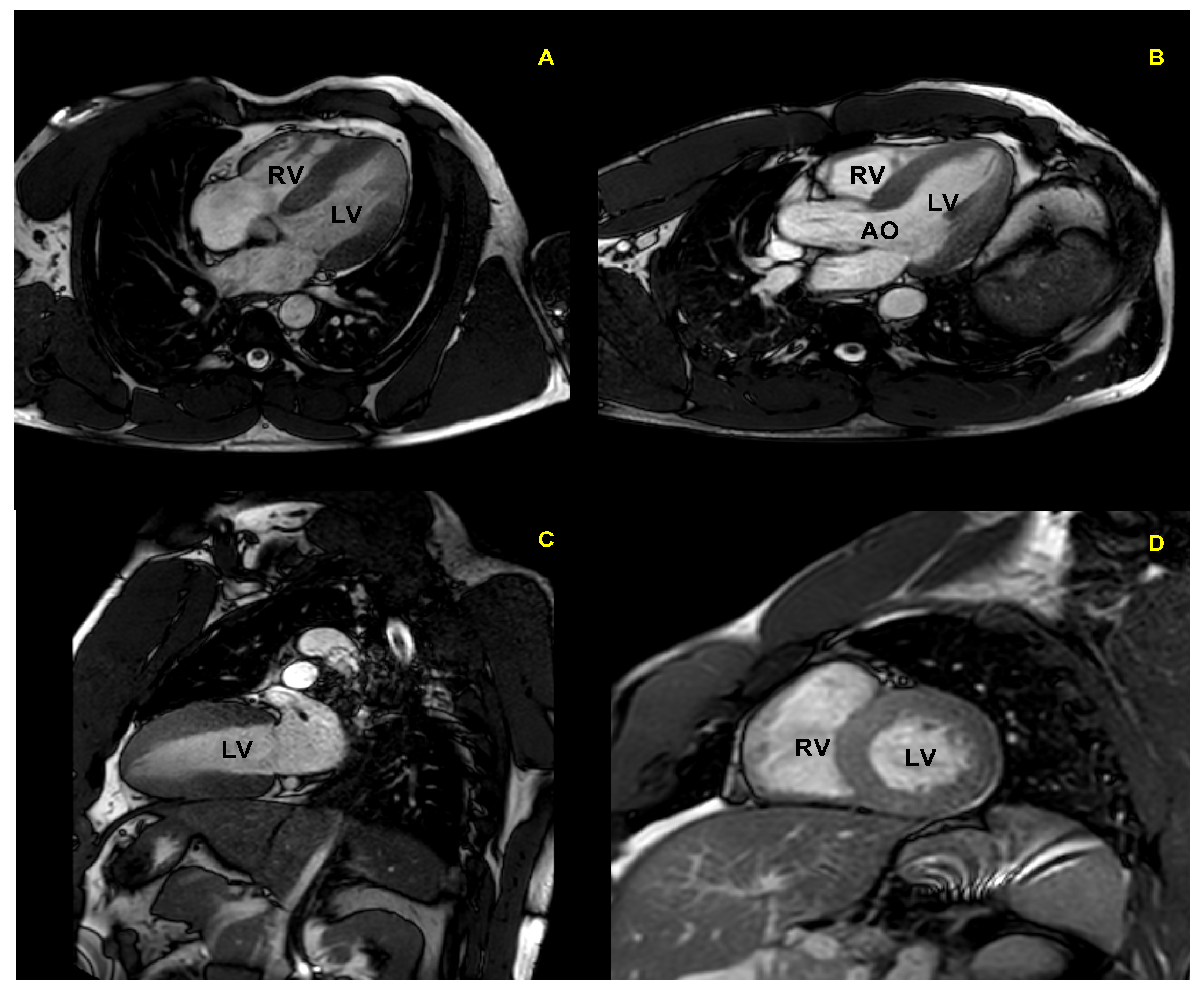
4. Cardiac Magnetic Resonance
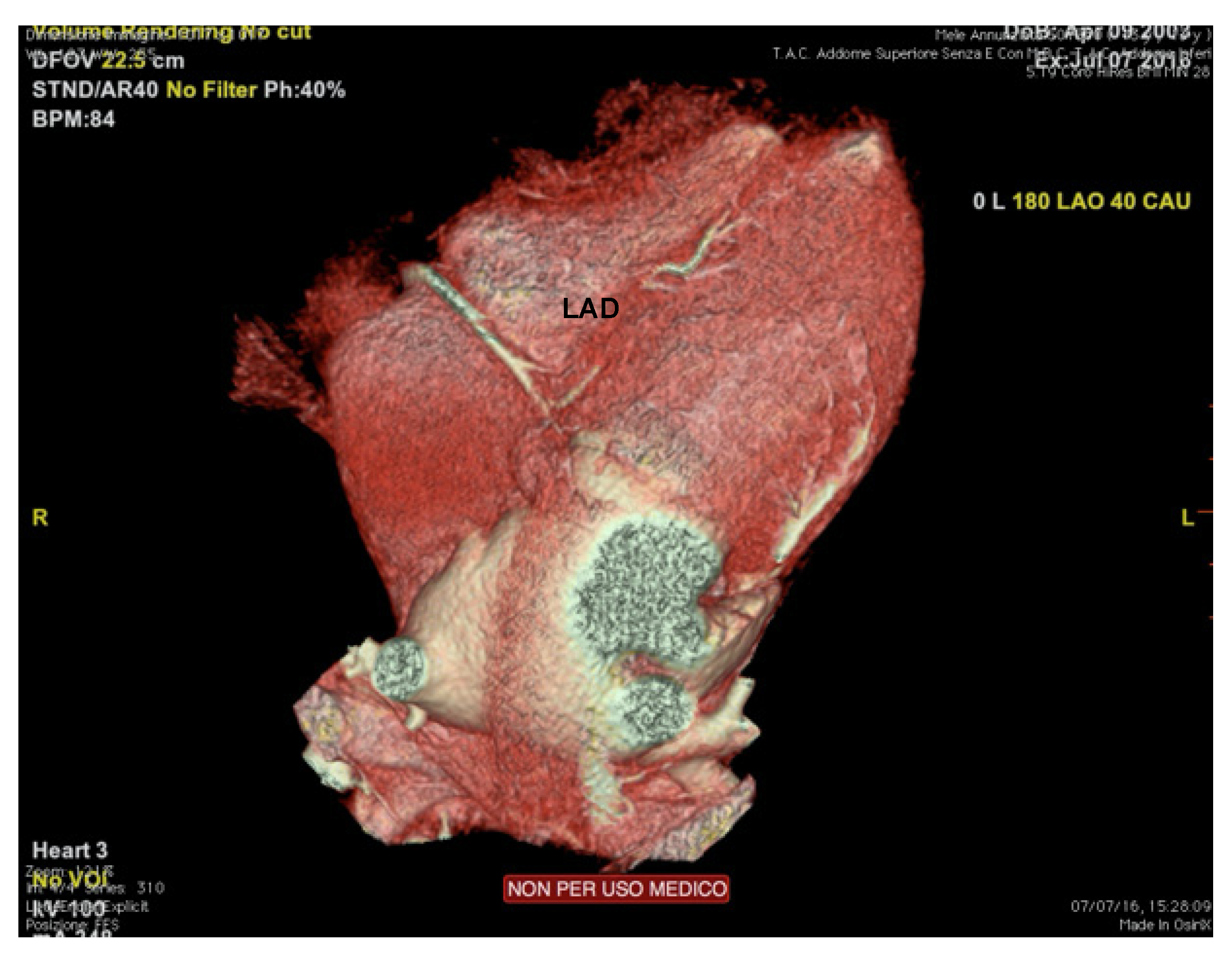
5. Cardiac Computed Tomography and Other Imaging Modalities
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Pelliccia, A.; Caselli, S.; Sharma, S.; Basso, C.; Bax, J.J.; Corrado, D.; D’Andrea, A.; D’Ascenzi, F.; Di Paolo, F.M.; Edvardsen, T.; et al. Internal reviewers for EAPC and EACVI. European Association of Preventive Cardiology (EAPC) and European Association of Cardiovascular Imaging (EACVI) joint position statement: Recommendations for the indication and interpretation of cardiovascular imaging in the evaluation of the athlete’s heart. Eur. Heart J. 2018, 39, 1949–1969. [Google Scholar] [CrossRef] [PubMed]
- Galderisi, M.; Cardim, N.; D’Andrea, A.; Bruder, O.; Cosyns, B.; Davin, L.; Donal, E.; Edvardsen, T.; Freitas, A.; Habib, G.; et al. The multi-modality cardiac imaging approach to the Athlete’s heart: An expert consensus of the European Association of Cardiovascular Imaging. Eur. Hear. J. Cardiovasc. Imaging 2015, 16, 353–353r. [Google Scholar] [CrossRef] [PubMed]
- Radmilovic, J.; D’Andrea, A.; D’Amato, A.; Tagliamonte, E.; Sperlongano, S.; Riegler, L.; Scarafile, R.; Forni, A.; Muscogiuri, G.; Pontone, G.; et al. Echocardiography in Athletes in Primary Prevention of Sudden Death. J. Cardiovasc. Echogr. 2019, 29, 139–148. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Mele, D.; Palermi, S.; Rizzo, M.; Campana, M.; Di Giannuario, G.; Gimelli, A.; Khoury, G.; Moreo, A. A nome dell’Area Cardioimaging dell’Associazione Nazionale Medici Cardiologi Ospedalieri (ANMCO). Le “zone grigie” degli adattamenti cardiovascolari all’esercizio fisico: Come orientarsi nella valutazione ecocardiografica del cuore d’atleta [Grey zones in cardiovascular adaptations to physical exercise: How to navigate in the echocardiographic evaluation of the athlete’s heart]. G. Ital. Cardiol. 2020, 21, 457–468. (In Italian) [Google Scholar] [CrossRef] [PubMed]
- Sharma, S.; Drezner, J.A.; Baggish, A.; Papadakis, M.; Wilson, M.; Prutkin, J.M.; La Gerche, A.; Ackerman, M.J.; Borjesson, M.; Salerno, J.C.; et al. International Recommendations for Electrocardiographic Interpretation in Athletes. J. Am. Coll. Cardiol. 2017, 69, 1057–1075. [Google Scholar] [CrossRef]
- Corrado, D.; Pelliccia, A.; Heidbuchel, H.; Sharma, S.; Link, M.; Basso, C.; Biffi, A.; Buja, G.; Delise, P.; Gussac, I.; et al. Recommendations for interpretation of 12-lead electrocardiogram in the athlete. Eur. Hear. J. 2009, 31, 243–259. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Ascenzi, F.; Anselmi, F.; Mondillo, S.; Finocchiaro, G.; Caselli, S.; La Garza, M.S.-D.; Schmied, C.; Adami, P.E.; Galderisi, M.; Adler, Y.; et al. The use of cardiac imaging in the evaluation of athletes in the clinical practice: A survey by the Sports Cardiology and Exercise Section of the European Association of Preventive Cardiology and University of Siena, in collaboration with the European Association of Cardiovascular Imaging, the European Heart Rhythm Association and the ESC Working Group on Myocardial and Pericardial Diseases. Eur. J. Prev. Cardiol. 2020, 28, 1071–1077. [Google Scholar] [CrossRef]
- Niederseer, D.; Rossi, V.A.; Kissel, C.; Scherr, J.; Caselli, S.; Tanner, F.C.; Bohm, P.; Schmied, C. Role of echocardiography in screening and evaluation of athletes. Heart 2020, 107, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Palermi, S.; Serio, A.; Vecchiato, M.; Sirico, F.; Gambardella, F.; Ricci, F.; Iodice, F.; Radmilovic, J.; Russo, V.; D’Andrea, A. Potential role of an athlete-focused echocardiogram in sports eligibility. World J. Cardiol. 2021, 13, 271–297. [Google Scholar] [CrossRef]
- Pelliccia, A.; Maron, B.J.; De Luca, R.; Di Paolo, F.M.; Spataro, A.; Culasso, F. Remodeling of Left Ventricular Hypertrophy in Elite Athletes After Long-Term Deconditioning. Circulation 2002, 105, 944–949. [Google Scholar] [CrossRef] [Green Version]
- Pelliccia, A.; Maron, B.J.; Spataro, A.; Proschan, M.A.; Spirito, P. The Upper Limit of Physiologic Cardiac Hypertrophy in Highly Trained Elite Athletes. N. Engl. J. Med. 1991, 324, 295–301. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzi, F.; Pisicchio, C.; Caselli, S.; Di Paolo, F.M.; Spataro, A.; Pelliccia, A. RV Remodeling in Olympic Athletes. JACC Cardiovasc. Imaging 2017, 10, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.; Ghani, S.; Sharma, R.; Oxborough, D.; Panoulas, V.F.; Sheikh, N.; Gati, S.; Papadakis, M.; Sharma, S. Physiological Right Ventricular Adaptation in Elite Athletes of African and Afro-Caribbean Origin. Circulation 2013, 127, 1783–1792. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; La Gerche, A.; Golia, E.; Teske, A.J.; Bossone, E.; Russo, M.G.; Calabrò, R.; Baggish, A.L. Right Heart Structural and Functional Remodeling in Athletes. Echocardiography 2014, 32, S11–S22. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Maron, B.J.; Di Paolo, F.M.; Biffi, A.; Quattrini, F.M.; Pisicchio, C.; Roselli, A.; Caselli, S.; Culasso, F. Prevalence and Clinical Significance of Left Atrial Remodeling in Competitive Athletes. J. Am. Coll. Cardiol. 2005, 46, 690–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; Riegler, L.; Cocchia, R.; Scarafile, R.; Salerno, G.; Gravino, R.; Golia, E.; Vriz, O.; Citro, R.; Limongelli, G.; et al. Left atrial volume index in highly trained athletes. Am. Hear. J. 2010, 159, 1155–1161. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Di Paolo, F.M.; Pisicchio, C.; Di Pietro, R.; Quattrini, F.M.; Di Giacinto, B.; Culasso, F.; Pelliccia, A. Three-Dimensional Echocardiographic Characterization of Left Ventricular Remodeling in Olympic Athletes. Am. J. Cardiol. 2011, 108, 141–147. [Google Scholar] [CrossRef]
- Pluim, B.M.; Zwinderman, A.H.; van der Laarse, A.; van der Wall, E.E. The Athlete’s Heart. Circulation 2000, 101, 336–344. [Google Scholar] [CrossRef] [Green Version]
- D’Andrea, A.; Riegler, L.; Golia, E.; Cocchia, R.; Scarafile, R.; Salerno, G.; Pezzullo, E.; Nunziata, L.; Citro, R.; Cuomo, S.; et al. Range of right heart measurements in top-level athletes: The training impact. Int. J. Cardiol. 2013, 164, 48–57. [Google Scholar] [CrossRef]
- Caselli, S.; Di Paolo, F.M.; Pisicchio, C.; Pandian, N.G.; Pelliccia, A. Patterns of Left Ventricular Diastolic Function in Olympic Athletes. J. Am. Soc. Echocardiogr. 2015, 28, 236–244. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, A.; Limongelli, G.; Caso, P.; Sarubbi, B.; Della Pietra, A.; Brancaccio, P.; Cice, G.; Scherillo, M.; Limongelli, F.; Calabrò, R. Association between left ventricular structure and cardiac performance during effort in two morphological forms of athlete’s heart. Int. J. Cardiol. 2002, 86, 177–184. [Google Scholar] [CrossRef]
- Cardim, N.; Oliveira, A.; Longo, S.; Ferreira, T.; Pereira, A.; Reis, R.P.; Correia, J.M. Doppler tissue imaging: Regional myocardial function in hypertrophic cardiomyopathy and in athlete’s heart. J. Am. Soc. Echocardiogr. 2003, 16, 223–232. [Google Scholar] [CrossRef] [PubMed]
- Vinereanu, D.; Florescu, N.; Sculthorpe, N.; Tweddel, A.C.; Stephens, M.R.; Fraser, A.G. Differentiation between pathologic and physiologic left ventricular hypertrophy by tissue doppler assessment of long-axis function in patients with hypertrophic cardiomyopathy or systemic hypertension and in athletes. Am. J. Cardiol. 2001, 88, 53–58. [Google Scholar] [CrossRef]
- D’Andrea, A.; Cocchia, R.; Riegler, L.; Scarafile, R.; Salerno, G.; Gravino, R.; Golia, E.; Pezzullo, E.; Citro, R.; Limongelli, G.; et al. Left Ventricular Myocardial Velocities and Deformation Indexes in Top-Level Athletes. J. Am. Soc. Echocardiogr. 2010, 23, 1281–1288. [Google Scholar] [CrossRef] [PubMed]
- Pelliccia, A.; Di Paolo, F.M.; De Blasiis, E.; Quattrini, F.M.; Pisicchio, C.; Guerra, E.; Culasso, F.; Maron, B.J. Prevalence and Clinical Significance of Aortic Root Dilation in Highly Trained Competitive Athletes. Circulation 2010, 122, 698–706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- D’Andrea, A.; Cocchia, R.; Riegler, L.; Scarafile, R.; Salerno, G.; Gravino, R.; Vriz, O.; Citro, R.; Limongelli, G.; Di Salvo, G.; et al. Aortic Root Dimensions in Elite Athletes. Am. J. Cardiol. 2010, 105, 1629–1634. [Google Scholar] [CrossRef] [PubMed]
- Iskandar, A.; Thompson, P.D. A Meta-Analysis of Aortic Root Size in Elite Athletes. Circulation 2013, 127, 791–798. [Google Scholar] [CrossRef] [Green Version]
- Spirito, P.; Pelliccia, A.; Proschan, M.A.; Granata, M.; Spataro, A.; Bellone, P.; Caselli, G.; Biffi, A.; Vecchio, C.; Maron, B.J. Morphology of the “athlete’s heart” assessed by echocardiography in 947 elite athletes representing 27 sports. Am. J. Cardiol. 1994, 74, 802–806. [Google Scholar] [CrossRef]
- Haugaa, K.H.; Basso, C.; Badano, L.P.; Bucciarelli-Ducci, C.; Cardim, N.; Gaemperli, O.; Galderisi, M.; Habib, G.; Knuuti, J.; Lancellotti, P.; et al. Comprehensive multi-modality imaging approach in arrhythmogenic cardiomyopathy—An expert consensus document of the European Association of Cardiovascular Imaging. Eur. Hear. J. Cardiovasc. Imaging 2017, 18, 237–253. [Google Scholar] [CrossRef] [Green Version]
- Marcus, F.I.; McKenna, W.J.; Sherrill, D.; Basso, C.; Bauce, B.; Bluemke, D.A.; Calkins, H.; Corrado, D.; Cox, M.G.; Daubert, J.P.; et al. Diagnosis of arrhythmogenic right ventricular cardiomyopathy/dysplasia: Proposed Modification of the Task Force Criteria. Eur. Hear. J. 2010, 31, 806–814. [Google Scholar] [CrossRef] [Green Version]
- Claessen, G.; La Gerche, A.; Voigt, J.-U.; Dymarkowski, S.; Schnell, F.; Petit, T.; Willems, R.; Claus, P.; Delcroix, M.; Heidbuchel, H. Accuracy of Echocardiography to Evaluate Pulmonary Vascular and RV Function During Exercise. JACC Cardiovasc. Imaging 2016, 9, 532–543. [Google Scholar] [CrossRef] [PubMed]
- Lancellotti, P.; Pellikka, P.A.; Budts, W.; Chaudhry, F.A.; Donal, E.; Dulgheru, R.; Edvardsen, T.; Garbi, M.; Ha, J.-W.; Kane, G.C.; et al. The clinical use of stress echocardiography in non-ischaemic heart disease: Recommendations from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. Eur. Hear. J. Cardiovasc. Imaging 2016, 17, 1191–1229. [Google Scholar] [CrossRef] [Green Version]
- Millar, L.M.; Fanton, Z.; Finocchiaro, G.; Sanchez-Fernandez, G.; Dhutia, H.; Malhotra, A.; Merghani, A.; Papadakis, M.; Behr, E.R.; Bunce, N.; et al. Differentiation between athlete’s heart and dilated cardiomyopathy in athletic individuals. Heart 2020, 106, 1059–1065. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzi, F.; Caselli, S.; Solari, M.; Pelliccia, A.; Cameli, M.; Focardi, M.; Padeletti, M.; Corrado, D.; Bonifazi, M.; Mondillo, S. Novel echocardiographic techniques for the evaluation of athletes’ heart: A focus on speckle-tracking echocardiography. Eur. J. Prev. Cardiol. 2015, 23, 437–446. [Google Scholar] [CrossRef] [PubMed]
- Cappelli, F.; Toncelli, L.; Cappelli, B.; De Luca, A.; Stefani, L.; Maffulli, N.; Galanti, G. Adaptative or maladaptative hypertrophy, different spatial distribution of myocardial contraction. Clin. Physiol. Funct. Imaging 2010, 30, 6–12. [Google Scholar] [CrossRef] [PubMed]
- Caselli, S.; Montesanti, D.; Autore, C.; Di Paolo, F.M.; Pisicchio, C.; Squeo, M.R.; Musumeci, B.; Spataro, A.; Pandian, N.G.; Pelliccia, A. Patterns of Left Ventricular Longitudinal Strain and Strain Rate in Olympic Athletes. J. Am. Soc. Echocardiogr. 2015, 28, 245–253. [Google Scholar] [CrossRef]
- Galderisi, M.; Lomoriello, V.S.; Santoro, A.; Esposito, R.; Olibet, M.; Raia, R.; Di Minno, M.; Guerra, G.; Mele, D.; Lombardi, G. Differences of Myocardial Systolic Deformation and Correlates of Diastolic Function in Competitive Rowers and Young Hypertensives: A Speckle-Tracking Echocardiography Study. J. Am. Soc. Echocardiogr. 2010, 23, 1190–1198. [Google Scholar] [CrossRef] [PubMed]
- Nottin, S.; Doucende, G.; Schuster-Beck, I.; Dauzat, M.; Obert, P. Alteration in left ventricular normal and shear strains evaluated by 2D-strain echocardiography in the athlete’s heart. J. Physiol. 2008, 586, 4721–4733. [Google Scholar] [CrossRef]
- Simsek, Z.; Tas, M.H.; Degirmenci, H.; Yazıcı, A.G.; Ipek, E.; Duman, H.; Gundogdu, F.; Karakelleoglu, S.; Senocak, H. Speckle Tracking Echocardiographic Analysis of Left Ventricular Systolic and Diastolic Functions of Young Elite Athletes with Eccentric and Concentric Type of Cardiac Remodeling. Echocardiography 2013, 30, 1202–1208. [Google Scholar] [CrossRef] [PubMed]
- Soullier, C.; Obert, P.; Doucende, G.; Nottin, S.; Cade, S.; Perez-Martin, A.; Messner-Pellenc, P.; Schuster, I. Exercise Response in Hypertrophic Cardiomyopathy. Circ. Cardiovasc. Imaging 2012, 5, 324–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Weiner, R.B.; Hutter, A.M.; Wang, F.; Kim, J.; Weyman, A.E.; Wood, M.J.; Picard, M.; Baggish, A.L. The Impact of Endurance Exercise Training on Left Ventricular Torsion. JACC: Cardiovasc. Imaging 2010, 3, 1001–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butz, T.; Van Buuren, F.; Mellwig, K.-P.; Langer, C.; Plehn, G.; Meissner, A.; Trappe, H.-J.; Horstkotte, D.; Faber, L. Two-dimensional strain analysis of the global and regional myocardial function for the differentiation of pathologic and physiologic left ventricular hypertrophy: A study in athletes and in patients with hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 2010, 27, 91–100. [Google Scholar] [CrossRef] [PubMed]
- Stefani, L.; Pedrizzetti, G.; De Luca, A.; Mercuri, R.; Innocenti, G.; Galanti, G. Real-time evaluation of longitudinal peak systolic strain (speckle tracking measurement) in left and right ventricles of athletes. Cardiovasc. Ultrasound 2009, 7, 17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oxborough, D.; Sharma, S.; Shave, R.; Whyte, G.; Birch, K.; Artis, N.; Batterham, A.M.; George, K. The Right Ventricle of the Endurance Athlete: The Relationship between Morphology and Deformation. J. Am. Soc. Echocardiogr. 2012, 25, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Teske, A.J.; Prakken, N.H.; De Boeck, B.W.; Velthuis, B.K.; Martens, E.P.; Doevendans, P.A.; Cramer, M.J. Echocardiographic tissue deformation imaging of right ventricular systolic function in endurance athletes. Eur. Hear. J. 2008, 30, 969–977. [Google Scholar] [CrossRef] [Green Version]
- Bauce, B.; Frigo, G.; Benini, G.; Michieli, P.; Basso, C.; Folino, A.F.; Rigato, I.; Mazzotti, E.; Daliento, L.; Thiene, G.; et al. Differences and similarities between arrhythmogenic right ventricular cardiomyopathy and athlete’s heart adaptations. Br. J. Sports Med. 2008, 44, 148–154.e1. [Google Scholar] [CrossRef] [PubMed]
- La Gerche, A.; Burns, A.T.; D’Hooge, J.; MacIsaac, A.I.; Heidbüchel, H.; Prior, D.L. Exercise Strain Rate Imaging Demonstrates Normal Right Ventricular Contractile Reserve and Clarifies Ambiguous Resting Measures in Endurance Athletes. J. Am. Soc. Echocardiogr. 2012, 25, 253–262. [Google Scholar] [CrossRef]
- Pagourelias, E.D.; Kouidi, E.; Efthimiadis, G.K.; Deligiannis, A.; Geleris, P.; Vassilikos, V. Right Atrial and Ventricular Adaptations to Training in Male Caucasian Athletes: An Echocardiographic Study. J. Am. Soc. Echocardiogr. 2013, 26, 1344–1352. [Google Scholar] [CrossRef]
- Esposito, R.; Galderisi, M.; M.D., V.S.; M.D., A.S.; De Palma, D.; Ippolito, R.; M.D., R.M.; Santoro, C.; Guerra, G.; Cameli, M.; et al. Nonsymmetric Myocardial Contribution to Supranormal Right Ventricular Function in the Athlete’s Heart: Combined Assessment by Speckle Tracking and Real Time Three-Dimensional Echocardiography. Echocardiography 2013, 31, 996–1004. [Google Scholar] [CrossRef] [PubMed]
- Oxborough, D.; Shave, R.; Warburton, D.; Williams, K.; Oxborough, A.; Charlesworth, S.; Foulds, H.; Hoffman, M.D.; Birch, K.; George, K. Dilatation and Dysfunction of the Right Ventricle Immediately After Ultraendurance Exercise. Circ. Cardiovasc. Imaging 2011, 4, 253–263. [Google Scholar] [CrossRef] [PubMed]
- Teske, A.J.; Cox, M.G.; De Boeck, B.W.; Doevendans, P.A.; Hauer, R.N.; Cramer, M.J. Echocardiographic Tissue Deformation Imaging Quantifies Abnormal Regional Right Ventricular Function in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy. J. Am. Soc. Echocardiogr. 2009, 22, 920–927. [Google Scholar] [CrossRef]
- Paraskevaidis, I.A.; Panou, F.; Papadopoulos, C.; Farmakis, D.; Parissis, J.; Ikonomidis, I.; Rigopoulos, A.; Iliodromitis, E.K.; Kremastinos, D.T. Evaluation of left atrial longitudinal function in patients with hypertrophic cardiomyopathy: A tissue Doppler imaging and two-dimensional strain study. Heart 2008, 95, 483–489. [Google Scholar] [CrossRef]
- Roşca, M.; Popescu, B.A.; Beladan, C.C.; Călin, A.; Muraru, D.; Popa, E.C.; Lancellotti, P.; Enache, R.; Coman, I.M.; Jurcuţ, R.; et al. Left Atrial Dysfunction as a Correlate of Heart Failure Symptoms in Hypertrophic Cardiomyopathy. J. Am. Soc. Echocardiogr. 2010, 23, 1090–1098. [Google Scholar] [CrossRef] [PubMed]
- Gabrielli, L.; Enríquez, A.; Córdova, S.; Yáñez, F.; Godoy, I.; Corbalán, R. Assessment of left atrial function in hypertrophic cardiomyopathy and athlete’s heart: A left atrial myocardial deformation study. Echocardiography 2012, 29, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Russell, K.; Eriksen, M.; Aaberge, L.; Wilhelmsen, N.; Skulstad, H.; Remme, E.W.; Haugaa, K.; Opdahl, A.; Fjeld, J.G.; Gjesdal, O.; et al. A novel clinical method for quantification of regional left ventricular pressure–strain loop area: A non-invasive index of myocardial work. Eur. Hear. J. 2012, 33, 724–733. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mele, D.; Smarrazzo, V.; Pedrizzetti, G.; Capasso, F.; Pepe, M.; Severino, S.; Luisi, G.A.; Maglione, M.; Ferrari, R. Intracardiac Flow Analysis: Techniques and Potential Clinical Applications. J. Am. Soc. Echocardiogr. 2019, 32, 319–332. [Google Scholar] [CrossRef]
- D’Andrea, A.; Bossone, E.; Radmilovic, J.; Caso, P.; Calabrò, R.; Russo, M.G.; Galderisi, M. The role of new echocardiographic techniques in athlete’s heart. F1000Research 2015, 4, 289. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scharf, M.; Brem, M.H.; Wilhelm, M.; Schoepf, U.J.; Uder, M.; Lell, M.M. Atrial and Ventricular Functional and Structural Adaptations of the Heart in Elite Triathletes Assessed with Cardiac MR Imaging. Radiology 2010, 257, 71–79. [Google Scholar] [CrossRef] [Green Version]
- Bluemke, D.A.; Krupinski, E.A.; Ovitt, T.; Gear, K.; Unger, E.; Axel, L.; Boxt, L.M.; Casolo, G.; Ferrari, V.; Funaki, B.; et al. MR Imaging of Arrhythmogenic Right Ventricular Cardiomyopathy: Morphologic Findings and Interobserver Reliability. Cardiology 2003, 99, 153–162. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzi, F.; Anselmi, F.; Piu, P.; Fiorentini, C.; Carbone, S.F.; Volterrani, L.; Focardi, M.; Bonifazi, M.; Mondillo, S. Cardiac Magnetic Resonance Normal Reference Values of Biventricular Size and Function in Male Athlete’s Heart. JACC: Cardiovasc. Imaging 2018, 12, 1755–1765. [Google Scholar] [CrossRef]
- Kim, R.J.; Fieno, D.S.; Parrish, T.; Harris, K.; Chen, E.-L.; Simonetti, O.; Bundy, J.; Finn, J.P.; Klocke, F.J.; Judd, R.M. Relationship of MRI Delayed Contrast Enhancement to Irreversible Injury, Infarct Age, and Contractile Function. Circulation 1999, 100, 1992–2002. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fieno, D.S.; Kim, R.J.; Chen, E.-L.; Lomasney, J.W.; Klocke, F.J.; Judd, R.M. Contrast-enhanced magnetic resonance imaging of myocardium at risk: Distinction between reversible and irreversible injury throughout infarct healing. J. Am. Coll. Cardiol. 2000, 36, 1985–1991. [Google Scholar] [CrossRef] [Green Version]
- Moon, J.; Reed, E.; Sheppard, M.; Elkington, A.G.; Ho, S.; Burke, M.; Petrou, M.; Pennell, D.J. The histologic basis of late gadolinium enhancement cardiovascular magnetic resonance in hypertrophic cardiomyopathy. J. Am. Coll. Cardiol. 2004, 43, 2260–2264. [Google Scholar] [CrossRef] [PubMed]
- Breuckmann, F.; Möhlenkamp, S.; Nassenstein, K.; Lehmann, N.; Ladd, S.; Schmermund, A.; Sievers, B.; Schlosser, T.; Jöckel, K.-H.; Heusch, G.; et al. Myocardial Late Gadolinium Enhancement: Prevalence, Pattern, and Prognostic Relevance in Marathon Runners. Radiology 2009, 251, 50–57. [Google Scholar] [CrossRef] [PubMed]
- Maestrini, V.; Torlasco, C.; Hughes, R.; Moon, J.C. Cardiovascular Magnetic Resonance and Sport Cardiology: A Growing Role in Clinical Dilemmas. J. Cardiovasc. Transl. Res. 2020, 13, 296–305. [Google Scholar] [CrossRef]
- Gastl, M.; Lachmann, V.; Christidi, A.; Janzarik, N.; Veulemans, V.; Haberkorn, S.; Holzbach, L.; Jacoby, C.; Schnackenburg, B.; Berrisch-Rahmel, S.; et al. Cardiac magnetic resonance T2 mapping and feature tracking in athlete’s heart and HCM. Eur. Radiol. 2021, 31, 2768–2777. [Google Scholar] [CrossRef]
- Mordi, I.; Carrick, D.; Bezerra, H.G.; Tzemos, N. T1andT2mapping for early diagnosis of dilated non-ischaemic cardiomyopathy in middle-aged patients and differentiation from normal physiological adaptation. Eur. Hear. J. Cardiovasc. Imaging 2015, 17, 797–803. [Google Scholar] [CrossRef] [Green Version]
- Caruso, M.R.; Garg, L.; Martinez, M.W. Cardiac Imaging in the Athlete: Shrinking the “Gray Zone”. Curr. Treat. Options Cardiovasc. Med. 2020, 22, 5. [Google Scholar] [CrossRef]
- Burchfield, J.S.; Xie, M.; Hill, J.A. Pathological Ventricular Remodeling. Circulation 2013, 128, 388–400. [Google Scholar] [CrossRef] [Green Version]
- Augustine, D.X.; Howard, L. Left Ventricular Hypertrophy in Athletes: Differentiating Physiology From Pathology. Curr. Treat. Options Cardiovasc. Med. 2018, 20, 96. [Google Scholar] [CrossRef]
- Missenard, O.; Gabaudan, C.; Astier, H.; Desmots, F.; Garnotel, E.; Massoure, P.-L. Absence of cardiac damage induced by long-term intensive endurance exercise training: A cardiac magnetic resonance and exercise echocardiography analysis in masters athletes. Am. J. Prev. Cardiol. 2021, 7, 100196. [Google Scholar] [CrossRef] [PubMed]
- Stuber, M.; Weiss, R.G. Coronary magnetic resonance angiography. J. Magn. Reson. Imaging 2007, 26, 219–234. [Google Scholar] [CrossRef] [PubMed]
- Fogante, M.; Agliata, G.; Basile, M.; Compagnucci, P.; Volpato, G.; Falanga, U.; Stronati, G.; Guerra, F.; Vignale, D.; Esposito, A.; et al. Cardiac Imaging in Athlete’s Heart: The Role of the Radiologist. Medicina 2021, 57, 455. [Google Scholar] [CrossRef] [PubMed]
- Czimbalmos, C.; Csecs, I.; Dohy, Z.; Toth, A.; Suhai, F.I.; Müssigbrodt, A.; Kiss, O.; Geller, L.; Merkely, B.; Vago, H. Cardiac magnetic resonance based deformation imaging: Role of feature tracking in athletes with suspected arrhythmogenic right ventricular cardiomyopathy. Int. J. Cardiovasc. Imaging 2018, 35, 529–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Małek, Ł.A.; Mazurkiewicz, Ł.; Marszałek, M.; Barczuk-Falęcka, M.; Simon, J.; Grzybowski, J.; Miłosz-Wieczorek, B.; Postuła, M.; Marczak, M. Deformation Parameters of the Heart in Endurance Athletes and in Patients with Dilated Cardiomyopathy—A Cardiac Magnetic Resonance Study. Diagnostics 2021, 11, 374. [Google Scholar] [CrossRef] [PubMed]
- Baggish, A.L.; Battle, R.W.; Beaver, T.A.; Border, W.L.; Douglas, P.S.; Kramer, C.M.; Martinez, M.W.; Mercandetti, J.H.; Phelan, D.; Singh, T.K.; et al. Recommendations on the Use of Multimodality Cardiovascular Imaging in Young Adult Competitive Athletes: A Report from the American Society of Echocardiography in Collaboration with the Society of Cardiovascular Computed Tomography and the Society for Cardiovascular Magnetic Resonance. J. Am. Soc. Echocardiogr. 2020, 33, 523–549. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.M.; Hwang, S.H.; Lee, H.-J. Role of Cardiac Computed Tomography in the Diagnosis of Left Ventricular Myocardial Diseases. J. Cardiovasc. Imaging 2019, 27, 73–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Clinical History |
| Family history of sudden cardiac death/cardiomyopathies |
| Palpitations |
| Chest pain |
| Syncope |
| Physical Examination |
| Cardiac murmurs/abnormal cardiac sounds |
| Marfanoid habitus |
| 12-Lead ECG |
| T-wave inversion * |
| ST-segment depression |
| Pathologic Q-waves |
| Complete LBBB Profound (QRS ≥140 ms) non-specific intraventricular conduction delay |
| RBBB + left anterior hemiblock ** Epsilon wave Ventricular pre-excitation |
| Long QTc (≥470 ms in men, ≥480 ms in women) |
| Type 1 Brugada pattern *** Sinus bradycardia <30 beats/min Sinus pauses ≥3 s First degree AV block ≥400 ms Mobitz type 2 second degree AV block Third-degree AV block Atrial tachyarrhythmias Ventricular arrhythmias PVCs ≥ 2 per 10 s tracing |
| Differential Diagnosis | Echocardiographic Features |
|---|---|
| HCM |
|
| |
| |
| |
| |
| |
| |
| |
| |
| DCM |
|
| |
| |
| Myocarditis |
|
| LVNC |
|
| |
| |
| |
| |
| AC |
|
| |
| |
| |
| |
| BAV |
|
| MVP |
|
| Coronary artery anomalies |
|
| Differential Diagnosis | CMR Features |
|---|---|
| HCM |
|
| DCM |
|
| Myocarditis |
|
| LVNC |
|
| AC |
|
| |
| |
| BAV |
|
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
D’Andrea, A.; Sperlongano, S.; Russo, V.; D’Ascenzi, F.; Benfari, G.; Renon, F.; Palermi, S.; Ilardi, F.; Giallauria, F.; Limongelli, G.; et al. The Role of Multimodality Imaging in Athlete’s Heart Diagnosis: Current Status and Future Directions. J. Clin. Med. 2021, 10, 5126. https://doi.org/10.3390/jcm10215126
D’Andrea A, Sperlongano S, Russo V, D’Ascenzi F, Benfari G, Renon F, Palermi S, Ilardi F, Giallauria F, Limongelli G, et al. The Role of Multimodality Imaging in Athlete’s Heart Diagnosis: Current Status and Future Directions. Journal of Clinical Medicine. 2021; 10(21):5126. https://doi.org/10.3390/jcm10215126
Chicago/Turabian StyleD’Andrea, Antonello, Simona Sperlongano, Vincenzo Russo, Flavio D’Ascenzi, Giovanni Benfari, Francesca Renon, Stefano Palermi, Federica Ilardi, Francesco Giallauria, Giuseppe Limongelli, and et al. 2021. "The Role of Multimodality Imaging in Athlete’s Heart Diagnosis: Current Status and Future Directions" Journal of Clinical Medicine 10, no. 21: 5126. https://doi.org/10.3390/jcm10215126