
A Pragmatic Benchmarking Study of an Evidence-Based Personalised Approach in 1938 Adolescents with High-Risk Idiopathic Scoliosis

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
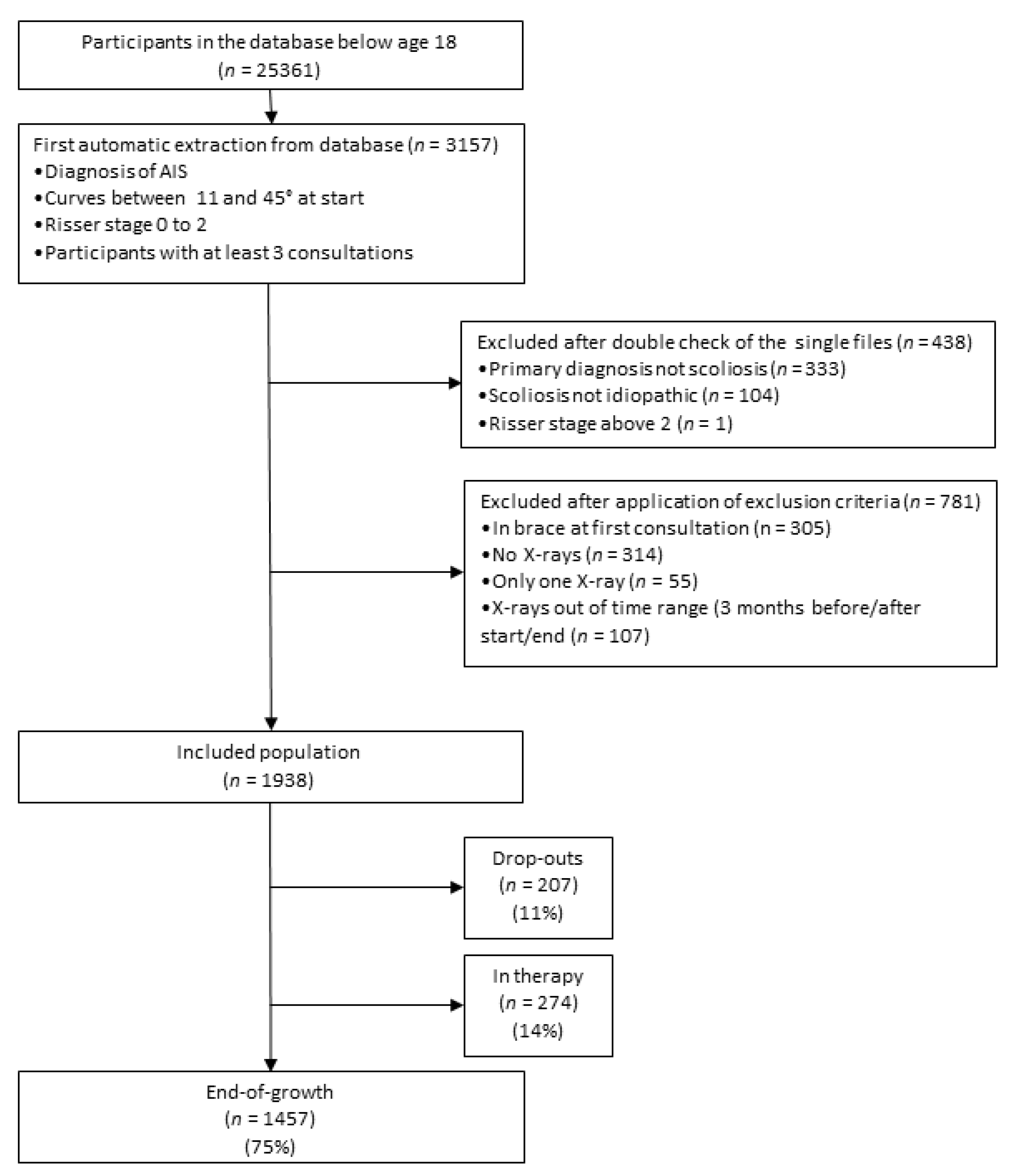
2.1. Study Design and Participants
2.2. Procedures
2.3. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Description of the Evidence-Based Personalised Approach (EBPA) Used in This Study

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Low (up to 20°) | Moderate (21–40°) | Severe (>40°) | |||||
|---|---|---|---|---|---|---|---|
| Min | Max | Min | Max | Min | Max | ||
| Infantile | Obs 3 | Obs 3 | Obs 3 | TTRB | TTRB | Su | |
| Juvenile | PPSE | PSSE | FTRB | HTRB | |||
| Adolescent | Risser 0 | Obs 6 | SSB | HTRB | TTRB | ||
| Risser 1 | PSSE | FTRB | |||||
| Risser 2 | |||||||
| Risser 3 | |||||||
| Risser 4 | Obs12 | SIR | |||||
| Adult up to 25 y | Nothing | PSSE | Obs12 | SIR | Obs6 | ||
| Adult | No Pain | PSSE | Obs12 | HTRB | |||
| Pain | PSSE | SSB | HTRB | PSSE | Su | ||
| Elderly | No Pain | Nothing | PSSE | Obs36 | PSSE | Obs12 | HTRB |
| Pain | PSSE | SSB | PSSE | HTRB | PSSE | Su | |
| Trunk decompensation | Obs6 | PTRB | |||||
| Guidelines | EBPA | Risser 0 | Risser 1 | Risser 2 | |
|---|---|---|---|---|---|
| Low (10–20°) | Minimum | Observation (6 months) | |||
| 10–20° | Minimum | 0. Observation (3 months) | 0. Observation (6 months) | ||
| Maximum | 2. Soft Scoliosis Brace | 1. Physiotherapeutic Scoliosis Specific Exercises | |||
| Maximum | Soft Scoliosis Brace | ||||
| Moderate (21–40°) | Minimum | Half-Time Rigid Bracing | Physiotherapeutic Scoliosis Specific Exercises | ||
| 21–30° | Minimum | 1. Physiotherapeutic Scoliosis-Specific Exercises | |||
| Maximum | 5. Half-Time Very Rigid Bracing | ||||
| 31–40° | Minimum | 3. Half-Time Rigid Bracing | |||
| Maximum | 6. Full-Time Very Rigid Bracing | ||||
| Maximum | Surgery | ||||
| Severe (>40°) | Minimum | 6. Total-Time Rigid Bracing | 6. Full-Time Rigid Bracing | ||
| 41–45° | Minimum | 6. Full-Time Very Rigid Bracing | |||
| Maximum | 6. Total-Time Very Rigid Bracing | ||||
| Maximum | Surgery | ||||

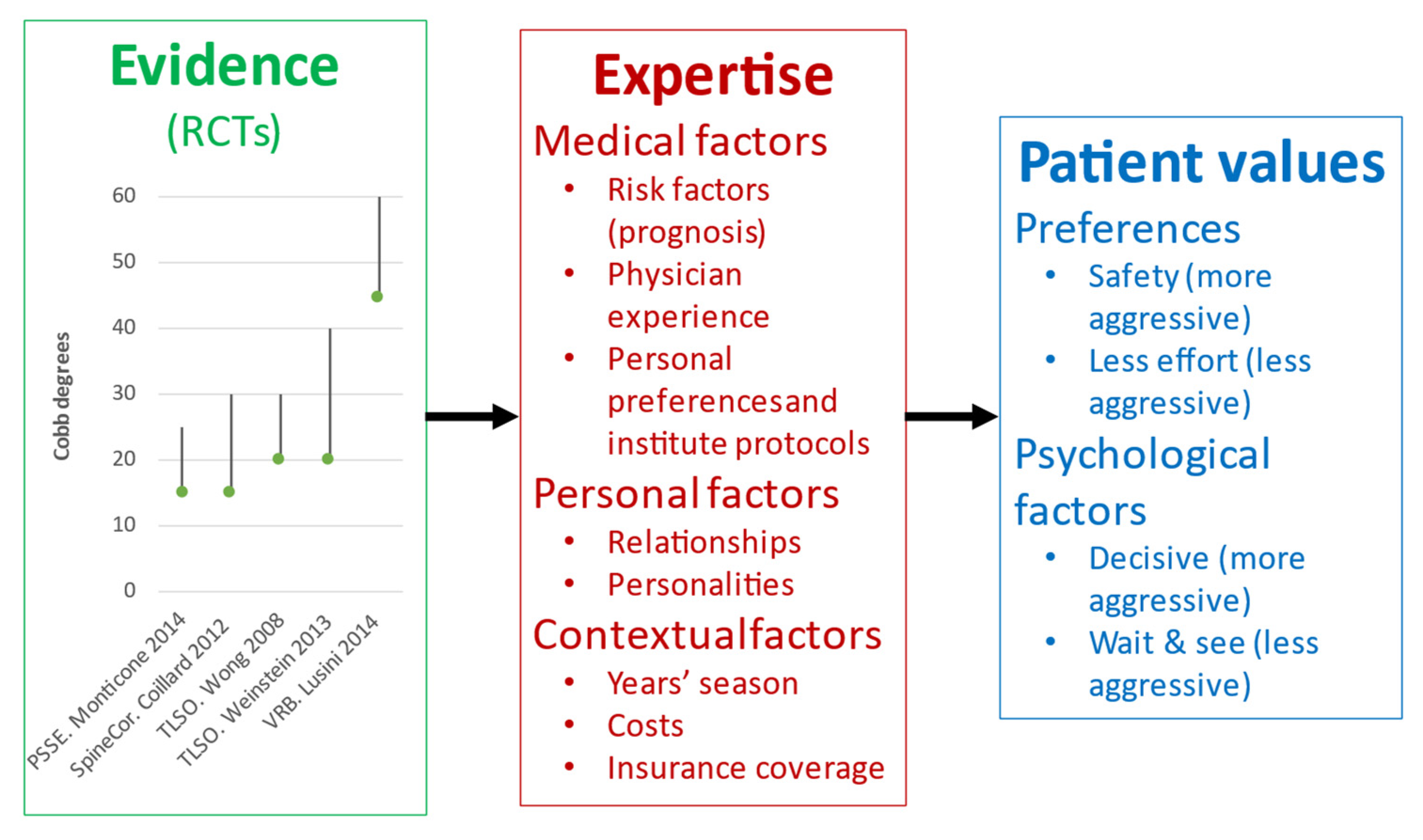
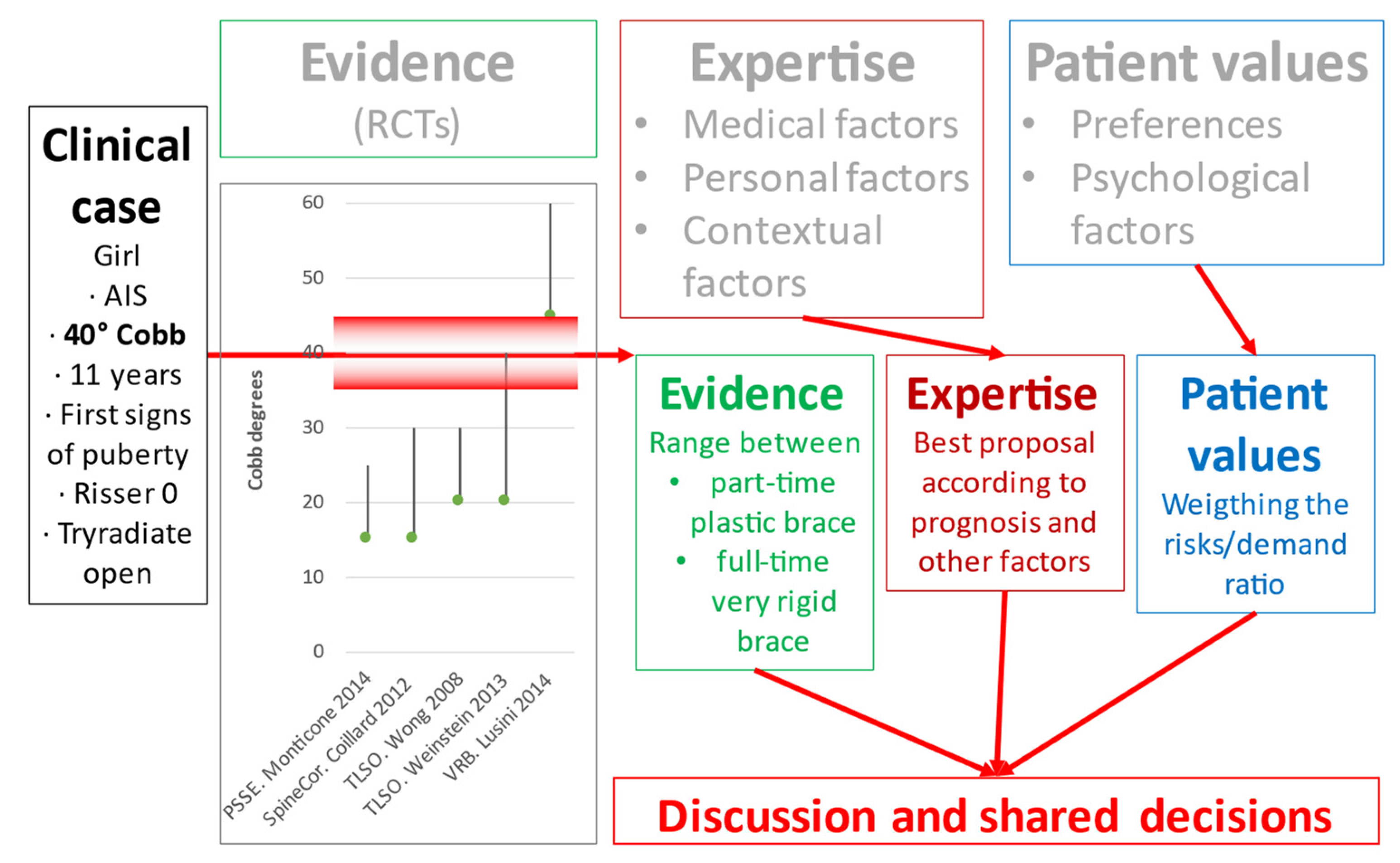
- Medical factors: they include commonly described risk factors determining the prognosis, even if without a complete certainty; physician experience drives to a more or less conservative or aggressive attitude; physicians’ preferences and institute protocols greatly influence the dosage (number of hours per day of treatment), since there are no strong scientific data on the topic.
- Personal factors: they include the relationships with patient and family, the evaluation of the personalities of patient and family, and how they could influence treatment.
- Preferences: the need for safety with as few risks as possible drives to a more aggressive attitude (more demanding treatments), while more significant attention to care and psychological well-being can lead to the opposite.
- Psychological factors: a more significant internal locus of control or an aggressive attitude will lead to more demanding treatments, while the opposite will become true on the other extreme of the psychological spectrum.



References
- Sackett, D.L.; Rosenberg, W.M.; Gray, J.A.; Haynes, R.B.; Richardson, W.S. Evidence Based Medicine: What It Is and What It Isn’t. BMJ 1996, 312, 71–72. [Google Scholar] [CrossRef] [Green Version]
- Ansmann, L.; Pfaff, H. Providers and Patients Caught Between Standardization and Individualization: Individualized Standardization as a Solution Comment on “(Re) Making the Procrustean Bed? Standardization and Customization as Competing Logics in Healthcare.” Int. J. Health Policy Manag. 2017, 7, 349–352. [Google Scholar] [CrossRef]
- Barratt, A. Evidence Based Medicine and Shared Decision Making: The Challenge of Getting Both Evidence and Preferences into Health Care. Patient Educ. Couns. 2008, 73, 407–412. [Google Scholar] [CrossRef]
- McCormack, J.; Elwyn, G. Shared Decision Is the Only Outcome That Matters When It Comes to Evaluating Evidence-Based Practice. BMJ Evid.-Based Med. 2018, 23, 137–139. [Google Scholar] [CrossRef] [PubMed]
- Jacke, C.O.; Albert, U.S.; Kalder, M. The Adherence Paradox: Guideline Deviations Contribute to the Increased 5-Year Survival of Breast Cancer Patients. BMC Cancer 2015, 15, 734. [Google Scholar] [CrossRef]
- Garber, A.M.; Tunis, S.R. Does Comparative-Effectiveness Research Threaten Personalized Medicine? N. Engl. J. Med. 2009, 360, 1925–1927. [Google Scholar] [CrossRef] [PubMed]
- Vandenbroucke, J.P. Why Do the Results of Randomised and Observational Studies Differ? BMJ 2011, 343, d7020. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L.; Dolan, L.A.; Wright, J.G.; Dobbs, M.B. Effects of Bracing in Adolescents with Idiopathic Scoliosis. New Engl. J. Med. 2013, 369, 1512–1521. [Google Scholar] [CrossRef] [Green Version]
- Coillard, C.; Circo, A.B.; Rivard, C.H. A Prospective Randomized Controlled Trial of the Natural History of Idiopathic Scoliosis versus Treatment with the Spinecor Brace. Sosort Award 2011 Winner. Eur. J. Phys. Rehabil. Med. 2014, 50, 479–487. [Google Scholar]
- Monticone, M.; Ambrosini, E.; Cazzaniga, D.; Rocca, B.; Ferrante, S. Active Self-Correction and Task-Oriented Exercises Reduce Spinal Deformity and Improve Quality of Life in Subjects with Mild Adolescent Idiopathic Scoliosis. Results of a Randomised Controlled Trial. Eur. Spine J. 2014, 23, 1204–1214. [Google Scholar] [CrossRef]
- Negrini, S.; Donzelli, S.; Aulisa, A.G.; Czaprowski, D.; Schreiber, S.; de Mauroy, J.C.; Diers, H.; Grivas, T.B.; Knott, P.; Kotwicki, T.; et al. 2016 SOSORT Guidelines: Orthopaedic and Rehabilitation Treatment of Idiopathic Scoliosis during Growth. Scoliosis Spinal. Disord 2018, 13, 3. [Google Scholar] [CrossRef] [Green Version]
- Weinstein, S.L.; Dolan, L.A.; Spratt, K.F.; Peterson, K.K.; Spoonamore, M.J.; Ponseti, I.V. Health and Function of Patients with Untreated Idiopathic Scoliosis: A 50-Year Natural History Study. JAMA 2003, 289, 559–567. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mayo, N.E.; Goldberg, M.S.; Poitras, B.; Scott, S.; Hanley, J. The Ste-Justine Adolescent Idiopathic Scoliosis Cohort Study. Part III: Back Pain. Spine 1994, 19, 1573–1581. [Google Scholar] [CrossRef]
- Negrini, S.; Hresko, T.M.; O’Brien, J.P.; Price, N.; SOSORT Boards; SRS Non-Operative Committee. Recommendations for Research Studies on Treatment of Idiopathic Scoliosis: Consensus 2014 between SOSORT and SRS Non-Operative Management Committee. Scoliosis 2015, 10, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Felice, F.; Zaina, F.; Donzelli, S.; Negrini, S. The Natural History of Idiopathic Scoliosis During Growth: A Meta-Analysis. Am. J. Phys. Med. Rehabil. 2018, 97, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Nachemson, A.L.; Peterson, L.E. Effectiveness of Treatment with a Brace in Girls Who Have Adolescent Idiopathic Scoliosis. A Prospective, Controlled Study Based on Data from the Brace Study of the Scoliosis Research Society. J. Bone Jt. Surg. Am. 1995, 77, 815–822. [Google Scholar] [CrossRef] [PubMed]
- Dolan, L.A.; Weinstein, S.L. Surgical Rates after Observation and Bracing for Adolescent Idiopathic Scoliosis: An Evidence-Based Review. Spine 2007, 32, S91–S100. [Google Scholar] [CrossRef]
- Zaina, F.; De Mauroy, J.C.; Grivas, T.; Hresko, M.T.; Kotwizki, T.; Maruyama, T.; Price, N.; Rigo, M.; Stikeleather, L.; Wynne, J.; et al. Bracing for Scoliosis in 2014: State of the Art. Eur. J. Phys. Rehabil. Med. 2014, 50, 93–110. [Google Scholar]
- Negrini, S.; Grivas, T.B.; Kotwicki, T.; Rigo, M.; Zaina, F.; International Society on Scoliosis Orthopaedic and Rehabilitation Treatment (SOSORT). Guidelines on “Standards of Management of Idiopathic Scoliosis with Corrective Braces in Everyday Clinics and in Clinical Research”: SOSORT Consensus 2008. Scoliosis 2009, 4, 2. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dunn, J.; Henrikson, N.B.; Morrison, C.C.; Blasi, P.R.; Nguyen, M.; Lin, J.S. Screening for Adolescent Idiopathic Scoliosis: Evidence Report and Systematic Review for the US Preventive Services Task Force. JAMA 2018, 319, 173–187. [Google Scholar] [CrossRef] [PubMed]
- Negrini, S.; Minozzi, S.; Bettany-Saltikov, J.; Chockalingam, N.; Grivas, T.B.; Kotwicki, T.; Maruyama, T.; Romano, M.; Zaina, F. Braces for Idiopathic Scoliosis in Adolescents. Cochrane Database Syst. Rev. 2015, 6, CD006850. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.; Minozzi, S.; Bettany-Saltikov, J.; Zaina, F.; Chockalingam, N.; Kotwicki, T.; Maier-Hennes, A.; Negrini, S. Exercises for Adolescent Idiopathic Scoliosis. Cochrane Database Syst. Rev. 2012, 8, CD007837. [Google Scholar] [CrossRef] [Green Version]
- Negrini, S.; Donzelli, S.; Negrini, A.; Parzini, S.; Romano, M.; Zaina, F. Specific Exercises Reduce the Need for Bracing in Adolescents with Idiopathic Scoliosis: A Practical Clinical Trial. Ann. Phys. Rehabil. Med. 2019, 62, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Fusco, C.; Zaina, F.; Atanasio, S.; Romano, M.; Negrini, A.; Negrini, S. Physical Exercises in the Treatment of Adolescent Idiopathic Scoliosis: An Updated Systematic Review. Physiother. Theory Pract. 2011, 27, 80–114. [Google Scholar] [CrossRef] [PubMed]
- Karol, L.A.; Virostek, D.; Felton, K.; Wheeler, L. Effect of Compliance Counseling on Brace Use and Success in Patients with Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. Am. 2016, 98, 9–14. [Google Scholar] [CrossRef] [Green Version]
- Romano, M.; Negrini, A.; Parzini, S.; Tavernaro, M.; Zaina, F.; Donzelli, S.; Negrini, S. SEAS (Scientific Exercises Approach to Scoliosis): A Modern and Effective Evidence Based Approach to Physiotherapic Specific Scoliosis Exercises. Scoliosis 2015, 10, 3. [Google Scholar] [CrossRef] [Green Version]
- Negrini, S.; Marchini, G.; Tessadri, F. Brace Technology Thematic Series—The Sforzesco and Sibilla Braces, and the SPoRT (Symmetric, Patient Oriented, Rigid, Three-Dimensional, Active) Concept. Scoliosis 2011, 6, 8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aulisa, A.G.; Mastantuoni, G.; Laineri, M.; Falciglia, F.; Giordano, M.; Marzetti, E.; Guzzanti, V. Brace Technology Thematic Series: The Progressive Action Short Brace (PASB). Scoliosis 2012, 7, 6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Donzelli, S.; Zaina, F.; Negrini, S. In Defense of Adolescents: They Really Do Use Braces for the Hours Prescribed, If Good Help Is Provided. Results from a Prospective Everyday Clinic Cohort Using Thermobrace. Scoliosis 2012, 7, 12. [Google Scholar] [CrossRef] [Green Version]
- Katz, D.E.; Herring, J.A.; Browne, R.H.; Kelly, D.M.; Birch, J.G. Brace Wear Control of Curve Progression in Adolescent Idiopathic Scoliosis. J. Bone Jt. Surg. Am. 2010, 92, 1343–1352. [Google Scholar] [CrossRef]





| Subgroup | Plastic Brace TLSO | Elastic Brace (SpineCor) | Physiotherapeutic Scoliosis-Specific Exercises |
|---|---|---|---|
| Acronym | BrAIST | EB | PSSE |
| Comparison RCT | Weinstein et al. [8] | Coillard et al. [9] | Monticone et al. [10] |
| Age (years) | 10–15 | 8–15 | 10 or older |
| Risser (grade) | 0–2 | 0–2 | 0–1 |
| Menarche | pre-menarchal or 1-year post-menarchal | - | - |
| Cobb angle | 20–40° | 15–30° | 11–25° |
| Curve | apex at, or caudal to T7 | - | - |
| Previous treatments | not for AIS | - | - |
| Intensity of Treatment | Treatment |
|---|---|
| 0 | Observation |
| 1 | Physiotherapeutic Scoliosis-Specific Exercises |
| 2 | Elastic brace (SpineCor) |
| 3 | Rigid plastic brace (Sibilla, Lapadula, PASB) brace 21 h/day or less |
| 4 | Rigid plastic brace (Sibilla, Lapadula, PASB) brace 22–24 h/day |
| 5 | Very rigid plastic brace (Sforzesco) brace 18–12 h/day |
| 6 | Very rigid plastic brace (Sforzesco) brace 22–24 h/day |
| Clinical Situation at the Start | Aims of Treatment According to Current Guidelines [11] | Thresholds of Over- and Under-Treatment | |||
|---|---|---|---|---|---|
| Degree of scoliosis | °Cobb | Primary aim | Minimal aim | Over-treatment | Under-treatment |
| Low | 11–20 | End of growth < 20° | End of growth < 45° | Improvement > 5° | End of growth > 30° |
| Moderate | 21–25 | End of growth < 30° | Improvement > | ||
| 26–30 | Progression > 5° # | ||||
| 31–40 | |||||
| Severe | 41–45 | End of growth < 45° | End of growth < 60° * | ||
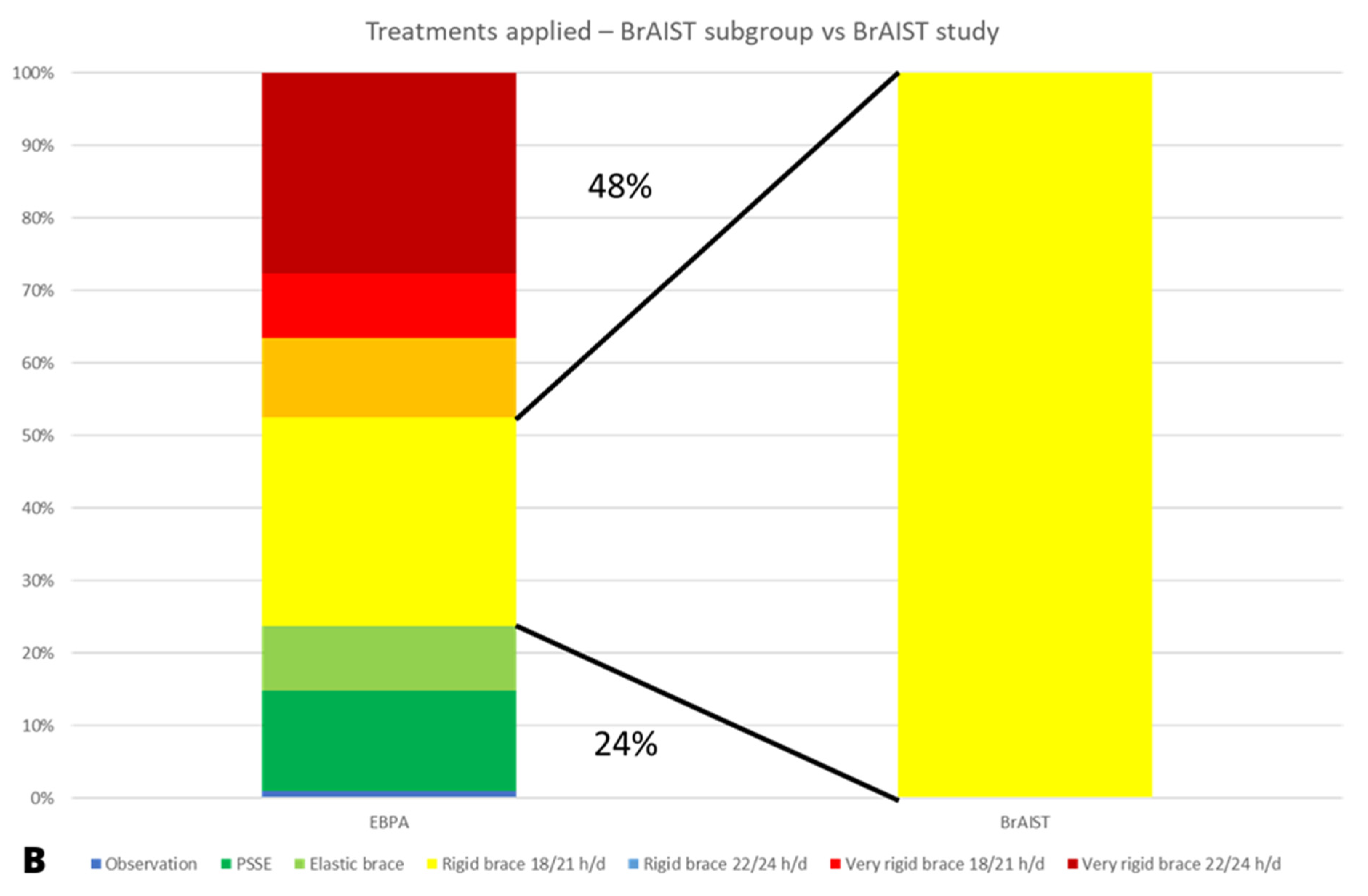
| BrAIST Subgroup vs. BrAIST RCT | EB Subgroup vs. Coillard RCT | PSSE Subgroup vs. Monticone RCT | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| BrAIST Subgroup of the Current Study | Comparison with BrAIST RCT Groups | Coillard Subgroup of the Current Study | Comparison with Coillard RCT Groups | PSSE Subgroup of the Current study | Comparison with Monticone RCT Groups | |||||||||||
| Observed | p | Treated | p | Observed | p | Treated | p | Observed | p | Treated | p | |||||
| Number | 687 | 96 | 146 | 884 | 36 | 21 | 590 | 55 | 55 | |||||||
| Age | 12.7 ± 1.3 | 12.7 ± 1.2 | NS | 12.7 ± 1.0 | NS | 12.11 ± 1.5 | 12.2 ± 2 | NS | 12.2 ± 2 | NS | 12.6 ± 1.4 | 12.5 ± 1.1 | NS | 12.4 ± 1.1 | NS | |
| Female sex | 83% (81–86) | 90% (84–96) | 0.13 | 92% (88–96) | 0.01 | 82% (80–85) | 86% (74–97) | 0.68 | 85% (69–100) | 0.88 | 82% (79–85) | 71% (59–83) | 0.07 | 75% (63–86) | 0.23 | |
| Race | White | 100% | 76% (67–85) | <0.0001 | 79% (72–86) | <0.0001 | 100% | NA | NA | (100%) | NA | NA | ||||
| Black | 0 | 11% (11–11) | 8% (8–8) | 0 | NA | NA | 0 | NA | NA | |||||||
| Other | 0 | 9% (9–9) | 5% (5–5) | 0 | NA | NA | 0 | NA | NA | |||||||
| Unknown | 0 | 3% (3–3) | 8% (8–8) | 0 | NA | NA | 0 | NA | NA | |||||||
| Height | 157.3 ± 9.1 | 153.6 ± 10.6 | 0.0002 | 156.5 ± 9.1 | NS | 158.7 ± 9.5 | 156.2 ± 9.1 | 146.3 ± 7.5 | <0.0001 | 147.0 ± 5.7 | <0.0001 | |||||
| Cobb angle of the largest curve | 28.4 ± 5.8 | 30.3 ± 6.5 | 0.003 | 30.5 ± 5.8 | <0.0001 | 22.3 ± 4.5 | 20.0 ± 4.1 | 0.002 | 22.0 ± 4.9 | 0.3 | 18.1 ± 4.1 | 19.3 ± 3.9 | 0.03 | 19.2 ± 2.5 | 0.05 | |
| Risser grade | 0 | 56% (52–60) | 64% (54–74) | NS | 56% (48–64) | NS | 48% (45–51) | 69% (65–73) | 45% (32–59) | 0.0007 | 45% (32–59) | 0.0007 | ||||
| 1 | 22% (19–25) | 20% (12–28) | 31% (23–39) | 43% (40–46) | 31% (27–35) | 55% (41–68) | 55% (41–68) | |||||||||
| 2 | 21% (18–24) | 13% (6–20) | 10% (5–15) | 29% (26–32) | ||||||||||||
| Treatment intensity | 0 Observation | 1% (0–1) | 100% (100–100) | 0% (0–0) | 1% (0–2) | 100% (100–100) | 0% (0–0) | 6% (4–8) | 100% (100–100) | 0% (0–0) | ||||||
| 1 PSSE (SEAS School) | 14% (11–16) | 41% (38–45) | 60% (56–64) | 0% (0–0) | 100% (100–100) | |||||||||||
| 2 Elastic brace (SpineCor) | 9% (7–11) | 10% (8–12) | 0% (0–0) | 100% (100–100) | 8% (6–10) | |||||||||||
| 3 Rigid brace 18/21 h/d | 29% (26–33) | 0% (0–0) | 100% (100–100) | 31% (28–34) | 20% (17–24) | |||||||||||
| 4 Rigid brace 22/24 h/d | 11% (9–13) | 5% (3–6) | 2% (1–3) | |||||||||||||
| 5 Very rigid brace (Sforzesco) 18–21 h/d | 9% (7–11) | 7% (5–9) | 3% (2–4) | |||||||||||||
| 6 Very rigid brace (Sforzesco) 22–24 h/d | 28% (24–31) | 5% (3–6) | 1% (0–2) | |||||||||||||
| Risser | 0 | 1 | 2 | |
|---|---|---|---|---|
| Cobb Degrees | Intensity of Treatment | |||
| 10–20° | 0 | 10% | 6% | 6% |
| 1 | 78% | 80% | 82% | |
| 2 | 5% | 4% | 1% | |
| 3 | 5% | 10% | 10% | |
| 4 | 1% | 0% | 0% | |
| 5 | 1% | 1% | 2% | |
| 6 | 0% | 0% | 0% | |
| 21–30° | 0 | 1% | 1% | 1% |
| 1 | 16% | 18% | 24% | |
| 2 | 14% | 9% | 6% | |
| 3 | 39% | 45% | 47% | |
| 4 | 13% | 7% | 6% | |
| 5 | 8% | 11% | 10% | |
| 6 | 9% | 8% | 7% | |
| 31–40° | 0 | 0% | 0% | 0% |
| 1 | 1% | 0% | 1% | |
| 2 | 0% | 1% | 1% | |
| 3 | 9% | 7% | 4% | |
| 4 | 16% | 15% | 9% | |
| 5 | 4% | 17% | 18% | |
| 6 | 70% | 59% | 67% | |
| Severe (41–45°) | 0 | 0% | 0% | 0% |
| 1 | 0% | 0% | 0% | |
| 2 | 0% | 0% | 0% | |
| 3 | 0% | 0% | 0% | |
| 4 | 2% | 0% | 0% | |
| 5 | 0% | 0% | 7% | |
| 6 | 98% | 100% | 93% | |
| Analysis | Groups | Relative Risk (RR) of Success | Number Needed to Treat (NNT) | ||||
|---|---|---|---|---|---|---|---|
| EBPA | RCT | RR | IC95 | p | NNT | IC95 | |
| Comparison with BrAIST Study | |||||||
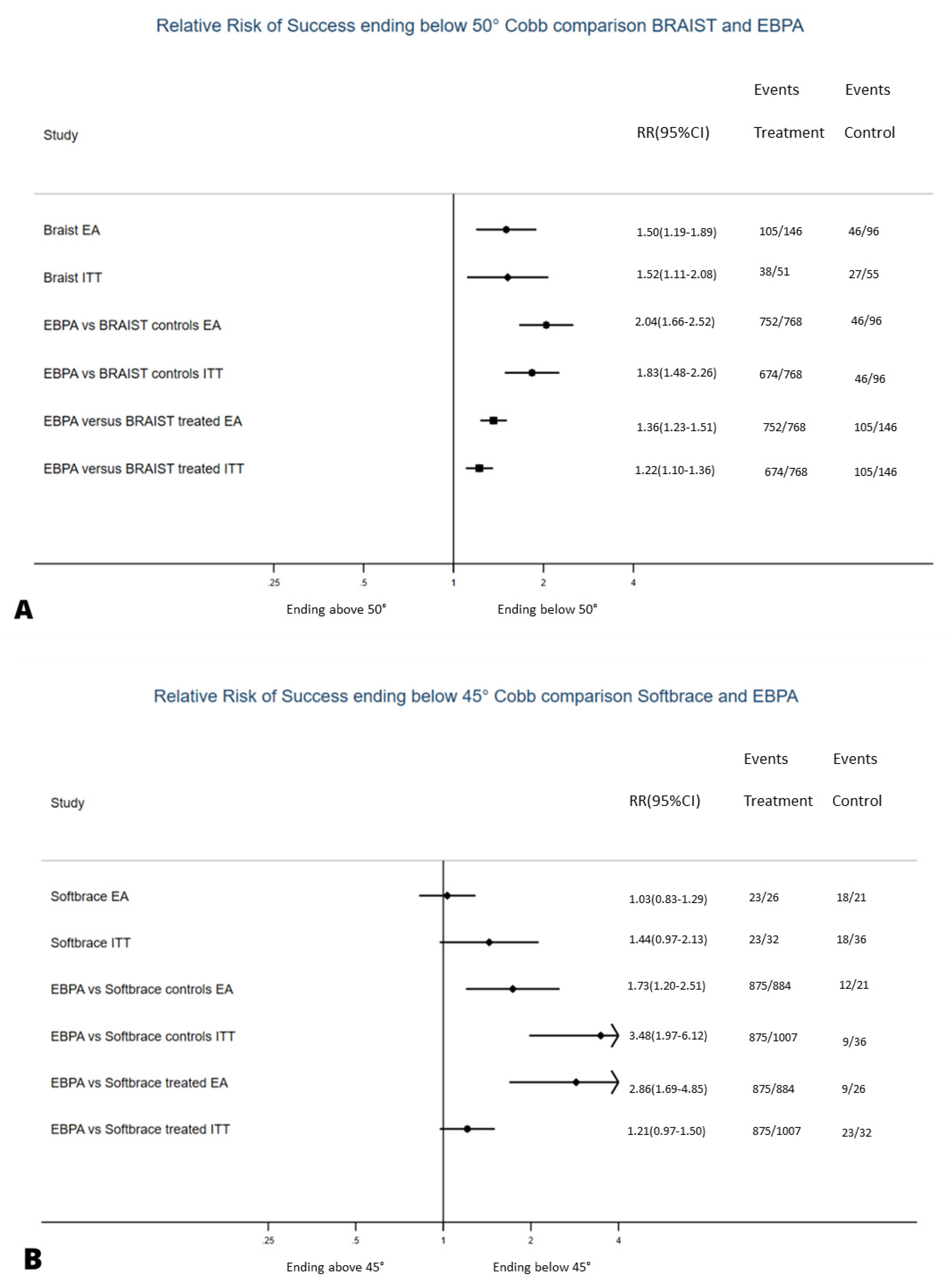
| Efficacy | treated EBPA | controls BrAIST | 2.0 | 1.7–2.5 | chi2 = 307.4 p < 0.001 | 2.0 | 1.7–2.5 |
| treated EBPA | treated BrAIST | 1.4 | 1.2–1.5 | chi2 = 141.8 p < 0.001 | 3.8 | 2.9–5.3 | |
| Intent to Treat | treated EBPA | controls BrAIST | 1.8 | 1.5–2.3 | chi2 = 97.5 p < 0.001 | 2.5 | 2.0–3.3 |
| treated EBPA | treated BrAIST | 1.2 | 1.1–1.4 | chi2 = 24.46 p < 0.001 | 6.3 | 4.2–12.5 | |
| Comparison with SpineCor Study | |||||||
| Efficacy | treated EBPA | controls SpineCor | 1.7 | 1.2–2.5 | chi2 = 184.2 p < 0.001 | 2.4 | 1.6–4.8 |
| treated EBPA | treated SpineCor | 2.9 | 1.7–4.9 | chi2 = 377.0 p < 0.001 | 1.6 | 1.2–2.2 | |
| Intent to Treat | treated EBPA | controls SpineCor | 3.5 | 2.0–6.1 | chi2 = 103.1 p < 0.001 | 1.6 | 1.3–2.1 |
| treated EBPA | treated SpineCor | 1.2 | 0.97–1.5 | chi2 = 5.96 p = 0.05 NS | 6.7 | 3.2–100 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Negrini, S.; Donzelli, S.; Negrini, F.; Arienti, C.; Zaina, F.; Peers, K. A Pragmatic Benchmarking Study of an Evidence-Based Personalised Approach in 1938 Adolescents with High-Risk Idiopathic Scoliosis. J. Clin. Med. 2021, 10, 5020. https://doi.org/10.3390/jcm10215020
Negrini S, Donzelli S, Negrini F, Arienti C, Zaina F, Peers K. A Pragmatic Benchmarking Study of an Evidence-Based Personalised Approach in 1938 Adolescents with High-Risk Idiopathic Scoliosis. Journal of Clinical Medicine. 2021; 10(21):5020. https://doi.org/10.3390/jcm10215020
Chicago/Turabian StyleNegrini, Stefano, Sabrina Donzelli, Francesco Negrini, Chiara Arienti, Fabio Zaina, and Koen Peers. 2021. "A Pragmatic Benchmarking Study of an Evidence-Based Personalised Approach in 1938 Adolescents with High-Risk Idiopathic Scoliosis" Journal of Clinical Medicine 10, no. 21: 5020. https://doi.org/10.3390/jcm10215020