
Intraosseous Venous Malformation of the Zygomatic Bone: Comparison between Virtual Surgical Planning and Standard Surgery with Review of the Literature


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
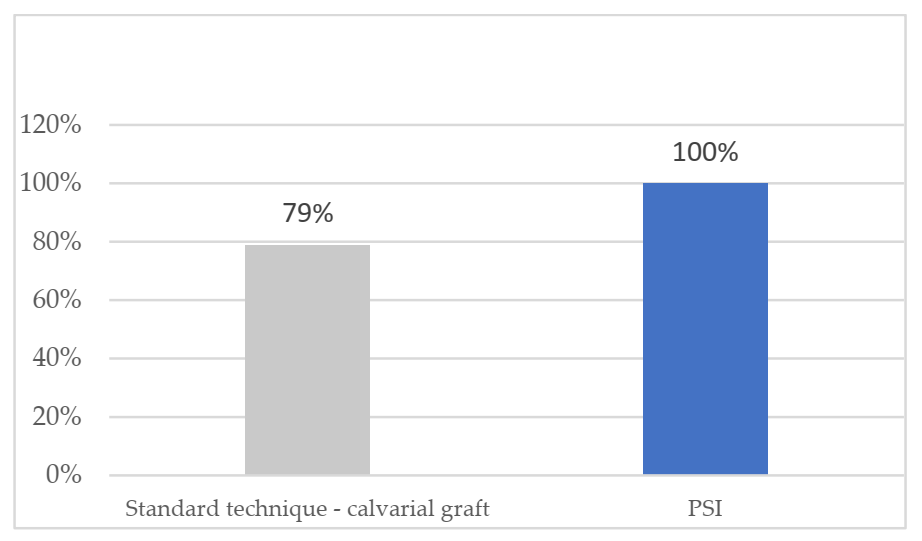
- Defect surface coverage through postoperative CT scan: the Radiodiagnostic Department compared the defect covered with a patient-specific implant in the VSP group and the defect covered with a calvarial graft in the standard technique group to assess precision and accuracy of both reconstructions. Phillips IntelliSpace Portal V.11.1 software was used to calculate the defect after resection of the malformation and the percentage coverage obtained after reconstruction.
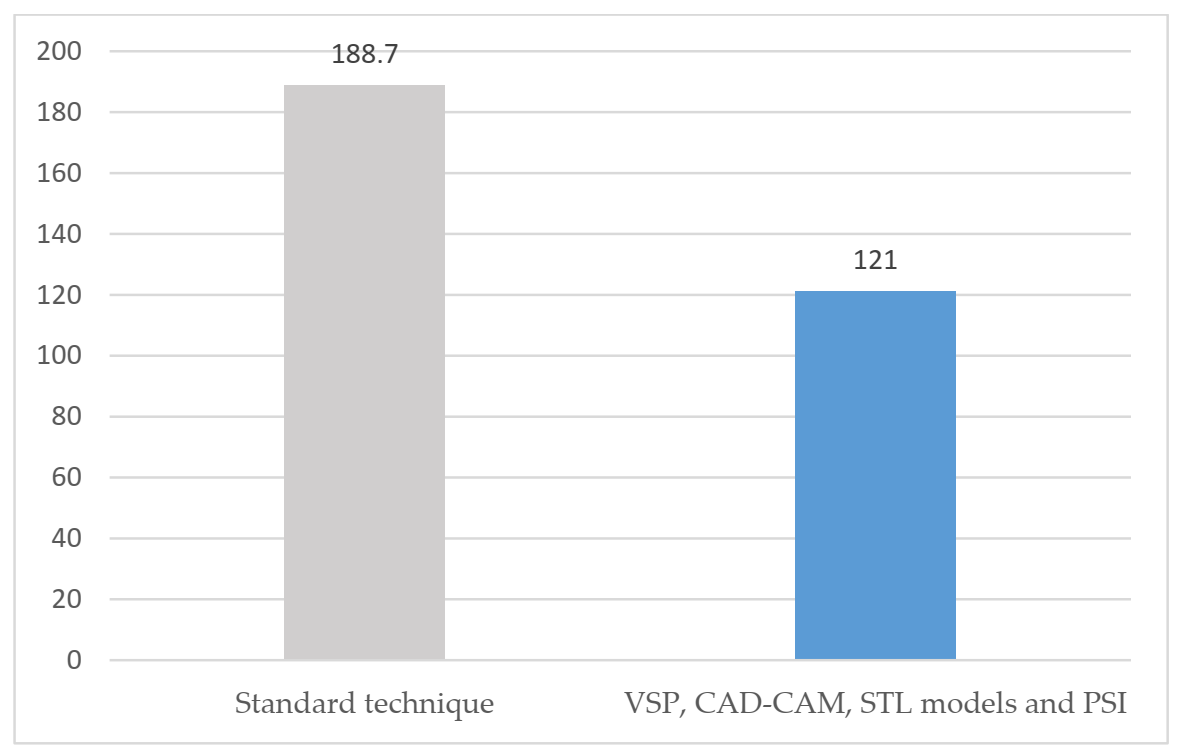
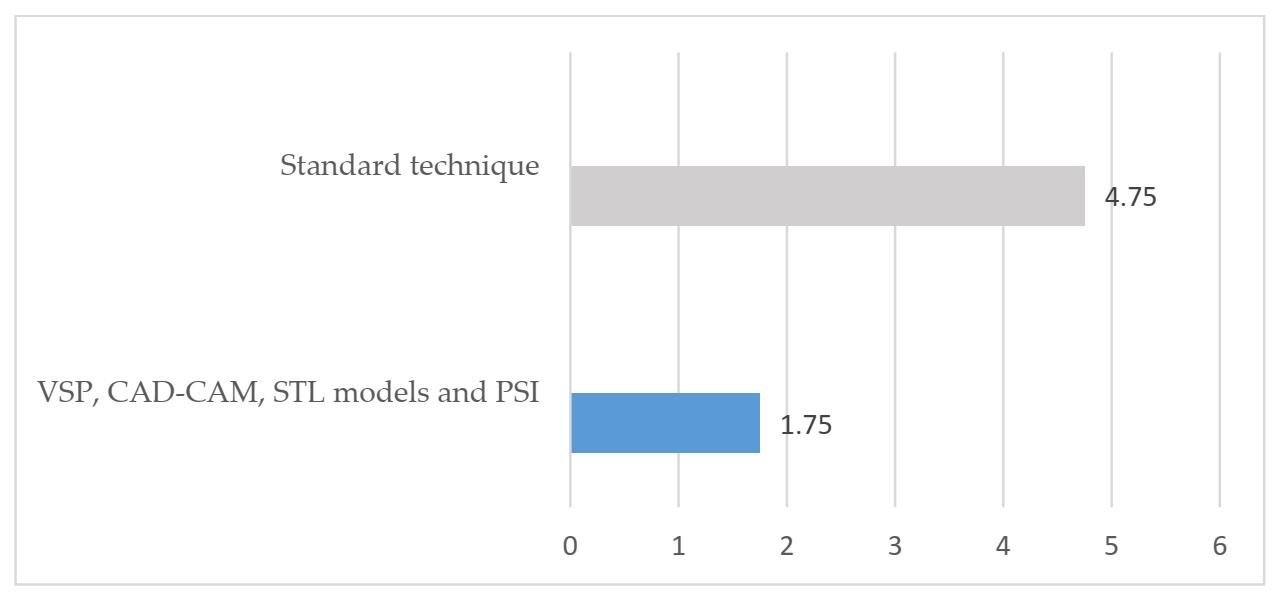
- Operation time and length of hospital stay between both techniques.
- Aesthetic result: aesthetic assessment was subjectively addressed by the patients regarding facial symmetry, facial scaring and facial projection and comparing the affected side with the non-affected side. The results were classified with scores 0 (poor), 1 (good) and 2 (excellent).
- Sequelae and complications with both techniques.
Review of the Literature
- hemangiomas: (intraosseous [Title] OR mandibular [Title] OR osseous [Title] OR central [Title]) AND (hemangioma [Title] OR hemangiomas [Title]) AND (face [Title] OR midface [Title] OR facial [Title] OR zygomatic [Title] OR zygoma [Title] OR malar [Title] OR maxilla [Title] OR maxillary [Title] OR orbital [Title] OR orbit [Title] OR mandible [Title] OR jaw [Title] OR jaws [Title] OR bone [Title]).
- vascular malformations: (intraosseous [Title] OR mandibular [Title] OR osseous [Title] OR central [Title]) AND (malformation [Title] OR malformations [Title]) AND (arteriovenous [Title] OR venous [Title] OR vascular [Title]) AND (face [Title] OR midface [Title] OR facial [Title] OR zygomatic [Title] OR zygoma [Title] OR malar [Title] OR maxilla [Title] OR maxillary [Title] OR orbital [Title] OR orbit [Title] OR mandible [Title] OR jaw [Title] OR jaws [Title] OR bone [Title]).
3. Results
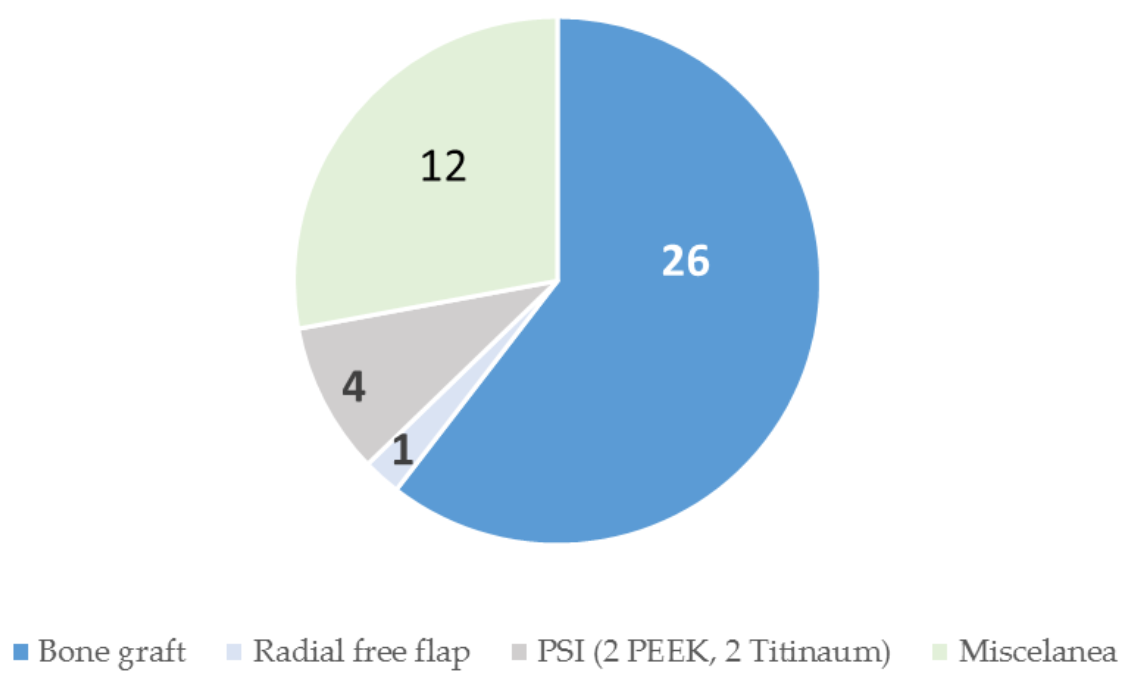
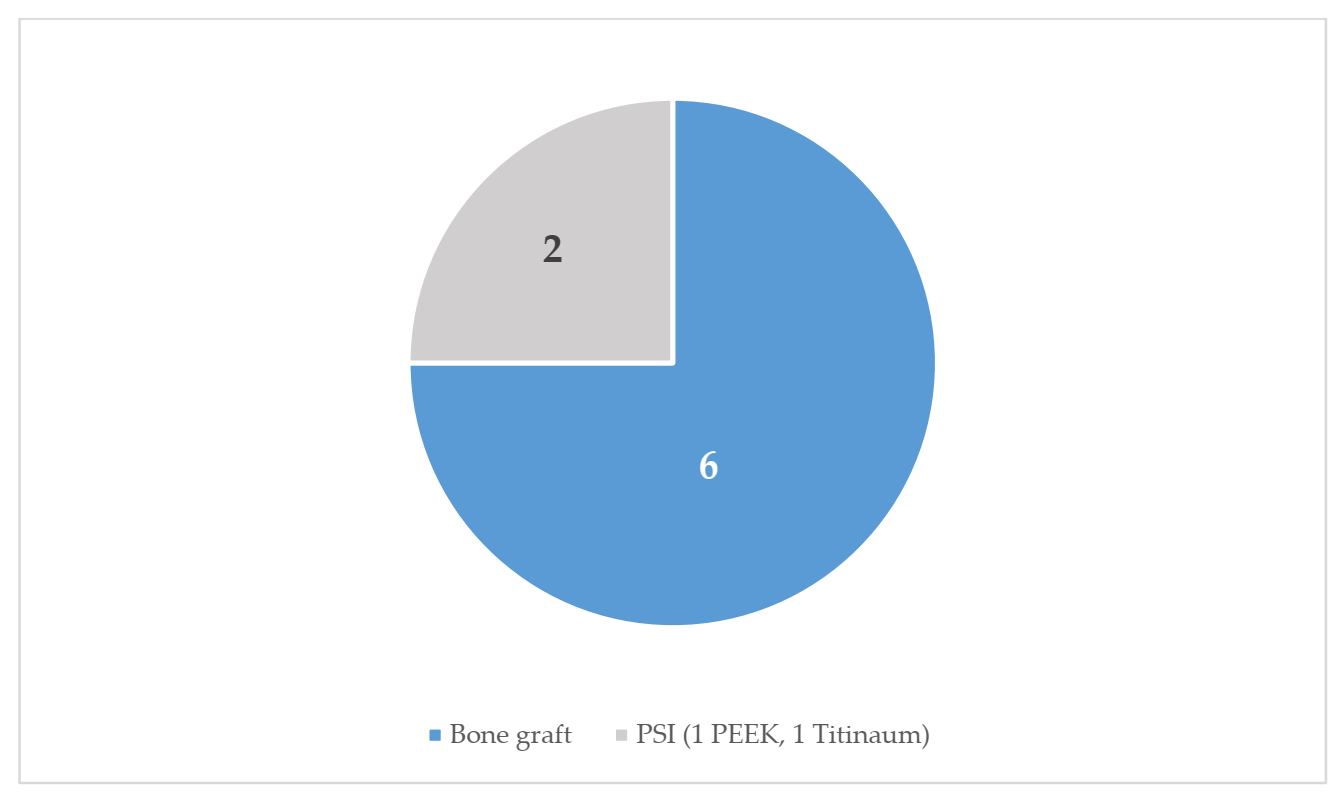
3.1. Characteristics of the Sample
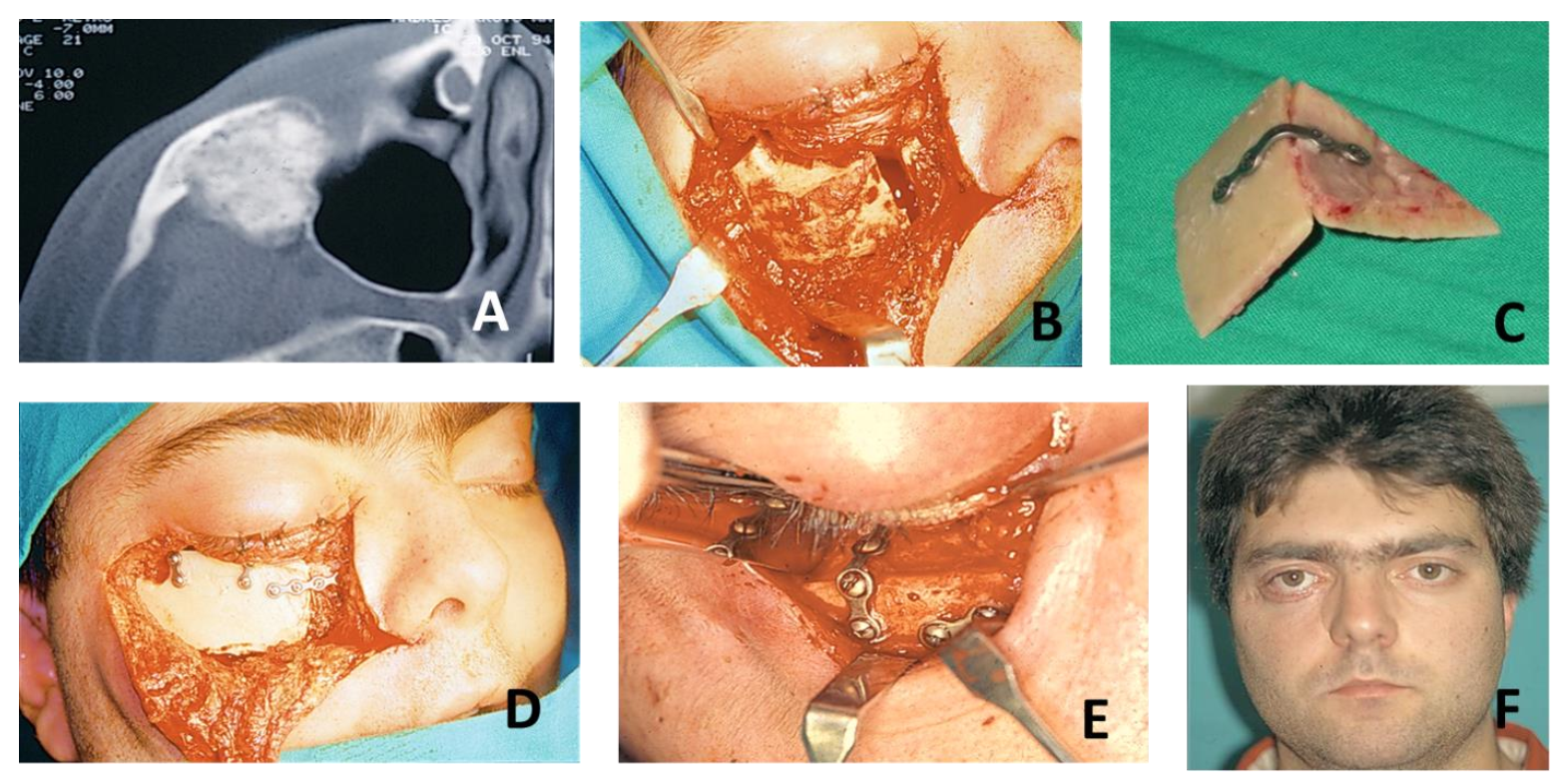
3.2. Outcomes in Patients Treated by Means of Standard Surgery
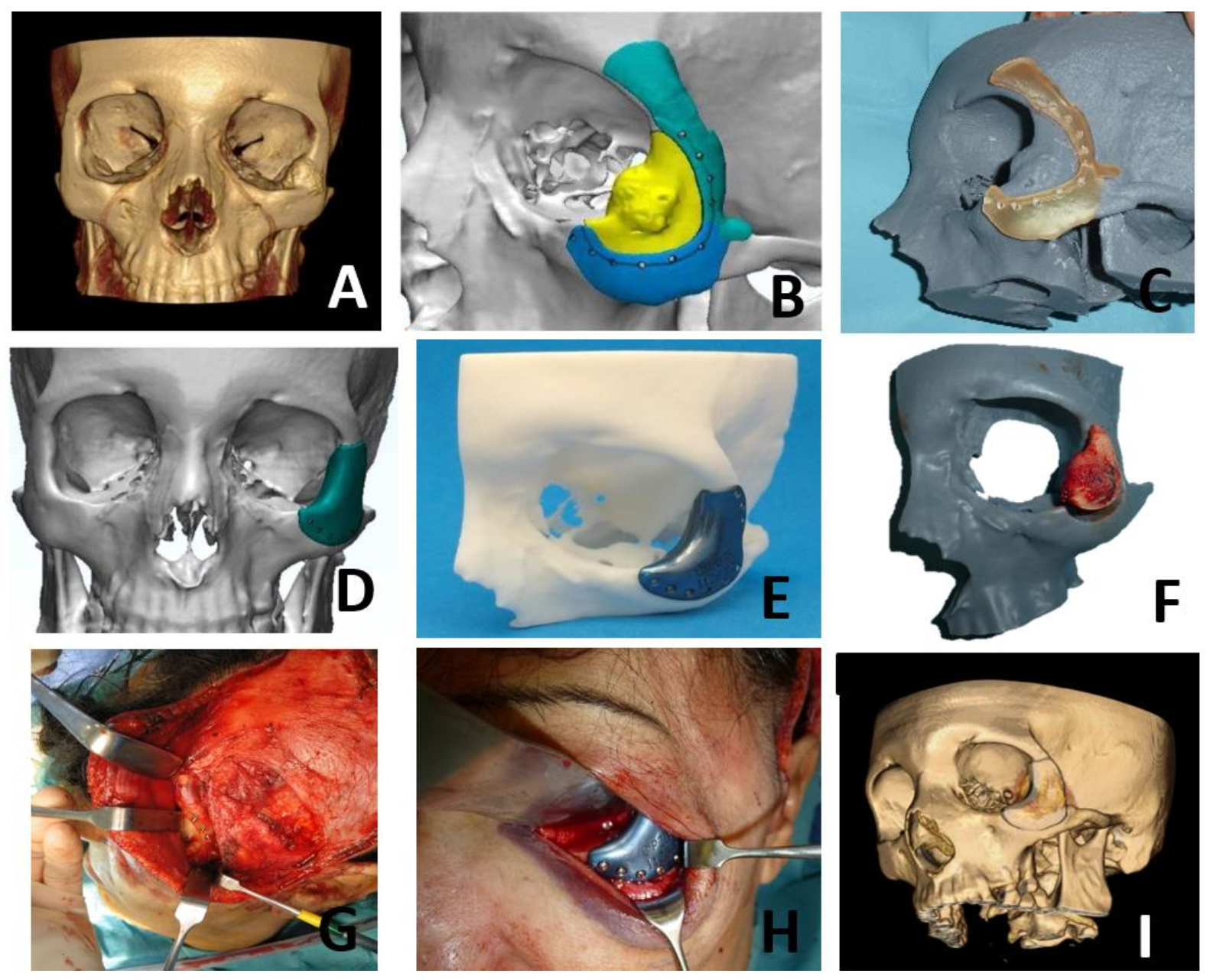
3.3. Outcomes in Patients Treated by Means of VSP, CAD-CAM, STL Models and PSI
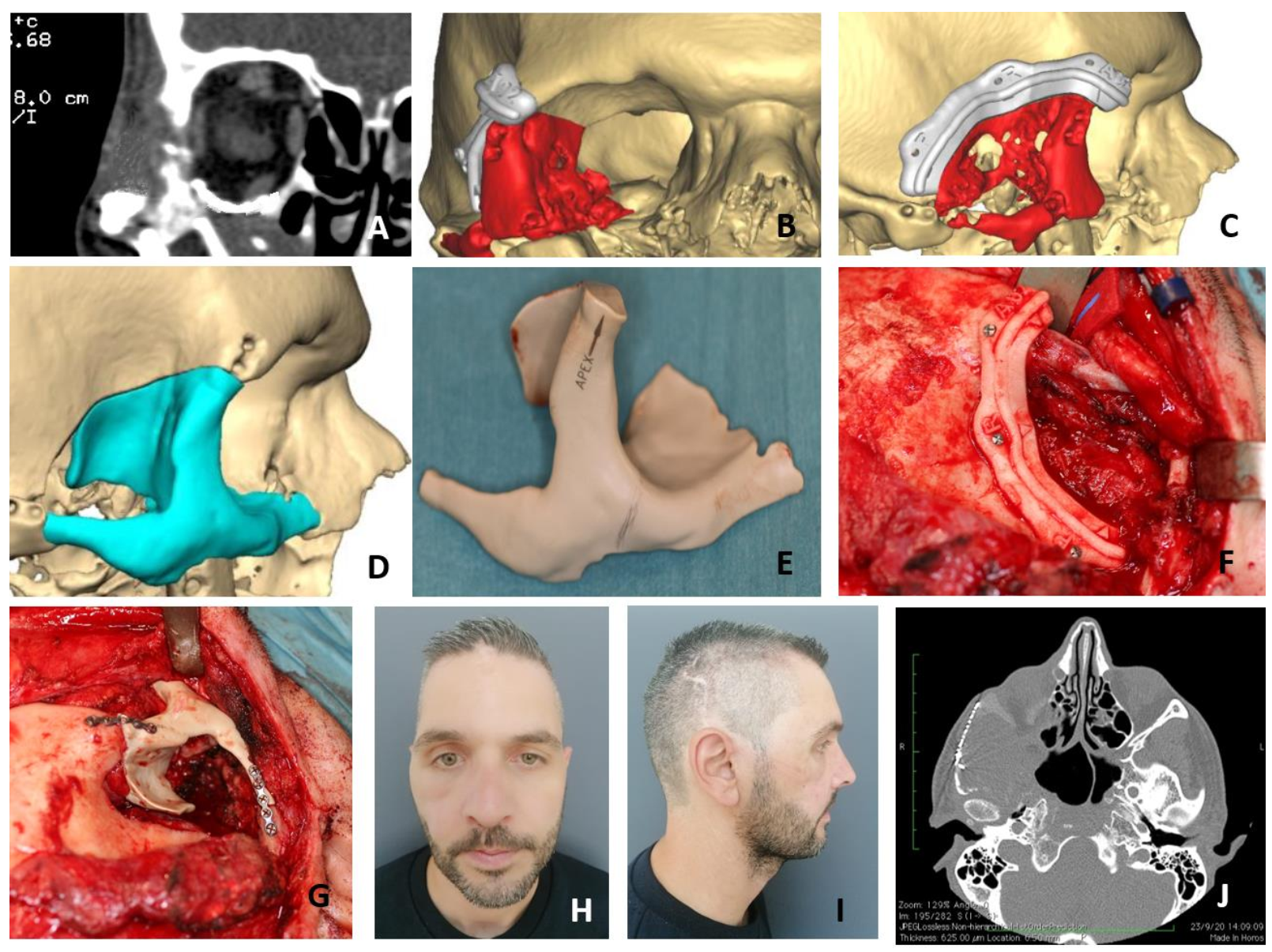
3.4. Case Presentation
3.5. Literature Review and Clarification on Diagnostics Terms
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CAD/CAM | Computer-Aided-Design/Computer-Aided-Manufacturing |
| CNC m.m. | Computer Numerical Control milling machine |
| CT scan | Computed tomography scan |
| ISSVA | International Society for the Study of Vascular Anomalies |
| MR | Magnetic Resonance |
| PEEK | Polyether-Ether-Ketone |
| PSI | Patient Specific Implant |
| STL model | stereolithographic model |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year of Publication) | Age/Sex | Side, Size | Duration | Pain | Ocular Findings | Traumatism | Imaging | Management | Surgical Approach | Reconstruction | Bleeding | Follow-Up, Recurrence | Inmunohistochemistry | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | Yueh-Bih Tang Chen et al. (1991) [38] | 44/F | R/3 × 2 cm | 1 y | Y | N | N | X-rays: radiolucent lesion | Excision | Coronal | Cranial bone graft | N | 6 y, no recurrence | ? |
| 2 | Srinivasan et al. (2009) [8] | 66/F | R, 3 × 3 cm | 4 y | N | N | N | CT: radiating spoke wheel | Excision | ? | Not required | N | 2.5 y, no recurrence | GLUT-1 negative |
| 3 | Defazio et al. (2012) [29] | 58/F | R, 1 × 1.5 cm | 2 y | N | N | Y | CT: sunburst; MRI: T2 with high signal intensity | Incisional biopsy; Surveillance | ? | Not required | ? | ? | GLUT-1 negative |
| 4 | Defazio et al. (2012) [29] | 53/F | R, 1 × 1.8 cm | ? | Y | ? | N | CT and MRI consistent with dx of intraosseous venous malformation | Initial incisional bi- opsy non-diagnos- tic; Surveillance; Complete resec- tion 2 y later | ? | Split calvarial bone graft | ? | ? | ? |
| 5 | Defazio et al. (2012) [29] | 49/M | R, 1 cm | 6 mo | N | N | N | CT: honeycomb | Complete resection | ? | Split calvarial bone graft | ? | ? | ? |
| 6 | Colletti et al. (2014) [27] | ?/F | ? | ? | ? | ? | ? | CT:sunburst pattern | En bloc resection | Lower lip incision | Split calvarial bone graft | ? | ? | ? |
| 7 | Colletti et al. (2014) [27] | ?/F | ? | ? | ? | ? | ? | ? | En bloc resection | Lower lip incision | Split calvarial bone graft | ? | ? | ? |
| 8 | Xiuling Huang (2017) [1] | 35/F | L/2.5 × 2.5 cm | 7 y | N | N | N | CT: sunburst pattern of radiating trabeculae with intact cortices | Excision | Lower-eyelid incision | free iliac bone graft and minititanium plate | N | 3 y, no recurrence | ? |
| 9 | Xiuling Huang (2017) [1] | 41/F | L/1.5 cm | 2 y | N | N | N | CT: sunburst pattern of radiating trabeculae with intact cortices | Partial resection | Lower-eyelid incision | N | N | 2 y, no recurrence | ? |
| 10 | Xiuling Huang (2017) [1] | 44/F | L/2 cm | 3 m | Y | N | N | CT: well defined bone eminence | Partially resected | lower eyelid incision | N | N | 12 y, no recurrence | ? |
| 11 | Xiuling Huang (2017) [1] | 49/F | R/1 cm | 4 m | N | N | N | CT: well-defined radiolucency with trabecular density inside | Aggressive curettage | ? | N | N | 7 y, no recurrence | ? |
| 12 | Zoltán Fábián et al. (2018) [4] | 15/M | L/100 cm3 | 4 y | Y | Y, left eye dislocated to medial and cranial, mildly limited mobility | Y | CT: expanded zygomatic bone | Preoperative embo- lization; Complete resection | Weber-Fergusson -Dieffenbach incision | Patient Specific Implant | Y, during biopsy Y, moderate | ? | ? |
| 13 | Antúnez-Conde et al(2021) [54] | 55/M | L/1.5 cm | Many years | Y | N | N | CT: "honeycombed osseous lesion", MRI | Excision | Coronal and subciliary | Patient Specific Implant | N | 6 m, no recurrence | GLUT-1 negative |
References
- Huang, X.; An, J.; Zhang, Y.; Cai, Z. Intraosseous Venous Malformations of the Zygoma: Report of 4 Cases and Literature Review. Ann. Otol. Rhinol. Laryngol. 2017, 126, 505–509. [Google Scholar] [CrossRef]
- Powers, D.B.; Fisher, E.; Erdmann, D. Zygomatic Intraosseous Hemangioma: Case Report and Literature Review. Cranio-Maxillofac. Trauma Reconstr. 2017, 10, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Mulliken, J.B.; Glowacki, J. Hemangiomas and vascular malformations in infants and children: A classification based on endothelial characteristics. Plast. Reconstr. Surg. 1982, 69, 412–422. [Google Scholar] [CrossRef] [PubMed]
- Fábián, Z.; Szabó, G.; Petrovan, C.; Horváth, K.U.; Babicsák, B.; Hüttl, K.; Németh, Z.; Bogdán, S. Intraosseous venous malformation of the zygomatico-orbital complex. Case report and literature review with focus on confusions in vascular lesion terms. Oral Maxillofac. Surg. 2018, 22, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Guijarro-Martínez, R.; Morales-Navarro, J.D.; Solís-García, I.; Ventura-Martínez, N.; Marqués-Mateo, M.; Puche-Torres, M. Malformación venosa intraósea primaria en hueso cigomático: Actualización en criterios diagnósticos. Rev. Esp. Cir. Oral Maxilofac. 2013, 35, 170–174. [Google Scholar] [CrossRef] [Green Version]
- Cuéllar, C.N.; Rial, M.T.; Antúnez-Conde, R.; Caicoya, S.O.; Cuéllar, I.N.; de Frutos, G.A.; Ángela, S.U.; Alonso, M.G.-H.; Vila, C.N.; Escobar, J.S. Virtual Surgical Planning, Stereolitographic Models and CAD/CAM Titanium Mesh for Three-Dimensional Reconstruction of Fibula Flap with Iliac Crest Graft and Dental Implants. J. Clin. Med. 2021, 10, 1922. [Google Scholar] [CrossRef] [PubMed]
- Thakker, J.S.; Pace, M.; Lowe, I.; Jung, P.; Herford, A.S. Virtual Surgical Planning in Maxillofacial Trauma. Atlas Oral Maxillofac. Surg. Clin. 2019, 27, 143–155. [Google Scholar] [CrossRef] [PubMed]
- Srinivasan, B.; Ethunandan, M.; Van Der Horst, C.; Markus, A. Intraosseous ‘haemangioma’ of the zygoma: More appropriately termed a venous malformation. Int. J. Oral Maxillofac. Surg. 2009, 38, 1066–1070. [Google Scholar] [CrossRef]
- Chepurnyi, Y.; Chernogorskyi, D.; Kopchak, A.; Petrenko, O. Clinical efficacy of peek patient-specific implants in orbital reconstruction. J. Oral Biol. Craniofac. Res. 2020, 10, 49–53. [Google Scholar] [CrossRef]
- Schlittler, F.; Vig, N.; Burkhard, J.; Lieger, O.; Michel, C.; Holmes, S. What are the limitations of the non-patient-specific implant in titanium reconstruction of the orbit? Br. J. Oral Maxillofac. Surg. 2020, 58, e80–e85. [Google Scholar] [CrossRef]
- Bathala, L.; Majeti, V.; Rachuri, N.; Singh, N.; Gedela, S. The Role of Polyether Ether Ketone (Peek) in Dentistry—A Review. J. Med. Life 2019, 12, 5–9. [Google Scholar] [CrossRef] [PubMed]
- Kilcline, C.; Frieden, I.J. Infantile Hemangiomas: How Common Are They? A Systematic Review of the Medical Literature. Pediatr. Dermatol. 2008, 25, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Drolet, B.A.; Swanson, E.A.; Frieden, I. Infantile Hemangiomas: An Emerging Health Issue Linked to an Increased Rate of Low Birth Weight Infants. J. Pediatr. 2008, 153, 712–715.e1. [Google Scholar] [CrossRef] [PubMed]
- Haggstrom, A.N.; Drolet, B.A.; Baselga, E.; Chamlin, S.L.; Garzon, M.C.; Horii, K.A. Prospective Study of Infantile Heman-giomas: Demographic, Prenatal, and Perinatal Characteristics. J. Pediatr. 2007, 150, 291–294. [Google Scholar] [CrossRef]
- Liang, M.G.; Frieden, I.J. Infantile and congenital hemangiomas. Semin. Pediatr. Surg. 2014, 23, 162–167. [Google Scholar] [CrossRef]
- Dickison, P.; Christou, E.; Wargon, O. A Prospective Study of Infantile Hemangiomas with a Focus on Incidence and Risk Factors. Pediatr. Dermatol. 2011, 28, 663–669. [Google Scholar] [CrossRef]
- McKenna, S.J.; Roddy, S. Delayed management of a mandibular vascular malformation. J. Oral Maxillofac. Surg. 1989, 47, 517–522. [Google Scholar] [CrossRef]
- Boon, L.M.; Enjolras, O.; Mulliken, J.B. Congenital hemangioma: Evidence of accelerated involution. J. Pediatr. 1996, 128, 329–335. [Google Scholar] [CrossRef]
- Enjolras, O.; Mulliken, J.B.; Boon, L.M.; Wassef, M.; Kozakewich, H.P.; Burrows, P.E. Non involuting congenital hemangioma: A rare cutaneous vascular anomaly. Plast. Recons. Surg. 2001, 107, 1647–1654. [Google Scholar] [CrossRef] [Green Version]
- North, P.; Waner, M.; James, C.; Mizeracki, A.; Frieden, I.; Mihm, M.J. Congenital non progressive hemangioma: A distinct clinicopathologic entity unlike infantile hemangioma. Arch Dermatol. 2001, 137, 1607–1620. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, B.B.; Baumgartner, I.; Berlien, P.; Bianchini, G.; Burrows, P.; Gloviczki, P.; Huang, Y.; Laredo, J.; Loose, D.A.; Markovic, J.; et al. International Union of Phlebology (2015) Diagnosis and treatment of venous malformations. Consensus document of the International Union of Phlebology (IUP): Updated 2013. Int. Angiol. 2015, 34, 97–149. [Google Scholar] [PubMed]
- Fan, X.; Qiu, W.; Zhang, Z.; Mao, Q. Comparative study of clinical manifestation, plain-film radiography, and com-puted tomographic scan in arteriovenous malformations of the jaws. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endod. 2002, 94, 503–509. [Google Scholar] [CrossRef] [PubMed]
- McRae, M.Y.; Adams, S.; Pereira, J.; Parsi, K.; Wargon, O. Venous malformations: Clinical course and management of vascular birthmark clinic cases. Australas. J. Dermatol. 2012, 54, 22–30. [Google Scholar] [CrossRef]
- Nguyen, H.L.; Boon, L.M.; Vikkula, M. Genetics of vascular malformations. Semin. Pediatr. Surg. 2014, 23, 221–226. [Google Scholar] [CrossRef]
- Limaye, N.; Wouters, V.; Uebelhoer, M.; Tuominen, M. Somatic Mutations in the Angiopoietin- Receptor TIE2 Can Cause Both Solitary and Multiple Sporadic Venous Malformations. Nat. Genet. 2009, 41, 118–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kondylidou-Sidira, A.; Dietrich, E.-M.; Koloutsos, G.; Sakkas, L.; Antoniades, K. Intraosseous vascular malformation of the mandibular condyle: Presentation of a case and differential diagnosis. Oral Radiol. 2012, 28, 150–156. [Google Scholar] [CrossRef]
- Colletti, G.; Frigerio, A.; Giovanditto, F.; Biglioli, F.; Chiapasco, M.; Grimmer, J.F. Surgical treatment of vascular malfor-mations of the facial bones. J. Oral Maxillofac. Surg. 2014, 72, 1326.e1–1326.e18. [Google Scholar] [CrossRef]
- Ethunandan, M.; Mellor, T.K. Haemangiomas and vascular malformations of the maxillofacial region—A review. Br. J. Oral Maxillofac. Surg. 2006, 44, 263–272. [Google Scholar] [CrossRef]
- DeFazio, M.V.; Kassira, W.; Camison, L.; Meshkov, L.; Robinson, P.G.; Kawamoto, H.K.; Thaller, S.R. Intraosseous Venous Malformations of the Zygoma. Ann. Plast. Surg. 2014, 72, 323–327. [Google Scholar] [CrossRef]
- Moore, S.L.; Chun, J.K.; Mitre, S.A.; Som, P.M. Intraosseous Hemangioma of the Zygoma: CT and MR Findings. Am. J. Neuroradiol. 2001, 22, 1383–1385. [Google Scholar]
- Tokgoz, N.; Oner, Y.A.; Kaymaz, M. Primary intraosseous meningioma: CT and MRI appearance. AJNR Am. J. Neuro-Radiol. 2005, 26, 2053–2056. [Google Scholar]
- Ferrés-Amat, E.; Prats-Armengol, J.; Maura-Solivellas, I.; Ferrés-Amat, E.; Mareque-Bueno, J.; Ferrés-Padró, E. Gingival bleeding of a high-flow mandibular arteriovenous malformation in a child with 8-year follow-up. Case Rep. Pediatr. 2015, 2015, 745718. [Google Scholar] [CrossRef] [Green Version]
- Cheng, N.; Lai, D.-M.; Hsie, M.-H.; Liao, S.-L.; Chen, Y.-B.T. Intraosseous Hemangiomas of the Facial Bone. Plast. Reconstr. Surg. 2006, 117, 2366–2372. [Google Scholar] [CrossRef]
- Marshak, G. Hemangioma of the zygomatic bone. Arch. Otolaryngol. 1980, 106, 581–582. [Google Scholar] [CrossRef]
- Zins, J.E.; Turegun, M.C.; Hosn, W.; Bauer, T.W. Reconstruction of intraosseous hemangiomas of the midface using split cal-varial bone grafts. Plast. Reconstr. Surg. 2006, 117, 948–953. [Google Scholar] [CrossRef]
- Hamada, M.; Shimizu, H.; Takasu, A.; Nishiyama, K.; Yura, Y. Piezosurgery for intraosseous venous malformation of the mandible. Ann. Maxillofac. Surg. 2018, 8, 333–336. [Google Scholar] [CrossRef]
- Clauser, L.; Meneghini, F.; Riga, M.; Rigo, L. Haemangioma of the Zygoma. Report of two cases with a review of the literature. J Cranio-Maxillofac. Surg. 1991, 19, 353–358. [Google Scholar] [CrossRef]
- Chen, Y.-B.T.; Wornom, I.L.; Whitaker, L.A. Intraosseous Vascular Malformations of the Orbit. Plast. Reconstr. Surg. 1991, 87, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Gil, M.C.; Navarro-Vila, C. Intraosseous hemangioma of the zygomatic bone. A case report. Int. J. Oral Maxillofac. Surg. 1992, 21, 287–291. [Google Scholar]
- De Ponte, F.S.; Becelli, R.; Rinna, C.; Sassano, P.P. Aesthetic and functional reconstruction in intraosseus hemangiomas of the zygoma. J. Craniofac. Surg. 1995, 6, 506–509. [Google Scholar] [CrossRef] [PubMed]
- Pinna, V.; Clauser, L.; Marchi, M.; Castellan, L. Haemangioma of the zygoma: Case report. Neuroradiology 1997, 39, 216–218. [Google Scholar] [CrossRef]
- Savastano, G.; Russo, A.; Dell’Aquila, A. Osseous hemangioma of the zygoma: A case report. J. Oral Maxillofac. Surg. 1997, 55, 1352–1356. [Google Scholar] [CrossRef]
- Konior, R.J.; Kelley, T.F.; Hemmer, D. Intraosseus zygomatic hemangioma. Otolaryngol. Neck Surg. 1999, 121, 122–125. [Google Scholar] [CrossRef]
- Ramchandani, P.L.; Sabesan, T.; Mellor, T.K. Intraosseous vascular anomaly (haemangioma) of the zygoma. Br. J. Oral Maxillofac. Surg. 2004, 42, 583–586. [Google Scholar] [CrossRef]
- Gómez, E.; González, T.; Arias, J.; Lasaletta, L. Three-dimensional reconstruction after removal of zygomatic intraosseous hemangioma. Oral Maxillofac. Surg. 2008, 12, 159–162. [Google Scholar] [CrossRef]
- Matsumiya, T.; Nemoto, H.; Kasai, Y.; Maruyama, N.; Sumiya, N. Intraosseous venous malformation of the zygoma: A case report and literature review. Int. J. Surg. Case Rep. 2015, 12, 132–136. [Google Scholar] [CrossRef] [Green Version]
- Har-El, G.; Hadar, T.; Zirkin, H.Y.; Sidi, J. Hemangioma of the Zygoma. Ann. Plast. Surg. 1987, 18, 533–540. [Google Scholar] [CrossRef] [PubMed]
- Jeter, T.S.; Hackney, F.L.; Aufdemorte, T.B. Cavernous hemangioma of the zygoma: Report of cases. J. Oral Maxillofac. Surg. 1990, 48, 508–512. [Google Scholar] [CrossRef]
- Pokala, A.; Devulapally, R.V.; Tejasvi, M.L.A.; Nedunooru, S. Central hemangioma of Zygoma—A rare case report with CT and MRI features. Indian J Pathol. Microbiol. 2021, 64, 334–338. [Google Scholar]
- Davis, E.; Morgan, L.R. Hemangioma of Bone. Arch. Otolaryngol. Head Neck Surg. 1974, 99, 443–445. [Google Scholar] [CrossRef] [PubMed]
- Valentini, V.; Nicolai, G.; Lorè, B.; Aboh, I.V. Intraosseous hemangiomas. J. Craniofac. Surg. 2008, 19, 1459–1464. [Google Scholar] [CrossRef]
- Choi, J.S.; Bae, Y.C.; Kang, G.B.; Choi, K.-U. Intraosseous hemangioma of the orbit. Arch. Craniofac. Surg. 2018, 19, 68–71. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arribas-Garcia, I.; Alcala-Galiano, A.; Garcia, A.F.; Montalvo, J.J. Zygomatic intraosseous haemangioma: Reconstruction with an alloplastic prosthesis based on a 3-D model. J. Plast. Reconstr. Aesthet. Surg. 2010, 63, e451–e453. [Google Scholar] [CrossRef] [PubMed]
- Antúnez-Conde, R.; Salmerón, J.I.; Navarro, C. Intraosseous Venous Malformation of the Zygomatic Bone: Virtual Surgical Planning and Reconstruction With Customized CAD-CAM Titanium Implant. J. Craniofac. Surg. 2021. [Google Scholar] [CrossRef] [PubMed]








| Age /Sex | Size cm. | Evolution | Clinics | Aesthetic Result | Histology | Sequelae/ Recurrence | Surgical Time (min.) | Coverage of Defect (%) | Hospital Days | Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 35/M | 1.5 | 10y | Pain | Good | Vascular malf. | Scalp scar dysesthesia, Pain/N | 210 | 71 | 4 | 15y |
| Case 2 | 41/F | 2 | 20y | No | Good | Venous malf. | Scalp scar dysesthesia/N | 180 | 79 | 6 | 11y |
| Case 3 | 55/M | 1 | 10m | No | Poor | Venous malf. | Scalp scar dysesthesia. Lagophtalmos/N Discomfort due to osteosynthesis material | 175 | 87 | 5 | 10y |
| Case 4 | 47/F | 1.5 | 7y | No | Excelent | Venous malf. | N/N | 190 | 82 | 4 | 6y |
| Age /Sex | Size cm. | Evolu-tion | Clinics | Aesthetic Result | Histology | Sequelae/ Recurrence | Surgical Time Min. | Coverage of Defect % | Hospital Days | Follow-Up | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Case 1 | 55/F | 1.5 | 20y | Pain | Excelent | Venous malf. | N/N | 143 | 100% | 2 | 5y |
| Case 2 | 60/F | 2 | 20y | No | Good | Venous malf. | Frontal paresia /N | 124 | 100% | 2 | 3y |
| Case 3 | 39/M | 1 | 2y | No | Excelent | Venous malf. | N/N | 99 | 100% | 1 | 3y |
| Case 4 | 40/F | 1.2 | 10y | No | Excelent | Venous malf. | N/N | 118 | 100% | 2 | 2y |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antúnez-Conde, R.; Navarro Cuéllar, C.; Salmerón Escobar, J.I.; Díez-Montiel, A.; Navarro Cuéllar, I.; Dell’Aversana Orabona, G.; del Castillo Pardo de Vera, J.L.; Navarro Vila, C.; Cebrián Carretero, J.L. Intraosseous Venous Malformation of the Zygomatic Bone: Comparison between Virtual Surgical Planning and Standard Surgery with Review of the Literature. J. Clin. Med. 2021, 10, 4565. https://doi.org/10.3390/jcm10194565
Antúnez-Conde R, Navarro Cuéllar C, Salmerón Escobar JI, Díez-Montiel A, Navarro Cuéllar I, Dell’Aversana Orabona G, del Castillo Pardo de Vera JL, Navarro Vila C, Cebrián Carretero JL. Intraosseous Venous Malformation of the Zygomatic Bone: Comparison between Virtual Surgical Planning and Standard Surgery with Review of the Literature. Journal of Clinical Medicine. 2021; 10(19):4565. https://doi.org/10.3390/jcm10194565
Chicago/Turabian StyleAntúnez-Conde, Raúl, Carlos Navarro Cuéllar, José Ignacio Salmerón Escobar, Alberto Díez-Montiel, Ignacio Navarro Cuéllar, Giovanni Dell’Aversana Orabona, José Luis del Castillo Pardo de Vera, Carlos Navarro Vila, and José Luis Cebrián Carretero. 2021. "Intraosseous Venous Malformation of the Zygomatic Bone: Comparison between Virtual Surgical Planning and Standard Surgery with Review of the Literature" Journal of Clinical Medicine 10, no. 19: 4565. https://doi.org/10.3390/jcm10194565