
AIM2 Inflammasome in Tumor Cells as a Biomarker for Predicting the Treatment Response to Antiangiogenic Therapy in Epithelial Ovarian Cancer Patients

 , , , and
, , , and 
Abstract
:1. Introduction
2. Materials and Methods
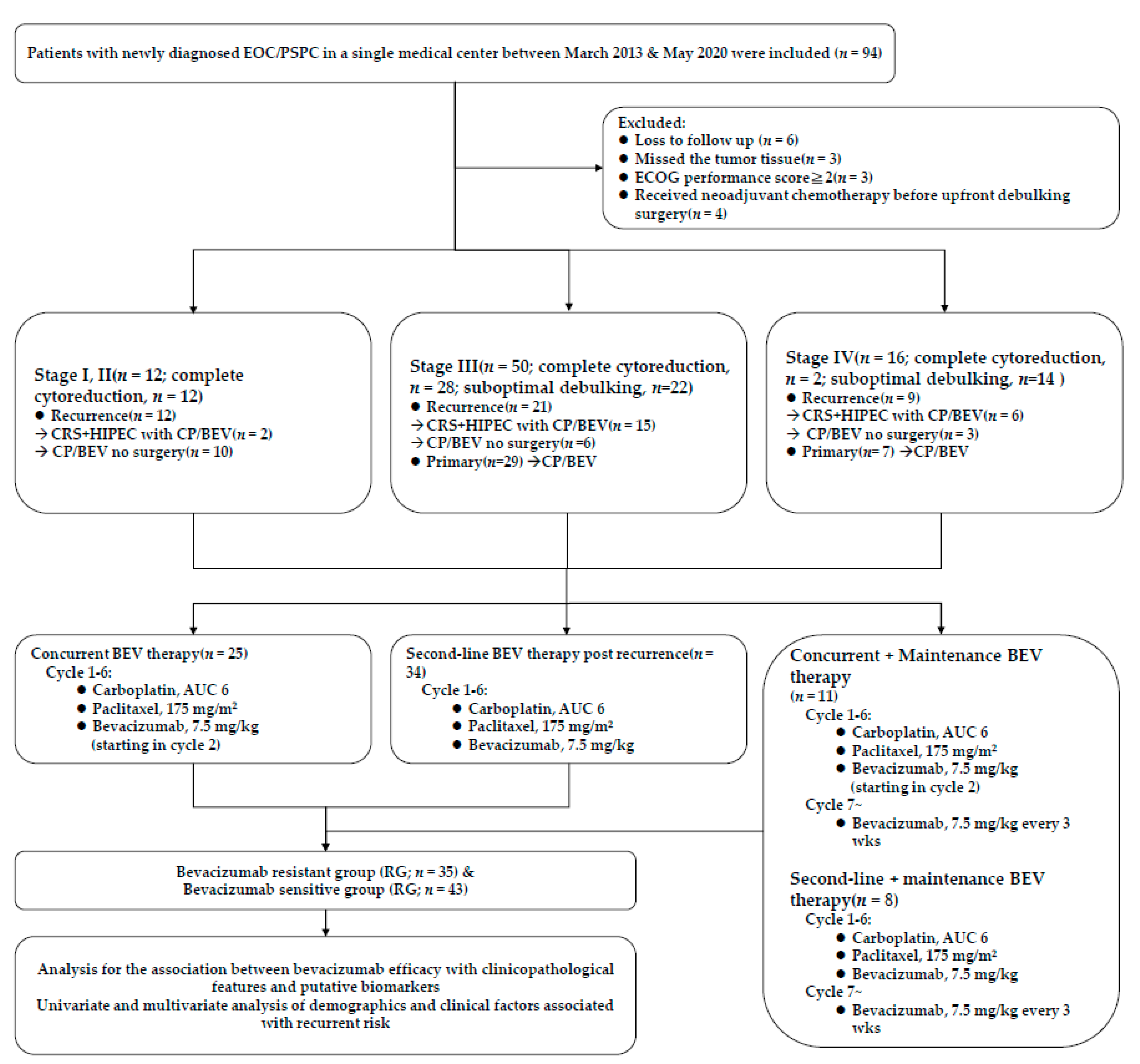
2.1. Patients and Specimens
2.2. Tissue Microarray
2.3. Immunohistochemistry Staining
2.4. Evaluation of AIM2, C3 and C5 Expression
2.5. Statistical Analysis
3. Results
3.1. Clinicopathological Characteristics in 78 Patients
3.2. Identification of Predictive Markers
3.3. Predictive Associations between IHC Scores for AIM2, C3, and C5 in Tumor Cells and Survival Outcome
3.4. Univariate and Multivariate Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bray, F.; Ferlay, J.; Soerjomataram, I.; Siegel, R.L.; Torre, L.A.; Jemal, A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA A Cancer J. Clin. 2018, 68, 394–424. [Google Scholar] [CrossRef] [Green Version]
- Lheureux, S.; Gourley, C.; Vergote, I.; Oza, A.M. Epithelial ovarian cancer. Lancet 2019, 393, 1240–1253. [Google Scholar] [CrossRef] [Green Version]
- Doherty, J.A.; Peres, L.C.; Wang, C.; Way, G.P.; Greene, C.S.; Schildkraut, J.M. Challenges and Opportunities in Studying the Epidemiology of Ovarian Cancer Subtypes. Curr. Epidemiol. Rep. 2017, 4, 211–220. [Google Scholar] [CrossRef]
- Chung, A.S.; Lee, J.; Ferrara, N. Targeting the tumour vasculature: Insights from physiological angiogenesis. Nat. Rev. Cancer 2010, 10, 505–514. [Google Scholar] [CrossRef]
- Zhao, Y.; Adjei, A.A. Targeting Angiogenesis in Cancer Therapy: Moving Beyond Vascular Endothelial Growth Factor. Oncol. 2015, 20, 660–673. [Google Scholar] [CrossRef] [Green Version]
- Oza, A.M.; Cook, A.D.; Pfisterer, J.; Embleton, A.; Ledermann, J.A.; Pujade-Lauraine, E.; Kristensen, G.; Carey, M.S.; Beale, P.; Cervantes, A.; et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): Overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015, 16, 928–936. [Google Scholar] [CrossRef]
- Aghajanian, C.; Blank, S.V.; Goff, B.A.; Judson, P.L.; Teneriello, M.G.; Husain, A.; Sovak, M.A.; Yi, J.; Nycum, L.R. OCEANS: A Randomized, Double-Blind, Placebo-Controlled Phase III Trial of Chemotherapy With or Without Bevacizumab in Patients With Platinum-Sensitive Recurrent Epithelial Ovarian, Primary Peritoneal, or Fallopian Tube Cancer. J. Clin. Oncol. 2012, 30, 2039–2045. [Google Scholar] [CrossRef] [Green Version]
- Pujade-Lauraine, E.; Hilpert, F.; Weber, B.; Reuss, A.; Poveda, A.; Kristensen, G.; Sorio, R.; Vergote, I.; Witteveen, P.; Bamias, A.; et al. Bevacizumab Combined With Chemotherapy for Platinum-Resistant Recurrent Ovarian Cancer: The AURELIA Open-Label Randomized Phase III Trial. J. Clin. Oncol. 2014, 32, 1302–1308. [Google Scholar] [CrossRef]
- Coleman, R.L.; Brady, M.F.; Herzog, T.J.; Sabbatini, P.; Armstrong, D.K.; Walker, J.L.; Kim, B.-G.; Fujiwara, K.; Tewari, K.S.; O’Malley, D.M.; et al. Bevacizumab and paclitaxel–carboplatin chemotherapy and secondary cytoreduction in recurrent, platinum-sensitive ovarian cancer (NRG Oncology/Gynecologic Oncology Group study GOG-0213): A multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2017, 18, 779–791. [Google Scholar] [CrossRef] [Green Version]
- Tewari, K.S.; Burger, R.A.; Enserro, D.; Norquist, B.M.; Swisher, E.M.; Brady, M.F.; Bookman, M.A.; Fleming, G.F.; Huang, H.; Homesley, H.D.; et al. Final Overall Survival of a Randomized Trial of Bevacizumab for Primary Treatment of Ovarian Cancer. J. Clin. Oncol. 2019, 37, 2317–2328. [Google Scholar] [CrossRef]
- Han, E.S.; Burger, R.A.; Darcy, K.M.; Sill, M.W.; Randall, L.M.; Chase, D.; Parmakhtiar, B.; Monk, B.J.; Greer, B.E.; Connelly, P.; et al. Predictive and prognostic angiogenic markers in a gynecologic oncology group phase II trial of bevacizumab in recurrent and persistent ovarian or peritoneal cancer. Gynecol. Oncol. 2010, 119, 484–490. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Secord, A.A.; Nixon, A.B.; Hurwitz, H.I. The search for biomarkers to direct antiangiogenic treatment in epithelial ovarian cancer. Gynecol. Oncol. 2014, 135, 349–358. [Google Scholar] [CrossRef] [PubMed]
- Hegde, P.S.; Jubb, A.M.; Chen, D.; Li, N.F.; Meng, Y.G.; Bernaards, C.; Elliott, R.; Scherer, S.J.; Chen, D. Predictive Impact of Circulating Vascular Endothelial Growth Factor in Four Phase III Trials Evaluating Bevacizumab. Clin. Cancer Res. 2013, 19, 929–937. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schmitt, J.; Matei, D. Targeting angiogenesis in ovarian cancer. Cancer Treat. Rev. 2012, 38, 272–283. [Google Scholar] [CrossRef]
- Chang, C.-M.; Wang, M.-L.; Lu, K.-H.; Yang, Y.-P.; Juang, C.-M.; Wang, P.-H.; Hsu, R.-J.; Yu, M.-H.; Chang, C.-C. Integrating the dysregulated inflammasome-based molecular functionome in the malignant transformation of endometriosis-associated ovarian carcinoma. Oncotarget 2017, 9, 3704–3726. [Google Scholar] [CrossRef] [Green Version]
- Sharma, B.R.; Karki, R.; Kanneganti, T. Role of AIM2 inflammasome in inflammatory diseases, cancer and infection. Eur. J. Immunol. 2019, 49, 1998–2011. [Google Scholar] [CrossRef] [Green Version]
- Karki, R.; Kanneganti, T.-D. Diverging inflammasome signals in tumorigenesis and potential targeting. Nat. Rev. Cancer 2019, 19, 197–214. [Google Scholar] [CrossRef]
- Farshchian, M.; Nissinen, L.; Siljamäki, E.; Riihilä, P.; Piipponen, M.; Kivisaari, A.; Kallajoki, M.; Grénman, R.; Peltonen, J.; Peltonen, S.; et al. Tumor cell-specific AIM2 regulates growth and invasion of cutaneous squamous cell carcinoma. Oncotarget 2017, 8, 45825–45836. [Google Scholar] [CrossRef]
- Chang, C.-M.; Yang, Y.-P.; Chuang, J.-H.; Chuang, C.-M.; Lin, T.-W.; Wang, P.-H.; Yu, M.-H.; Chang, C.-C. Discovering the Deregulated Molecular Functions Involved in Malignant Transformation of Endometriosis to Endometriosis-Associated Ovarian Carcinoma Using a Data-Driven, Function-Based Analysis. Int. J. Mol. Sci. 2017, 18, 2345. [Google Scholar] [CrossRef] [Green Version]
- Cuzick, J.; Otto, F.; Baron, J.A.; Brown, P.H.; Burn, J.; Greenwald, P.; Jankowski, J.; La Vecchia, C.; Meyskens, F.; Senn, H.J.; et al. Aspirin and non-steroidal anti-inflammatory drugs for cancer prevention: An international consensus statement. Lancet Oncol. 2009, 10, 501–507. [Google Scholar] [CrossRef] [Green Version]
- Bjørge, L.; Hakulinen, J.; Vintermyr, O.K.; Jarva, H.; Jensen, T.S.; E Iversen, O.; Meri, S. Ascitic complement system in ovarian cancer. Br. J. Cancer 2005, 92, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Su, K.-M.; Lin, T.-W.; Liu, L.-C.; Yang, Y.-P.; Wang, M.-L.; Tsai, P.-H.; Wang, P.-H.; Yu, M.-H.; Chang, C.-M.; Chang, C.-C. The Potential Role of Complement System in the Progression of Ovarian Clear Cell Carcinoma Inferred from the Gene Ontology-Based Immunofunctionome Analysis. Int. J. Mol. Sci. 2020, 21, 2824. [Google Scholar] [CrossRef] [Green Version]
- Trinchieri, G. Cancer and Inflammation: An Old Intuition with Rapidly Evolving New Concepts. Annu. Rev. Immunol. 2012, 30, 677–706. [Google Scholar] [CrossRef] [PubMed]
- Balkwill, F.R.; Mantovani, A. Cancer-related inflammation: Common themes and therapeutic opportunities. Semin. Cancer Biol. 2012, 22, 33–40. [Google Scholar] [CrossRef]
- Hajishengallis, G.; Reis, E.S.; Mastellos, D.C.; Ricklin, D.; Lambris, J.D. Novel mechanisms and functions of complement. Nat. Immunol. 2017, 18, 1288–1298. [Google Scholar] [CrossRef]
- Katayama, Y.; Uchino, J.; Chihara, Y.; Tamiya, N.; Kaneko, Y.; Yamada, T.; Takayama, K. Tumor Neovascularization and Developments in Therapeutics. Cancers 2019, 11, 316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chellappan, D.K.; Leng, K.H.; Jia, L.J.; Aziz, N.A.B.A.; Hoong, W.C.; Qian, Y.C.; Ling, F.Y.; Wei, G.S.; Ying, T.; Chellian, J.; et al. The role of bevacizumab on tumour angiogenesis and in the management of gynaecological cancers: A review. Biomed. Pharmacother. 2018, 102, 1127–1144. [Google Scholar] [CrossRef]
- Wade, K.S.; Brady, M.; Thai, T.; Wang, Y.; Zheng, B.; Salani, R.; Tewari, K.; Gray, H.; Bakkum-Gamez, J.; Burger, R.; et al. Measurements of adiposity as prognostic biomarkers for survival with anti-angiogenic treatment in epithelial ovarian cancer: An NRG Oncology/Gynecologic Oncology Group ancillary data analysis of GOG 218. Gynecol. Oncol. 2019, 155, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-W.; West, X.Z.; Byzova, T.V. Inflammation and oxidative stress in angiogenesis and vascular disease. J. Mol. Med. 2013, 91, 323–328. [Google Scholar] [CrossRef] [Green Version]
- González Martín, A.; Oza, A.M.; Embleton, A.C.; Pfisterer, J.; Ledermann, J.A.; Pujade-Lauraine, E.; Perren, T. Exploratory outcome analyses according to stage and/or residual disease in the ICON7 trial of carboplatin and paclitaxel with or without bevacizumab for newly diagnosed ovarian cancer. Gynecol. Oncol. 2019, 152, 53–60. [Google Scholar] [CrossRef] [Green Version]
- Raja, F.A.; Hook, J.M.; Ledermann, J.A. Biomarkers in the development of anti-angiogenic therapies for ovarian cancer. Cancer Treat. Rev. 2012, 38, 662–672. [Google Scholar] [CrossRef] [PubMed]
- Gerger, A.; LaBonte, M.; Lenz, H.-J. Molecular Predictors of Response to Antiangiogenesis Therapies. Cancer J. 2011, 17, 134–141. [Google Scholar] [CrossRef] [PubMed]
- Secord, A.A.; Burdett, K.B.; Owzar, K.; Tritchler, D.; Sibley, A.B.; Liu, Y.; Starr, M.D.; Brady, J.C.; Lankes, H.A.; Hurwitz, H.I.; et al. Predictive Blood-Based Biomarkers in Patients with Epithelial Ovarian Cancer Treated with Carboplatin and Paclitaxel with or without Bevacizumab: Results from GOG-0218. Clin. Cancer Res. 2020, 26, 1288–1296. [Google Scholar] [CrossRef] [PubMed] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Bevacizumab Sensitive Group (SG; n = 43) | Bevacizumab Resistant Group (RG; n = 35) | ||
|---|---|---|---|
| No. (%) | No. (%) | p Value | |
| Age, M(SD) | 58.2(9.6) | 60.1(8.6) | 0.510 |
| BMI, M(SD) | 22.8(3.7) | 24.5(4.1) | 0.051 |
| Number of BEV used times, M(SD) | 13.4(9.1) | 10.9(7.6) | 0.189 |
| Origin | 0.456 | ||
| Ovary | 40(57.1) | 30(42.9) | |
| PSPC | 3(37.5) | 5(62.5) | |
| Tumor marker | 0.499 | ||
| CA-125 > 35 U/mL | 41(53.9) | 35(46.1) | |
| CA-125 > 70 U/mL | 40(53.3) | 35(46.7) | |
| CA-125 > 105 U/mL | 38(52.1) | 35(47.9) | |
| FIGO stage | 0.088 | ||
| I | 6(85.7) | 1(14.3) | |
| II | 3(60) | 2(40) | |
| III | 29(58) | 21(42) | |
| IV | 5(31.2) | 11(68.8) | |
| Histology | 0.455 | ||
| other adenocarcinoma | 4(57.1) | 3(42.9) | |
| serous | 30(51.7) | 28(48.3) | |
| endometrioid | 4 (100) | 0(0) | |
| clear cell | 4(57.1) | 3(42.9) | |
| mucinous | 1(50) | 1(50) | |
| Surgery | |||
| Complete cytoreduction (CC 0/1) | 24(75) | 8(25) | 0.007 |
| Suboptimal | 9(39.1) | 14(60.9) | 0.112 |
| CRS + HIPEC | 10(43.5) | 13(56.5) | 0.277 |
| BEV therapy | |||
| Maintenance | |||
| Concurrent (Maintenance | 10(90.9) | 1(9.1) | 0.019 |
| Second-line(Maintenance | 5(62.5) | 3(37.5) | 0.724 |
| Concurrent | 15(60) | 10(40) | 0.726 |
| Second-line | 13(38.2) | 21(61.8) | 0.016 |
| AIM2 score, M(SD) | 297.1(27.7) | 355.5(43.3) | <0.001 |
| ≤310 | 38(88.4) | 9(25.7) | <0.001 |
| >310 | 5(11.6) | 26(74.3) | |
| C3 score, M(SD) | 285.4(36.5) | 306.9(65.7) | 0.077 |
| C5 score, M(SD) | 229.3(31.6) | 243.6(57.2) | 0.326 |
| Platinum Sensitive Group (PS; n = 26) | Platinum Resistant Group (PR; n = 16) | ||
|---|---|---|---|
| No. (%) | No. (%) | p Value | |
| AIM2 score, M(SD) | 313.8(25.2) | 331.6(38.9) | 0.178 |
| C3 score, M(SD) | 291.3(38.2) | 304.2(62.2) | 0.302 |
| C5 score, M(SD) | 221.5(28.9) | 238.4(48.6) | 0.196 |
| Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|
| Crude HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | |
| Age | 1.01 (0.98–1.04) | 0.609 | 1.00 (0.97–1.04) | 0.993 |
| BMI | 1.06 (0.99–1.13) | 0.100 | 0.96 (0.89–1.04) | 0.350 |
| Number of BEV used times | 0.96 (0.93–0.99) | 0.021 | 0.98 (0.91–1.06) | 0.590 |
| FIGO (III + IV vs. I + II) | 9.41 (2.25–39.4) | 0.002 | 26.14 (4.06–168.24) | 0.001 |
| Histology (others vs. serous) | 0.67 (0.33–1.34) | 0.255 | 0.93 (0.38–2.26) | 0.871 |
| CA-125 Surgery | 21.33 (0.02–21.27) | 0.384 | N/A | |
| Complete cytoreduction (CC 0/1) | 1.00 (reference) | (reference) | 1.00 (reference) | (reference) |
| Suboptimal | 2.69 (1.30–5.56) | 0.008 | 1.27 (0.55–2.91) | 0.578 |
| CRS + HIPEC BEV therapy | 1.88 (0.90–3.90) | 0.091 | 1.29 (0.57–2.91) | 0.545 |
| Concurrent | 1.00 (reference) | (reference) | 1.00 (reference) | (reference) |
| Second-line | 1.82 (0.96–3.46) | 0.067 | 1.58 (0.66–3.79) | 0.303 |
| Maintenance | 0.37 (0.15–0.92) | 0.033 | 0.11 (0.02–0.62) | 0.012 |
| AIM2 score (>310 vs. <=310) | 2.79 (1.50–5.18) | 0.001 | 4.44 (2.01–9.80) | <0.001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsu, P.-C.; Chao, T.-K.; Chou, Y.-C.; Yu, M.-H.; Wang, Y.-C.; Lin, Y.-H.; Lee, Y.-L.; Liu, L.-C.; Chang, C.-C. AIM2 Inflammasome in Tumor Cells as a Biomarker for Predicting the Treatment Response to Antiangiogenic Therapy in Epithelial Ovarian Cancer Patients. J. Clin. Med. 2021, 10, 4529. https://doi.org/10.3390/jcm10194529
Hsu P-C, Chao T-K, Chou Y-C, Yu M-H, Wang Y-C, Lin Y-H, Lee Y-L, Liu L-C, Chang C-C. AIM2 Inflammasome in Tumor Cells as a Biomarker for Predicting the Treatment Response to Antiangiogenic Therapy in Epithelial Ovarian Cancer Patients. Journal of Clinical Medicine. 2021; 10(19):4529. https://doi.org/10.3390/jcm10194529
Chicago/Turabian StyleHsu, Po-Chao, Tai-Kuang Chao, Yu-Ching Chou, Mu-Hsien Yu, Yu-Chi Wang, Yi-Hsin Lin, Yi-Liang Lee, Li-Chun Liu, and Cheng-Chang Chang. 2021. "AIM2 Inflammasome in Tumor Cells as a Biomarker for Predicting the Treatment Response to Antiangiogenic Therapy in Epithelial Ovarian Cancer Patients" Journal of Clinical Medicine 10, no. 19: 4529. https://doi.org/10.3390/jcm10194529