
Association between Serum Osteoprotegerin Levels and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
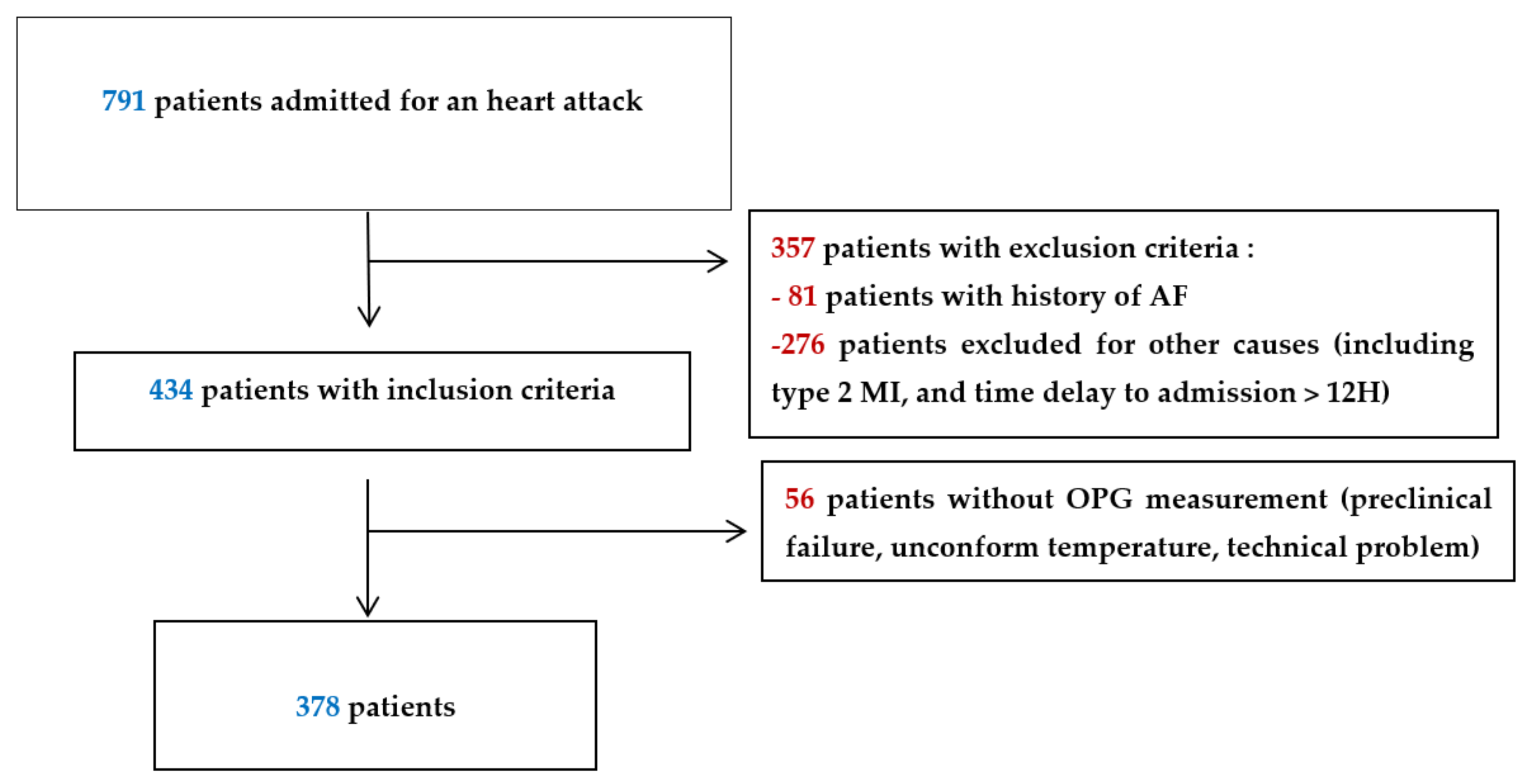
2.1. Population
2.2. Data Collection
2.3. Serum OPG Level Assessment
2.4. Coronary Angiography
2.5. Statistical Analysis
3. Results
4. Discussion
4.1. OPG Is Associated with the Severity of Coronary Artery Disease
4.2. OPG as a New Biomarker in Coronary Artery Disease
4.3. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Collin-Osdoby, P. Regulation of vascular calcification by osteoclast regulatory factors RANKL and osteoprotegerin. Circ. Res. 2004, 95, 1046–1057. [Google Scholar] [CrossRef]
- Hofbauer, L.C.; Khosla, S.; Dunstan, C.R.; Lacey, D.L.; Boyle, W.J.; Riggs, B.L. The roles of osteoprotegerin and osteoprotegerin ligand in the paracrine regulation of bone resorption. J. Bone Miner. Res. 2000, 15, 2–12. [Google Scholar] [CrossRef]
- Emery, J.G.; McDonnell, P.; Burke, M.B.; Deen, K.C.; Lyn, S.; Silverman, C.; Dul, E.; Appelbaum, E.R.; Eichman, C.; DiPrinzio, D.; et al. Osteoprotegerin is a receptor for the cytotoxic ligand TRAIL. J. Biol. Chem. 1998, 273, 14363–14367. [Google Scholar] [CrossRef] [Green Version]
- Schoppet, M.; Preissner, K.T.; Hofbauer, L.C. RANK ligand and osteoprotegerin: Paracrine regulators of bone metabolism and vascular function. Arterioscler. Thromb. Vasc. Biol. 2002, 22, 549–553. [Google Scholar] [CrossRef] [Green Version]
- Hao, Y.; Tsuruda, T.; Sekita-Hatakeyama, Y.; Kurogi, S.; Kubo, K.; Sakamoto, S.; Nakamura, M.; Udagawa, N.; Sekimoto, T.; Hatakeyama, K.; et al. Cardiac hypertrophy is exacerbated in aged mice lacking the osteoprotegerin gene. Cardiovasc. Res. 2016, 110, 62–72. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harper, E.; Forde, H.; Davenport, C.; Rochfort, K.D.; Smith, D.; Cummins, P.M. Vascular calcification in type-2 diabetes and cardiovascular disease: Integrative roles for OPG, RANKL and TRAIL. Vascul. Pharmacol. 2016, 82, 30–40. [Google Scholar] [CrossRef] [PubMed]
- Kiechl, S.; Schett, G.; Wenning, G.; Redlich, K.; Oberhollenzer, M.; Mayr, A.; Santer, P.; Smolen, J.; Poewe, W.; Willeit, J. Osteoprotegerin is a risk factor for progressive atherosclerosis and cardiovascular disease. Circulation 2004, 109, 2175–2180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vik, A.; Mathiesen, E.B.; Brox, J.; Wilsgaard, T.; Njølstad, I.; Jørgensen, L.; Hansen, J.B. Serum osteoprotegerin is a predictor for incident cardiovascular disease and mortality in a general population: The Tromsø Study. J. Thromb. Haemost. 2011, 9, 638–644. [Google Scholar] [CrossRef]
- Abedin, M.; Omland, T.; Ueland, T.; Khera, A.; Aukrust, P.; Murphy, S.A.; Jain, T.; Gruntmanis, U.; McGuire, D.K.; de Lemos, J.A. Relation of osteoprotegerin to coronary calcium and aortic plaque (from the Dallas Heart Study). Am. J. Cardiol. 2007, 99, 513–518. [Google Scholar] [CrossRef]
- Jono, S.; Ikari, Y.; Shioi, A.; Mori, K.; Miki, T.; Hara, K.; Nishizawa, Y. Serum osteoprotegerin levels are associated with the presence and severity of coronary artery disease. Circulation 2002, 106, 1192–1194. [Google Scholar] [CrossRef] [Green Version]
- Schoppet, M.; Sattler, A.M.; Schaefer, J.R.; Herzum, M.; Maisch, B.; Hofbauer, L.C. Increased osteoprotegerin serum levels in men with coronary artery disease. J. Clin. Endocrinol. Metab. 2003, 88, 1024–1028. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Cottin, Y.; Vergely, C. The role of osteoprotegerin in the crosstalk between vessels and bone: Its potential utility as a marker of cardiometabolic diseases. Pharmacol. Ther. 2018, 182, 115–132. [Google Scholar] [CrossRef] [PubMed]
- Putot, A.; Chague, F.; Manckoundia, P.; Cottin, Y.; Zeller, M. Post-infectious Myocardial Infarction: New Insights for Improved Screening. J. Clin. Med. 2019, 8, 827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S.; et al. ESC Scientific Document GroupESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation. Eur. Heart J. 2018, 39, 119–177. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2020, 29, ehaa575. [Google Scholar] [CrossRef]
- Donal, E.; Place, C.D. Étude de la fonction systolique ventriculaire gauche par échocardiographie Doppler: Anciennes et nouvelles approches. MT Cardio. 2006, 2, 329–338. [Google Scholar]
- Kappetein, A.P.; Dawkins, K.D.; Mohr, F.W.; Morice, M.C.; Mack, M.J.; Russell, M.E.; Pomar, J.; Serruys, P.W.J.C. Current percutaneous coronary intervention and coronary artery bypass grafting practices for three-vessel and left main coronary artery disease. Insights from the SYNTAX run-in phase. Eur. Assoc. Cardiothorac. Surg. 2006, 29, 486–491. [Google Scholar] [CrossRef] [Green Version]
- Nakahara, T.; Dweck, M.R.; Narula, N.; Pisapia, D.; Narula, J.; Strauss, H.W. Coronary Artery Calcification: From Mechanism to Molecular Imaging. JACC Cardiovasc. Imaging 2017, 10, 582–593. [Google Scholar] [CrossRef]
- Lee, G.L.; Yeh, C.C.; Wu, J.Y.; Lin, H.C.; Wang, Y.F.; Kuo, Y.Y.; Hsieh, Y.T.; Hsu, Y.J.; Kuo, C.C. TLR2 Promotes Vascular Smooth Muscle Cell Chondrogenic Differentiation and Consequent Calcification via the Concerted Actions of Osteoprotegerin Suppression and IL-6-Mediated RANKL Induction. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 432–445. [Google Scholar] [CrossRef] [PubMed]
- Jono, S.; Otsuki, S.; Higashikuni, Y.; Shioi, A.; Mori, K.; Hara, K.; Hashimoto, H.; Ikari, Y. Serum osteoprotegerin levels and long-term prognosis in subjects with stable coronary artery disease. J. Thromb. Haemost. 2010, 8, 1170–1175. [Google Scholar] [CrossRef]
- Venuraju, S.M.; Yerramasu, A.; Corder, R.; Lahiri, A. Osteoprotegerin as a Predictor of Coronary Artery Disease and Cardiovascular Mortality and Morbidity. J. Am. Coll. Cardiol. 2010, 55, 2049–2061. [Google Scholar] [CrossRef] [Green Version]
- Kiechl, S.; Werner, P.; Knoflach, M.; Furtner, M.; Willeit, J.; Schett, G. The osteoprotegerin/RANK/RANKL system: A bone key to vascular disease. Expert. Rev. Cardiovasc. Ther. 2006, 4, 801–811. [Google Scholar] [CrossRef]
- Montecucco, F.; Steffens, S.; Mach, F. The immune response is involved in atherosclerotic plaque calcification: Could the RANKL/RANK/OPG system be a marker of plaque instability? Clin. Dev. Immunol. 2007, 2007, 75805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morisawa, T.; Nakagomi, A.; Kohashi, K.; Kosugi, M.; Kusama, Y.; Atarashi, H.; Shimizu, W. Osteoprotegerin is Associated With Endothelial Function and Predicts Early Carotid Atherosclerosis in Patients With Coronary Artery Disease. Int. Heart J. 2015, 56, 605–612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ghaffari, S.; Yaghoubi, A.; Baghernejad, R.; Sepehrvand, N.; Sokhanvar, S.; Haghjou, A.G. The value of serum osteoprotegerin levels in patients with angina like chest pain undergoing diagnostic coronary angiography. Cardiol. J. 2013, 20, 261–267. [Google Scholar] [CrossRef] [Green Version]
- Morena, M.; Dupuy, A.-M.; Jaussent, I.; Vernhet, H.; Gahide, G.; Klouche, K.; Bargnoux, A.-S.; Delcourt, C.; Canaud, B.; Cristol, J.-P. A cut-off value of plasma osteoprotegerin level may predict the presence of coronary artery calcifications in chronic kidney disease patients. Nephrol. Dial. Transplant. 2009, 24, 3389–3397. [Google Scholar] [CrossRef] [Green Version]
- Homorodean, C.; Iancu, A.C.; Dregoesc, I.M.; Spînu, M.; Ober, M.C.; Tãtaru, D.; Leucuta, D.; Olinic, M. Renal Failure Impact on the Outcomes of ST-Segment Elevation Myocardial Infarction Patients Due to a Left Main Coronary Culprit Lesion Treated Using a Primary Percutaneous Coronary Intervention. J. Clin. Med. 2019, 8, 565. [Google Scholar] [CrossRef] [Green Version]
- Lin, T.; Wang, L.; Guo, J.; Liu, P.; Chen, L.; Wei, M.; Li, G. Association Between Serum LDL-C and ApoB and SYNTAX Score in Patients With Stable Coronary Artery Disease. Angiology 2018, 69, 724–729. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.-J.; Song, Y.; Jiang, P.; Gao, Z.; Li, J.-X.; Chen, J.; Yang, Y.-J.; Gao, R.-L.; Xu, B.; Yuan, J.-Q. Effect of prior stroke on long-term outcomes of percutaneous coronary interventions in Chinese patients: A large single-center study. Catheter. Cardiovasc. Interv. 2019, 93, E75–E80. [Google Scholar] [CrossRef]
- Rochette, L.; Meloux, A.; Rigal, E.; Zeller, M.; Malka, G.; Cottin, Y.; Vergely, C. The Role of Osteoprotegerin in Vascular Calcification and Bone Metabolism: The Basis for Developing New Therapeutics. Calcif. Tissue Int. 2019, 105, 239–251. [Google Scholar] [CrossRef]
- Puymirat, E.; Cayla, G.; Cottin, Y.; Elbaz, M.; Henry, P.; Gerbaud, E.; Lemesle, G.; Popovic, B.; Labèque, J.N.; Roubille, F.; et al. Twenty-year trends in profile, management and outcomes of patients with ST-segment elevation myocardial infarction according to use of reperfusion therapy: Data from the FAST-MI program 1995–2015. Am. Heart J. 2019, 214, 97–106. [Google Scholar] [CrossRef] [PubMed]
- De Ciriza, C.P.; Lawrie, A.; Varo, N. Influence of pre-analytical and analytical factors on osteoprotegerin measurements. Clin. Biochem. 2014, 47, 1279–1285. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| SYNTAX Score | ||||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p | |
| N = 125 | N = 128 | N = 125 | ||
| SYNTAX score | 5 (3–6) | 11 (9–13) | 20 (18–23) | <0.001 |
| Min_max | 2–7 | 8–16 | 17–36 | |
| Risk factors | ||||
| Age (year) | 58 (53–71) | 64 (56–74) | 69 (58–83) | <0.001 |
| Age > 65 year | 53 (42%) | 67 (52%) | 83 (66%) | <0.001 |
| BMI (kg/m2) | 26 (24–29) | 27 (24–30) | 26 (24–30) | 0.404 |
| Women | 44 (35%) | 39 (31%) | 35 (28%) | 0.514 |
| Hypertension | 63 (50%) | 74 (58%) | 81 (65%) | 0.051 |
| Diabetes | 26 (21%) | 29 (23%) | 44 (35%) | 0.016 |
| Hypercholesterolemia | 48 (38%) | 48 (38%) | 67 (53%) | 0.013 |
| Family history of CAD | 31 (24%) | 31 (24%) | 22 (18%) | 0.333 |
| Current smoking | 55 (43%) | 32 (25%) | 31 (25%) | 0.001 |
| CV history | ||||
| Chronic coronary syndrome | 36% (28%) | 54 (42%) | 43 (34%) | 0.067 |
| Prior MI | 16 (13%) | 12 (9%) | 20 (16%) | 0.284 |
| CABG | 0 (0%) | 0 (0%) | 6 (5%) | 0.002 |
| PCI | 18 (14%) | 13 (10%) | 16 (13%) | 0.612 |
| ASCVD | 32 (25%) | 20 (16%) | 46 (37%) | 0.001 |
| Chronic renal failure | 7 (6%) | 5 (4%) | 9 (7%) | 0.518 |
| Congestive heart failure | 2 (2%) | 0 (0%) | 1 (1%) | 0.364 |
| Admission data | ||||
| Time to admission (min) | 148 (93–440) | 153 (89–383) | 170 (80–329) | 0.729 |
| HR (b/min) | 77 (63–88) | 78 (65–90) | 78 (70–91) | 0.024 |
| SBP (mmHg) | 143 (128–168) | 147 (126–170) | 134 (114–165) | 0.209 |
| SBP (mmHg) | 89 (77–96) | 87 (74–100) | 79 (65–100) | 0.113 |
| LVEF (%) | 60 (50–60) | 58 (50–60) | 50 (45–55) | <0.001 |
| LVEF < 40% | 5 (4%) | 10 (8%) | 16 (13%) | 0.029 |
| STEMI | 64 (50%) | 73 (57%) | 70 (56%) | 0.520 |
| Anterior wall location | 11 (9%) | 23 (18%) | 40 (32%) | <0.001 |
| GRACE risk score | 128 (105–155) | 140 (112–161) | 150 (133–178) | 0.028 |
| Revascularization | ||||
| PCI | 88 (70%) | 123 (96%) | 88 (70%) | <0.001 |
| CABG | 0 (0%) | 1 (1%) | 29 (23%) | <0.001 |
| In-hospiral events | ||||
| CV death | 2 (2%) | 1 (1%) | 9 (7%) | 0.006 |
| Heart failure | 5 (4%) | 7 (6%) | 15 (12%) | 0.030 |
| Recurrent MI | 1 (1%) | 1 (1%) | 3 (2%) | 0.430 |
| SYNTAX Score | ||||
|---|---|---|---|---|
| Tertile 1 | Tertile 2 | Tertile 3 | p-Value | |
| N = 125 | N = 128 | N = 125 | ||
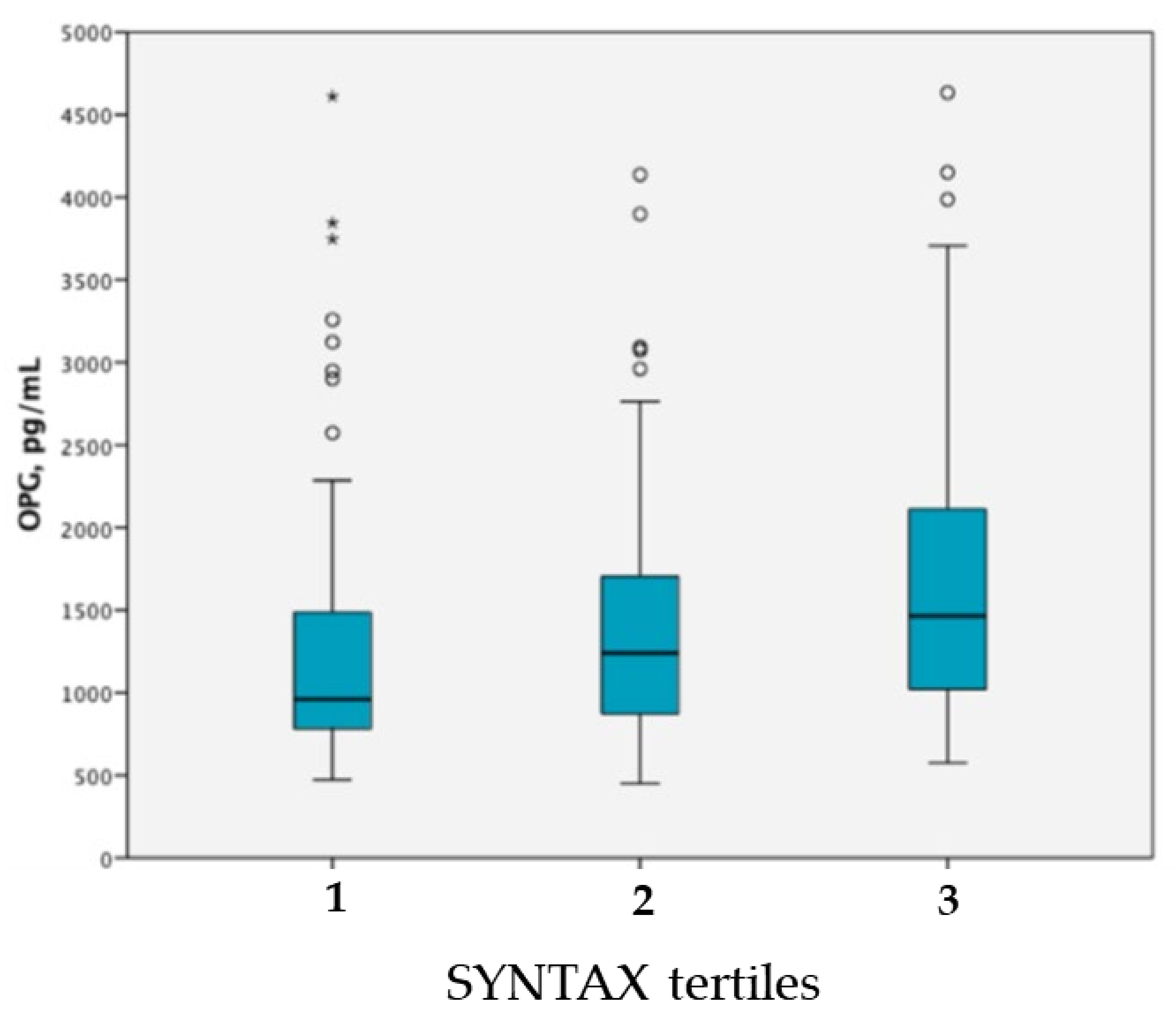
| OPG, pg/mL | 962 (782–1497) | 1240 (870–1707) | 1464 (1011–2129) | <0.001 |
| OPG >1080 pg/mL | 46 (23%) | 70 (35%) | 82 (41%) | <0.001 |
| Creatinine (μmol/L) | 75 (61–92) | 77 (68–91) | 82 (69–97) | 0.002 |
| GFR(mL/min/1.73 m2) | 93 (77–101) | 85 (71–97) | 78 (59–95) | <0.001 |
| Total cholesterol (mmol/L) | 5.11 (4.59–6.08) | 5.42 (4.51–6.21) | 5.06 (3.89–5.99) | 0.094 |
| HDL cholesterol (mmol/L) | 1.23 (1.04–1.58) | 1.32 (1.03–1.55) | 1.27 (1.00–1.50) | 0.577 |
| LDL cholesterol (mmol/L) | 3.20 (2.38–3.82) | 3.29 (2.50–4.11) | 3.05 (2.07–3.88) | 0.151 |
| Triglycerides (mmol/L) | 1.34 (0.89–2.10) | 1.53 (1.02–2.16) | 1.40 (0.98–2.00) | 0.518 |
| Blood glucose (mmol/L) | 7.1 (5.9–8.8) | 6.9 (5.8–8.4) | 7.1 (6.2–9.0) | 0.016 |
| CRP (mg/L) | 4.3 (2.9–8.9) | 3.0 (2.9–9.9) | 4.1 (2.9–10.2) | 0.027 |
| Ntpro-BNP (pg/mL) | 135 (50–1015) | 183 (80–1120) | 511 (104–1829) | <0.001 |
| Troponine Ic peak (μg/L) | 30.5 (8.2–78.8) | 22.0 (4.5–93.8) | 34.5 (4.7–157.5) | 0.246 |
| OR (95% CI) | p | |
|---|---|---|
| OPG > 1080 pg/mL | 2.10 (1.29–3.49) | 0.003 |
| Hypercholesterolemia | 1.69 (1.08–2.89) | 0.019 |
| Prior CAD | 1.47 (1.11–4.56) | 0.018 |
| GFR < 60 mL/min/1.73 m2 | 1.99 (1.20–3.05) | 0.002 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cottin, Y.; Issa, R.; Benalia, M.; Mouhat, B.; Meloux, A.; Tribouillard, L.; Bichat, F.; Rochette, L.; Vergely, C.; Zeller, M. Association between Serum Osteoprotegerin Levels and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction. J. Clin. Med. 2021, 10, 4326. https://doi.org/10.3390/jcm10194326
Cottin Y, Issa R, Benalia M, Mouhat B, Meloux A, Tribouillard L, Bichat F, Rochette L, Vergely C, Zeller M. Association between Serum Osteoprotegerin Levels and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction. Journal of Clinical Medicine. 2021; 10(19):4326. https://doi.org/10.3390/jcm10194326
Chicago/Turabian StyleCottin, Yves, Rany Issa, Mourad Benalia, Basile Mouhat, Alexandre Meloux, Laura Tribouillard, Florence Bichat, Luc Rochette, Catherine Vergely, and Marianne Zeller. 2021. "Association between Serum Osteoprotegerin Levels and Severity of Coronary Artery Disease in Patients with Acute Myocardial Infarction" Journal of Clinical Medicine 10, no. 19: 4326. https://doi.org/10.3390/jcm10194326