
Results of Simultaneous Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction: A Systematic Review


 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Eligibility Criteria
2.2. Search Methods for Identification of Studies
2.3. Data Collection Process
2.4. Methodological Quality Assessment
3. Results
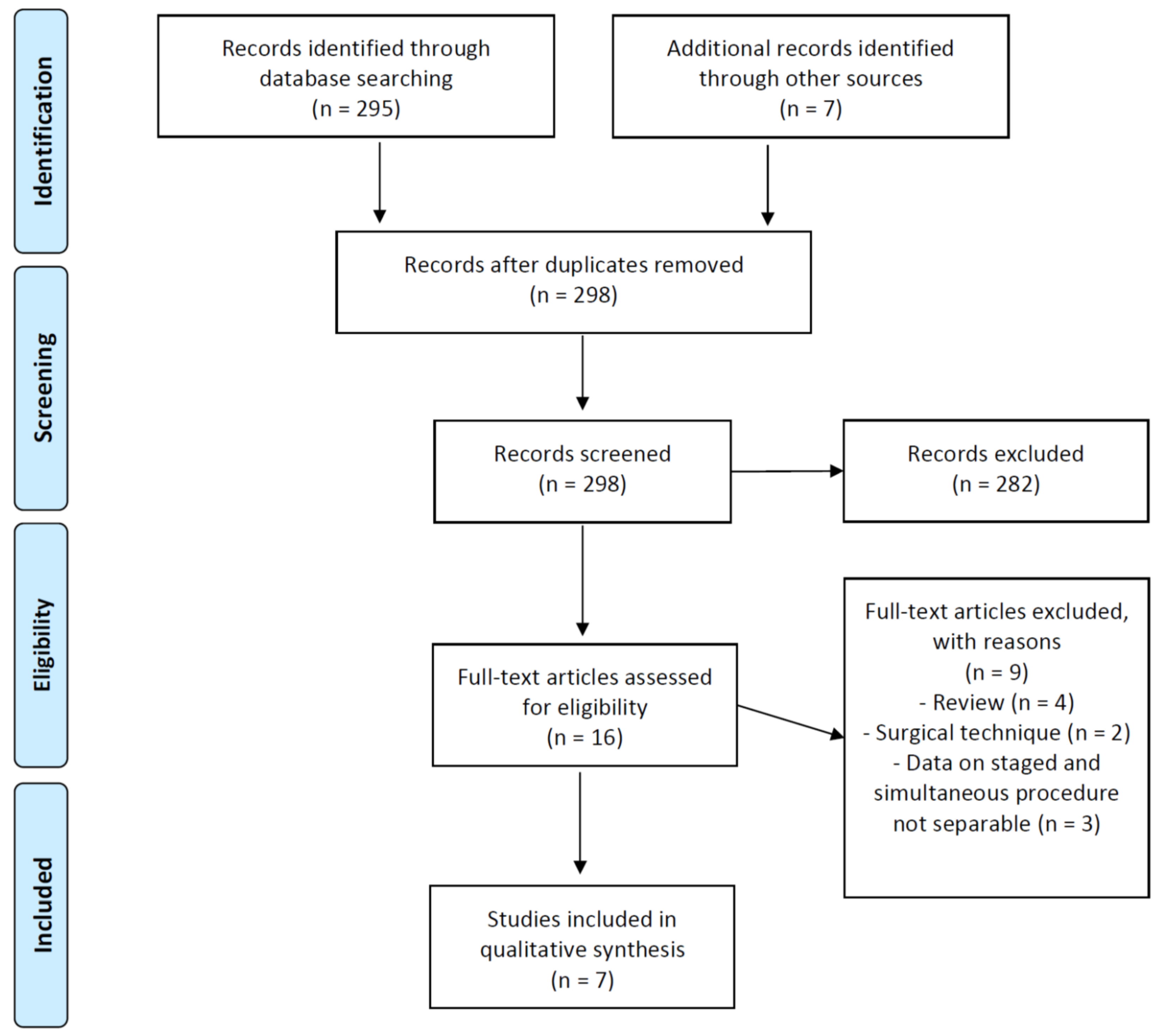
3.1. Search Results
3.2. Study Characteristics and Demographic Details
3.3. Preoperative Assessment
3.3.1. Surgical Indications and Preoperative Symptoms
3.3.2. Clinical and Radiological Examination
3.4. Surgical Technique
3.5. Rehabilitation Protocols
3.6. Clinical and Radiological Outcomes
Detailed Outcomes
3.7. Complications
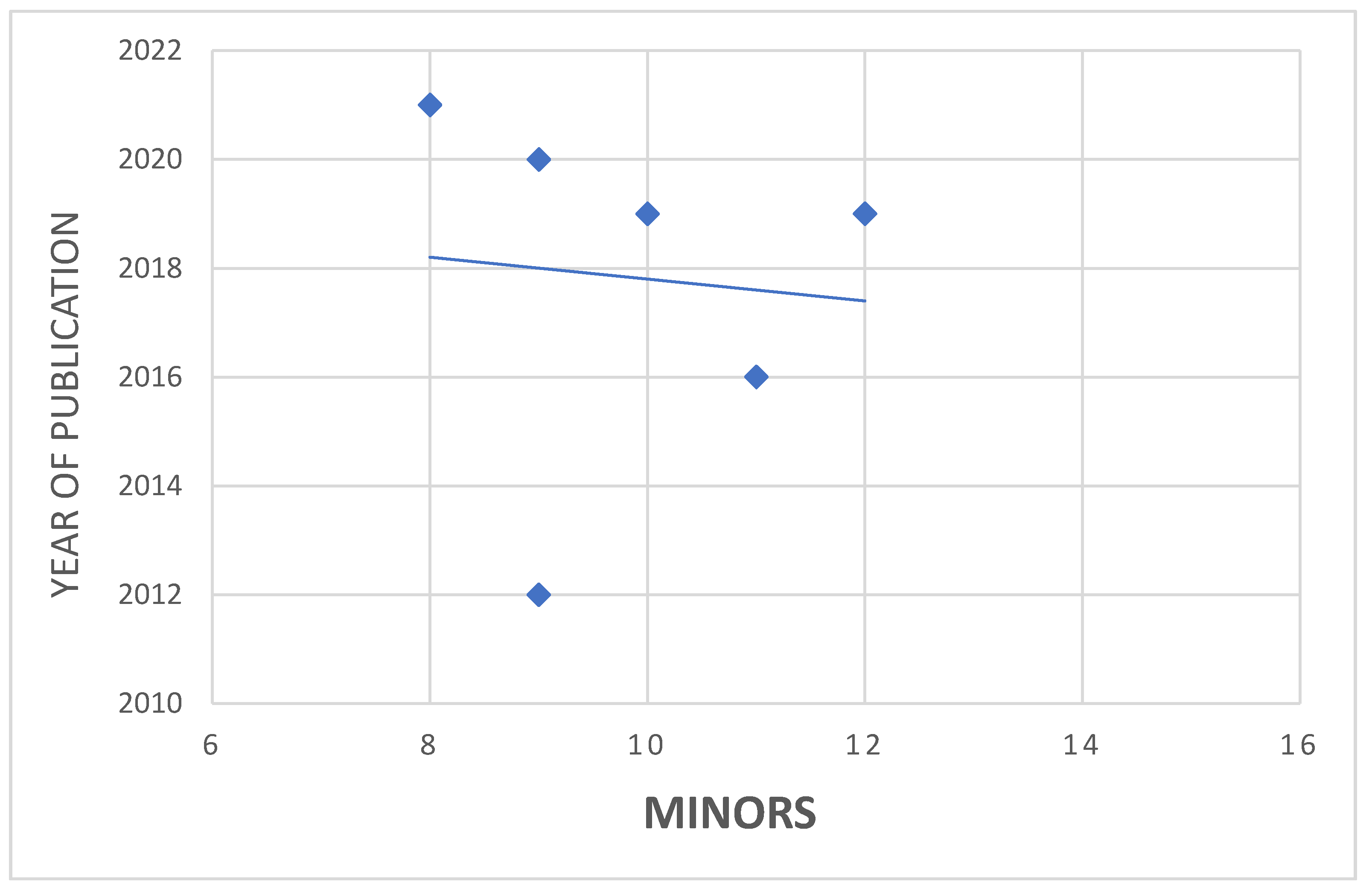
3.8. Methodological Evaluation
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Felson, D.T.; Naimark, A.; Anderson, J.; Kazis, L.; Castelli, W.; Meenan, R.F. The Prevalence of Knee Osteoarthritis in the Elderly. The Framingham Osteoarthritis Study. Arthritis Rheum. 1987, 30, 914–918. [Google Scholar] [CrossRef]
- Gillquist, J.; Messner, K. Anterior Cruciate Ligament Reconstruction and the Long-Term Incidence of Gonarthrosis. Sports Med. 1999, 27, 143–156. [Google Scholar] [CrossRef]
- McDaniel, W.J.; Dameron, T.B. The Untreated Anterior Cruciate Ligament Rupture. Clin. Orthop. Relat. Res. 1983, 172, 158–163. [Google Scholar] [CrossRef]
- Dejour, H.; Neyret, P.; Boileau, P.; Donell, S.T. Anterior Cruciate Reconstruction Combined with Valgus Tibial Osteotomy. Clin. Orthop. Relat. Res. 1994, 299, 220–228. [Google Scholar] [CrossRef]
- Demey, G.; Magnussen, R.A.; Lustig, S.; Servien, E.; Neyret, P. Total Knee Arthroplasty for Advanced Osteoarthritis in the Anterior Cruciate Ligament Deficient Knee. Int. Orthop. 2012, 36, 559–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Strickland, L.H.; Rahman, A.; Jenkinson, C.; Pandit, H.G.; Murray, D.W. Early Recovery Following Total and Unicompartmental Knee Arthroplasty Assessed Using Novel Patient-Reported Measures. J. Arthroplasty 2021. [Google Scholar] [CrossRef]
- Mancuso, F.; Hamilton, T.W.; Kumar, V.; Murray, D.W.; Pandit, H. Clinical Outcome after UKA and HTO in ACL Deficiency: A Systematic Review. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 112–122. [Google Scholar] [CrossRef] [PubMed]
- Ghomrawi, H.M.; Eggman, A.A.; Pearle, A.D. Effect of Age on Cost-Effectiveness of Unicompartmental Knee Arthroplasty Compared with Total Knee Arthroplasty in the U.S. J. Bone Joint Surg. Am. 2015, 97, 396–402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, G.; Papannagari, R.; DeFrate, L.E.; Yoo, J.D.; Park, S.E.; Gill, T.J. The Effects of ACL Deficiency on Mediolateral Translation and Varus-Valgus Rotation. Acta Orthop. 2007, 78, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Deschamps, G.; Lapeyre, B. Rupture of the anterior cruciate ligament: A frequently unrecognized cause of failure of unicompartmental knee prostheses. Apropos of a series of 79 Lotus prostheses with a follow-up of more than 5 years. Rev. Chir. Orthop. Reparatrice l’Appareil Mot. 1987, 73, 544–551. [Google Scholar]
- Goodfellow, J.W.; Kershaw, C.J.; Benson, M.K.; O’Connor, J.J. The Oxford Knee for Unicompartmental Osteoarthritis. The First 103 Cases. J. Bone Joint Surg. Br. 1988, 70, 692–701. [Google Scholar] [CrossRef] [PubMed]
- Kozinn, S.C.; Scott, R. Unicondylar Knee Arthroplasty. J. Bone Joint Surg. Am. 1989, 71, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Zampogna, B.; Vasta, S.; Torre, G.; Gupta, A.; Hettrich, C.M.; Bollier, M.J.; Wolf, B.R.; Amendola, A. Return to Sport After Anterior Cruciate Ligament Reconstruction in a Cohort of Division I NCAA Athletes From a Single Institution. Orthop. J. Sports Med. 2021, 9, 2325967120982281. [Google Scholar] [CrossRef] [PubMed]
- Bortone, I.; Moretti, L.; Bizzoca, D.; Caringella, N.; Delmedico, M.; Piazzolla, A.; Moretti, B. The Importance of Biomechanical Assessment after Return to Play in Athletes with ACL-Reconstruction. Gait Posture 2021, 88, 240–246. [Google Scholar] [CrossRef] [PubMed]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; the PRISMA-P Group. Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols (PRISMA-P) 2015: Elaboration and Explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Slim, K.; Nini, E.; Forestier, D.; Kwiatkowski, F.; Panis, Y.; Chipponi, J. Methodological Index for Non-Randomized Studies (MINORS): Development and Validation of a New Instrument: Methodological Index for Non-Randomized Studies. ANZ J. Surg. 2003, 73, 712–716. [Google Scholar] [CrossRef]
- Kennedy, J.A.; Molloy, J.; Mohammad, H.R.; Mellon, S.J.; Dodd, C.A.F.; Murray, D.W. Mid- to Long-Term Function and Implant Survival of ACL Reconstruction and Medial Oxford UKR. Knee 2019, 26, 897–904. [Google Scholar] [CrossRef]
- Tian, S.; Wang, B.; Wang, Y.; Ha, C.; Liu, L.; Sun, K. Combined Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction in Knees with Osteoarthritis and Deficient Anterior Cruciate Ligament. BMC Musculoskelet Disord. 2016, 17, 327. [Google Scholar] [CrossRef] [Green Version]
- Tinius, M.; Hepp, P.; Becker, R. Combined Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 2012, 20, 81–87. [Google Scholar] [CrossRef] [PubMed]
- Iriberri, I.; Suau, S.; Payán, L.; Aragón, J.F. Long-Term Deterioration after One-Stage Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction. Musculoskelet. Surg. 2019, 103, 251–256. [Google Scholar] [CrossRef]
- Ventura, A.; Legnani, C.; Terzaghi, C.; Macchi, V.; Borgo, E. Unicompartmental Knee Replacement Combined to Anterior Cruciate Ligament Reconstruction: Midterm Results. J. Knee Surg. 2020, 33, 1152–1156. [Google Scholar] [CrossRef]
- Aslan, H.; Çevik, H.B. Outcomes of Combined Unicondylar Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction. J. Knee Surg. 2021, s-0040-1722322. [Google Scholar] [CrossRef]
- Tecame, A.; Savica, R.; Rosa, M.A.; Adravanti, P. Anterior Cruciate Ligament Reconstruction in Association with Medial Unicompartmental Knee Replacement: A Retrospective Study Comparing Clinical and Radiological Outcomes of Two Different Implant Design. Int. Orthop. (SICOT) 2019, 43, 2731–2737. [Google Scholar] [CrossRef] [PubMed]
- Jin, Q.H.; Lee, W.-G.; Song, E.-K.; Jin, C.; Seon, J.-K. Comparison of Long-Term Survival Analysis Between Open-Wedge High Tibial Osteotomy and Unicompartmental Knee Arthroplasty. J. Arthroplasty 2021, 36, 1562–1567.e1. [Google Scholar] [CrossRef] [PubMed]
- Weston-Simons, J.S.; Pandit, H.; Jenkins, C.; Jackson, W.F.M.; Price, A.J.; Gill, H.S.; Dodd, C.A.F.; Murray, D.W. Outcome of Combined Unicompartmental Knee Replacement and Combined or Sequential Anterior Cruciate Ligament Reconstruction: A Study of 52 Cases with Mean Follow-up of Five Years. J. Bone Joint Surg. Br. 2012, 94, 1216–1220. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pandit, H.; Beard, D.J.; Jenkins, C.; Kimstra, Y.; Thomas, N.P.; Dodd, C.A.F.; Murray, D.W. Combined Anterior Cruciate Reconstruction and Oxford Unicompartmental Knee Arthroplasty. J. Bone Joint Surg. Br. 2006, 88, 887–892. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Authors | Year | Type of Study | LOE | Participants | M/F | Study Timelapse | Mean Age (Years ± SD) | Mean FollowUp (Years) | MINORS Score |
|---|---|---|---|---|---|---|---|---|---|
| Tinius et al. [19] | 2012 | RCS | IV | 27 | 16/11 | 2003–2009 | 44 ± 3.7 (range 38–53) | 4.2 ± 1.0 (range 0.75–5.9) | 9/16 |
| Tian et al. [18] | 2016 | PCS | IV | 28 | 18/10 | 2008–2014 | 50.5 ± 3.5 (range 41–61) | 4.3 ± 0.7 (range 1–8) | 11/16 |
| Iriberri et al. [20] | 2019 | RCS | IV | 8 | 5/3 | 1994–2004 | 52 (range 42–60) | 14.6 (range 9.8 –21.5) | 10/16 |
| Tecame et al. [23] | 2019 | RCS | III | 24 Group 1: 9 Group 2: 15 | 20/4 | 2007–2013 | Group 1: 47.8 (range 41–53) Group 2: 48.4 (range 43–54) | Group 1: 4.4 ± 0.7 Group 2: 3.5 ± 0.6 | 14/24 |
| Kennedy et al. [17] | 2019 | PCS | IV | 58 | 44/14 | 2001–2016 | 53.8 (range 41–71) | 5.5 (range 1–12) | 12/16 |
| Ventura et al. [21] | 2020 | RCS | IV | 12 | 8/4 | 2006–2010 | 54 ± 3.9 | 7.8 (range: 6–10) | 9/16 |
| Aslan et al. [22] | 2021 | RCS | IV | 12 | NA | 2011–2014 | NA | 3.8 ± 0.4 (range 3.3–4.3) | 8/16 |
| Authors | Patients | OA Classification (n. of Patients) | Bearing and Fixation | Tendon Graft | Outcome | Preoperative (Mean) | Postoperative (Mean) |
|---|---|---|---|---|---|---|---|
| Tinius et al. [19] | 27 | Ahlbäck Type 4 (27) | Fixed-Bearing Cemented (27) | Four-Stranded Hamstring | KSS-KS | 38.4 ± 10 | 83.2 ± 6.8 |
| KSS-FS | 38.7 ± 8.8 | 82.7 ± 8.2 | |||||
| KSS | 77 ± 11.6 | 166 ± 12.1 | |||||
| Tian et al. [18] | 28 | NA | Mobile-Bearing Cemented (12) | Four-Stranded Hamstring | OKS | 31 ± 7.1 | 43 ± 4.2 |
| KSS-KS | 60.4 ± 7.1 | 84.5 ± 6.3 | |||||
| KSS-FS | 63.7 ± 6.5 | 86.9 ± 5.3 | |||||
| TAS | 4.4 ± 1.2 | 5.3 ± 0.8 | |||||
| Iriberri et al. [20] | 8 | Ahlbäck Type 2 (6) and Type 3 (2) | Fixed-Bearing Cemented (8) | Four-Stranded Hamstring | KSS | 94 (62–165) | 154 (102–200) |
| WOMAC | 59 (3–81) | 26 (1–52) | |||||
| Tecame et al. [23] | 24 Group 1: 9 Group 2: 15 | Kellgler–Lawrence grade 4 | Mobile-Bearing (9) Fixed-Bearing (15) Cemented (24) | Four-Stranded Hamstring | KSS-KS | G1: 37.3 ± 4.3 G2: 38.6 ± 3.8 | G1: 73.4 ± 9.3 G2: 77.3 ± 10.5 |
| KSS-FS | G1: 71.2 ± 7.4 G2: 70.2 ± 6.4 | G1: 86.2 ± 6.2 G2: 84.7 ± 5.9 | |||||
| WOMAC | G1: 55.78 ± 7.6 G2: 59 ± 8.1 | G1: 79.3 ± 7.3 G2: 81.3 ± 7.6 | |||||
| Kennedy et al. [17] | 58 | NA | Mobile-Bearing Cementless (NA), cemented (NA) | Hamstring | OKS | 29.1 ± 8 | 45 (41 to 47) |
| TAS | 2.9 ± 1 | 3.6 ± 2 | |||||
| Ventura et al. [21] | 12 | Ahlbäck Type 2–4 (NA) | Fixed-Bearing Cemented | Four-Stranded Hamstring | OKS | 28.8 ± 10.1 | 42.4 ± 8.9 |
| KSS-KS | 45 ± 12.9 | 75 ± 13.5 | |||||
| KSS-FS | 80 ± 14.2 | 88 ± 16.2 | |||||
| KOOS | 62.4 ± 8.1 | 80.2 ± 11.7 | |||||
| WOMAC | 71.9 ± 11.5 | 84.9 ± 9.3 | |||||
| Aslan et al. [22] | 12 | Ahlbäck Type 4 (12) | Mobile-Bearing Cementless (5), hybrid (3), cemented (4) | Four-Stranded Hamstring | OKS | 29 ± 6.1 | 45.2 ± 3.7 |
| KOOS | 68.5 ± na | 86.3 ± na |
| Authors | Rehabilitation Protocols |
|---|---|
| Tinius et al. | NA |
| Tian et al. |
|
| Iriberri et al. | NA |
| Tecame et al. |
|
| Kennedy et al. [3] | NA |
| Ventura et al. |
|
| Aslan et al. | NA |
| ROM: range of motion | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Albo, E.; Campi, S.; Zampogna, B.; Torre, G.; Papalia, G.F.; Diaz Balzani, L.A.; Alifano, A.M.; Papalia, R.; Denaro, V. Results of Simultaneous Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction: A Systematic Review. J. Clin. Med. 2021, 10, 4290. https://doi.org/10.3390/jcm10194290
Albo E, Campi S, Zampogna B, Torre G, Papalia GF, Diaz Balzani LA, Alifano AM, Papalia R, Denaro V. Results of Simultaneous Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction: A Systematic Review. Journal of Clinical Medicine. 2021; 10(19):4290. https://doi.org/10.3390/jcm10194290
Chicago/Turabian StyleAlbo, Erika, Stefano Campi, Biagio Zampogna, Guglielmo Torre, Giuseppe Francesco Papalia, Lorenzo Alirio Diaz Balzani, Anna Maria Alifano, Rocco Papalia, and Vincenzo Denaro. 2021. "Results of Simultaneous Unicompartmental Knee Arthroplasty and Anterior Cruciate Ligament Reconstruction: A Systematic Review" Journal of Clinical Medicine 10, no. 19: 4290. https://doi.org/10.3390/jcm10194290