
Elevated Plasma Soluble PD-L1 Levels in Out-of-Hospital Cardiac Arrest Patients

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Patient Characteristics
2.2. Soluble PD-L1 Measurements
2.3. Statistical Analyses
3. Results
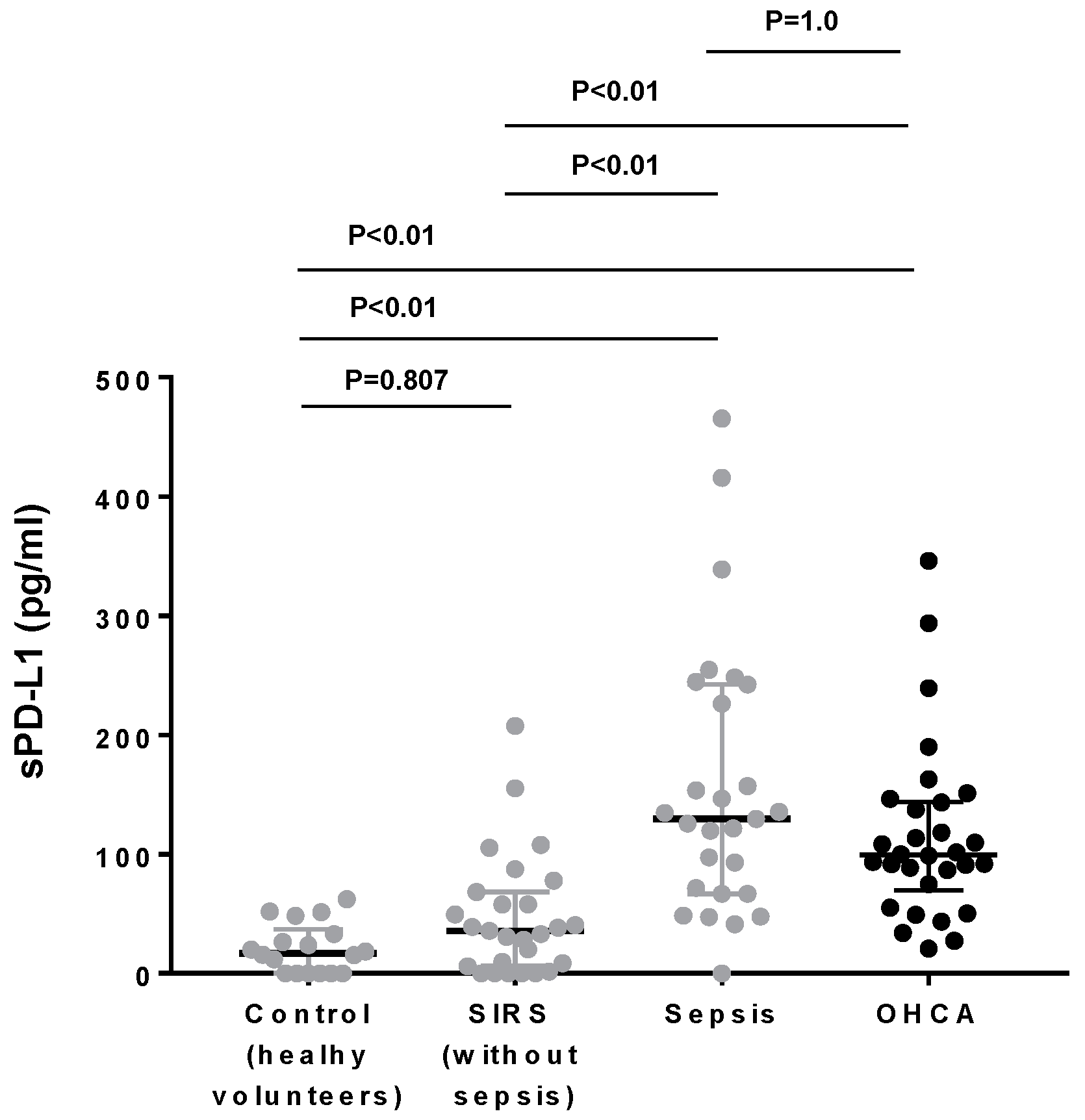
3.1. Plasma PD-L1 Levels in OHCA Patients Were as High as Those in Sepsis Patients
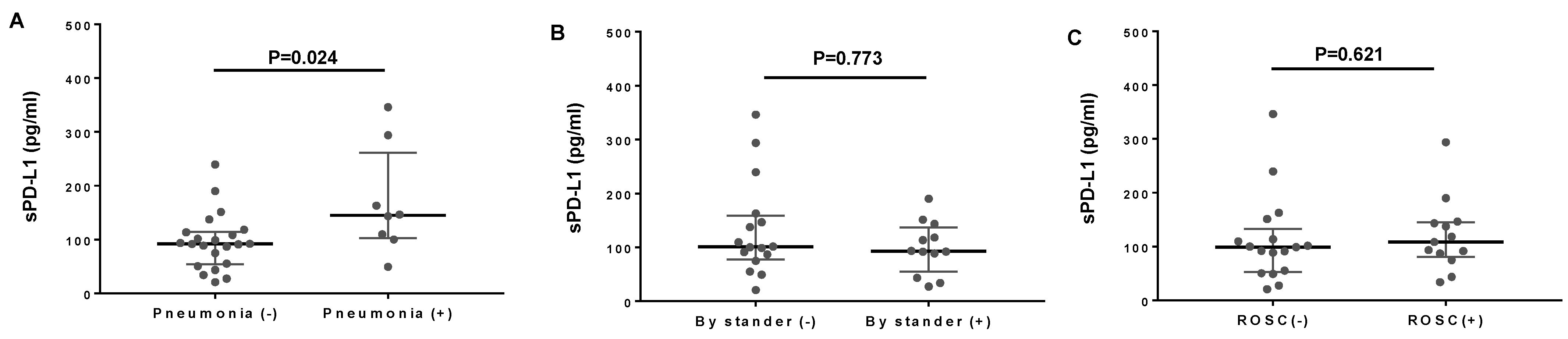
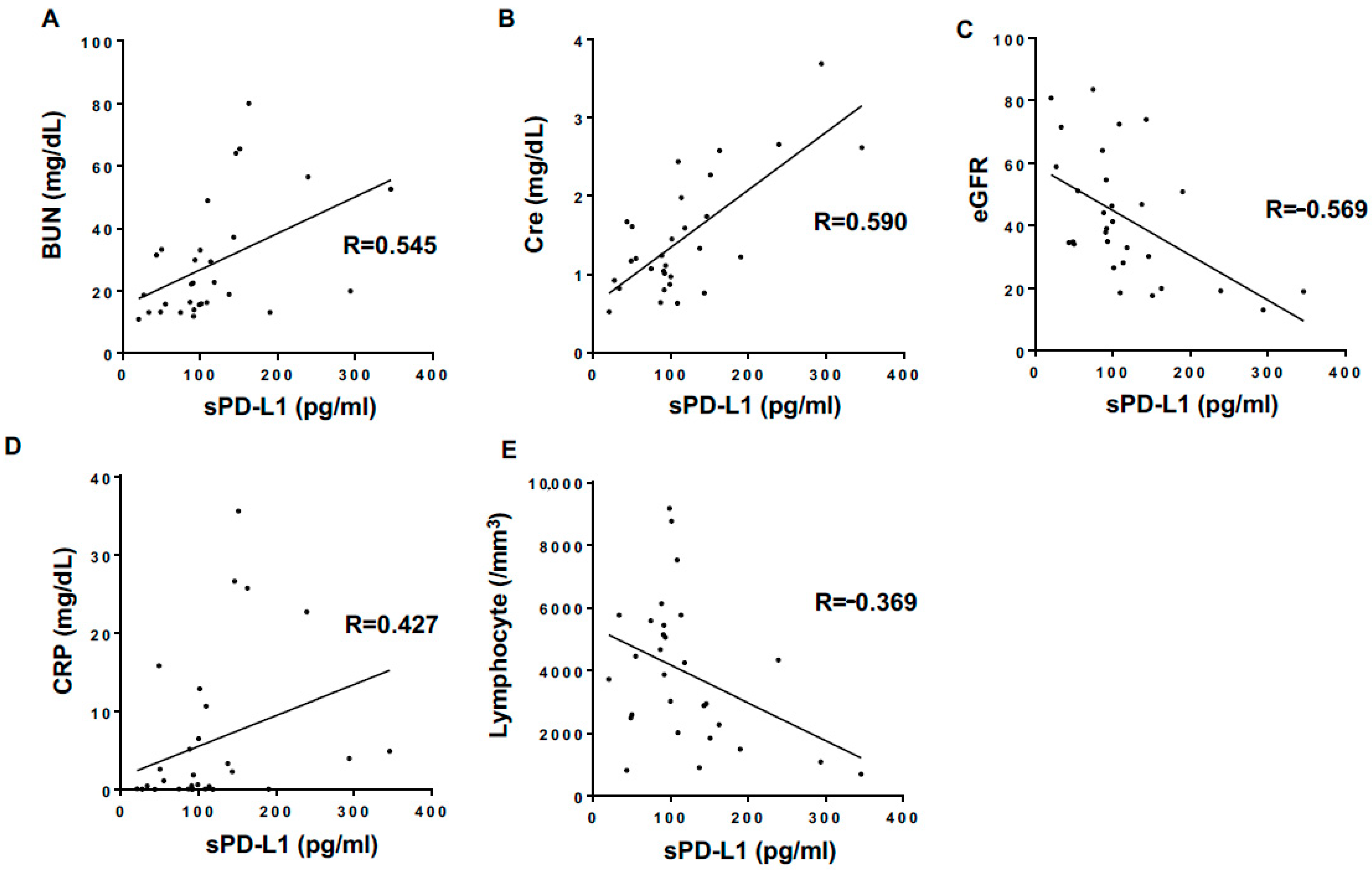
3.2. Correlations of Plasma sPD-L1 Levels with Clinical Parameters in OHCA Patients
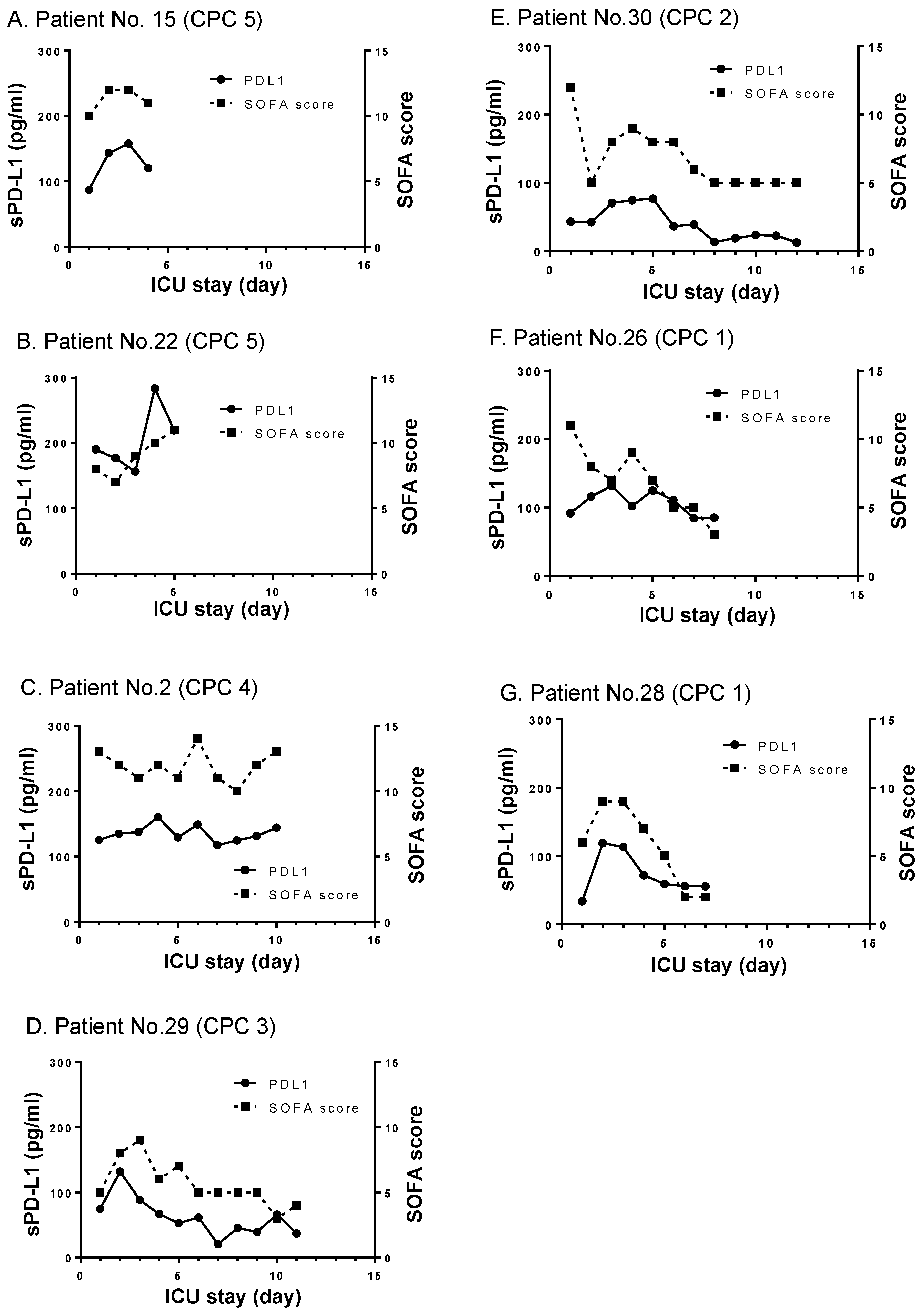
3.3. Longitudinal Changes of sPD-L1 Levels in ROSC Cases
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Binks, A.; Nolan, J.P. Post-cardiac arrest syndrome. Minerva Anestesiol. 2010, 76, 362–368. [Google Scholar]
- Nolan, J.P.; Neumar, R.W.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A Scientific Statement from the International Liaison Committee on Resuscitation; the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; the Council on Stroke. Resuscitation 2008, 79, 350–379. [Google Scholar] [CrossRef]
- Topjian, A.A.; De Caen, A.; Wainwright, M.S.; Abella, B.S.; Abend, N.S.; Atkins, D.L.; Bembea, M.M.; Fink, E.L.; Guerguerian, A.M.; Haskell, S.E.; et al. Pediatric post-cardiac arrest care: A scientific statement from the American Heart Association. Circulation 2019, 140, e194–e233. [Google Scholar] [CrossRef]
- Neumar, R.W.; Nolan, J.P.; Adrie, C.; Aibiki, M.; Berg, R.A.; Böttiger, B.W.; Callaway, C.; Clark, R.S.; Geocadin, R.G.; Jauch, E.C.; et al. Post-cardiac arrest syndrome: Epidemiology, pathophysiology, treatment, and prognostication. A consensus statement from the International Liaison Committee on Resuscitation (American Heart Association, Australian and New Zealand Council on Resuscitation, European Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Council of Asia, and the Resuscitation Council of Southern Africa); the American Heart Association Emergency Cardiovascular Care Committee; the Council on Cardiovascular Surgery and Anesthesia; the Council on Cardiopulmonary, Perioperative, and Critical Care; the Council on Clinical Cardiology; and the Stroke Council. Circulation 2008, 118, 2452–2483. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adrie, C.; Adib-Conquy, M.; Laurent, I.; Monchi, M.; Vinsonneau, C.; Fitting, C.; Fraisse, F.; Dinh-Xuan, A.T.; Carli, P.; Spaulding, C.; et al. Successful cardiopulmonary resuscitation after cardiac arrest as a “sepsis-like” syndrome. Circulation 2002, 106, 562–568. [Google Scholar] [CrossRef] [PubMed]
- Hellenkamp, K.; Onimischewski, S.; Kruppa, J.; Faßhauer, M.; Becker, A.; Eiffert, H.; Hünlich, M.; Hasenfuß, G.; Wachter, R. Early pneumonia and timing of antibiotic therapy in patients after nontraumatic out-of-hospital cardiac arrest. Crit. Care 2016, 20, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Timmermans, K.; Kox, M.; Gerretsen, J.; Peters, E.; Scheffer, G.J.; Van der Hoeven, J.G.; Pickkers, P.; Hoedemaekers, C.W. The involvement of danger-associated molecular patterns in the development of immunoparalysis in cardiac arrest patients. Crit. Care Med. 2015, 43, 2332–2338. [Google Scholar] [CrossRef]
- Qi, Z.; An, L.; Liu, B.; Zhang, Q.; Yin, W.; Yu, H.; Li, C. Patients with out-of-hospital cardiac arrest show decreased human leucocyte antigen-DR expression on monocytes and B and T lymphocytes after return of spontaneous circulation. Scand. J. Immunol. 2018, 88, e12707. [Google Scholar] [CrossRef]
- Keir, M.E.; Butte, M.J.; Freeman, G.J.; Sharpe, A.H. PD-1 and its ligands in tolerance and immunity. Annu. Rev. Immunol. 2008, 26, 677–704. [Google Scholar] [CrossRef] [Green Version]
- Pauken, K.E.; Wherry, E.J. Overcoming T cell exhaustion in infection and cancer. Trends Immunol. 2015, 36, 265–276. [Google Scholar] [CrossRef] [Green Version]
- Chen, D.S.; Mellman, I. Elements of cancer immunity and the cancer-immune set point. Nature 2017, 541, 321–330. [Google Scholar] [CrossRef]
- Nakamori, Y.; Park, E.J.; Shimaoka, M. Immune deregulation in sepsis and septic shock: Reversing immune paralysis by targeting PD-1/PD-L1 pathway. Front. Immunol. 2020, 11, 624279. [Google Scholar] [CrossRef]
- Hotchkiss, R.S.; Monneret, G.; Payen, D. Sepsis-induced immunosuppression: From cellular dysfunctions to immunotherapy. Nat. Rev. Immunol. 2013, 13, 862–874. [Google Scholar] [CrossRef]
- Jalali, S.; Price-Troska, T.; Bothun, C.; Villasboas, J.; Kim, H.J.; Yang, Z.Z.; Novak, A.J.; Dong, H.; Ansell, S.M. Reverse signaling via PD-L1 supports malignant cell growth and survival in classical Hodgkin lymphoma. Blood Cancer J. 2019, 9, 22. [Google Scholar] [CrossRef] [PubMed]
- Zhu, X.; Lang, J. Soluble PD-1 and PD-L1: Predictive and prognostic significance in cancer. Oncotarget 2017, 8, 97671–97682. [Google Scholar] [CrossRef] [Green Version]
- Xu, J.; Wang, J.; Wang, X.; Tan, R.; Qi, X.; Liu, Z.; Qu, H.; Pan, T.; Zhan, Q.; Zuo, Y.; et al. Soluble PD-L1 improved direct ARDS by reducing monocyte-derived macrophages. Cell Death Dis. 2020, 11, 934. [Google Scholar] [CrossRef]
- Shi, B.; Du, X.; Wang, Q.; Chen, Y.; Zhang, X. Increased PD-1 on CD4(+)CD28(−) T cell and soluble PD-1 ligand-1 in patients with T2DM: Association with atherosclerotic macrovascular diseases. Metabolism 2013, 62, 778–785. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Sun, C.; Li, J.; Hu, L.; Li, M.; Liu, J.; Pu, L.; Xiong, S. The prognostic significance of soluble programmed death ligand 1 expression in cancers: A systematic review and meta-analysis. Scand. J. Immunol. 2017, 86, 361–367. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kawamoto, E.; Masui-Ito, A.; Eguchi, A.; Soe, Z.Y.; Prajuabjinda, O.; Darkwah, S.; Park, E.J.; Imai, H.; Shimaoka, M. Integrin and PD-1 ligand expression on circulating extracellular vesicles in systemic inflammatory response syndrome and sepsis. Shock 2019, 52, 13–22. [Google Scholar] [CrossRef]
- Yuana, Y.; Bertina, R.M.; Osanto, S. Pre-analytical and analytical issues in the analysis of blood microparticles. Thromb. Haemost. 2011, 105, 396–408. [Google Scholar] [CrossRef]
- Mentzelopoulos, S.D.; Zakynthinos, S.G. Post-cardiac arrest syndrome: Pathological processes, biomarkers and vasopressor support, and potential therapeutic targets. Resuscitation 2017, 121, A12–A14. [Google Scholar] [CrossRef]
- Edgren, E.; Hedstrand, U.; Kelsey, S.; Sutton-Tyrrell, K.; Safar, P. Assessment of neurological prognosis in comatose survivors of cardiac arrest. BRCT I Study Group. Lancet 1994, 343, 1055–1059. [Google Scholar] [CrossRef]
- Yu, X.; Pan, Y.; Fei, Q.; Lin, X.; Chen, Z.; Huang, H. Serum soluble PD-1 plays a role in predicting infection complications in patients with acute pancreatitis. Immun. Inflamm. Dis. 2021, 9, 310–318. [Google Scholar] [CrossRef] [PubMed]
- Wu, X.; Xu, L.; Cheng, Q.; Nie, L.; Zhang, S.; Du, Y.; Xue, J. Increased serum soluble programmed death ligand 1(sPD-L1) is associated with the presence of interstitial lung disease in rheumatoid arthritis: A monocentric cross-sectional study. Respir. Med. 2020, 166, 105948. [Google Scholar] [CrossRef] [PubMed]
- Du, Y.; Nie, L.; Xu, L.; Wu, X.; Zhang, S.; Xue, J. Serum levels of soluble programmed death-1 (sPD-1) and soluble programmed death ligand 1(sPD-L1) in systemic lupus erythematosus: Association with activity and severity. Scand. J. Immunol. 2020, 92, e12884. [Google Scholar] [CrossRef]
- Grabie, N.; Gotsman, I.; DaCosta, R.; Pang, H.; Stavrakis, G.; Butte, M.J.; Keir, M.E.; Freeman, G.J.; Sharpe, A.H.; Lichtman, A.H. Endothelial programmed death-1 ligand 1 (PD-L1) regulates CD8+ T-cell mediated injury in the heart. Circulation 2007, 116, 2062–2071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grundmann, S.; Fink, K.; Rabadzhieva, L.; Bourgeois, N.; Schwab, T.; Moser, M.; Bode, C.; Busch, H.J. Perturbation of the endothelial glycocalyx in post cardiac arrest syndrome. Resuscitation 2012, 83, 715–720. [Google Scholar] [CrossRef]
- Bro-Jeppesen, J.; Johansson, P.I.; Kjaergaard, J.; Wanscher, M.; Ostrowski, S.R.; Bjerre, M.; Hassager, C. Level of systemic inflammation and endothelial injury is associated with cardiovascular dysfunction and vasopressor support in post-cardiac arrest patients. Resuscitation 2017, 121, 179–186. [Google Scholar] [CrossRef]
- Bro-Jeppesen, J.; Johansson, P.I.; Hassager, C.; Wanscher, M.; Ostrowski, S.R.; Bjerre, M.; Kjaergaard, J. Endothelial activation/injury and associations with severity of post-cardiac arrest syndrome and mortality after out-of-hospital cardiac arrest. Resuscitation 2016, 107, 71–79. [Google Scholar] [CrossRef]
- Pohl, J.; Rammos, C.; Totzeck, M.; Stock, P.; Kelm, M.; Rassaf, T.; Luedike, P. MIF reflects tissue damage rather than inflammation in post-cardiac arrest syndrome in a real life cohort. Resuscitation 2016, 100, 32–37. [Google Scholar] [CrossRef] [PubMed]
- Sauneuf, B.; Bouffard, C.; Cornet, E.; Daubin, C.; Desmeulles, I.; Masson, R.; Seguin, A.; Valette, X.; Terzi, N.; Parienti, J.J.; et al. Immature/total granulocyte ratio: A promising tool to assess the severity and the outcome of post-cardiac arrest syndrome. Resuscitation 2014, 85, 1115–1119. [Google Scholar] [CrossRef] [PubMed]
- Dezutter-Dambuyant, C.; Durand, I.; Alberti, L.; Bendriss-Vermare, N.; Valladeau-Guilemond, J.; Duc, A.; Magron, A.; Morel, A.P.; Sisirak, V.; Rodriguez, C.; et al. A novel regulation of PD-1 ligands on mesenchymal stromal cells through MMP-mediated proteolytic cleavage. Oncoimmunology 2016, 5, e1091146. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hira-Miyazawa, M.; Nakamura, H.; Hirai, M.; Kobayashi, Y.; Kitahara, H.; Bou-Gharios, G.; Kawashiri, S. Regulation of programmed-death ligand in the human head and neck squamous cell carcinoma microenvironment is mediated through matrix metalloproteinase-mediated proteolytic cleavage. Int. J. Oncol. 2018, 52, 379–388. [Google Scholar] [CrossRef]
- Romero, Y.; Wise, R.; Zolkiewska, A. Proteolytic processing of PD-L1 by ADAM proteases in breast cancer cells. Cancer Immunol. Immunother. 2020, 69, 43–55. [Google Scholar] [CrossRef] [PubMed]
- Orme, J.J.; Jazieh, K.A.; Xie, T.; Harrington, S.; Liu, X.; Ball, M.; Madden, B.; Charlesworth, M.C.; Azam, T.U.; Lucien, F.; et al. ADAM10 and ADAM17 cleave PD-L1 to mediate PD-(L)1 inhibitor resistance. Oncoimmunology 2020, 9, 1744980. [Google Scholar] [CrossRef] [Green Version]
- Lindsey, M.; Wedin, K.; Brown, M.D.; Keller, C.; Evans, A.J.; Smolen, J.; Burns, A.R.; Rossen, R.D.; Michael, L.; Entman, M. Matrix-dependent mechanism of neutrophil-mediated release and activation of matrix metalloproteinase 9 in myocardial ischemia/reperfusion. Circulation 2001, 103, 2181–2187. [Google Scholar] [CrossRef]
- Hohjoh, H.; Horikawa, I.; Nakagawa, K.; Segi-Nishida, E.; Hasegawa, H. Induced mRNA expression of matrix metalloproteinases Mmp-3, Mmp-12, and Mmp-13 in the infarct cerebral cortex of photothrombosis model mice. Neurosci. Lett. 2020, 739, 135406. [Google Scholar] [CrossRef]
- Fujii, T.; Duarte, S.; Lee, E.; Ke, B.; Busuttil, R.W.; Coito, A.J. Tissue inhibitor of metalloproteinase 3 deficiency disrupts the hepatocyte e-cadherin/β-catenin complex and induces cell death in liver ischemia/reperfusion injury. Liver Transplant. 2020, 26, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Gutsaeva, D.R.; Shalaby, L.; Powell, F.L.; Thounaojam, M.C.; Abouhish, H.; Wetzstein, S.A.; Jadeja, R.N.; Kwok, H.F.; Martin, P.M.; Bartoli, M. Inactivation of endothelial ADAM17 reduces retinal ischemia-reperfusion induced neuronal and vascular damage. Int. J. Mol. Sci. 2020, 21, 5379. [Google Scholar] [CrossRef] [PubMed]
- Deng, R.; Cassady, K.; Li, X.; Yao, S.; Zhang, M.; Racine, J.; Lin, J.; Chen, L.; Zeng, D. B7H1/CD80 interaction augments PD-1-dependent T cell apoptosis and ameliorates graft-versus-host disease. J. Immunol. 2015, 194, 560–574. [Google Scholar] [CrossRef] [Green Version]
- Shi, F.; Shi, M.; Zeng, Z.; Qi, R.Z.; Liu, Z.W.; Zhang, J.Y.; Yang, Y.P.; Tien, P.; Wang, F.S. PD-1 and PD-L1 upregulation promotes CD8(+) T-cell apoptosis and postoperative recurrence in hepatocellular carcinoma patients. Int. J. Cancer 2011, 128, 887–896. [Google Scholar] [CrossRef]
- Wilson, J.K.; Zhao, Y.; Singer, M.; Spencer, J.; Shankar-Hari, M. Lymphocyte subset expression and serum concentrations of PD-1/PD-L1 in sepsis-pilot study. Crit. Care 2018, 22, 95. [Google Scholar] [CrossRef]
- Shankar-Hari, M.; Fear, D.; Lavender, P.; Mare, T.; Beale, R.; Swanson, C.; Singer, M.; Spencer, J. Activation-associated accelerated apoptosis of memory B cells in critically ill patients with sepsis. Crit. Care Med. 2017, 45, 875–882. [Google Scholar] [CrossRef]
- Jaworska, K.; Ratajczak, J.; Huang, L.; Whalen, K.; Yang, M.; Stevens, B.K.; Kinsey, G.R. Both PD-1 ligands protect the kidney from ischemia reperfusion injury. J. Immunol. 2015, 194, 325–333. [Google Scholar] [CrossRef] [Green Version]
- Ueki, S.; Castellaneta, A.; Yoshida, O.; Ozaki, K.; Zhang, M.; Kimura, S.; Isse, K.; Ross, M.; Shao, L.; Stolz, D.B.; et al. Hepatic B7 homolog 1 expression is essential for controlling cold ischemia/reperfusion injury after mouse liver transplantation. Hepatology 2011, 54, 216–228. [Google Scholar] [CrossRef] [Green Version]
- Ren, X.; Akiyoshi, K.; Vandenbark, A.A.; Hurn, P.D.; Offner, H. Programmed death-1 pathway limits central nervous system inflammation and neurologic deficits in murine experimental stroke. Stroke 2011, 42, 2578–2583. [Google Scholar] [CrossRef] [PubMed]
- Bodhankar, S.; Chen, Y.; Vandenbark, A.A.; Murphy, S.J.; Offner, H. PD-L1 enhances CNS inflammation and infarct volume following experimental stroke in mice in opposition to PD-1. J. Neuroinflamm. 2013, 10, 111. [Google Scholar] [CrossRef] [Green Version]
- Qi, Z.; Liu, Q.; Zhang, Q.; Liu, B.; Li, C. Overexpression of programmed cell death-1 and human leucocyte antigen-DR on circulatory regulatory T cells in out-of-hospital cardiac arrest patients in the early period after return of spontaneous circulation. Resuscitation 2018, 130, 13–20. [Google Scholar] [CrossRef] [PubMed]
- Kumagai, S.; Togashi, Y.; Kamada, T.; Sugiyama, E.; Nishinakamura, H.; Takeuchi, Y.; Vitaly, K.; Itahashi, K.; Maeda, Y.; Matsui, S.; et al. The PD-1 expression balance between effector and regulatory T cells predicts the clinical efficacy of PD-1 blockade therapies. Nat. Immunol. 2020, 21, 1346–1358. [Google Scholar] [CrossRef]
- Chen, Y.; Wang, Q.; Shi, B.; Xu, P.; Hu, Z.; Bai, L.; Zhang, X. Development of a sandwich ELISA for evaluating soluble PD-L1 (CD274) in human sera of different ages as well as supernatants of PD-L1+ cell lines. Cytokine 2011, 56, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Düring, J.; Annborn, M.; Cronberg, T.; Dankiewicz, J.; Devaux, Y.; Hassager, C.; Horn, J.; Kjaergaard, J.; Kuiper, M.; Nikoukhah, H.R.; et al. Copeptin as a marker of outcome after cardiac arrest: A sub-study of the TTM trial. Crit. Care 2020, 24, 185. [Google Scholar] [CrossRef]
- Zhuang, Y.G.; Chen, Y.Z.; Zhou, S.Q.; Peng, H.; Chen, Y.Q.; Li, D.J. High plasma levels of pro-inflammatory factors interleukin-17 and interleukin-23 are associated with poor outcome of cardiac-arrest patients: A single center experience. BMC Cardiovasc. Disord. 2020, 20, 170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shin, H.; Kim, J.G.; Kim, W.; Lim, T.H.; Jang, B.H.; Cho, Y.; Choi, K.S.; Ahn, C.; Lee, J.; Na, M.K. Procalcitonin as a prognostic marker for outcomes in post-cardiac arrest patients: A systematic review and meta-analysis. Resuscitation 2019, 138, 160–167. [Google Scholar] [CrossRef]
- Weiser, C.; Schwameis, M.; Sterz, F.; Herkner, H.; Lang, I.M.; Schwarzinger, I.; Spiel, A.O. Mortality in patients resuscitated from out-of-hospital cardiac arrest based on automated blood cell count and neutrophil lymphocyte ratio at admission. Resuscitation 2017, 116, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Wada, T.; Jesmin, S.; Gando, S.; Yanagida, Y.; Mizugaki, A.; Sultana, S.N.; Zaedi, S.; Yokota, H. Angiogenic factors and their soluble receptors predict organ dysfunction and mortality in post-cardiac arrest syndrome. Crit. Care 2012, 16, R171. [Google Scholar] [CrossRef] [PubMed] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient | Cause of OHCA | Age | Gender | UMC | sPDL1 (pg/mL) | EMS 1 (mins) | Hospital 2 (mins) | Bystander CPR | Rhythms 3 | ROSC 4 | CPC Scale |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1 | AD | 87 | F | HT | 101.5 | 9 | 27 | N | |||
| 2 | Myocarditis | 48 | M | HL | 137.5 | 6 | 18 | N | + 4 | 4 | |
| 3 | Pneumonia | 80 | M | DM | 146.4 | 8 | 39 | N | + | 5 | |
| 4 | SAH | 63 | F | 108.5 | 12 | 25 | + | N | + | ||
| 5 | CHF | 70 | M | 50.3 | 11 | 27 | + | S | |||
| 6 | Pneumonia | 89 | M | 109.7 | 12 | 38 | N | ||||
| 7 | AD | 90 | F | HT | 92.1 | 9 | 15 | + | N | ||
| 8 | CHF | 82 | M | OMI | 88.6 | 12 | 30 | + | N | ||
| 9 | AMI | 92 | F | DM | 93.4 | 11 | 30 | + | N | + | 5 |
| 10 | Hanging | 87 | F | RA | 98.9 | 7 | 20 | N | |||
| 11 | AD | 90 | F | AF, TAA | 91.0 | 8 | 31 | N | |||
| 12 | AD | 62 | M | DM, CKD | 113.6 | 9 | 22 | + | N | ||
| 13 | Hyperkalemia | 65 | F | SLE, CKD, HT | 151.3 | 12 | 23 | + | N | ||
| 14 | Pneumonia | 75 | F | CI, OMI | 162.8 | 9 | 31 | N | |||
| 15 | AMI | 91 | F | DM, HT | 87.0 | 17 | 29 | N | + 4 | 5 | |
| 16 | Pneumonia | 85 | M | HT | 346.0 | 6 | 19 | N | |||
| 17 | AMI | 83 | M | HT, OMI | 118.3 | 9 | 26 | + | N | + | 5 |
| 18 | Pneumonia | 82 | M | DM | 143.3 | 5 | 20 | + | N | + | 5 |
| 19 | CHF | 78 | M | 239.3 | 7 | 29 | N | ||||
| 20 | AMI | 89 | F | 20.7 | 8 | 14 | N | ||||
| 21 | Pneumonia | 76 | F | 49.1 | 17 | 41 | N | ||||
| 22 | Hanging | 50 | M | Depression | 190.1 | 6 | 30 | + | N | + 4 | 5 |
| 23 | Pneumonia | 86 | F | 100.1 | 11 | 29 | N | ||||
| 24 | Asphyxia | 88 | M | 27.4 | 11 | 21 | + | N | |||
| 25 | Pneumonia | 86 | M | DM, HT, CKD | 293.8 | 9 | 27 | N | + | 5 | |
| 26 | AMI | 52 | M | DM, HT, AF | 91.6 | 10 | 28 | + | S | + 4 | 1 |
| 27 | AMI | 52 | M | 55.3 | 6 | 21 | N | ||||
| 28 | AMI | 69 | M | CI | 33.9 | 6 | 29 | + | S | + 4 | 1 |
| 29 | AMI | 58 | M | CHF | 74.8 | 8 | 15 | S | + 4 | 3 | |
| 30 | CHF | 58 | M | HL, OMI, AF | 43.6 | 11 | 28 | + | N | + 4 | 2 |
| 1 R Values Correlated with sPD-L1 | |
|---|---|
| Total protein | −0.147 |
| Albumin | −0.199 |
| Blood urea nitrogen | 0.545 * |
| Creatinine | 0.590 * |
| Estimated glomerular filtration rate | −0.569 * |
| Na | 0.190 |
| K | 0.172 |
| Cl | 0.141 |
| Aspartate transaminase | 0.186 |
| Alanine transaminase | 0.062 |
| Total bilirubin | 0.147 |
| C-reactive protein | 0.427 * |
| White blood cell counts | −0.236 |
| Red blood cell counts | −0.221 |
| Haemoglobin | −0.101 |
| Haematocrit | −0.123 |
| Neutrophil | −0.166 |
| Lymphocyte | −0.369 * |
| Monocyte | −0.258 |
| Platelet | 0.137 |
| Activated partial thromboplastin time | −0.102 |
| Prothrombin time | −0.015 |
| Prothrombin time (%) | 0.012 |
| Prothrombin time-international normalized ratio | −0.022 |
| Fibrinogen | 0.098 |
| D-dimer | 0.058 |
| pH | 0.049 |
| Partial pressure of arterial oxygen | 0.171 |
| Partial pressure of arterial carbon dioxide | −0.152 |
| HCO3− | 0.015 |
| Lactate | 0.156 |
| Troponin I | 0.069 |
| 2 EMS arrival time | −0.278 |
| 3 EMS-to-hospital time | 0.072 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sumiyoshi, M.; Kawamoto, E.; Nakamori, Y.; Esumi, R.; Ikejiri, K.; Shinkai, T.; Akama, Y.; Ito-Masui, A.; Imai, H.; Gaowa, A.; et al. Elevated Plasma Soluble PD-L1 Levels in Out-of-Hospital Cardiac Arrest Patients. J. Clin. Med. 2021, 10, 4188. https://doi.org/10.3390/jcm10184188
Sumiyoshi M, Kawamoto E, Nakamori Y, Esumi R, Ikejiri K, Shinkai T, Akama Y, Ito-Masui A, Imai H, Gaowa A, et al. Elevated Plasma Soluble PD-L1 Levels in Out-of-Hospital Cardiac Arrest Patients. Journal of Clinical Medicine. 2021; 10(18):4188. https://doi.org/10.3390/jcm10184188
Chicago/Turabian StyleSumiyoshi, Miho, Eiji Kawamoto, Yuki Nakamori, Ryo Esumi, Kaoru Ikejiri, Toru Shinkai, Yuichi Akama, Asami Ito-Masui, Hiroshi Imai, Arong Gaowa, and et al. 2021. "Elevated Plasma Soluble PD-L1 Levels in Out-of-Hospital Cardiac Arrest Patients" Journal of Clinical Medicine 10, no. 18: 4188. https://doi.org/10.3390/jcm10184188