
Differences in the Prevalence of Clinical Adjacent Segment Pathology among Continents after Anterior Cervical Fusion: Meta-Analysis of Randomized Controlled Trials


Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction and Outcome Measures
2.4. Statistical Analysis
3. Results
3.1. Literature Search Results
3.2. Analysis of Data
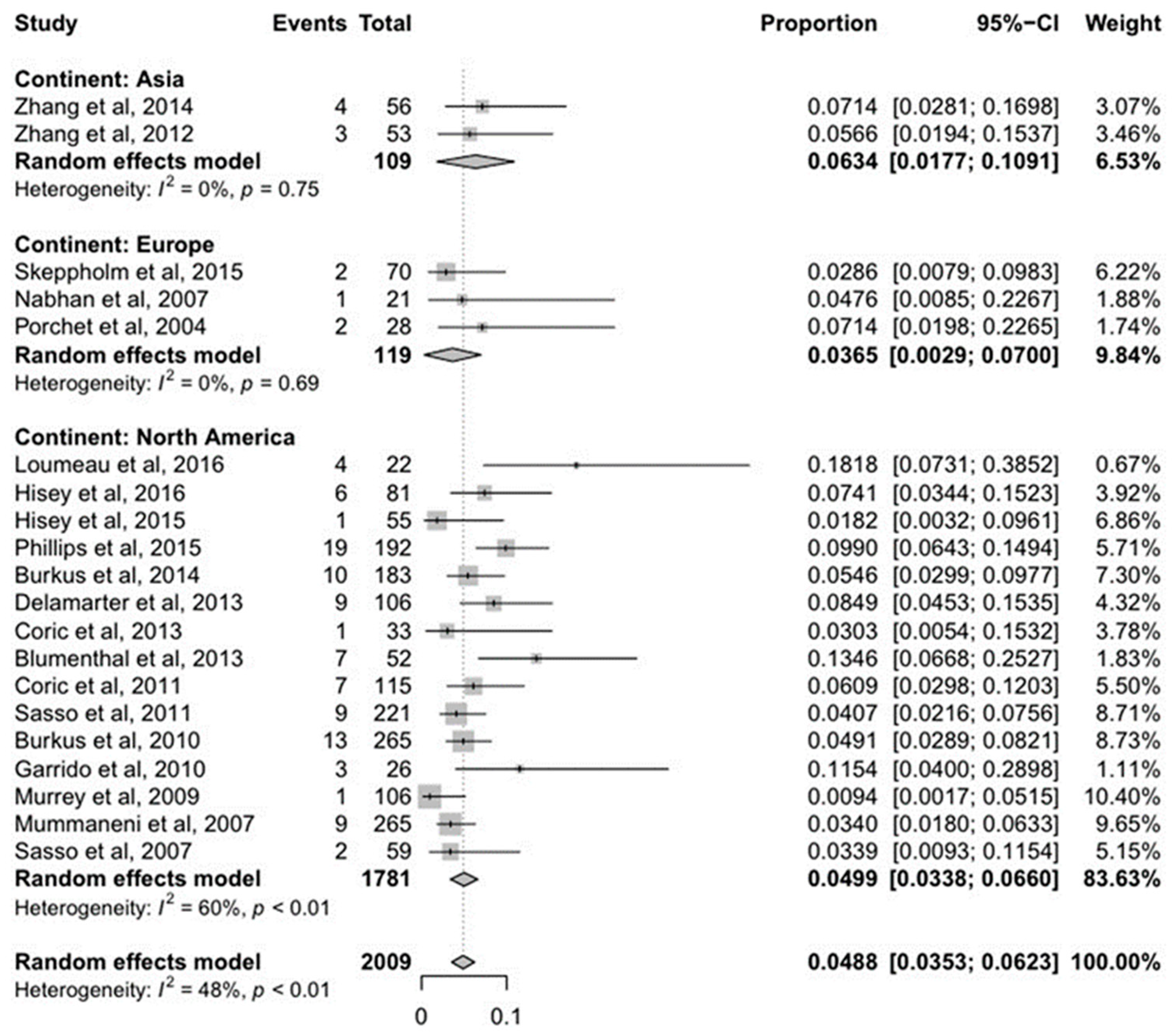
3.2.1. Continents
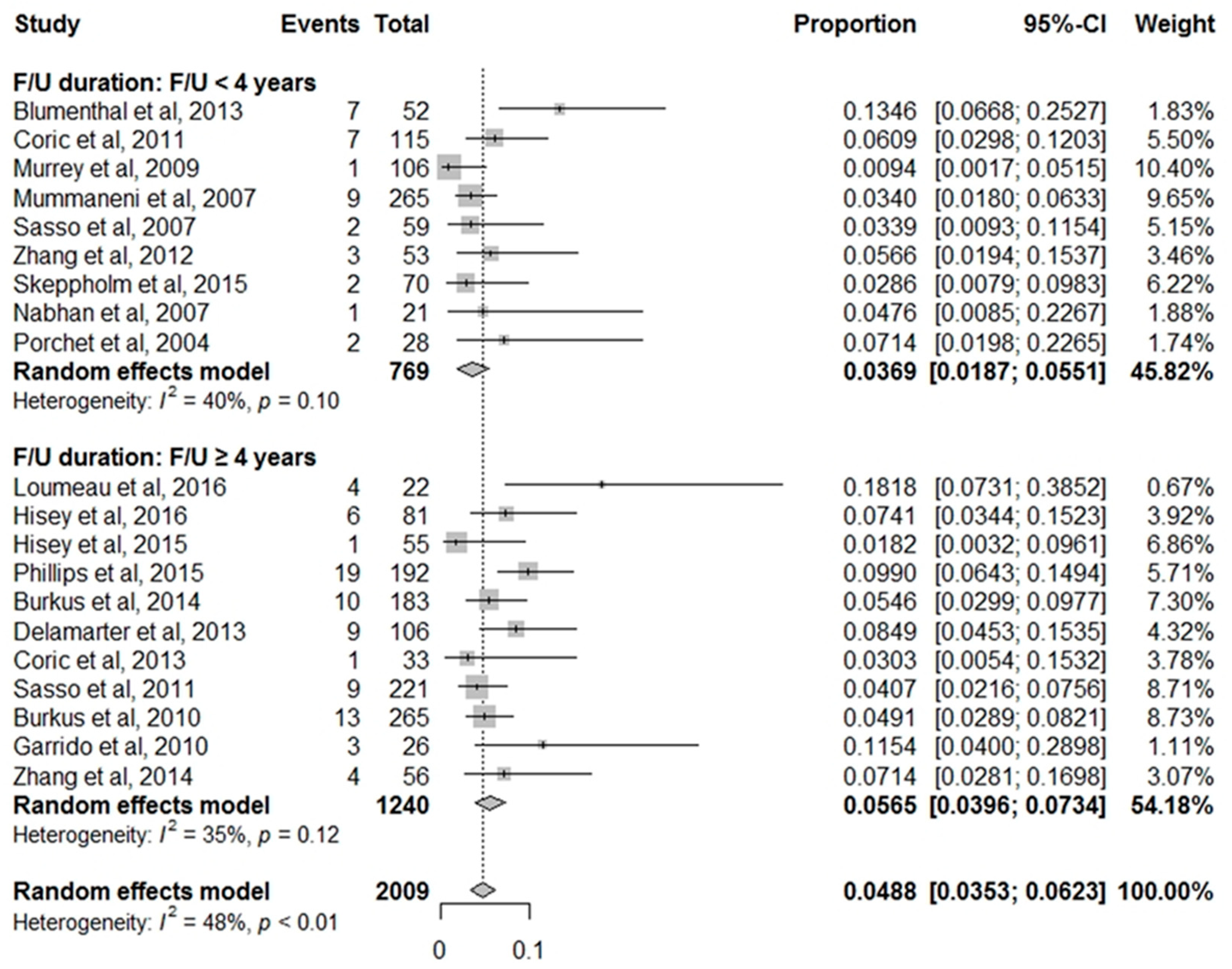
3.2.2. Follow-Up Duration
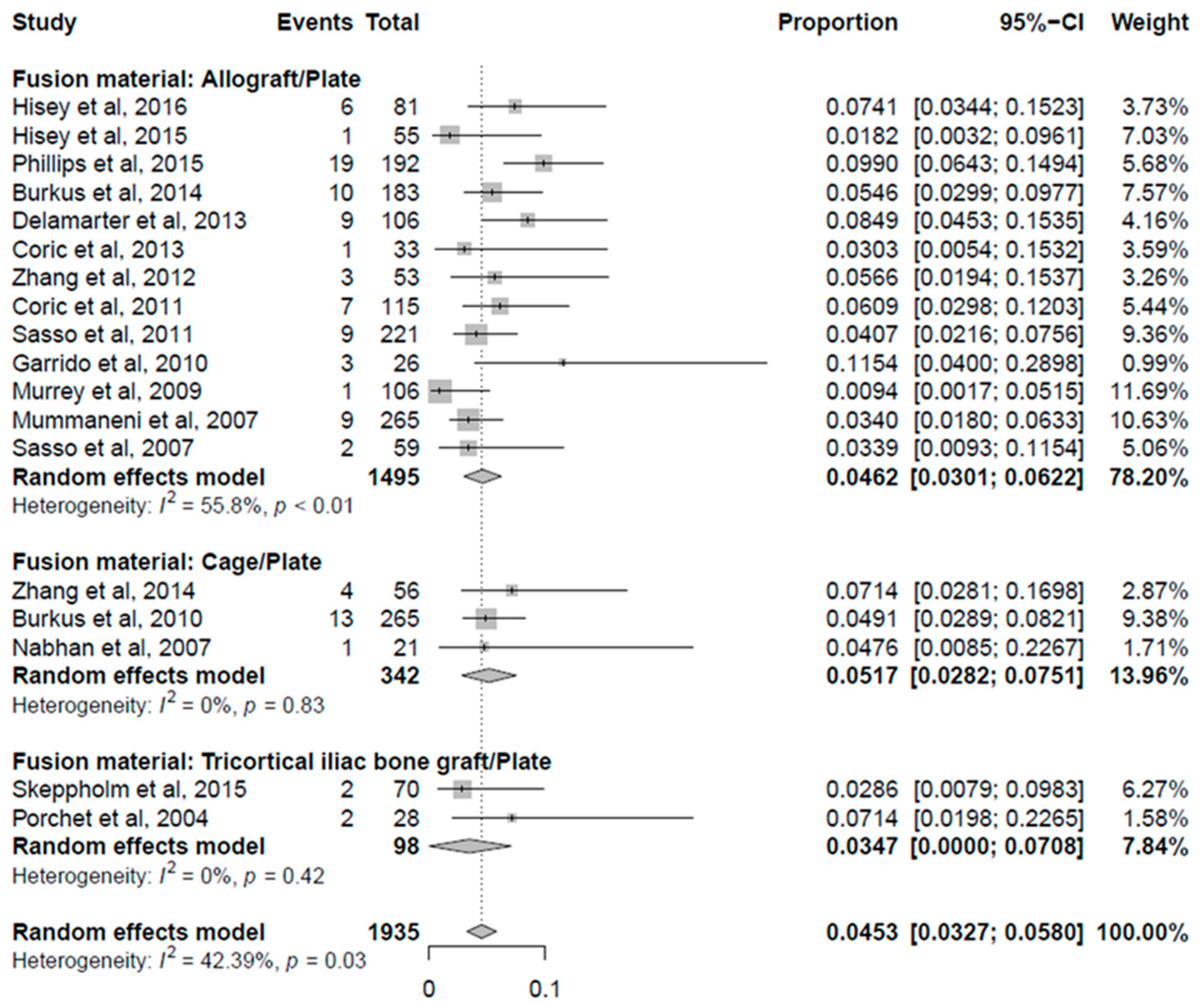
3.2.3. Fusion Material
4. Discussion
4.1. Background
4.2. Setting Up of Study Topic
4.3. Analysis of Our Results
4.4. Limitation of Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Burkhardt, B.W.; Brielmaier, M.; Schwerdtfeger, K.; Oertel, J.M. Clinical outcome following anterior cervical discectomy and fusion with and without anterior cervical plating for the treatment of cervical disc herniation—A 25-year follow-up study. Neurosurg. Rev. 2018, 41, 473–482. [Google Scholar] [CrossRef]
- Burkhardt, B.W.; Simgen, A.; Wagenpfeil, G.; Hendrix, P.; Dehnen, M.; Reith, W.; Oertel, J.M. Is there a difference in the grade of degeneration at the cervical spine following anterior cervical fusion with respect to clinical outcome, diagnosis, and repeat procedure? An MRI study of 102 patients with a mean follow-up of 25 years. J. Neurosurg. Spine 2019, 32, 335–343. [Google Scholar] [CrossRef]
- Hirvonen, T.; Siironen, J.; Marjamaa, J.; Niemelä, M.; Koski-Palkén, A. Anterior cervical discectomy and fusion in young adults leads to favorable outcome in long-term follow-up. Spine J. 2020, 20, 1073–1084. [Google Scholar] [CrossRef]
- Panjabi, M.M.; Duranceau, J.; Goel, V.; Oxland, T.; Takata, K. Cervical human vertebrae. Quantitative three-dimensional anatomy of the middle and lower regions. Spine (Phila. Pa 1976) 1991, 16, 861–869. [Google Scholar] [CrossRef]
- Tan, S.H.; Teo, E.C.; Chua, H.C. Quantitative three-dimensional anatomy of cervical, thoracic and lumbar vertebrae of Chinese Singaporeans. Eur. Spine J. 2004, 13, 137–146. [Google Scholar] [CrossRef] [Green Version]
- Yao, Q.; Yin, P.; Khan, K.; Tsai, T.Y.; Li, J.S.; Hai, Y.; Tang, P.; Li, G. Differences of the Morphology of Subaxial Cervical Spine Endplates between Chinese and White Men and Women. Biomed. Res. Int. 2018, 20, 2854175. [Google Scholar] [CrossRef]
- Higgins, J.P.; Altman, D.G.; Gøtzsche, P.C.; Jüni, P.; Moher, D.; Oxman, A.D.; Savovic, J.; Schulz, K.F.; Weeks, L.; Sterne, J.A. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ 2011, 18, 343. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, H.X.; Shao, Y.D.; Chen, Y.; Hou, Y.; Cheng, L.; Si, M.; Nie, L. A prospective, randomised, controlled multicentre study comparing cervical disc replacement with anterior cervical decompression and fusion. Int Orthop. 2014, 38, 2533–2541. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Zhang, X.; Chen, C.; Zhang, Y.; Wang, Z.; Wang, B.; Yan, W.; Li, M.; Yuan, W.; Wang, Y. Randomized, controlled, multicenter, clinical trial comparing BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion in China. Spine (Phila. Pa 1976) 2012, 37, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Skeppholm, M.; Lindgren, L.; Henriques, T.; Vavruch, L.; Löfgren, H.; Olerud, C. The Discover artificial disc replacement versus fusion in cervical radiculopathy—A randomized controlled outcome trial with 2-year follow-up. Spine J. 2015, 15, 1284–1294. [Google Scholar] [CrossRef]
- Nabhan, A.; Steudel, W.I.; Nabhan, A.; Pape, D.; Ishak, B. Segmental kinematics and adjacent level degeneration following disc replacement versus fusion: RCT with three years of follow-up. J. Long Term Eff. Med. Implants 2007, 17, 229–236. [Google Scholar] [CrossRef]
- Porchet, F.; Metcalf, N.H. Clinical outcomes with the Prestige II cervical disc: Preliminary results from a prospective randomized clinical trial. Neurosurg. Focus 2004, 17, E6. [Google Scholar] [CrossRef] [PubMed]
- Loumeau, T.P.; Darden, B.V.; Kesman, T.J.; Odum, S.M.; Van Doren, B.A.; Laxer, E.B.; Murrey, D.B. A RCT comparing 7-year clinical outcomes of one level symptomatic cervical disc disease (SCDD) following ProDisc-C total disc arthroplasty (TDA) versus anterior cervical discectomy and fusion (ACDF). Eur. Spine J. 2016, 25, 2263–2270. [Google Scholar] [CrossRef] [PubMed]
- Hisey, M.S.; Zigler, J.E.; Jackson, R.; Nunley, P.D.; Bae, H.W.; Kim, K.D.; Ohnmeiss, D.D. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. Int. J. Spine Surg. 2016, 10, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Phillips, F.M.; Geisler, F.H.; Gilder, K.M.; Reah, C.; Howell, K.M.; McAfee, P.C. Long-term Outcomes of the US FDA IDE Prospective, Randomized Controlled Clinical Trial Comparing PCM Cervical Disc Arthroplasty With Anterior Cervical Discectomy and Fusion. Spine (Phila. Pa 1976) 2015, 40, 674–683. [Google Scholar] [CrossRef] [Green Version]
- Hisey, M.S.; Bae, H.W.; Davis, R.J.; Gaede, S.; Hoffman, G.; Kim, K.D.; Nunley, P.D.; Peterson, D.; Rashbaum, R.F.; Stokes, J. Prospective, Randomized Comparison of Cervical Total Disk Replacement Versus Anterior Cervical Fusion: Results at 48 Months Follow-up. J. Spinal Disord. Tech. 2015, 28, E237–E243. [Google Scholar] [CrossRef]
- Burkus, J.K.; Traynelis, V.C.; Haid, R.W., Jr.; Mummaneni, P.V. Clinical and radiographic analysis of an artificial cervical disc: 7-year follow-up from the Prestige prospective randomized controlled clinical trial: Clinical article. J. Neurosurg. Spine 2014, 21, 516–528. [Google Scholar] [CrossRef]
- Delamarter, R.B.; Zigler, J. Five-year reoperation rates, cervical total disc replacement versus fusion, results of a prospective randomized clinical trial. Spine (Phila. Pa 1976) 2013, 38, 711–717. [Google Scholar] [CrossRef]
- Coric, D.; Kim, P.K.; Clemente, J.D.; Boltes, M.O.; Nussbaum, M.; James, S. Prospective randomized study of cervical arthroplasty and anterior cervical discectomy and fusion with long-term follow-up: Results in 74 patients from a single site. J. Neurosurg. Spine 2013, 18, 36–42. [Google Scholar] [CrossRef]
- Blumenthal, S.L.; Ohnmeiss, D.D.; Guyer, R.D.; Zigler, J.E. Reoperations in cervical total disc replacement compared with anterior cervical fusion: Results compiled from multiple prospective food and drug administration investigational device exemption trials conducted at a single site. Spine (Phila. Pa 1976) 2013, 38, 1177–1182. [Google Scholar] [CrossRef]
- Coric, D.; Nunley, P.D.; Guyer, R.D.; Musante, D.; Carmody, C.N.; Gordon, C.R.; Lauryssen, C.; Ohnmeiss, D.D.; Boltes, M.O. Prospective, randomized, multicenter study of cervical arthroplasty: 269 patients from the Kineflex|C artificial disc investigational device exemption study with a minimum 2-year follow-up: Clinical article. J. Neurosurg. Spine 2011, 15, 348–358. [Google Scholar] [CrossRef]
- Sasso, R.C.; Anderson, P.A.; Riew, K.D.; Heller, J.G. Results of cervical arthroplasty compared with anterior discectomy and fusion: Four-year clinical outcomes in a prospective, randomized controlled trial. J. Bone Joint Surg. Am. 2011, 93, 1684–1692. [Google Scholar] [CrossRef] [Green Version]
- Burkus, J.K.; Haid, R.W.; Traynelis, V.C.; Mummaneni, P.V. Long-term clinical and radiographic outcomes of cervical disc replacement with the Prestige disc: Results from a prospective randomized controlled clinical trial. J. Neurosurg. Spine 2010, 13, 308–318. [Google Scholar] [CrossRef]
- Garrido, B.J.; Taha, T.A.; Sasso, R.C. Clinical outcomes of Bryan cervical disc arthroplasty a prospective, randomized, controlled, single site trial with 48-month follow-up. J. Spinal Disord. Tech. 2010, 23, 367–371. [Google Scholar] [CrossRef]
- Murrey, D.; Janssen, M.; Delamarter, R.; Goldstein, J.; Zigler, J.; Tay, B.; Darden, B. Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J. 2009, 9, 275–286. [Google Scholar] [CrossRef] [PubMed]
- Mummaneni, P.V.; Burkus, J.K.; Haid, R.W.; Traynelis, V.C.; Zdeblick, T.A. Clinical and radiographic analysis of cervical disc arthroplasty compared with allograft fusion: A randomized controlled clinical trial. J. Neurosurg. Spine 2007, 6, 198–209. [Google Scholar] [CrossRef]
- Sasso, R.C.; Smucker, J.D.; Hacker, R.J.; Heller, J.G. Artificial disc versus fusion: A prospective, randomized study with 2-year follow-up on 99 patients. Spine (Phila. Pa 1976) 2007, 32, 2933–2940. [Google Scholar] [CrossRef] [PubMed]
- Dmitriev, A.E.; Cunningham, B.W.; Hu, N.; Sell, G.; Vigna, F.; McAfee, P.C. Adjacent level intradiscal pressure and segmental kinematics following a cervical total disc arthroplasty: An in vitro human cadaveric model. Spine (Phila. Pa 1976) 2005, 30, 1165–1172. [Google Scholar] [CrossRef] [PubMed]
- Alhashash, M.; Allouch, H.; Boehm, H.; Shousha, M. Results of Four-Level Anterior Cervical Discectomy and Fusion Using Stand-Alone Interbody Titanium Cages. Asian Spine J. 2021. [Google Scholar] [CrossRef]
- Kanna, R.M.; Perambuduri, A.S.; Shetty, A.P.; Rajasekaran, S. A Randomized Control Trial Comparing Local Autografts and Allografts in Single Level Anterior Cervical Discectomy and Fusion Using a StandAlone Cage. Asian Spine J. 2020. [Google Scholar] [CrossRef]
- Fuller, D.A.; Kirkpatrick, J.S.; Emery, S.E.; Wilber, R.G.; Davy, D.T. A kinematic study of the cervical spine before and after segmental arthrodesis. Spine (Phila. Pa 1976) 1998, 23, 1649–1656. [Google Scholar] [CrossRef]
- Kulkarni, V.; Rajshekhar, V.; Raghuram, L. Accelerated spondylotic changes adjacent to the fused segment following central cervical corpectomy: Magnetic resonance imaging study evidence. J. Neurosurg. 2004, 100 (Suppl. S1), 2–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Matsunaga, S.; Kabayama, S.; Yamamoto, T.; Yone, K.; Sakou, T.; Nakanishi, K. Strain on intervertebral discs after anterior cervical decompression and fusion. Spine (Phila. Pa 1976) 1999, 24, 670–675. [Google Scholar] [CrossRef] [PubMed]
- Hilibrand, A.S.; Carlson, G.D.; Palumbo, M.A.; Jones, P.K.; Bohlman, H.H. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J. Bone Joint Surg. Am. 1999, 81, 519–528. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chung, J.Y.; Kim, S.K.; Jung, S.T.; Lee, K.B. Clinical adjacent-segment pathology after anterior cervical discectomy and fusion: Results after a minimum of 10-year follow-up. Spine J. 2014, 14, 2290–2298. [Google Scholar] [CrossRef] [PubMed]
- Chung, J.Y.; Park, J.B.; Seo, H.Y.; Kim, S.K. Adjacent Segment Pathology after Anterior Cervical Fusion. Asian Spine J. 2016, 10, 582–592. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, M.K.; Kwak, D.S.; Park, C.K.; Park, S.H.; Oh, S.M.; Lee, S.W.; Han, S.H. Quantitative anatomy of the endplate of the middle and lower cervical vertebrae in Koreans. Spine (Phila. Pa 1976) 2007, 32, E376–E381. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No | Authors | Journal | Year | cASP * That Underwent Surgery (%) | Country | Number of Patients | Follow-Up (Years) |
|---|---|---|---|---|---|---|---|
| 1 | Zhang et al. [8] | Int. Orthop. | 2014 | 4 (7.1%) | China | 56 | 4 |
| 2 | Zhang et al. [9] | Spine (Phila. Pa 1976) | 2012 | 3 (5.7%) | China | 53 | 2 |
| 3 | Skeppholm et al. [10] | Spine J. | 2015 | 2 (2.9%) | Sweden | 70 | 2 |
| 4 | Nabhan et al. [11] | J. Long Term Eff. Med. Implants | 2007 | 1 (5%) | Germany | 21 | 3 |
| 5 | Porchet et al. [12] | Neurosurg. Focus | 2004 | 2 (7%) | Switzerland | 28 | 2 |
| 6 | Loumeau et al. [13] | Eur. Spine J. | 2016 | 4 (18.2%) | USA | 22 | 7 |
| 7 | Hisey et al. [14] | Int. J. Spine Surg. | 2016 | 6 (7.4%) | USA | 81 | 5 |
| 8 | Phillips et al. [15] | Spine (Phila. Pa 1976) | 2015 | 19 (9.9%) | USA | 192 | 5 |
| 9 | Hisey et al. [16] | J. Spinal Disord. Tech. | 2015 | 1 (1.8%) | USA | 55 | 4 |
| 10 | Burkus et al. [17] | J. Neurosurg. Spine | 2014 | 10 (5.4%) | USA | 183 | 7 |
| 11 | Delamarter et al. [18] | Spine (Phila. Pa 1976) | 2013 | 6 (5.7%) | USA | 106 | 5 |
| 12 | Coric et al. [19] | J. Neurosurg. Spine | 2013 | 1 (3.0%) | USA | 33 | 4 |
| 13 | Blumenthal et al. [20] | Spine (Phila. Pa 1976) | 2013 | 7 (13.5%) | USA | 52 | 2 |
| 14 | Coric et al. [21] | J. Neurosurg. Spine | 2011 | 7 (6.1%) | USA | 115 | 2 |
| 15 | Sasso et al. [22] | JBJS | 2011 | 9 (6.5%) | USA | 138 | 4 |
| 16 | Burkus et al. [23] | J. Neurosurg. Spine | 2010 | 13 (10.2%) | USA | 127 | 5 |
| 17 | Garrido et al. [24] | J. Spinal Disord. Tech. | 2010 | 3 (11.5%) | USA | 26 | 4 |
| 18 | Murrey et al. [25] | Spine J. | 2009 | 1 (1.0%) | USA | 106 | 2 |
| 19 | Mummaneni et al. [26] | J. Neurosurg. Spine | 2007 | 9 (3.4%) | USA | 265 | 2 |
| 20 | Sasso et al. [27] | Spine (Phila. Pa 1976) | 2007 | 2 (3.4%) | USA | 59 | 2 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, Y.-W.; Kim, S.-K.; Park, Y.-J. Differences in the Prevalence of Clinical Adjacent Segment Pathology among Continents after Anterior Cervical Fusion: Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2021, 10, 4125. https://doi.org/10.3390/jcm10184125
Chung Y-W, Kim S-K, Park Y-J. Differences in the Prevalence of Clinical Adjacent Segment Pathology among Continents after Anterior Cervical Fusion: Meta-Analysis of Randomized Controlled Trials. Journal of Clinical Medicine. 2021; 10(18):4125. https://doi.org/10.3390/jcm10184125
Chicago/Turabian StyleChung, Young-Woo, Sung-Kyu Kim, and Yong-Jin Park. 2021. "Differences in the Prevalence of Clinical Adjacent Segment Pathology among Continents after Anterior Cervical Fusion: Meta-Analysis of Randomized Controlled Trials" Journal of Clinical Medicine 10, no. 18: 4125. https://doi.org/10.3390/jcm10184125