
Triglyceride-Glucose Index in Non-Diabetic, Non-Obese Patients with Obstructive Sleep Apnoea

 ,
,  ,
,  , ,
, ,
Abstract
:1. Introduction
2. Methods
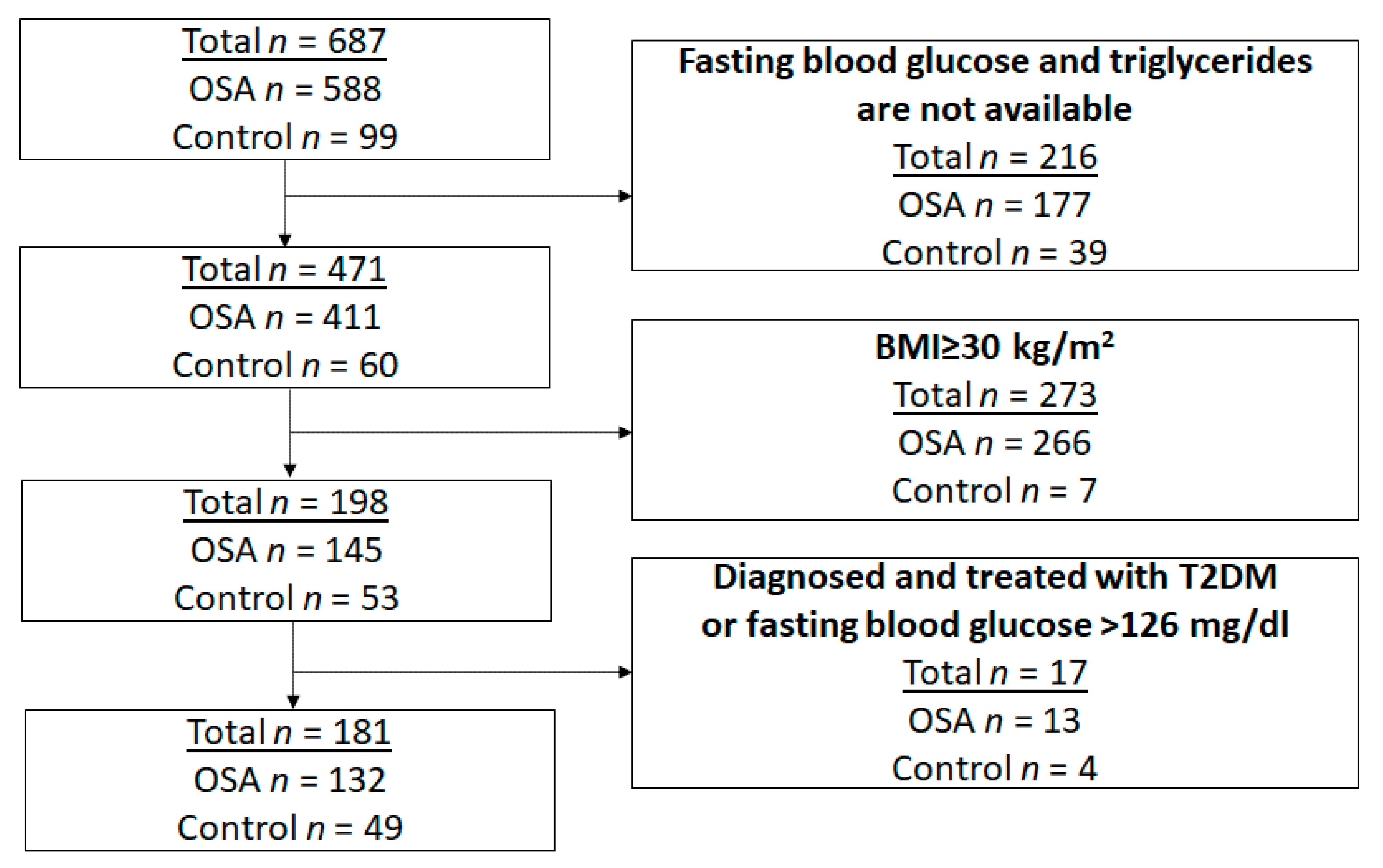
2.1. Study Subjects and Design
2.2. Sleep Studies
2.3. Statistical Analysis
3. Results
3.1. Demographics and Clinical Characteristics of the OSA and Control Groups
3.2. Relationship between Triglyceride-Glucose Index and Demographics as Well as Sleep and Clinical Characteristics
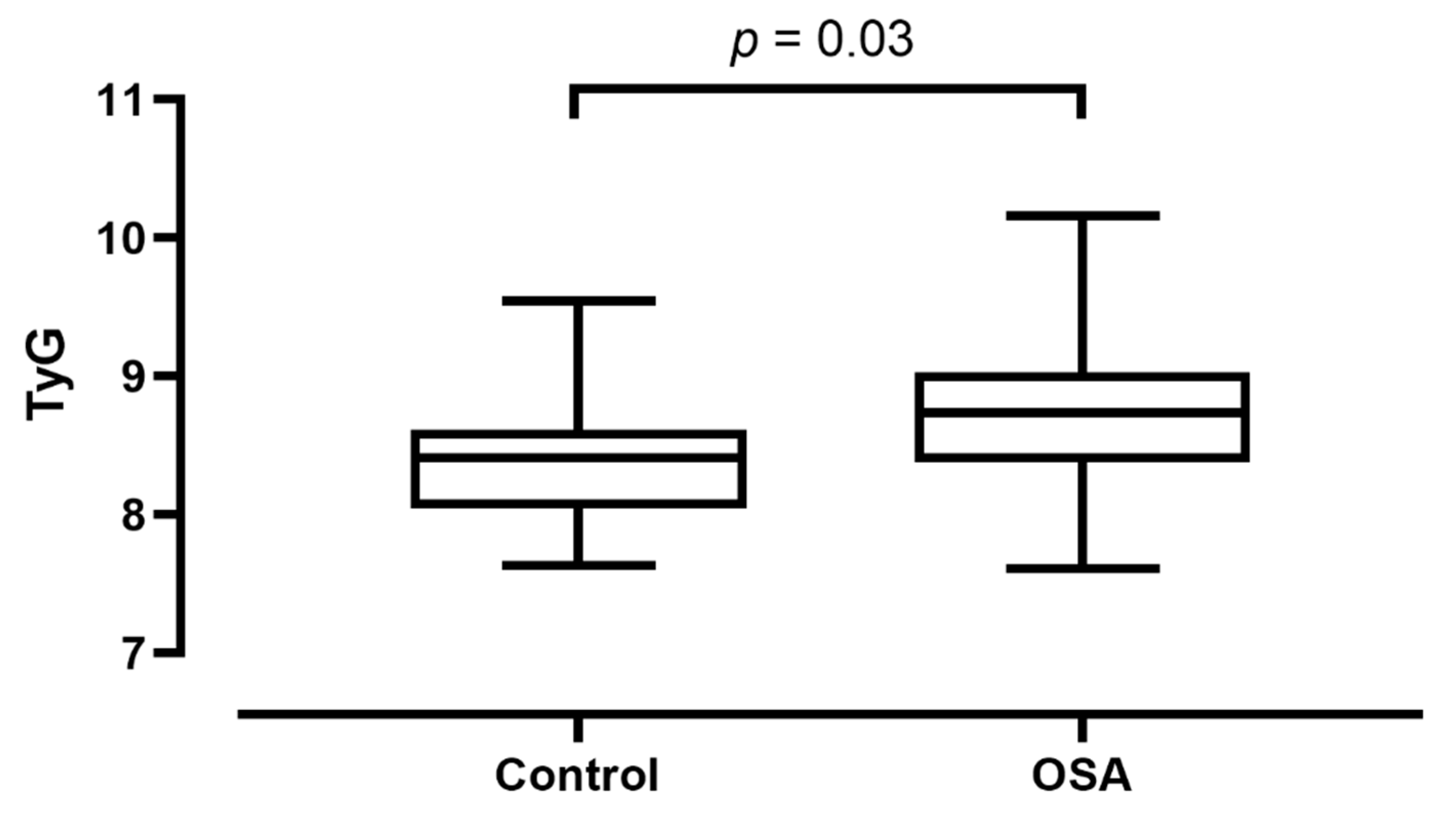
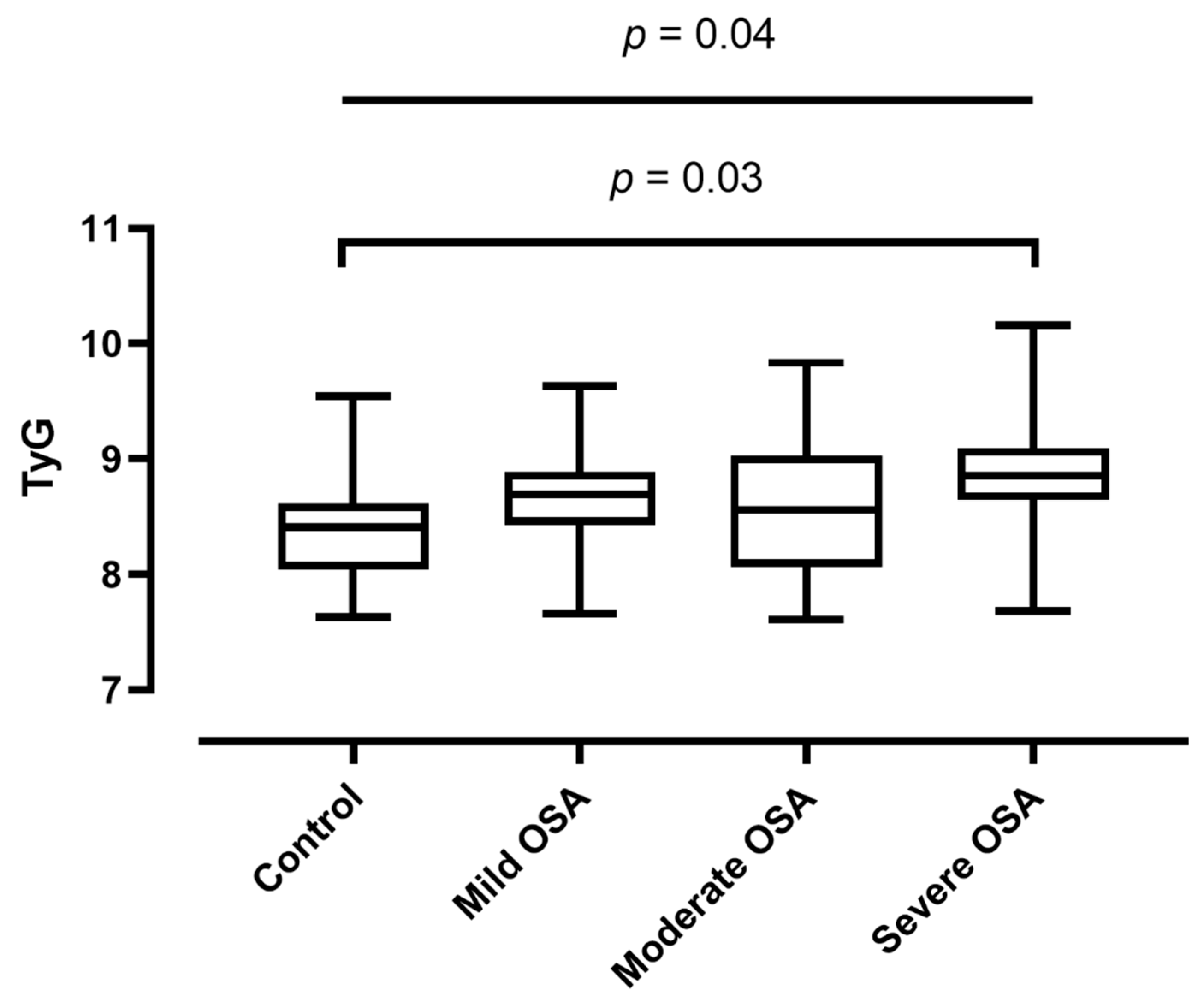
3.3. Triglyceride-Glucose Index in OSA vs. Controls
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Kent, B.D.; Grote, L.; Ryan, S.; Pépin, J.L.; Bonsignore, M.R.; Tkacova, R.; Saaresranta, T.; Verbraecken, J.; Lévy, P.; Hedner, J.; et al. Diabetes mellitus prevalence and control in sleep-disordered breathing: The European Sleep Apnea Cohort (ESADA) study. Chest 2014, 146, 982–990. [Google Scholar] [CrossRef]
- Ormazabal, V.; Nair, S.; Elfeky, O.; Aguayo, C.; Salomon, C.; Zuñiga, F.A. Association between insulin resistance and the development of cardiovascular disease. Cardiovasc. Diabetol. 2018, 17, 122. [Google Scholar] [CrossRef] [PubMed]
- Zhou, M.-S.; Schulman, I.H.; Raij, L. Vascular inflammation, insulin resistance, and endothelial dysfunction in salt-sensitive hypertension: Role of nuclear factor kappa B activation. J. Hypertens. 2010, 28, 527–535. [Google Scholar] [CrossRef] [PubMed]
- Kahn, B.B.; Flier, J.S. Obesity and insulin resistance. J. Clin. Investig. 2000, 106, 473–481. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Howard, G.; O’Leary, D.H.; Zaccaro, D.J.; Haffner, S.M.; Rewers, M.; Hamman, R.F.; Selby, J.V.; Saad, M.F.; Savage, P.J.; Bergman, R.N. Insulin sensitivity and atherosclerosis. Circulation 1996, 93, 1809–1817. [Google Scholar] [CrossRef]
- Gast, K.B.; Tjeerdema, N.; Stijnen, T.; Smit, J.W.A.; Dekkers, O.M. Insulin resistance and risk of incident cardiovascular events in adults without diabetes: Meta-analysis. PLoS ONE 2012, 7, e52036. [Google Scholar] [CrossRef] [Green Version]
- Lindberg, E.; Theorell-Haglöw, J.; Svensson, M.; Gislason, T.; Berne, C.; Janson, C. Sleep apnea and glucose metabolism: A long-term follow-up in a community-based sample. Chest 2012, 142, 935–942. [Google Scholar] [CrossRef]
- Gabryelska, A.; Karuga, F.F.; Szmyd, B.; Białasiewicz, P. HIF-1α as a mediator of insulin resistance, T2DM, and its complications: Potential links with obstructive sleep apnea. Front. Physiol. 2020, 11. [Google Scholar] [CrossRef]
- Sacramento, J.; Ribeiro, M.; Rodrigues, T.; Guarino, M.; Diogo, L.; Seiça, R.; Monteiro, E.; Matafome, P.; Conde, S. Insulin resistance is associated with tissue-specific regulation of HIF-1α and HIF-2α during mild chronic intermittent hypoxia. Respir. Physiol. Neurobiol. 2016, 228, 30–38. [Google Scholar] [CrossRef]
- Murphy, A.M.; Thomas, A.; Crinion, S.J.; Kent, B.D.; Tambuwala, M.M.; Fabre, A.; Pepin, J.-L.; Roche, H.M.; Arnaud, C.; Ryan, S. Intermittent hypoxia in obstructive sleep apnoea mediates insulin resistance through adipose tissue inflammation. Eur. Respir. J. 2017, 49, 1601731. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, S.O.; He, K.; Narla, R.R.; Kang, H.G.; Ryu, H.U.; Boyko, E.J. Metabolic consequences of obstructive sleep apnea especially pertaining to diabetes mellitus and insulin sensitivity. Diabetes Metab. J. 2019, 43, 144–155. [Google Scholar] [CrossRef] [PubMed]
- Bonsignore, M.R.; Borel, A.-L.; Machan, E.; Grunstein, R. Sleep apnoea and metabolic dysfunction. Eur. Respir. Rev. 2013, 22, 353–364. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chen, L.; Kuang, J.; Pei, J.-H.; Chen, H.-M.; Chen, Z.; Li, Z.-W.; Yang, H.-Z.; Fu, X.-Y.; Wang, L.; Chen, Z.-J.; et al. Continuous positive airway pressure and diabetes risk in sleep apnea patients: A systemic review and meta-analysis. Eur. J. Intern. Med. 2017, 39, 39–50. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tohidi, M.; Arbab, P.; Ghasemi, A. Assay-dependent variability of serum insulin concentrations: A comparison of eight assays. Scand. J. Clin. Lab. Investig. 2017, 77, 122–129. [Google Scholar] [CrossRef]
- Sánchez-García, A.; Rodríguez-Gutiérrez, R.; Mancillas-Adame, L.; González-Nava, V.; González-Colmenero, A.D.; Solis, R.C.; Álvarez-Villalobos, N.A.; González-González, J.G. Diagnostic accuracy of the triglyceride and glucose index for insulin resistance: A systematic review. Int. J. Endocrinol. 2020, 2020, 1–7. [Google Scholar] [CrossRef]
- Kang, H.H.; Kim, S.W.; Lee, S.H. Association between triglyceride glucose index and obstructive sleep apnea risk in Korean adults: A cross-sectional cohort study. Lipids Health Dis. 2020, 19, 1–8. [Google Scholar] [CrossRef]
- Zou, J.; Wang, Y.; Xu, H.; Xia, Y.; Qian, Y.; Zou, J.; Guan, J.; Chen, B.; Yi, H.; Yin, S. The use of visceral adiposity variables in the prediction of obstructive sleep apnea: Evidence from a large cross-sectional study. Sleep Breath. 2020, 24, 1373–1382. [Google Scholar] [CrossRef]
- Peppard, P.E.; Young, T.; Barnet, J.H.; Palta, M.; Hagen, E.W.; Hla, K.M. Increased prevalence of sleep-disordered breathing in adults. Am. J. Epidemiol. 2013, 177, 1006–1014. [Google Scholar] [CrossRef] [Green Version]
- Dresner, A.; Laurent, D.; Marcucci, M.; Griffin, M.E.; Dufour, S.; Cline, G.W.; Slezak, L.A.; Andersen, D.K.; Hundal, R.S.; Rothman, D.L.; et al. Effects of free fatty acids on glucose transport and IRS-1–associated phosphatidylinositol 3-kinase activity. J. Clin. Investig. 1999, 103, 253–259. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Barnes, G.T.; Yang, Q.; Tan, G.; Yang, D.; Chou, C.J.; Sole, J.; Nichols, A.; Ross, J.S.; Tartaglia, L.A.; et al. Chronic inflammation in fat plays a crucial role in the development of obesity-related insulin resistance. J. Clin. Investig. 2003, 112, 1821–1830. [Google Scholar] [CrossRef]
- Bikov, A.; Lazar, Z.; Horvath, P.; Tarnoki, D.L.; Tarnoki, A.D.; Fesus, L.; Horvath, M.; Meszaros, M.; Losonczy, G.; Kunos, L. Association between serum lipid profile and obstructive respiratory events during REM and non-REM sleep. Lung 2019, 197, 443–450. [Google Scholar] [CrossRef] [Green Version]
- Guan, J.; Yi, H.; Zou, J.; Meng, L.; Tang, X.; Zhu, H.; Yu, D.; Zhou, H.; Su, K.; Yang, M.; et al. Distinct severity stages of obstructive sleep apnoea are correlated with unique dyslipidaemia: Large-scale observational study. Thorax 2016, 71, 347–355. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikov, A.; Frent, S.; Pleava, R.; Kunos, L.; Bokhari, S.; Meszaros, M.; Mihaicuta, S. The burden of associated comorbidities in patients with obstructive sleep apnea—Regional differences in two Central-Eastern European sleep centers. J. Clin. Med. 2020, 9, 3583. [Google Scholar] [CrossRef] [PubMed]
- Kushida, C.A.; Littner, M.R.; Morgenthaler, T.; Alessi, C.A.; Bailey, D.; Coleman, J.; Friedman, L.; Hirshkowitz, M.; Kapen, S.; Kramer, M.; et al. Practice parameters for the indications for polysomnography and related procedures: An update for 2005. Sleep 2005, 28, 499–523. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berry, R.B.; Budhiraja, R.; Gottlieb, D.J.; Gozal, D.; Iber, C.; Kapur, V.K.; Marcus, C.L.; Mehra, R.; Parthasarathy, S.; Quan, S.F.; et al. Rules for scoring respiratory events in sleep: Update of the 2007 AASM Manual for the Scoring of Sleep and Associated Events. Deliberations of the sleep apnea definitions Task Force of the American Academy of Sleep Medicine. J. Clin. Sleep Med. 2012, 8, 597–619. [Google Scholar] [CrossRef] [Green Version]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.-G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Behav. Res. Methods 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bianchi, V.E.; Herbert, W.G.; Myers, J.; Ribisl, P.M.; Miller, L.E.; Dalman, R.L. Relationship of obstructive sleep apnea and cardiometabolic risk factors in elderly patients with abdominal aortic aneurysm. Sleep Breath. 2015, 19, 593–598. [Google Scholar] [CrossRef] [PubMed]
- Meszaros, M.; Tarnoki, A.D.; Tarnoki, D.L.; Kovacs, D.T.; Forgo, B.; Lee, J.; Sung, J.; Vestbo, J.; Müller, V.; Kunos, L.; et al. Obstructive sleep apnea and hypertriglyceridaemia share common genetic background: Results of a twin study. J. Sleep Res. 2020, 29, e12979. [Google Scholar] [CrossRef] [Green Version]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2019, 130, 158–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabryelska, A.; Szmyd, B.; Szemraj, J.; Stawski, R.; Sochal, M.; Białasiewicz, P. Patients with obstructive sleep apnea present with chronic upregulation of serum HIF-1α protein. J. Clin. Sleep Med. 2020, 16, 1761–1768. [Google Scholar] [CrossRef]
- Gaspar, J.M.; Velloso, L.A. Hypoxia inducible factor as a central regulator of metabolism—Implications for the development of obesity. Front. Neurosci. 2018, 12, 813. [Google Scholar] [CrossRef] [PubMed]
- Mesarwi, O.; Polak, J.; Jun, J.; Polotsky, V.Y. Sleep disorders and the development of insulin resistance and obesity. Endocrinol. Metab. Clin. N. Am. 2013, 42, 617–634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bikov, A.; Meszaros, M.; Kunos, L.; Negru, A.; Frent, S.; Mihaicuta, S. Atherogenic index of plasma in obstructive sleep apnoea. J. Clin. Med. 2021, 10, 417. [Google Scholar] [CrossRef] [PubMed]
- Szmyd, B.; Rogut, M.; Białasiewicz, P.; Gabryelska, A. The impact of glucocorticoids and statins on sleep quality. Sleep Med. Rev. 2021, 55, 101380. [Google Scholar] [CrossRef] [PubMed]
- Tramunt, B.; Smati, S.; Grandgeorge, N.; Lenfant, F.; Arnal, J.-F.; Montagner, A.; Gourdy, P. Sex differences in metabolic regulation and diabetes susceptibility. Diabetologia 2020, 63, 453–461. [Google Scholar] [CrossRef] [Green Version]
- Xie, Y.; Guo, R.; Li, Z.; Guo, X.; Sun, G.; Sun, Z.; Zheng, J.; Sun, Y.; Zheng, L. Temporal relationship between body mass index and triglyceride-glucose index and its impact on the incident of hypertension. Nutr. Metab. Cardiovasc. Dis. 2019, 29, 1220–1229. [Google Scholar] [CrossRef] [Green Version]
- Bikov, A.; Kolossváry, M.; Jermendy, A.L.; Drobni, Z.D.; Tarnoki, A.D.; Tarnoki, D.L.; Forgó, B.; Kovacs, D.T.; Losonczy, G.; Kunos, L.; et al. Comprehensive coronary plaque assessment in patients with obstructive sleep apnea. J. Sleep Res. 2019, 28, e12828. [Google Scholar] [CrossRef]
- Hong, S.; Han, K.; Park, C.Y. The triglyceride glucose index is a simple and low-cost marker associated with atherosclerotic cardiovascular disease: A population-based study. BMC Med. 2020, 18, 361. [Google Scholar] [CrossRef]
- Da Silva, A.; Caldas, A.P.; Hermsdorff, H.H.; Bersch-Ferreira, Â.C.; Torreglosa, C.R.; Weber, B.; Bressan, J. Triglyceride-glucose index is associated with symptomatic coronary artery disease in patients in secondary care. Cardiovasc. Diabetol. 2019, 18, 89. [Google Scholar] [CrossRef]
- Park, G.-M.; Cho, Y.-R.; Won, K.-B.; Yang, Y.J.; Park, S.; Ann, S.H.; Kim, Y.-G.; Park, E.J.; Kim, S.-J.; Lee, S.-G.; et al. Triglyceride glucose index is a useful marker for predicting subclinical coronary artery disease in the absence of traditional risk factors. Lipids Health Dis. 2020, 19, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Won, K.-B.; Park, E.J.; Han, D.; Lee, J.H.; Choi, S.-Y.; Chun, E.J.; Park, S.H.; Han, H.-W.; Sung, J.; Jung, H.O.; et al. Triglyceride glucose index is an independent predictor for the progression of coronary artery calcification in the absence of heavy coronary artery calcification at baseline. Cardiovasc. Diabetol. 2020, 19, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Irace, C.; Carallo, C.; Scavelli, F.B.; De Franceschi, M.S.; Esposito, T.; Tripolino, C.; Gnasso, A. Markers of insulin resistance and carotid atherosclerosis. A comparison of the homeostasis model assessment and triglyceride glucose index. Int. J. Clin. Pract. 2013, 67, 665–672. [Google Scholar] [CrossRef] [PubMed]
- Wang, K.; He, G.; Zhang, Y.; Yin, J.; Yan, Y.; Zhang, Y.; Wang, K. Association of triglyceride-glucose index and its interaction with obesity on hypertension risk in Chinese: A population-based study. J. Hum. Hypertens. 2021, 35, 232–239. [Google Scholar] [CrossRef] [PubMed]
- Zhu, B.; Wang, J.; Chen, K.; Yan, W.; Wang, A.; Wang, W.; Gao, Z.; Tang, X.; Yan, L.; Wan, Q.; et al. A high triglyceride glucose index is more closely associated with hyper-tension than lipid or glycemic parameters in elderly individuals: A cross-sectional survey from the Reaction Study. Cardiovasc. Diabetol. 2020, 19, 112. [Google Scholar] [CrossRef]
- Lambrinoudaki, I.; Kazani, M.V.; Armeni, E.; Georgiopoulos, G.; Tampakis, K.; Rizos, D.; Augoulea, A.; Kaparos, G.; Alexandrou, A.; Stamatelopoulos, K. The TyG index as a marker of subclinical atherosclerosis and arterial stiffness in lean and overweight postmenopausal women. Heart Lung Circ. 2018, 27, 716–724. [Google Scholar] [CrossRef]
- Randerath, W.; Bassetti, C.L.; Bonsignore, M.R.; Farre, R.; Ferini-Strambi, L.; Grote, L.; Hedner, J.; Kohler, M.; Martinez-Garcia, M.A.; Mihaicuta, S.; et al. Challenges and perspectives in obstructive sleep apnoea: Report by an ad hoc working group of the Sleep Disordered Breathing Group of the European Respiratory Society and the European Sleep Research Society. Eur. Respir. J. 2018, 52, 1702616. [Google Scholar] [CrossRef]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J. Clin. Sleep Med. 2017, 13, 479–504. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| OSA (n = 132) | Control (n = 49) | p | |
|---|---|---|---|
| Age (years) | 53/44–60/ | 47/29–59/ | 0.03 |
| Gender (male%) | 70 | 33 | <0.01 |
| BMI (kg/m2) | 26.8/24.8–28.6/ | 23.9/20.8–26.9/ | <0.01 |
| Smoking (ever%) | 39 | 4 | <0.01 |
| Cigarette pack years | 0/0–11/ | 0/0–0/ | <0.01 |
| Hypertension (%) | 55 | 35 | 0.03 |
| Cardiovascular and cerebrovascular disease (%) | 23 | 4 | <0.01 |
| Arrhythmia (%) | 22 | 18 | 0.75 |
| Total cholesterol (mmol/L) | 5.0/4.3–6.1/ | 5.2/4.7–5.9/ | 0.28 |
| HDL-C (mmol/L) | 1.1/1.0–1.4/ | 1.6/1.4–2.0/ | <0.01 |
| LDL-C (mmol/L) | 2.9/2.3–3.8/ | 3.0/2.6–3.7/ | 0.85 |
| TG (mmol/L) | 1.7/1.2–2.0/ | 1.2/0.9–1.5/ | <0.01 |
| Glucose (mmol/L) | 4.8/4.4–5.3/ | 4.7/4.2–4.9/ | 0.02 |
| TyG | 8.72 ± 0.49 | 8.37 ± 0.40 | <0.01 |
| ESS | 8.0/5.0–10.0/ | 6.0/4.0–9.0/ | 0.07 |
| TST (min) | 420/367–453/ | 388/354–431/ | 0.11 |
| SPT (min) | 466/430–505/ | 425/398–463/ | <0.01 |
| Sleep% (%) | 92/82–96/ | 94/84–99/ | 0.12 |
| REM% (%) | 15/12–19/ | 14/10–19/ | 0.11 |
| AHI (1/h) | 24.1/12.2–40.7/ | 1.9/1.2–2.8/ | <0.01 |
| ODI (1/h) | 21.4/9.9–35.4/ | 0.9/0.2–1.7/ | <0.01 |
| TST90% (%) | 3.4/0.2–13.2/ | 0.0/0.0–0.1/ | <0.01 |
| MinSatO2 (%) | 85/81–88/ | 91/89–93/ | <0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bikov, A.; Frent, S.M.; Meszaros, M.; Kunos, L.; Mathioudakis, A.G.; Negru, A.G.; Gaita, L.; Mihaicuta, S. Triglyceride-Glucose Index in Non-Diabetic, Non-Obese Patients with Obstructive Sleep Apnoea. J. Clin. Med. 2021, 10, 1932. https://doi.org/10.3390/jcm10091932
Bikov A, Frent SM, Meszaros M, Kunos L, Mathioudakis AG, Negru AG, Gaita L, Mihaicuta S. Triglyceride-Glucose Index in Non-Diabetic, Non-Obese Patients with Obstructive Sleep Apnoea. Journal of Clinical Medicine. 2021; 10(9):1932. https://doi.org/10.3390/jcm10091932
Chicago/Turabian StyleBikov, Andras, Stefan M. Frent, Martina Meszaros, Laszlo Kunos, Alexander G. Mathioudakis, Alina Gabriela Negru, Laura Gaita, and Stefan Mihaicuta. 2021. "Triglyceride-Glucose Index in Non-Diabetic, Non-Obese Patients with Obstructive Sleep Apnoea" Journal of Clinical Medicine 10, no. 9: 1932. https://doi.org/10.3390/jcm10091932