
Impact of Adjuvant Chemotherapy on Survival of Patients with Advanced Residual Disease at Radical Cystectomy following Neoadjuvant Chemotherapy: Systematic Review and Meta-Analysis

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Inclusion Criteria
2.3. Data Extraction
2.4. Quality and Risk-of-Bias Assessment
2.5. Statistical Analysis
3. Results
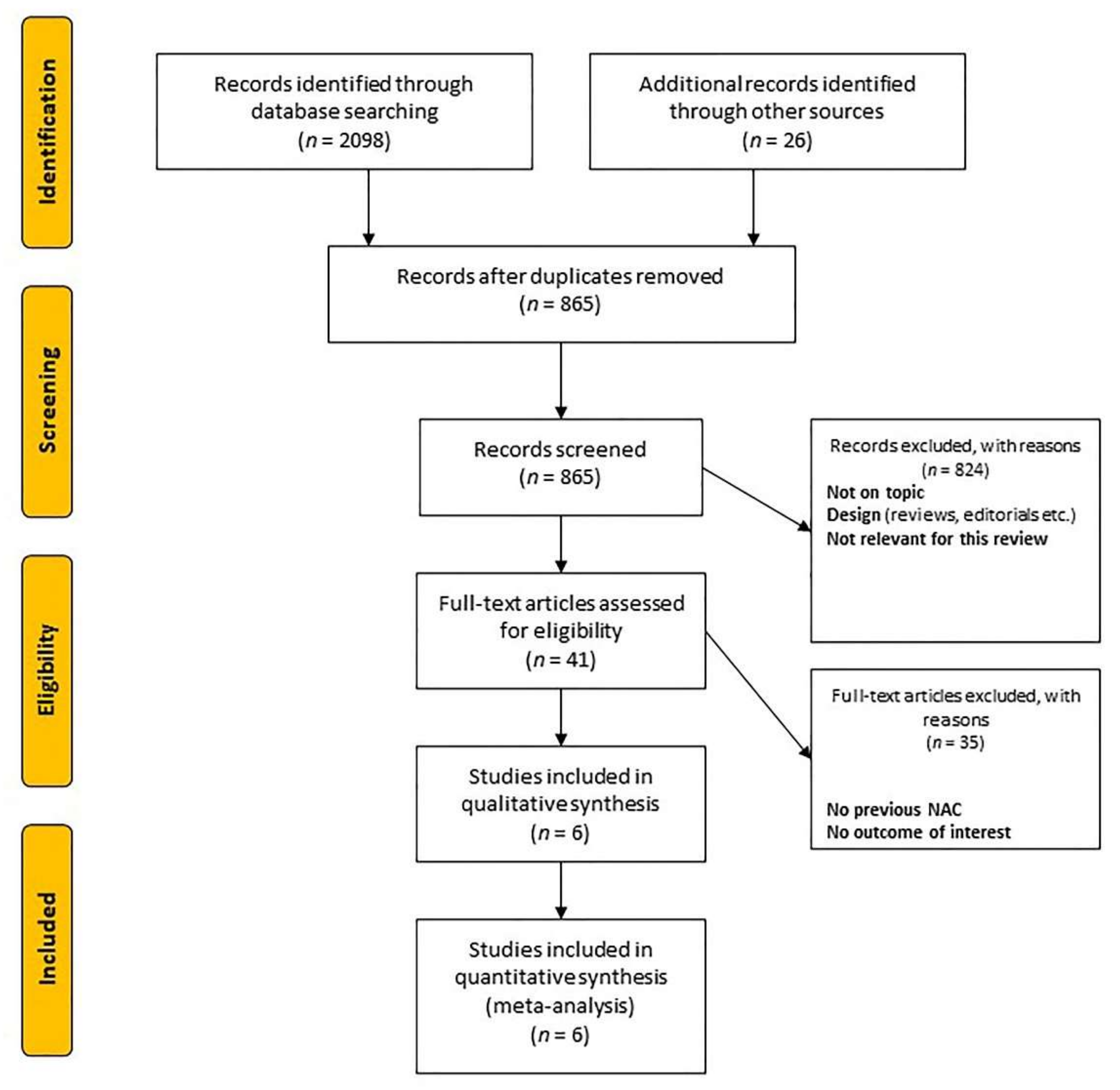
3.1. Study Identification and Quality Assessment
3.2. Clinical Characteristics and Pathological Data
3.3. Risk-of-Bias Assessment
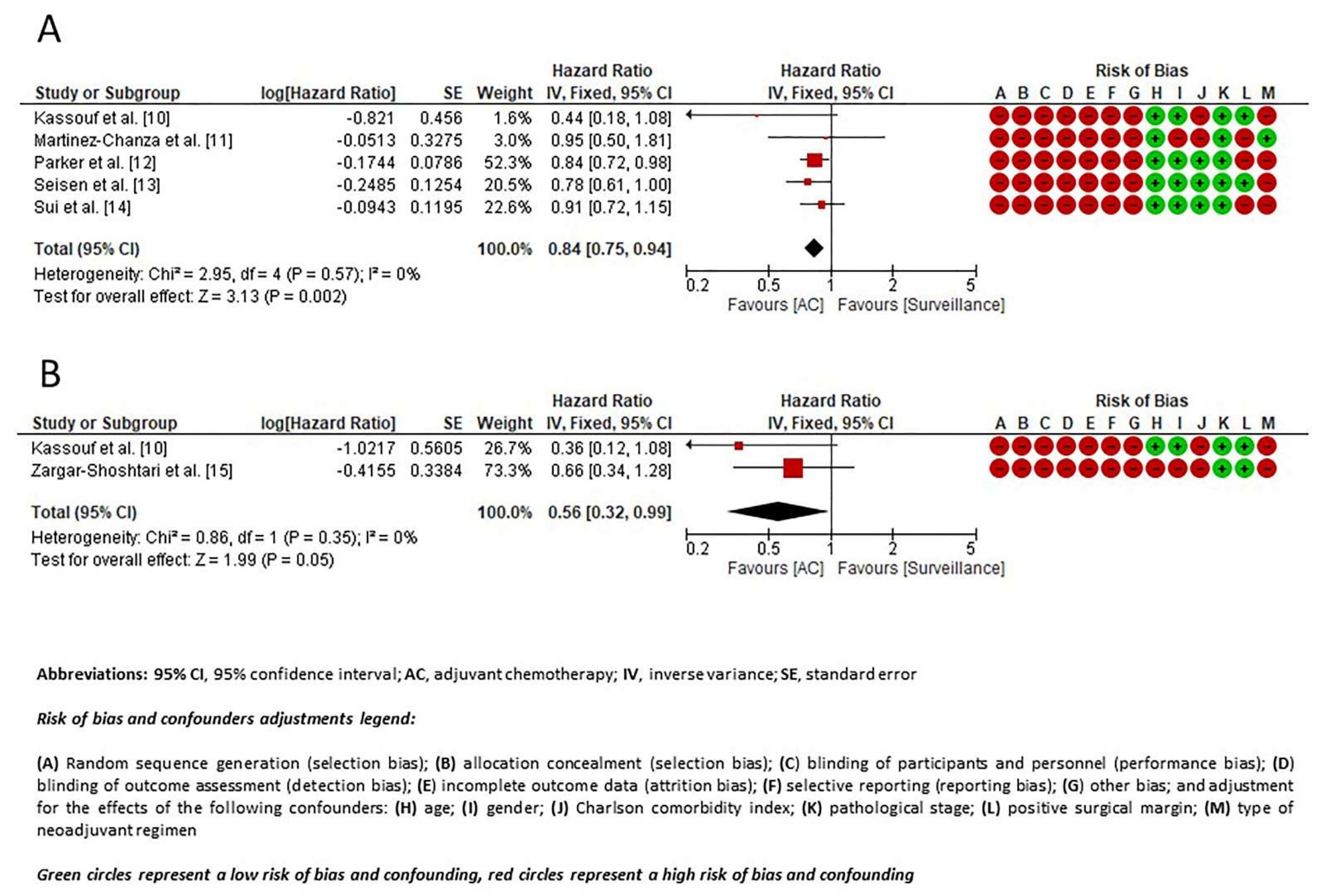
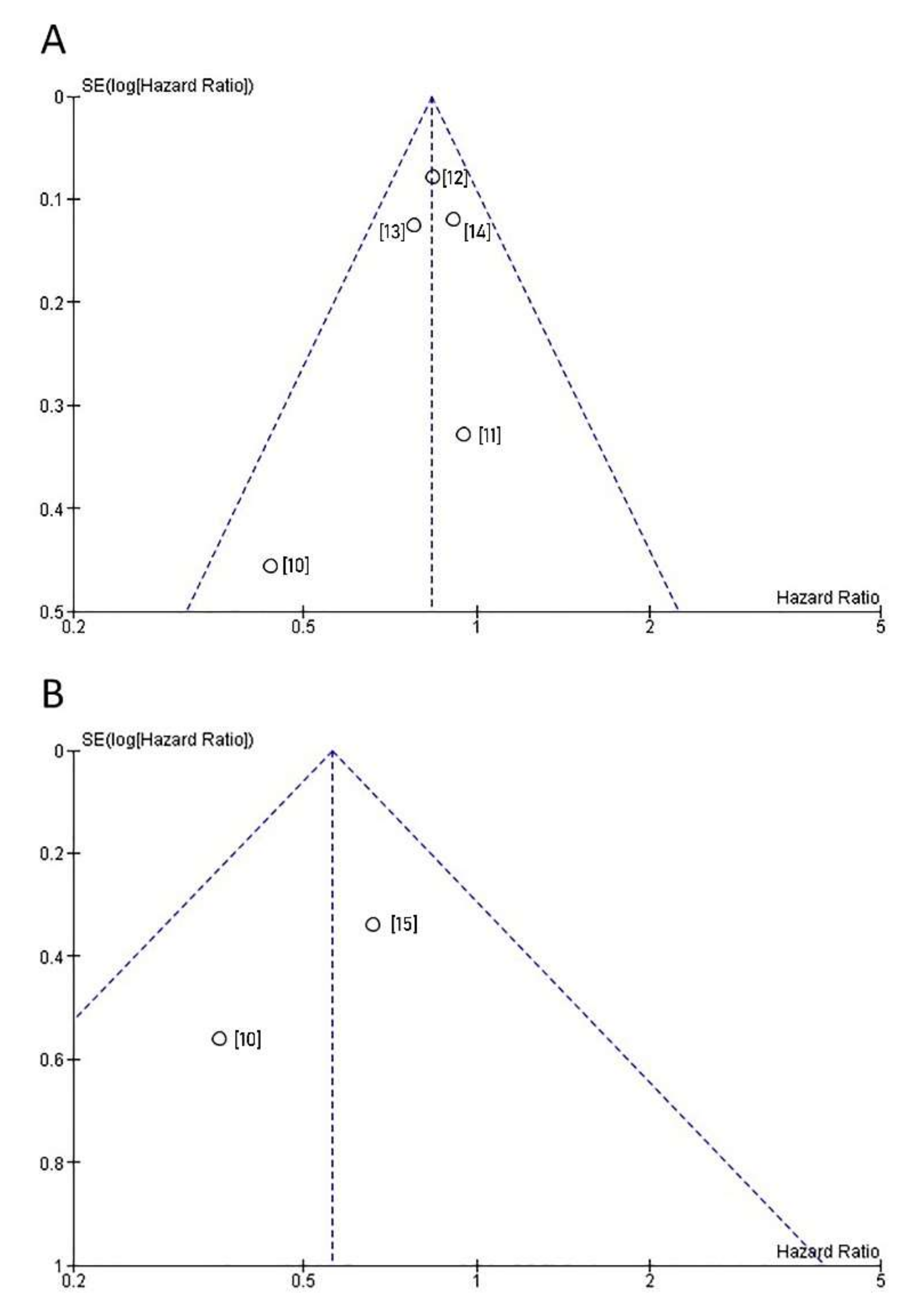
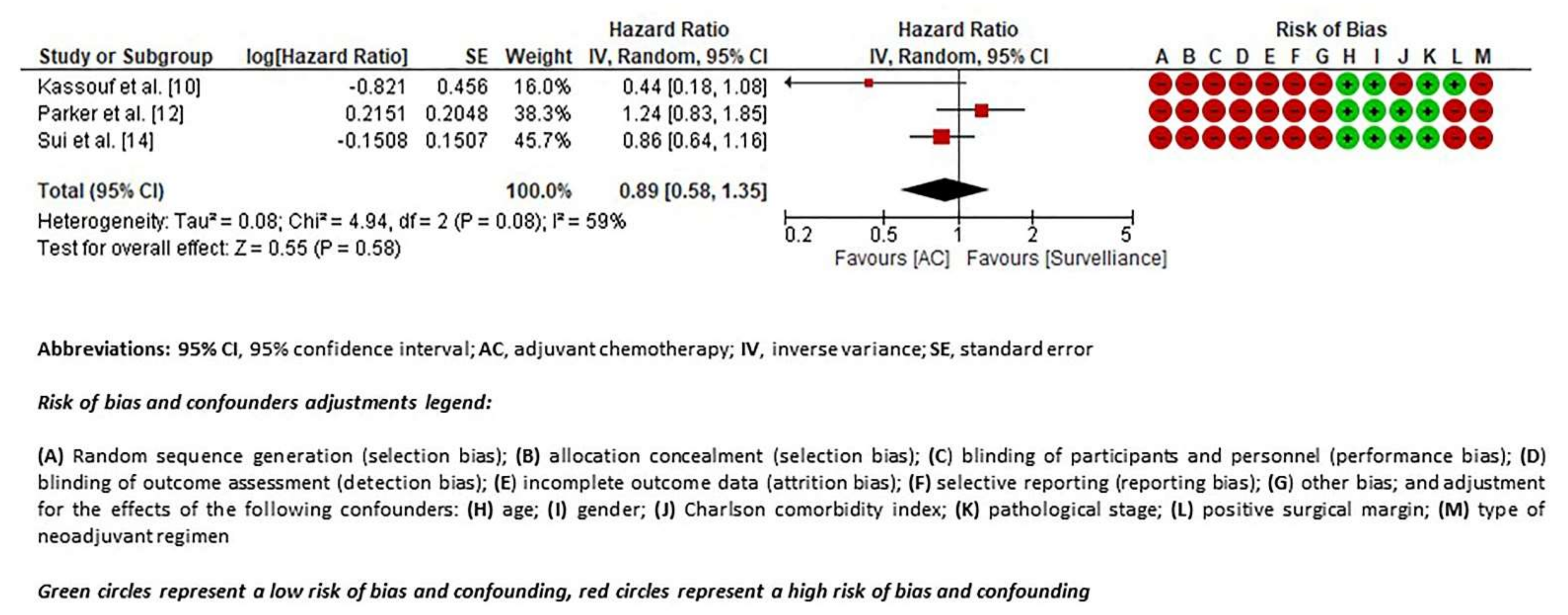
3.4. Meta-Analysis Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Witjes, J.A.; Lebret, T.; Compérat, E.M.; Cowan, N.C.; De Santis, M.; Bruins, H.M.; Hernández, V.; Espinós, E.L.; Dunn, J.; Rouanne, M.; et al. Updated 2016 EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer. Eur. Urol. 2017, 71, 462–475. [Google Scholar] [CrossRef] [PubMed]
- Yin, M.; Joshi, M.; Meijer, R.P.; Glantz, M.; Holder, S.; Harvey, H.A.; Kaag, M.; Van De Putte, E.E.F.; Horenblas, S.; Drabick, J.J. Neoadjuvant Chemotherapy for Muscle-Invasive Bladder Cancer: A Systematic Review and Two-Step Meta-Analysis. Oncol. 2016, 21, 708–715. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manoharan, M.; Katkoori, D.; Kishore, T.A.; Kava, B.; Singal, R.; Soloway, M.S. Outcome after radical cystectomy in patients with clinical T2 bladder cancer in whom neoadjuvant chemotherapy has failed. BJU Int. 2009, 104, 1646–1649. [Google Scholar] [CrossRef] [PubMed]
- Mertens, L.S.; Meijer, R.P.; Meinhardt, W.; Van Der Poel, H.G.; Bex, A.; Kerst, J.M.; Van Der Heijden, M.S.; Bergman, A.M.; Horenblas, S.; Van Rhijn, B.W.G. Occult lymph node metastases in patients with carcinoma invading bladder muscle: Incidence after neoadjuvant chemotherapy and cystectomy vs after cystectomy alone. BJU Int. 2014, 114, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Galsky, M.D.; Stensland, K.D.; Moshier, E.; Sfakianos, J.P.; McBride, R.B.; Tsao, C.-K.; Casey, M.; Boffetta, P.; Oh, W.K.; Mazumdar, M.; et al. Effectiveness of Adjuvant Chemotherapy for Locally Advanced Bladder Cancer. J. Clin. Oncol. 2016, 34, 825–832. [Google Scholar] [CrossRef] [PubMed]
- Leow, J.J.; Martin-Doyle, W.; Rajagopal, P.S.; Patel, C.G.; Anderson, E.M.; Rothman, A.T.; Cote, R.J.; Urun, Y.; Chang, S.L.; Choueiri, T.K.; et al. Adjuvant Chemotherapy for Invasive Bladder Cancer: A 2013 Updated Systematic Review and Meta-Analysis of Randomized Trials. Eur. Urol. 2014, 66, 42–54. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; Prisma Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions version 6.1 (updated September 2020); John Wiley & Sons: Chichester, UK, 2020; Available online: www.training.cochrane.org/handbook (accessed on 1 November 2020).
- Wells, G.; Shea, B.; O’connell, D.; Peterson, J.; Welch, V.; Losos, M.; Tugwell, P. The Newcastle–Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. The Ottawa Hospital Research Institute Clinical Epidemiology Program. 2012. Available online: http://www.ohri.ca/programs/clinical_epidemiology/nosgen.pdf (accessed on 1 November 2020).
- Kassouf, W.; Agarwal, P.K.; Grossman, H.B.; Leibovici, D.; Munsell, M.F.; Siefker-Radtke, A.; Pisters, L.L.; Swanson, D.A.; Dinney, C.P.; Kamat, A.M. Outcome of Patients with Bladder Cancer With pN+ Disease After Preoperative Chemotherapy and Radical Cystectomy. Urology 2009, 73, 147–152. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chanza, N.M.; Werner, L.; Plimack, E.; Yu, E.Y.; Alva, A.S.; Crabb, S.J.; Powles, T.; Rosenberg, J.E.; Baniel, J.; Vaishampayan, U.N.; et al. Incidence, Patterns, and Outcomes with Adjuvant Chemotherapy for Residual Disease After Neoadjuvant Chemotherapy in Muscle-invasive Urinary Tract Cancers. Eur. Urol. Oncol. 2020, 3, 671–679. [Google Scholar] [CrossRef] [Green Version]
- Parker, W.P.; Habermann, E.B.; Day, C.N.; Zaid, H.B.; Frank, I.; Thompson, R.H.; Tollefson, M.K.; Boorjian, S.A.; Pagliaro, L.; Karnes, R.J. Adverse Pathology After Neoadjuvant Chemotherapy and Radical Cystectomy: The Role of Adjuvant Chemotherapy. Clin. Genitourin. Cancer 2018, 16, 64–71. [Google Scholar] [CrossRef]
- Seisen, T.; Jamzadeh, A.; Leow, J.J.; Rouprêt, M.; Cole, A.P.; Lipsitz, S.R.; Kibel, A.S.; Nguyen, P.L.; Sun, M.; Menon, M.; et al. Adjuvant Chemotherapy vs Observation for Patients with Adverse Pathologic Features at Radical Cystectomy Previously Treated with Neoadjuvant Chemotherapy. JAMA Oncol. 2018, 4, 225–229. [Google Scholar] [CrossRef] [PubMed]
- Sui, W.; Lim, E.A.; DeCastro, G.J.; McKiernan, J.M.; Anderson, C.B. Use of Adjuvant Chemotherapy in Patients with Advanced Bladder Cancer after Neoadjuvant Chemotherapy. Bl. Cancer 2017, 3, 181–189. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zargar-Shoshtari, K.; Kongnyuy, M.; Sharma, P.; Fishman, M.N.; Gilbert, S.M.; Poch, M.A.; Pow-Sang, J.M.; Spiess, P.E.; Zhang, J.; Sexton, W.J. Clinical role of additional adjuvant chemotherapy in patients with locally advanced urothelial carcinoma following neoadjuvant chemotherapy and cystectomy. World J. Urol. 2016, 34, 1567–1573. [Google Scholar] [CrossRef] [PubMed]
- Harshman, L.C.; Werner, L.; Wong, Y.-N.; Yu, E.Y.; Alva, A.S.; Crabb, S.J.; Powles, T.; Rosenberg, J.E.; Baniel, J.; Vaishampayan, U.N.; et al. Adjuvant chemotherapy for residual disease after neoadjuvant chemotherapy for muscle invasive urothelial cancer (MIUC). J. Clin. Oncol. 2015, 33, 4524. [Google Scholar] [CrossRef]
- Millikan, R.; Dinney, C.; Swanson, D.; Sweeney, P.; Ro, J.Y.; Smith, T.L.; Williams, D.; Logothetis, C. Integrated Therapy for Locally Advanced Bladder Cancer: Final Report of a Randomized Trial of Cystectomy Plus Adjuvant M-VAC Versus Cystectomy with Both Preoperative and Postoperative M-VAC. J. Clin. Oncol. 2001, 19, 4005–4013. [Google Scholar] [CrossRef] [PubMed]
- Apolo, A.B.; Infante, J.R.; Balmanoukian, A.; Patel, M.R.; Wang, D.; Kelly, K.; Mega, A.E.; Britten, C.D.; Ravaud, A.; Mita, A.C.; et al. Avelumab, an Anti-Programmed Death-Ligand 1 Antibody, In Patients with Refractory Metastatic Urothelial Carcinoma: Results from a Multicenter, Phase Ib Study. J. Clin. Oncol. 2017, 35, 2117–2124. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Wang, Y.; Song, B.; Li, H. Patients’ self-report anxiety, depression and quality of life and their predictive factors in muscle invasive bladder cancer patients receiving adjuvant chemotherapy. Psychol. Health Med. 2019, 25, 190–200. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Country | Design | Duration | Number of Patients AC/Surveillance | Follow Up Median (Months) | Reported Outcomes of Interest | NOS |
|---|---|---|---|---|---|---|---|
| [10] | Canada | Retrospective | 1993–2003 | 11/24 | 50 | OS, DSS | 5 |
| [11] | United States | Retrospective | 1991–2013 | 23/106 | 30 | OS | 7 |
| [12] | United States | Retrospective | 2006–2012 | 326/1033 | 44.4 | OS | 6 |
| [13] | United States | Retrospective | 2006–2012 | 184/604 | 45.7 | OS | 6 |
| [14] | United States | Retrospective | 2004–2013 | 168/537 | 44 | OS | 6 |
| [15] | United States | Retrospective | 2001–2013 | 29/51 | NR | DSS | 6 |
| Study | Group | No. of Patients | Age (Median, IQR) | Gender, Male (%) | CCI, (%) | NAC Regimen, (%) | No. of NAC Cycles (Median, IQR) | Clinical Stage (%) | Pathological Stage (%) | Positive Nodal Status (pN+) (%) | Positive Surgical Margins, (%) | VH, (%) | AC Regimen (%) | No. of AC Cycles (Median, IQR) |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| [10] | AC | 11 | 52 | NA | NR | Platinum-based: 81% Other/unknown: 19% | 5 | NA | NA | 100% | NA | NA | Platinum-based: 73% Other/unknown: 27% | NR |
| Surveillance | 24 | 64 | - | - | ||||||||||
| [11] | AC | 23 | 61 (51–68) | 74% | 0: 39% 1–2: 35% >2: 26% | Cisplatin-based: 64% Carboplatin-based: 21% Other/unknown: 13% | 3 (3–4) | >cT2: 22% cN+: 17% | pT3a–T4a: 17% pT4b and/or pN+: 83% | NA | 17% | 21.7% | Cisplatin-based: 47% Carboplatin-based: 22% Other/unknown: 30% | 4 (3–4) |
| Surveillance | 106 | 66 (59–71) | 71% | 0: 48% 1–2: 25% >2: 25% | Cisplatin-based: 70% Carboplatin-based: 15% Other/unknown: 15% | 3 (3–4) | >cT2: 39% cN+: 16% | pT3a–pT4a: 53% pT4b and/or pN+: 47% | NA | 16% | 21.7% | - | - | |
| [12] | AC | 326 | <60 years: 31.8% ≥60 years: 66.8% | 73.3% | 0: 74.2% 1: 19.6% ≥2: 6.1% | NR | NR | NR | pT3N0: 25.9% pT4N0: 13.7% pTanyN+: 60.4% | 60.4% | NR | NR | NR | NR |
| Surveillance | 1033 | <60 years: 32.1% ≥60 years: 67.9% | 74.7% | 0: 74.4% 1: 20.1% ≥2: 5.4% | NR | NR | NR | pT3N0: 34.8% pT4N0: 11.3% pTanyN+: 53.9% | 53.9% | NR | NR | - | - | |
| [13] * | AC | 184 | mean (SD) 65.7 (10.0) | 75.8% | 0: 75% 1: 20.3% ≥2: 4.7% | NR | NR | NR | pT3N0: 40.8% pT4N0: 13.7% pTanyN+: 45.5% | 45.5% | 17.1% | NR | NR | NR |
| Surveillance | 604 | mean (SD) 65.3 (9.3) | 76.6% | 0: 74.5% 1: 21% ≥2: 5.5% | NR | NR | NR | pT3N0: 39.9% pT4N0: 14.3% pTanyN+: 45.8% | 45.8% | 16.8% | NR | - | - | |
| [14] | AC | 168 | <60 years: 38% ≥60 years: 62% | 67% | 0: 76% 1: 19% ≥2: 5% | NR | NR | NR | ≥pT3: 87% | 57% | NR | NR | NR | NR |
| Surveillance | 537 | <60 years: 33% ≥60 years: 68% | 66% | 0: 74% 1: 20% ≥2: 6% | NR | NR | NR | ≥pT3: 90% | 45% | NR | NR | - | - | |
| [15] | AC | 29 | 66 (56–76) | 83% | median (IQR) 3 (2–4) | Cisplatin-based: 79% Carboplatin-based: 21% Other/unknown: 0% | 3 (3–4) | >cT2: 48% cN+: 20% | pT3–T4: 76% | 83% | 24% | NR | Cisplatin-based: 27.6% Carboplatin-based: 55.2% Other/unknown: 17.2% | 5 (3–8) 4 (2–6) 4 (4–6) |
| Surveillance | 51 | 68 (63–75) | 69% | median (IQR) 3 (2–3) | Cisplatin-based: 74% Carboplatin-based: 26% Other/unknown: 0% | 3 (3–4) | >cT2: 57% cN+: 29% | pT3–T4: 88% | 50% | 34% | NR | - | - |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krajewski, W.; Nowak, Ł.; Moschini, M.; Poletajew, S.; Chorbińska, J.; Necchi, A.; Montorsi, F.; Briganti, A.; Sanchez-Salas, R.; Shariat, S.F.; et al. Impact of Adjuvant Chemotherapy on Survival of Patients with Advanced Residual Disease at Radical Cystectomy following Neoadjuvant Chemotherapy: Systematic Review and Meta-Analysis. J. Clin. Med. 2021, 10, 651. https://doi.org/10.3390/jcm10040651
Krajewski W, Nowak Ł, Moschini M, Poletajew S, Chorbińska J, Necchi A, Montorsi F, Briganti A, Sanchez-Salas R, Shariat SF, et al. Impact of Adjuvant Chemotherapy on Survival of Patients with Advanced Residual Disease at Radical Cystectomy following Neoadjuvant Chemotherapy: Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(4):651. https://doi.org/10.3390/jcm10040651
Chicago/Turabian StyleKrajewski, Wojciech, Łukasz Nowak, Marco Moschini, Sławomir Poletajew, Joanna Chorbińska, Andrea Necchi, Francesco Montorsi, Alberto Briganti, Rafael Sanchez-Salas, Shahrokh F Shariat, and et al. 2021. "Impact of Adjuvant Chemotherapy on Survival of Patients with Advanced Residual Disease at Radical Cystectomy following Neoadjuvant Chemotherapy: Systematic Review and Meta-Analysis" Journal of Clinical Medicine 10, no. 4: 651. https://doi.org/10.3390/jcm10040651