1. Introduction
The clinical management of adolescent concussion has generally relied upon subjective symptom reporting and neuropsychological assessments for determining the recovery status [
1,
2,
3]. Despite the frequent utilization of these clinical assessments, their validity and reliability have been challenged [
4]. Evidence suggests that young adults and adolescents may intentionally minimize self-reported symptom severity [
5,
6,
7,
8]. Post-concussion symptoms appear to be nonspecific, making it difficult for clinicians to identify latent deficits in function that can extend beyond the typical window of recovery, which is approximately four weeks postinjury [
9,
10]. Between 2001–2012, the adolescent age bracket (10–19 years old) was found to have the greatest increase in concussion incidence rate (>140%) compared to any other group [
11]. The period of adolescence marks a critical stage in neurological development, and as such, the underlying maturation process in adolescents may contribute to the higher reported susceptibility to persistent deficits compared to their adult counterparts [
12,
13]. The shortcomings in clinical assessment strategies to formulate recovery prognoses raise concern, as premature return to a sport or academics may expose concussed adolescents to a greater risk of reinjury [
14] or symptom re-emergence [
15]. Thus, more objective markers of the outcome are essential for implementing an appropriate management plan for concussed adolescents.
Heart rate variability (HRV) is a widely used and reliable index of cardio-autonomic function [
16], which has recently emerged as a potential biomarker for monitoring concussion outcomes [
17]. In a resting state, HRV quantifies the intrinsic beat-to-beat variations in heart rate that arise through the Vagus nerve to reflect the inhibitory actions of parasympathetic nervous system function on the sinoatrial node [
18,
19]. The Neurovisceral Integration model proposes an important functional relationship between HRV and the regulation of cognitive and behavioral processes [
20]. Multiple studies indicate HRV can peripherally index top-down activity from the prefrontal neural structures, as HRV modulates as a function of changes in prefrontal activation, as well as behavioral functioning that preferentially activates the prefrontal cortex [
21,
22]. In healthy individuals, greater HRV indicates that the autonomic nervous system (ANS) has sufficient reactivity to regulate physiological systems at rest [
23,
24]. In response to physiological stressors, healthy individuals display a relative degree of vagal withdrawal in order to meet neurometabolic demands, which is followed by a subsequent reduction in HRV [
25,
26]. Deviations in HRV at rest or in response to stress may indicate that dysfunction is present and may result from neurological disorders such as a traumatic brain injury (TBI) [
27,
28]. Preliminary research shows that concussed individuals may demonstrate exaggerated and/or blunted cardio-autonomic activity and reactivity (i.e., abnormal HRV) compared to uninjured controls [
29,
30,
31,
32,
33]. Therefore, alterations to HRV that occur in concussed individuals may also indicate the presence of cognitive and neurobehavioral deficits that could otherwise go undetected with standard clinical assessment approaches, especially in adolescent cases.
Recent evidence has shown that HRV metrics are associated with symptom severity and postinjury deficits in cognitive function following a concussion [
34,
35]. Although promising, the current literature is incomplete and has not yet examined HRV as a predictive marker of the adolescent concussion outcome. Accordingly, our objectives were to (1) examine the associations between subacute resting-state HRV at rest and during a brief physiological stressor and adolescent concussion outcome by evaluating the clinical and depressive symptoms, neurobehavioral function, and cognitive performance and (2) investigate the predictive value of subacute HRV for determining a post-acute outcome. As such, we hypothesized that (1) HRV metrics would be associated with post-concussion outcomes at the subacute evaluation, and (2) subacute HRV metrics would predict a post-acute concussion outcome.
4. Discussion
The purpose of the present study was to investigate the association and value of HRV during rest and physical exertion to predict concussion outcomes in adolescent patients. We found that HRV metrics were associated with clinical symptoms and neurobehavioral function at the subacute evaluation but did not predict the post-acute symptom severity. Furthermore, the HRV indices quantified during this investigation were neither associated with nor predicted depressive symptoms. However, HRV metrics at rest and during a physical exertion task did predict the neurobehavioral regulation and cognitive performance at the post-acute evaluation, suggesting it may be of clinical utility for healthcare providers.
Following concussion, the autonomic nervous system (ANS) and cardiovascular system decouple on multiple levels [
50]. This form of autonomic dysregulation includes sympathetic hyperarousal (e.g., decreased regulation of norepinephrine) and altered hypothalamic–pituitary axis functioning (e.g., increased cortisol). In addition, glucometabolic decoupling in the brain leads to a marked increase in neurometabolic demand following concussion [
51]. The Neurovisceral Integration Model states that HRV serves as a means of quantifying the efficiency of neural communication between higher-order prefrontal structures and physio-regulatory systems (i.e., cardiovascular) [
16,
38]. The authors suggest that dynamic connectivity between such regions is necessary to coordinate behavioral responses to meet the metabolic demand [
52]. Concussion produces a transient loss of functional connectivity in the brain [
53,
54,
55], which perpetuates cardio-autonomic impairment. Cardio-autonomic impairment is commonly reflected by abnormal HRV following a concussive brain injury.
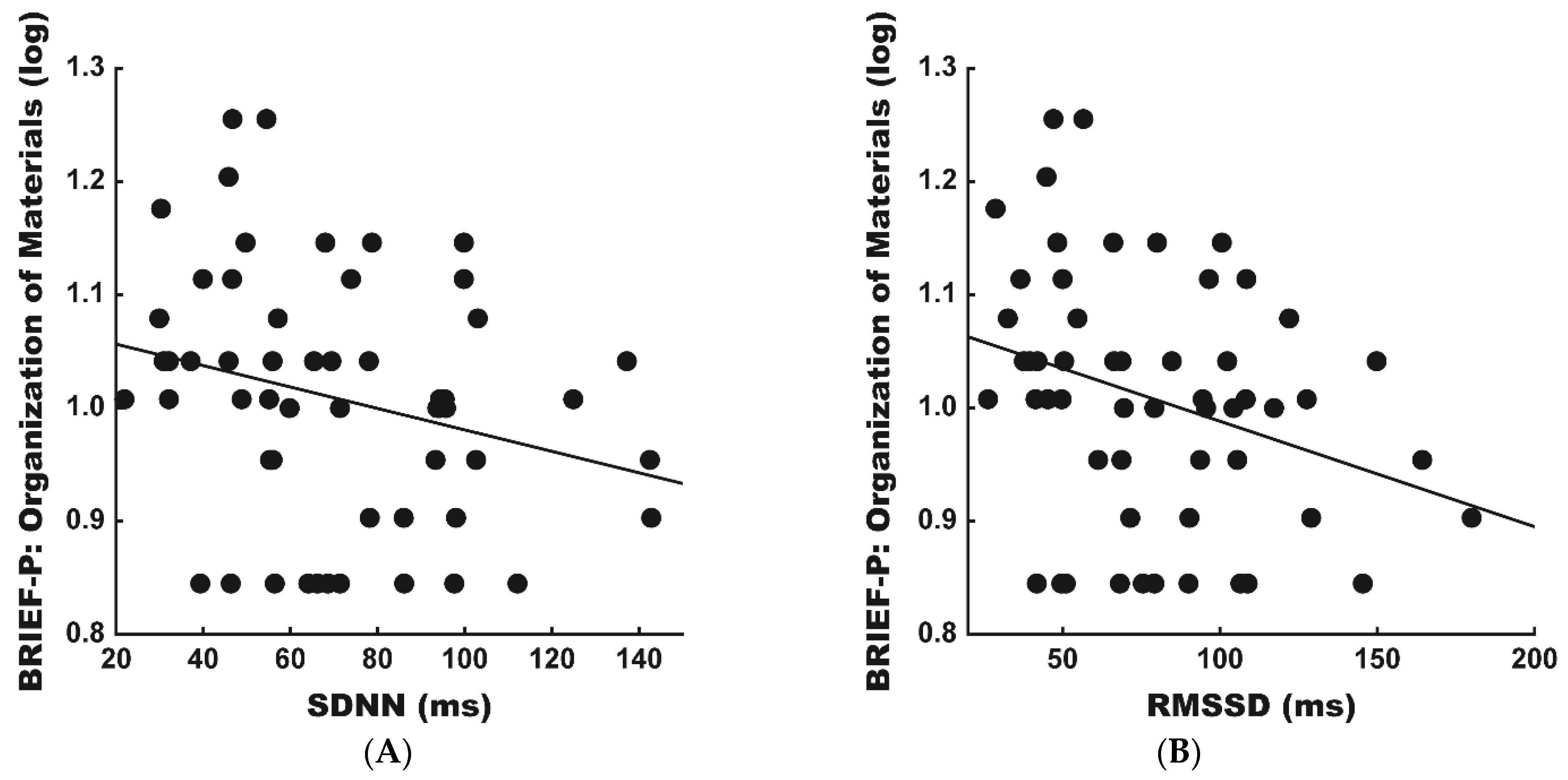
Accordingly, we observed that diminished SDNN and RMSSD were significantly associated with more severe somatic symptomology at the subacute evaluation. Our findings are consistent with observations of attenuated resting-state HRV during the acute and subacute recovery phases, often characterized by the presence of concussion symptoms [
29,
30]. It is hypothesized that the ability to acutely depress the basal metabolic rate following concussion is necessary to foster neuronal rehabilitation [
51,
56]. At rest, the ANS actively engages a vagal “brake” on sympathetic activity to protect the oxygen-dependent central nervous system from costly metabolic reactions [
57]. Therefore, the relationship observed between a greater HRV and lesser severe symptoms could reflect that an early hypometabolic resting state is needed to support recovery following concussive brain injury. However, during the post-acute phase of injury, concussed and non-injured adolescents rarely differ in measures of cardio-autonomic function at rest [
28,
58,
59]. This evidence may explain why associations between subacute HRV and post-acute clinical symptoms were not present in the current study.
In contrast, we did not observe a relationship between the metrics of HRV and depression at either timepoint. This finding was contrary to our hypotheses and prior evidence suggesting that HRV metrics may predict a later onset of depressive symptoms in adult females with a mTBI (mild traumatic brain injury) [
60]. However, prior research examined adults and used the adult version of the Beck Depression Inventory, which contains related but different questions [
61]. It is also worth noting that the menstrual cycle phase at the time of injury has been shown to impact the postinjury symptoms and quality of life at one-month postinjury [
62]. Given the ages of our participants and statistical analyses combining both sexes into the models, the possibility exists that differences within our female participants in the context of menarche, eumenorrhea, and the use of hormone-based contraceptives could have contributed to our lack of similar observations. With further data collections and a larger sample size of females, the analyses may elucidate potential sex-based differences.
In addition, we observed that higher indices of vagal activity were associated with poorer behavioral regulation scores (SDNN and RMSSD) and slower cognitive performance as indexed by correct moves per second on GML (SDNN and RMSSD) at the subacute evaluation. Furthermore, a greater HRV during physical exertion was associated with slower cognitive performance as indexed by the reaction time and reaction time variability on the ONB task at the subacute evaluation (RMSSD). These findings corroborate prior research that observed associations between higher HRV and poorer emotional and cognitive symptoms in concussed adolescents [
35]. Recent literature demonstrates that concussed patients may exhibit an inappropriate increase in vagal tone in response to physiological and cognitive stress compared to healthy controls [
32,
33]. The current theories propose that a failure to suppress the vagal tone may reflect an inability to orient one’s resources toward environmental stressors [
63]. As such, we further observed that greater SDNN and RMSSD during physical exertion predicted a slower cognitive performance on the ONB task at the post-acute evaluation. With the existing literature in mind, these findings may indicate that acutely concussed adolescents with higher HRV may exhibit an inability to adequately withdraw vagal resources in response to stressors. Interestingly, we observed that higher subacute HRV at rest predicted better “external” organization (SDNN and RMSSD) scores at the post-acute evaluation. These contradicting results are perplexing and warrant further investigation into the relationship between HRV at rest and during physical challenges and organizational skills in adolescents.
Beyond traditional HRV variables, we observed consistent associations between HR dispersion and concussion outcomes across the timepoints. We observed that those with greater HR dispersion reported more severe emotional and cognitive symptoms, as well as performed worse on cognitive tasks at the subacute evaluation. Moreover, a greater HR dispersion at rest and during stress predicted a poorer cognitive performance on the GMR and ONB tasks at the post-acute evaluation. These findings corroborate those of Brandt and colleagues, who identified RSA indices as potential predictors of adverse mTBI outcomes [
64].
The preliminary research also suggests that HRV complexity (i.e., ApEn; approximate entropy/SampEn) may be attenuated during the acute, subacute, and post-acute phases of concussion recovery [
40,
65]. Accordingly, we observed that lower SampEn values were significantly associated with poorer neurobehavioral regulation scores and ONB accuracy at the subacute evaluation. Lower subacute SampEn also predicted slower GML performance at the post-acute evaluation, suggesting adolescents with attenuated HRV complexity exhibit persisting neurobehavioral and cognitive dysfunctions. Although, both HR dispersion and SampEn present beneficial values in predicting post-concussion outcomes, their true values as physiological biomarkers for clinicians has yet to be determined.
Together, our results help advance the scientific understanding of the relations between HRV and concussion outcomes. Our results are the first to suggest that HRV may predict neurobehavioral and cognitive outcomes beyond the subacute phase of injury. This is an important point, as prior subacute associations between HRV across domains of functioning have led many researchers and clinicians to suggest that HRV is just a general marker of dysfunction bereft of specificity and predictive power. However, our results point to a specific predictive value of HRV to post-acute neurobehavioral functions and cognitive functions independent of symptom questionnaires. Thus, HRV may be a simple and effective way for clinicians to identify patients who are likely to experience persisting alterations in neurobehavioral functioning and cognition. This would provide clinicians the opportunity to preemptively change management strategies to maximize the positive outcomes.
Although the current results serve to provide a specific relation between HRV and concussion outcomes, the present study is not without limitations. First, although age was adjusted for in our regression analyses, our results may not fully account for individual differences in physiological maturity among this sample of adolescents. The current findings also cannot inform us regarding the differences in female populations across estrous cycles or across birth control types. Although both sexes were represented in the current study, menarche, estrous phase, and hormonal contraceptives can influence HRV. Furthermore, as this study was conducted in a clinic and not a laboratory, we cannot determine the central mechanisms (biochemical and psychophysiological) that mediate the relation between HRV metrics and functional outcomes. Additionally, as the preinjury baseline measures were not captured, the current study cannot tell us how these relations may change as a function of sport and sub-concussive impacts, which affect the neuronal integrity centrally and peripherally. Furthermore, while we controlled for the BMI and physical activity level, we did not have objective measures of cardiorespiratory fitness, which may influence the resting HR and HRV. Thus, additional research is still needed from a scientific and clinical perspective to determine the predictive value of HRV across different populations and demographic factors.

 ,
, 



{kind=link}
{kind=link}