
P2Y12 Inhibitor Monotherapy after Percutaneous Coronary Intervention

1
Division of Cardiology, University of Florida College of Medicine, Jacksonville, FL 32209, USA
2
Department of Internal Medicine, University of Alabama at Birmingham Montgomery, Montgomery, AL 36116, USA
*
Author to whom correspondence should be addressed.
J. Cardiovasc. Dev. Dis. 2022, 9(10), 340; https://doi.org/10.3390/jcdd9100340
Submission received: 11 September 2022
/
Revised: 5 October 2022
/
Accepted: 5 October 2022
/
Published: 6 October 2022
(This article belongs to the Special Issue New Insights into Antithrombotic Therapy for Cardio- and Cerebrovascular Disease: From Molecular Mechanisms to Clinical Application)
Abstract
:In patients with acute and chronic coronary artery disease undergoing percutaneous coronary intervention (PCI), dual antiplatelet therapy (DAPT) has been the cornerstone of pharmacotherapy for the past two decades. Although its antithrombotic benefit is well established, DAPT is associated with an increased risk of bleeding, which is independently associated with poor prognosis. The improvement of the safety profiles of drug-eluting stents has been critical in investigating and implementing shorter DAPT regimens. The introduction into clinical practice of newer generation oral P2Y12 inhibitors such as prasugrel and ticagrelor, which provide more potent and predictable platelet inhibition, has questioned the paradigm of standard DAPT durations after coronary stenting. Over the last five years, several trials have assessed the safety and efficacy of P2Y12 inhibitor monotherapy after a short course of DAPT in patients treated with PCI. Moreover, ongoing studies are testing the role of P2Y12 inhibitor monotherapy immediately after PCI in selected patients. In this review, we provide up-to-date evidence on the efficacy and safety of P2Y12 inhibitor monotherapy after a short period of DAPT compared to DAPT in patients undergoing PCI as well as outcomes associated with P2Y12 inhibitor monotherapy compared to aspirin for long-term prevention.
1. Introduction
Percutaneous coronary intervention (PCI) with stent implantation has emerged as the predominant revascularization strategy in patients with obstructive coronary artery disease (CAD) [1,2,3]. After PCI, antiplatelet therapy plays a pivotal role in preventing stent-related complications such as stent thrombosis and secondary prevention for non-stent-related ischemic events such as myocardial infarction (MI) and stroke [4,5,6]. The combination of aspirin and an oral P2Y12 receptor inhibitor, known as dual antiplatelet therapy (DAPT), has become the guideline-recommended standard strategy after PCI based on data derived from more than 35 randomized clinical trials (RCTs) [1,2,7,8,9,10].
Clopidogrel is the most prescribed oral P2Y12 inhibitor [11]. In particular, clopidogrel is the only guideline recommended P2Y12 inhibitor after PCI in patients with chronic coronary syndromes (CCS) [1,2,7,8]. However, clopidogrel is a prodrug that requires hepatic cytochrome P450 2C19 (CYP2C19) metabolism to its active form, which leads to high variability in its pharmacodynamic (PD) effects [12,13]. Importantly, patients who persist with high platelet reactivity (HPR) while on clopidogrel are at increased risk of thrombotic events after PCI [14]. Indeed, patients with acute coronary syndromes (ACS) are at increased risk for HPR. Thus, the newer generation P2Y12 inhibitors prasugrel and ticagrelor characterized by potent and predictable antiplatelet effects are preferred over clopidogrel as the standard of care in patients with ACS [1,2,9,15].
Even though the efficacy of DAPT is well established, it is also associated with an unavoidable increased risk of bleeding, which is associated with poor outcomes, including increased mortality [16]. Several investigations have led to defining the phenotype of patients more prone to bleeding, setting the foundation for introducing the high bleeding risk (HBR) concept [17]. In 2019, the Academic Research Consortium (ARC) formally defined HBR patients as those who are at risk of ≥4% of having type 3 or 5 bleeding according to the bleeding academic research consortium (BARC) or ≥1% of intracranial hemorrhage (ICH), both at 1 year [18]. Moreover, the ARC-HBR proposed a diagnostic criterion based on clinical and laboratory characteristics that has been classified into major and minor criteria, the presence of 1 major or 2 minor criteria are needed to fulfil the HBR definition.
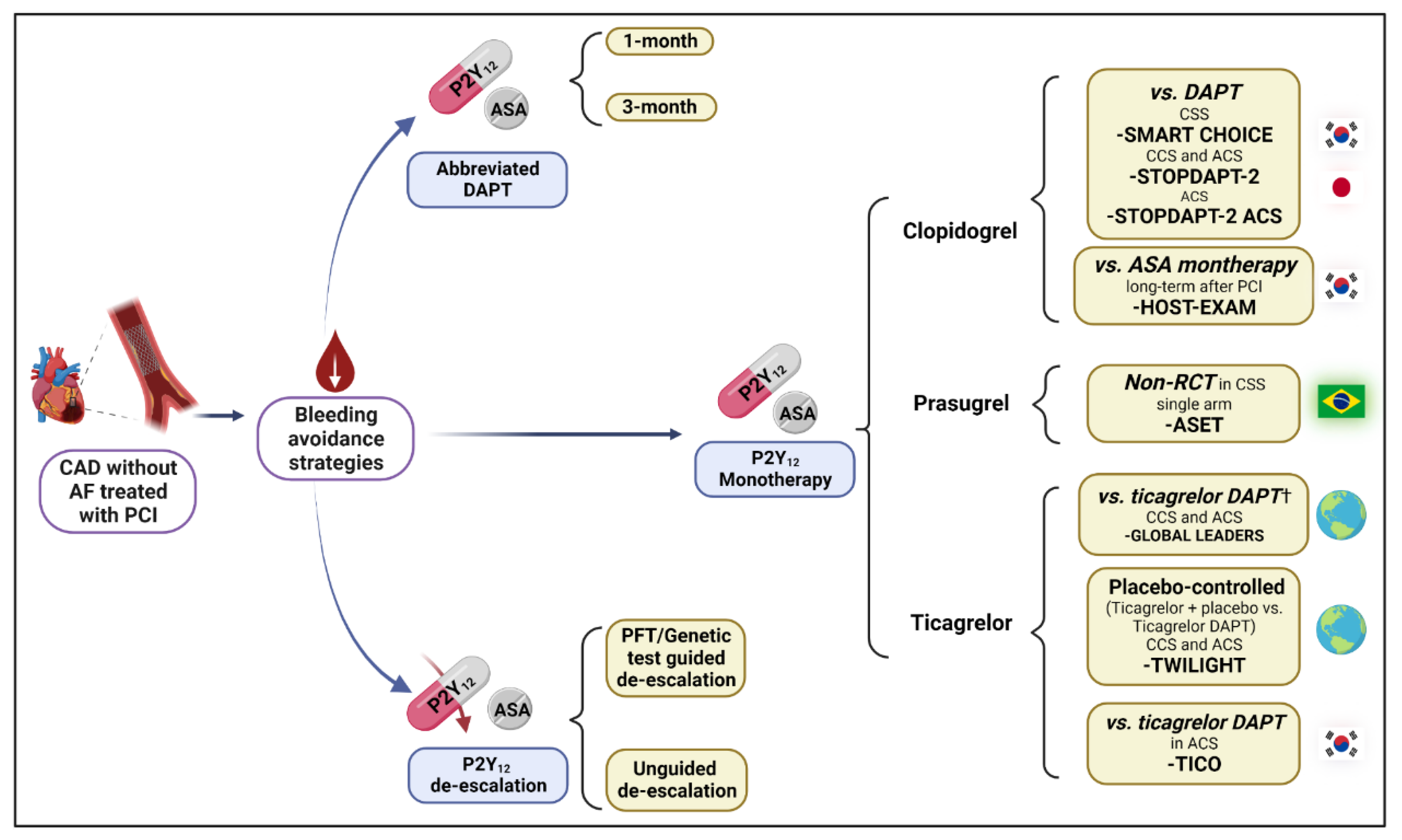
Overall, these observations have prompted investigations evaluating “bleeding avoidance strategies” for patients undergoing PCI. The goal of these approaches is to minimize bleeding risk while preserving efficacy. Bleeding reduction strategies are directed to optimize the choice, duration, and modulation of DAPT (Figure 1). Amongst these, the strategy of discontinuation of aspirin after a short period of DAPT and maintaining P2Y12 inhibitor monotherapy has been a subject of extensive investigation. This strategy was first investigated in patients requiring concomitant use of an oral anticoagulant agent. The details of this approach go beyond the scope of this manuscript and are described elsewhere [19,20]. In this manuscript, we provide an overview of P2Y12 inhibitor monotherapy after a short course of DAPT in patients undergoing PCI without an indication of anticoagulation as well as the impact of P2Y12 inhibitor monotherapy compared to aspirin for long term secondary prevention in patients with CCS.
2. Rationale for P2Y12 Inhibitor Monotherapy
Platelet activation is a complex biological mechanism involving multiple activating factors such as thromboxane A2 and adenosine diphosphate (ADP), which represent the targets of aspirin and P2Y12 inhibitors, respectively [21]. Aspirin irreversibly blocks cyclooxygenase-1 (COX-1), the key enzyme in the arachidonic acid pathway of thromboxane A2 generation. On the other hand, P2Y12 inhibitors prevent ADP-mediated platelet activation by receptor blocking effect [22]. The exact mechanism can vary according to the type of drug. Clopidogrel and prasugrel (thienopyridines) require conversion to an active metabolite and mediate irreversible inhibition. Meanwhile, ticagrelor (nonthienopyridine) is a direct and reversible receptor antagonist [13]. Prasugrel and ticagrelor provide more potent and predictable platelet inhibition compared to clopidogrel [23,24]. These better PD profiles of prasugrel and ticagrelor compared to clopidogrel translate into lower ischemic/thrombotic events in pivotal RCTs, at the expense of increased bleeding events [25,26]. All these pivotal investigations have been performed on a background of aspirin therapy, under the notion that aspirin and P2Y12 inhibitors (mainly demonstrated with clopidogrel) have synergetic effects on platelet inhibition, representing the foundation for the use of DAPT [27,28].
Although DAPT has remained the standardized therapy after PCI, the usage and duration of aspirin have been challenged based on three major arguments. First, the synergism between aspirin and P2Y12 inhibitors was mainly established by early studies on aspirin with clopidogrel [28]. In the presence of potent P2Y12 blockade, in vitro pharmacodynamic investigations have shown that aspirin does not provide much additional antiplatelet effect [29]. This was also confirmed in a series of ex vivo pharmacodynamic studies [30,31,32]. While withdrawal of aspirin indeed eliminates its specific inhibitory effects mediated by the COX-1 pathway, other platelet signaling pathways are still affected by potent P2Y12 blockade [20,33]. Second, aspirin is associated with gastrointestinal (GI) adverse effects, from mild dyspepsia to ulceration and GI bleeding [34]. Systemically, aspirin irreversibly and non-selectively inhibits COX enzyme, leads to systemic prostaglandin depletion that compromises gastric mucosal barrier function and increases acid secretion [34]. Locally, aspirin may reduce surface hydrophobicity and destabilize the phospholipid barrier, which makes the mucosa susceptible to direct injury by gastric acid [35]. Although several approaches are used to mitigate aspirin gastric injury (i.e., consumption with food, proton pump inhibitors, and new aspirin formulations), the most effective way to reduce aspirin GI effects is by minimizing aspirin treatment duration [36]. Third, the introduction of newer drug-eluting stents has markedly decreased the rate of stent thrombosis, and the widespread usage of lipid-lowering therapies has further reduced the incidence of MI unrelated to the stent, which was assumed to be in part driven by the beneficial effects of DAPT [37].
3. Current Evidence of P2Y12 Inhibitor Monotherapy
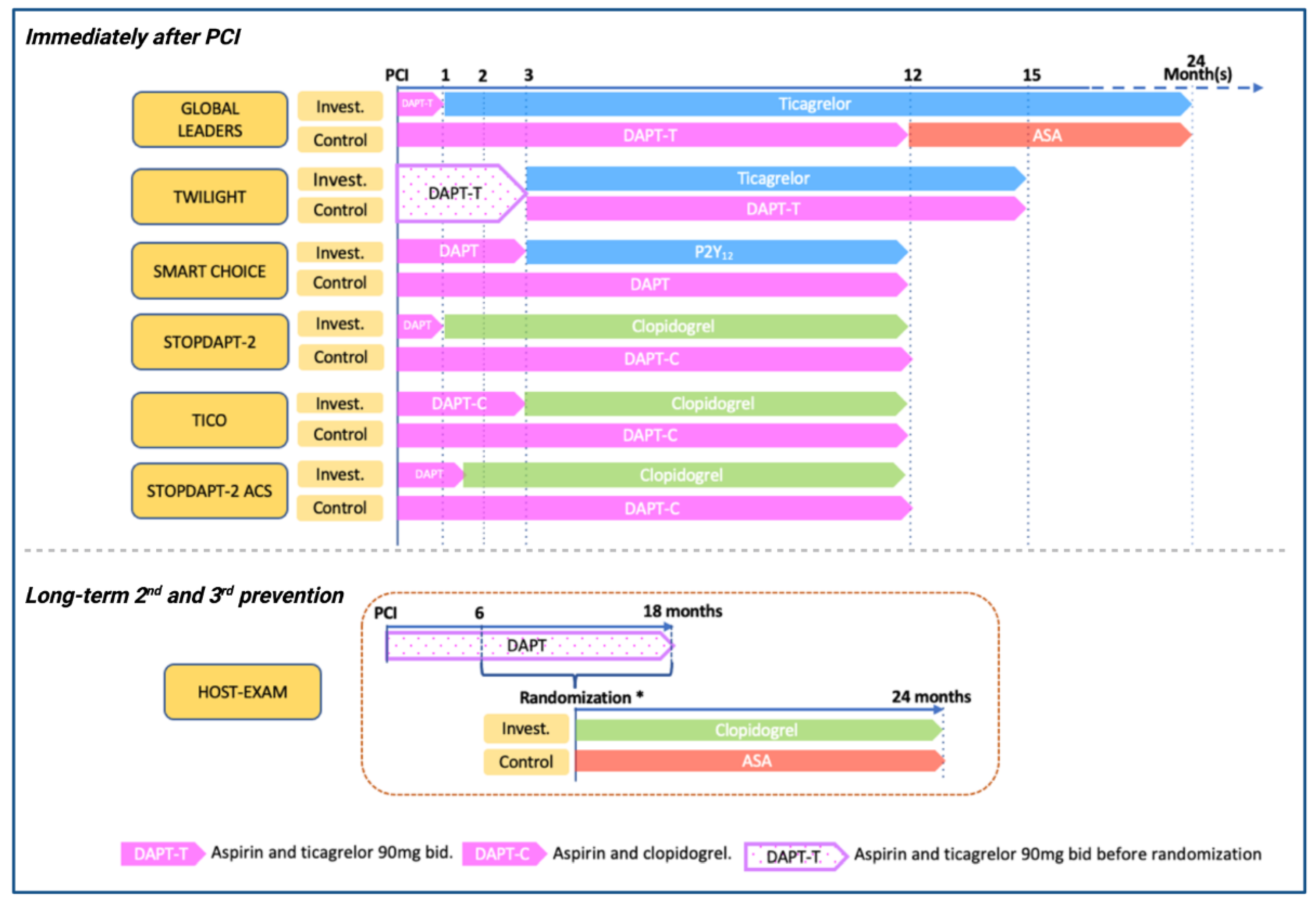
Over the last years, several large-scale RCTs have assessed the safety and efficacy of aspirin-free antiplatelet strategies after coronary stenting (Figure 2 and Table 1). Two main approaches have been assessed: (a) trials comparing P2Y12 monotherapy versus conventional DAPT regimens after PCI and (b) trials comparing P2Y12 inhibitors vs aspirin monotherapy for long-term secondary prevention.
4. P2Y12 Monotherapy versus DAPT after PCI
4.1. Clopidogrel
SMART-CHOICE (Comparison Between P2Y12 Antagonist Monotherapy vs Dual Antiplatelet Therapy in Patients Undergoing Implantation of Coronary Drug-Eluting Stents) was an open-label RCT comparing 3-month DAPT followed by P2Y12 inhibitor monotherapy vs. standard 12-month DAPT after PCI in terms of major adverse cardiac and cerebrovascular events (MACCE) in a non-inferiority analysis [38]. A total of 2993 patients were enrolled. There were no restrictions on the type of P2Y12 inhibitor or clinical presentation. The P2Y12 inhibitor monotherapy was noninferior compared to DAPT in MACCE (Hazard ratio [HR], 1.19; 95% Confidence interval [CI], [−∞%–1.3%]; pnoninferiority = 0.007). There were no significant differences in the primary endpoint components, but there was a significantly lower BARC 2–5 bleeding rate in the P2Y12 inhibitor monotherapy than the DAPT group (HR, 0.58; 95%CI [0.36–0.92]; p = 0.020).
Two main post-hoc analyses have been reported. First, the clopidogrel–only cohort (80% of the total sample size), there were no significant differences between clopidogrel monotherapy versus clopidogrel–based DAPT in MACCE (HR, 1.02; 95%CI, [0.64–1.65]; p = 0.100) and BARC 2–5 bleeding (HR, 0.71; 95%CI, [0.42–1.21]; p = 0.150) [39]. Second, in the platelet reactivity sub-study (n = 833), 108 (13.0%) patients had HPR who had a significantly increased risk of MACCE compared to those without HPR (8.7% vs. 1.5%; HR, 3.03; 95%CI, [1.06–8.69]; p = 0.038) [40]. However, the treatment effect of clopidogrel monotherapy for the 12-month MACCE was not significantly different compared with DAPT in patients with HPR or without HPR (HR, 0.71; 95%CI, [0.18–2.73]; p = 0.628 and HR, 2.58; 95%CI, [0.68–9.77]; p = 0.161; pinteraction = 0.170). These results suggest that the main driver of adverse events was the HPR status rather than the allocated treatment, denoting the importance of optimizing platelet inhibition [41].
STOPDAPT-2 (Short and Optimal Duration of Dual Antiplatelet Therapy After Everolimus-Eluting Cobalt–Chromium Stent) was a prospective, open-labeled RCT comparing 1 month of DAPT (clopidogrel or prasugrel 3.75 mg od) followed by clopidogrel monotherapy versus 12 months DAPT with aspirin and clopidogrel in patients who underwent PCI [42]. A total of 3045 participants were recruited. The primary endpoint was a composite of ischemic (cardiovascular death, MI, stroke, or stent thrombosis) and bleeding endpoints (Thrombolysis in Myocardial Infarction [TIMI] major or minor bleeding) at 12 months. Clopidogrel monotherapy group met the prespecified criteria for noninferiority and superiority compared to the standard DAPT (HR, 0.64; 95%CI, [0.42–0.98]; p < 0.001 for noninferiority, p = 0.04 for superiority). There was no difference in the ischemic endpoints (HR, 0.79; 95%CI, [0.49–1.29]; p = 0.340), but there was a significant lower bleeding rate in the clopidogrel monotherapy than 12 months of DAPT (HR, 0.26; 95%CI, [0.11–0.64]; p = 0.004).
STOPDAPT-2 ACS (Short and Optimal Duration of Dual Antiplatelet Therapy-2 Study for the Patients With ACS) trial was a prospective, open-label RCT with the same design as the STOPDAPT-2, but including only patients with ACS, the ACS cohorts of both trials were combined (3008 newly enrolled and 1161 pooled form previous trial, in total 4169 patients were randomized) [43]. At the 1-year follow-up, 1–2 months DAPT (aspirin and clopidogrel) followed by clopidogrel monotherapy failed to meet the noninferior criteria compared to the 12-month DAPT (HR, 1.44; 95%CI, [0.80–1.62]; pnoninferiority = 0.06). The rate of major bleeding was significantly lower in the monotherapy group compared to the DAPT (HR, 0.46; 95%CI, [0.23–0.94]; p = 0.03). However, there was a significant increase in MI in the monotherapy group compared to the DAPT group (HR, 1.91; 95%CI, [1.06–3.44]; p = 0.03). The underlying reasons for which there was an increased risk of adverse events in the ACS cohort in patients treated with monotherapy compared to standard DAPT remains unclear but may be likely attributed to the presence of HPR among patients treated with clopidogrel only and no added antiplatelet effect given the withdrawal of aspirin.
STOPDAPT-2 Total Cohort the STOPDAPT investigators performed a prespecified pooled STOPDAPT-2 and STOPDAPT-2-ACS (n = 5997 in total), the rationale for this pooled analysis was that in both trials there had a lower-than-expected event rate that could affect the trials results [44]. The authors followed the same methodology and endpoints as in the main trials. One-month DAPT was noninferior but not superior to 12-month DAPT for the primary endpoint (HR, 0.94; 95%CI, [0.70–1.27]; pnoninferiority = 0.001 and psuperiority = 0.68). There was no significant risk-difference for the cardiovascular endpoint between groups (HR, 1.24; 95% CI, [0.88–1.75]; p = 0.23), but one-month DAPT was associated with a lower risk of the bleeding than 12-month DAPT (HR, 0.38 95%CI, [0.21–0.70]; p = 0.002). When the results were analyzed according to clinical presentation (ACS vs. CCS), one-month DAPT was associated with a lower risk for major bleeding than 12-month DAPT in ACS or CCS patients (HR, 0.46; 95%CI, [0.23–0.94]; p = 0.03. and HR, 0.26; 95%CI, [0.09–0.79]; p = 0.02; pinteraction = 0.40), but there was a numerical increase in cardiovascular events in ACS patients, but not in CCS patients (HR, 1.50; 95%CI, [0.99–2.27]; p = 0.053, and HR, 0.74; 95%CI, [0.38–1.45]; p = 0.39; pinteraction = 0.08).
4.2. Prasugrel
ASET (Acetyl Salicylic Elimination Trial) was a pilot, prospective, open-label, single-arm non-randomized study assessing the safety of prasugrel monotherapy in patients with CCS. All participants (n = 201) were on standard DAPT at the time of the index PCI, after successful PCI with platinum-chromium everolimus-eluting stent (Pt-EES), aspirin was discontinued and prasugrel was loaded and maintained for 3 months [45]. The primary ischemic endpoint was the composite of cardiac death, spontaneous target vessel MI, or definite stent thrombosis. The primary bleeding endpoint was major bleeding. There was only one event (cardiac death following intracranial bleeding). The compelling results of the ASET trial should be interpreted in the light of its small and very selected population and low lesion complexity.
4.3. Ticagrelor
GLOBAL LEADERS (A Clinical Study Comparing Two Forms of Antiplatelet Therapy After Stent Implantation) trial was a prospective, open-label RCT. Patients were randomized after successful PCI with a biolimus A9-eluting stent to either aspirin plus 90 mg ticagrelor twice daily for 1 month, followed by 23 months of ticagrelor monotherapy (90 mg, twice daily) or standard DAPT with clopidogrel (for patients with stable CAD) or ticagrelor (for patients with ACS) for 12 months, followed by aspirin monotherapy for another 12 months. A total of 15,968 patients were enrolled. The primary efficacy endpoint was all-cause death or non-fatal new Q-wave MI, and the primary safety endpoint was major bleeding, defined as BARC 3 or 5 bleeding. At 2 years, ticagrelor monotherapy was not superior to standard DAPT for reducing the primary efficacy (RR, 0.87; 95%CI, [0.75–1.01]; p = 0.073) or safety endpoints (RR, 0.97; 95%CI, [0.78–1.20]; p = 0.770). The adherence rate at two years was 77.6% in the experimental group and 93.1% in the control group, consistent with the premature ticagrelor discontinuation rate (25%) observed in other studies and mainly related to adverse events such as bleeding and dyspnea [46,47].
One of the main limitations of the GLOBAL LEADERS trial was the lack of independent event adjudication. Therefore, the prespecified GLASSY (GLOBAL LEADERS Adjudication Sub-Study) study was conducted following the same methodology as the main trial [48]. The study included approximately 47% of the main trial sample size enrolled in the top 20 enrolling sites. At 2 years, ticagrelor monotherapy was noninferior but not superior to standard 12 months DAPT for reducing the primary efficacy endpoint (RR, 0.85; 95%CI, [0.72–0.99]; pnoninferiority < 0.001 and psuperiority = 0.046 at alpha of 2.5%). There were no significant differences between groups in major bleeding regardless of the definition.
The prespecified [49,50,51,52,53,54,55,56] and selected post-hoc analyses [57,58,59,60,61] performed by the GLOBAL LEADERS investigators for exploring the effect size of the intervention on different subgroups are shown in Table S1.
TWILIGHT (Ticagrelor with Aspirin or Alone in High-Risk Patients after Coronary Intervention) was prospective, double-blind, placebo-controlled RCT that compared ticagrelor plus placebo vs. ticagrelor-based DAPT in event-free and high-risk PCI patients who completed 3 months of DAPT with aspirin and ticagrelor [62]. The primary endpoint was defined as clinically relevant bleeding (BARC 2, 3, or 5). The key secondary endpoint was the composite of all-cause death, nonfatal MI, or nonfatal stroke. A total of 7119 patient were randomized. At 1 year, the incidence of clinically relevant bleeding was significantly lower in the ticagrelor monotherapy group than in the ticagrelor-based DAPT group (HR, 0.56; 95%CI, [0.45–0.68]; p < 0.001). The secondary endpoint of BARC type 3 or 5 bleeding was also significantly less in the ticagrelor monotherapy group (HR, 0.49; 95%CI, [0.33–0.74]; p < 0.001). In the key secondary ischemic composite endpoint, ticagrelor monotherapy was non-inferior to ticagrelor-based DAPT group (HR, 0.99; 95%CI, [0.78–1.24]; pnoninferiority < 0.001).
The main results of the TWILIGHT trial have been shown to be consistent in several subgroup analyses such as age [63], gender [64], East Asian ethnicity [65], DM status [66], CKD status [67], prior MI [68], clinical presentation [69], stent used [70], and HBR status [71]. Overall, all indicate a reduced risk of clinically relevant bleeding and without a significant increase in ischemic events. A complete list of the prespecified and post-hoc analyses performed by the TWILIGHT investigators are shown in Table S2.
TICO (Ticagrelor Monotherapy After 3 Months in the Patients Treated With New Generation Sirolimus-eluting Stent for Acute Coronary Syndrome) trial was prospective, open-label RCT comparing ticagrelor monotherapy after 3 months of DAPT versus ticagrelor-based DAPT for 12 months in patients with ACS treated with PCI [72]. The primary outcome was a net adverse clinical event (NACE, composite of MACCE [composite of all-cause death, MI, stent thrombosis, stroke, or target vessel revascularization] and TIMI major bleeding). A total of 3056 patients were randomized. At 1 year, ticagrelor monotherapy significantly reduced NACE compared to ticagrelor-based DAPT (HR, 0.66; 95%CI, [0.48–0.92]; p = 0.01). There was significant reduction in major bleeding between two groups (HR, 0.56; 95%CI, [0.34–0.91]; p = 0.02), but not in MACCE (HR, 0.69; 95%CI, [0.45–1.06]; p = 0.09).
The main results of the TICO trial have been shown to be consistent in several subgroup analyses such as DM status [73], high-ischemic risk [74], ST-segment elevation myocardial infarction (STEMI) [75], and HBR status [76]. A complete list of the prespecified and post-hoc analyses performed by the TICO investigators are shown in Table S3.
4.4. Meta-Analysis
Several meta-analyses have been reported. However, the most comprehensive data reported are the individual patient data metanalysis by Valgimigli et al. [77]. In total, 24,096 patients from the GLASSY, SMART-CHOICE, STOPDAPT-2, TICO, and TWILIGHT trials were included. The primary efficacy endpoint was defined as a composite of all-cause death, MI, and stroke, and the key safety endpoint was major bleeding (BARC type 3 or 5). In the intention-treat analysis, P2Y12 monotherapy was non-inferior but not superior to DAPT for the primary endpoint (HR, 0.93; 95%CI, [0.79–1.09]; p = 0.005 for noninferiority; p = 0.380). The bleeding risk was significantly lower with P2Y12 inhibitor monotherapy than DAPT (HR, 0.49; 95%CI, [0.39–0.63]; p < 0.001). In the subgroup analysis, there was a significant interaction of sex in the effect size of P2Y12 monotherapy and DAPT, there was a significant reduction in the primary endpoint in women but not in men (HR, 0.64; 95%CI, [0.46–0.89] and HR, 1.00; 95%CI, [0.83–1.19]; pinteraction = 0.02). The interaction was mainly driven by a reduction of cardiovascular mortality in women but not in men (HR, 0.31; 95%CI, [0.15–0.65] and HR, 0.86; 95%CI, [0.59–1.25]; pinteraction = 0.02). Furthermore, there was no significant interaction of the type of P2Y12 inhibitor (clopidogrel vs. newer P2Y12 inhibitor [mainly ticagrelor]) in the primary endpoint (HR, 0.94; 95%CI, [0.66–1.33] and HR, 0.89; 95%CI, [0.75–1.06]; pinteraction = 0.16) or major bleeding (HR, 0.60; 95%CI, [0.34–1.06] and HR, 0.47; 95%CI, [0.36–0.62]; pinteraction = 0.41).
5. P2Y12 Inhibitor versus Aspirin Monotherapy for Long-Term Secondary Prevention
CAPRIE (A Randomized Blinded Trial of Clopidogrel Versus Aspirin in Patients at Risk of Ischaemic Events) trial was a prospective double-blind RCT reported in 1996 comparing clopidogrel monotherapy with aspirin (325 mg daily) monotherapy in patients with atherosclerotic vascular disease (defined as recent ischemic stroke, recent MI, or symptomatic peripheral arterial disease) [78]. A total of 19,185 patients were enrolled with a mean follow-up of 1.91 years. The primary endpoint was a composite of ischemic stroke, MI, or vascular death, which was significantly lower in the clopidogrel monotherapy group than the aspirin group (relative risk reduction, 8.7%; 95%CI, [0.3–16.5]; p = 0.043). Clopidogrel monotherapy had a significant lower rate of gastrointestinal hemorrhage events (patients ever reporting: 2.0% vs. 2.7%; p < 0.05 and severe gastrointestinal hemorrhage: 0.5% vs. 0.7%; p < 0.05). Moreover, clopidogrel monotherapy had a better upper GI tolerability than aspirin alone, with significant less indigestion/nausea/vomiting reported (patients ever reporting: 15.0% vs. 17.56%; p < 0.05) [78]. Despite the benefits of clopidogrel over aspirin, aspirin has remained the mainstay of therapy considering its reduced costs with clopidogrel being recommended over aspirin only in patients who could not tolerate or with hypersensitivity to aspirin. However, over two decades later with the availability of generic formulations of clopidogrel, there has been a re-appraisal for P2Y12 inhibitor monotherapy for long-term secondary prevention.
HOST-EXAM (Harmonizing Optimal Strategy for Treatment of Coronary Artery Stenosis-Extended Antiplatelet Monotherapy) trial was a prospective, open-label RCT comparing clopidogrel monotherapy or aspirin monotherapy for 24 months in event-free patients who were on DAPT for 6–18 months after PCI (n = 5530) [79]. The primary endpoint was a composite of all-cause death, non-fatal MI, stroke, readmission due to ACS, and major bleeding (BARC 3–5). At 2 years, clopidogrel monotherapy significantly reduced the primary endpoint compared to aspirin monotherapy (HR, 0.73; 95%CI, [0.59–0.90]; p = 0.003), driven by both the ischemic composite endpoint (HR, 0.68; 95%CI, [0.52–0.87]; p = 0.003) and major bleeding (HR, 0.63; 95%CI, [0.41–0.97]; p = 0.035).
GLOBAL LEADERS investigators performed a post-hoc landmark analysis between the first and second year of follow-up in patients who were event free during the first year [80]. In particular, during this period, patients were on ticagrelor monotherapy and aspirin monotherapy. There was a lower rate of MI in the ticagrelor monotherapy compared to the aspirin monotherapy group (adjusted HR, 0.74; 95%CI, [0.58–0.96]; p = 0.022), but at the expense of a higher rate of major bleeding (adjusted HR, 1.89; 95%CI, [1.03–3.45]; p = 0.005).
Meta-Analysis
The P2Y12 inhibitor or aspirin monotherapy as secondary prevention in patients with coronary artery disease: an individual patient data meta-analysis of randomized trials (PANTHER) trial assessed the role of long-term P2Y12 monotherapy compared to aspirin monotherapy for the prevention of recurrent events in patients with CAD [81]. This analysis included 24,325 patients from seven RCTs. The primary endpoint was the composite of cardiovascular or vascular death, any non-fatal MI, and any non-fatal stroke. At a median of 557 days, P2Y12 monotherapy was associated with a significant reduction in the primary endpoint compared to aspirin monotherapy (HR, 0.88; 95%CI, [0.79–0.97]; p = 0.014). The P2Y12 monotherapy was associated with a significant reduction in MI (HR, 0.89; 95%CI, [0.81–0.98]; p = 0.020) and definite/probable stent thrombosis (HR, 0.46; 95%CI, [0.23–0.92]; p = 0.028) without a significant reduction in major bleedings (HR, 0.87; 95%CI, [0.70–1.09]; p = 0.230), and all cause-death (HR, 1.04; 95%CI, [0.91–1.20]; p = 0.560). Concerning the bleeding causes, P2Y12 monotherapy was associated with a significant reduction in gastrointestinal bleeding (HR, 0.75; 95%CI, [0.57–0.97]; p = 0.027) and ICH (HR, 0.32; 95%CI, [0.14–0.75]; p = 0.009).
6. Guidelines on P2Y12 Inhibitor Monotherapy
Several scientific societies have incorporated P2Y12 monotherapy among their recommendations in patients treated with PCI. The 2020 European Society of Cardiology (ESC) guidelines for the management of non-ST-elevation acute coronary syndrome (NSTE-ACS) recommend stopping aspirin after 3–6 months should be considered, depending on the balance between the ischemic and bleeding risk [9]. The 2021 American College of Cardiology (ACC), American Heart Association (AHA), and Society for Cardiovascular Angiography and Interventions (SCAI) guidelines for coronary artery revascularization which were developed after the ESC guidelines and thus had more data available, state that in selected patients undergoing PCI, shorter duration DAPT (1–3 months) is reasonable, with subsequent transition to P2Y12 inhibitor monotherapy to reduce the risk of bleeding events (Table 2) [2]. For long-term secondary prevention, clopidogrel is recommended in patients who cannot take aspirin due to intolerance or hypersensitivity [8].
7. Ongoing Studies of P2Y12 Inhibitor Monotherapy
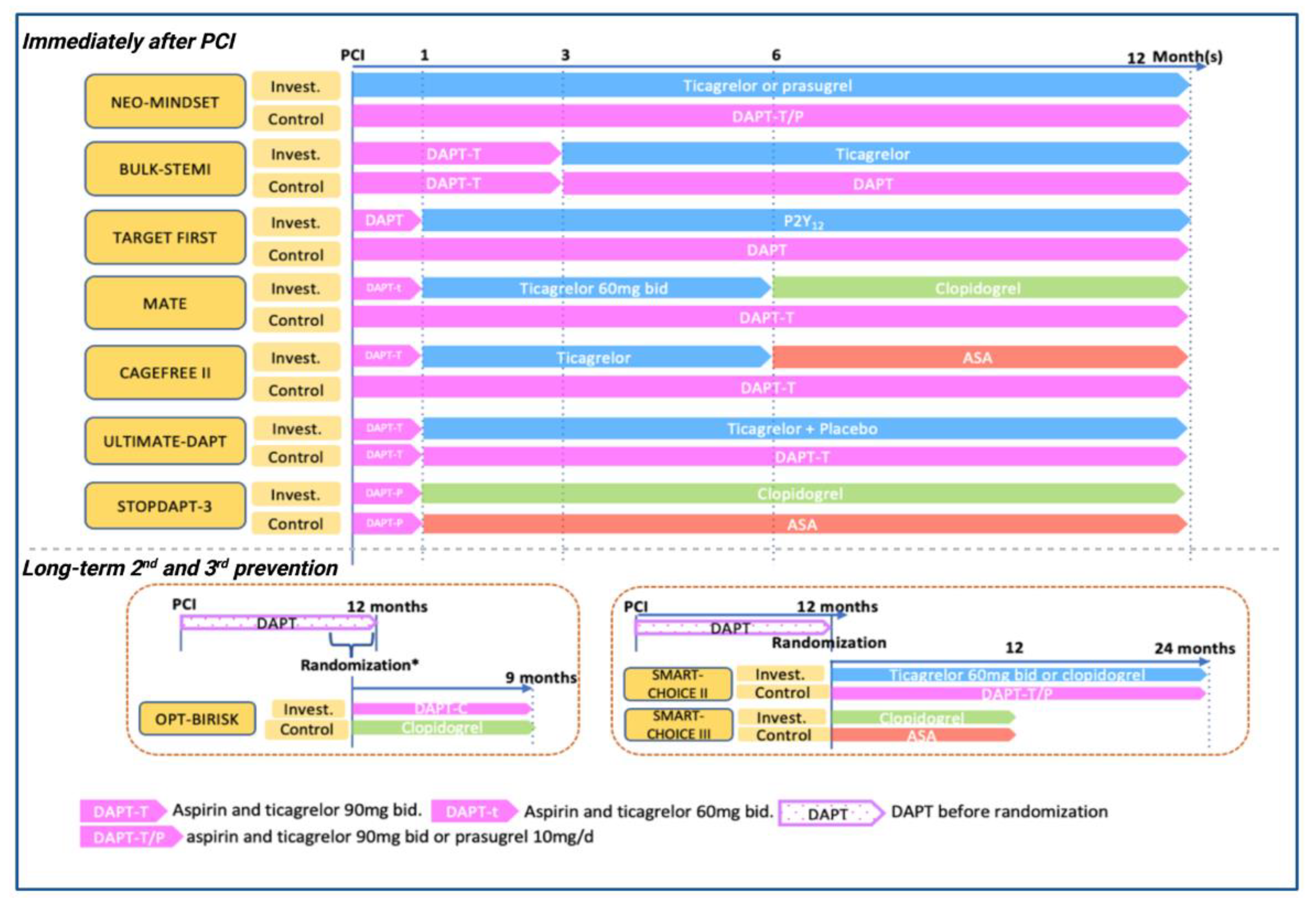
The role of P2Y12 monotherapy in patients treated with PCI is currently a topic of extensive research with more than 10 ongoing RCTs (Table 3 and Figure 3). Overall, most of the ongoing trials are focused on ACS patients. In particular, ULTIMATE-DAPT is a placebo-controlled RCT that will recruit event-free patients after 1 month of DAPT and compare ticagrelor plus placebo or ticagrelor-based DAPT for 11 months. The MATE and CAGEFREE II trials are investigating a de-escalation strategy consisting of 1 month of DAPT, followed by 5 months of ticagrelor monotherapy, and finalized by 6 months of clopidogrel or aspirin monotherapy. Among HBR or ACS patients, STOPDAPT-3 will compare a short course if clopidogrel-based DAPT with standard clopidogrel DAPT duration. The BULK-STEMI will determine the efficacy of ticagrelor monotherapy after 3 months of ticagrelor-based DAPT in patients presenting with STEMI. Two studies, ASET-JAPAN and NEO-MINDSET, will also assess the role of prasugrel monotherapy, with peri-PCI aspirin only instead of short-term aspirin in other studies. Moreover, in the setting of prolonged antiplatelet therapy after a standard DAPT, SMART-CHOICE II, OPT-BIRISK, and SMART-CHOICE III trials will assess different long-term P2Y12 monotherapy regimens vs. DAPT or ASA monotherapy.
8. Gaps in Evidence
There are still several gaps in the knowledge that require further research. First, five out of seven trials studying P2Y12 monotherapy enrolled exclusively East Asian populations, who have lower ischemic risk and a higher tendency of serious bleeding than Caucasians (i.e., East Asian Paradox), limiting extrapolation of many of the study findings to other ethnicities [82]. Second, as a potent P2Y12 inhibitor, compared to ticagrelor, prasugrel has advantages including its once daily regimen and the less respiratory side effect, which greatly improves adherence. However, there are no dedicated RCTs of prasugrel monotherapy. Third, although HBR patients could benefit more from P2Y12 monotherapy as a bleeding reduction strategy, there are no dedicated RCTs in HBR patients and the current evidence is derived from post-hoc analysis. Fourth, four out seven trials used clopidogrel as the main P2Y12 inhibitor, platelet function testing or CYP2C19 genotyping to assess the probability of HPR was not performed in any of these trials and it is unclear if adverse events could be related to clopidogrel poor responders [41,83]. Ultimately, P2Y12 monotherapy has been mainly compared with standard DAPT regimens and it is unknown how this strategy compares with other bleeding avoidance strategies, including short DAPT with discontinuation of P2Y12 inhibitor and maintaining aspirin or de-escalation DAPT approaches (e.g., switching from ticagrelor/prasugrel to clopidogrel or reducing the dose of ticagrelor/prasugrel) [84]. The current gaps in knowledge and ongoing trials are summarized in Table 4.
9. Practical Implications
The P2Y12 monotherapy is an emerging strategy to be considered among the available bleeding avoidance strategies in selected patients taking into consideration the following. First, the safety and efficacy of monotherapy outside of RCTs are very limited, underscoring that the eligible patients are those who meet the specific selection criteria of the RCTs [85]. It should be underscored that these trials are heterogeneous in terms of enrolled populations (Western countries vs. East Asian countries) which could impact the thrombotic and bleeding risk profiles of the studied populations. Furthermore, previous studies have shown that different bleeding avoidance strategies (i.e., abbreviated DAPT vs. de-escalation) are associated with different impact on clinical outcomes, suggesting that the selected strategy should be tailored according to patient characteristics and desired outcomes [84]. Moreover, procedural characteristics could also raise the concern about the outcomes in patients treated with complex PCI. Nevertheless, post-hoc analyses of these trials have not shown impaired outcomes among patients treated with complex PCI [86]. Second, the clinical presentation and the selected P2Y12 inhibitor appear to impact outcomes. In particular, prasugrel, and ticagrelor are recommended over clopidogrel in patients with ACS. In the GLOBAL LEADERS, TWILIGHT, and TICO trials, patients with ACS treated with ticagrelor monotherapy reduced bleeding without affecting ischemic outcomes. However, in patients with ACS and clopidogrel monotherapy, the STOPDAPT-2 ACS trial showed reduced bleeding but increased ischemic events [43]. On the other hand, in CCS, clopidogrel appears to be a safe and effective drug, as shown in the SMART-CHOICE and STOPDAPT-2 trials [39,42]. Moreover, ticagrelor can also be an option in CCS with high ischemic risk as reported in the TWILIGHT trial [62]. Third, most of these trials were designed with run-in phases and randomized only event-free patients after a short course of DAPT (i.e., 1–3 months). Therefore, in daily clinical practice, the decision to drop aspirin and continue P2Y12 inhibitor monotherapy should be made according to these protocols. Ultimately, P2Y12 inhibitor monotherapy has been compared mainly with standard DAPT (i.e., guideline-recommended duration) up to one year after the index PCI or randomization. Therefore, the clinical benefit of P2Y12 inhibitor monotherapy compared to other DAPT regimens and beyond the following 12–15 months of PCI is uncertain. Nevertheless, the only recent piece of information about P2Y12 monotherapy for long-term 24 months in event-free patients who were on DAPT for 6–18 months after PCI) comes from the HOST-EXAM trial, which suggests that clopidogrel monotherapy is safe and effective strategy compared to aspirin monotherapy [79].
10. Conclusions
Although DAPT with aspirin and a P2Y12 inhibitor is the standard care and guideline-recommended strategy in patients treated with PCI, recent pharmacodynamic studies have shown limited synergistic effects of aspirin in addition to potent oral P2Y12 inhibitors and have challenged the need for DAPT to achieve optimal platelet inhibition. In fact, while DAPT is associated with a reduction in ischemic events, it also increases bleeding, the risk of which is proportional to the intensity and duration of DAPT. As thrombotic complications mostly occur early after PCI, while bleeding accrues over the time, bleeding reduction strategies have been developed so that enhanced antithrombotic effects are present in the early phases post-PCI end then reduced afterwards. To this extent, several RCTs have assessed the role of P2Y12 inhibitor monotherapy compared to a standard DAPT regimen. Overall, P2Y12 inhibitor monotherapy is safe and effective for reducing bleeding without compromising ischemic outcomes in event-free patients treated with PCI after a short course of DAPT. In particular, ticagrelor has shown optimal results in patients with ACS, whereas clopidogrel and ticagrelor have been safe and effective for preventing recurrent events in CCS. The P2Y12 inhibitor monotherapy has already been incorporated in European and American guidelines as a reasonable antiplatelet strategy in patients treated with PCI. Over ten RCTs are ongoing to confirm previous findings and provide new insights P2Y12 inhibitor monotherapy immediately after PCI, the role of prasugrel, and outcomes in patients with STEMI. Ultimately, ongoing research is warranted to define whether P2Y12 inhibitor monotherapy should be preferred over aspirin for long-term secondary prevention in patients with CCS.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/article/10.3390/jcdd9100340/s1, Table S1: Prespecified and selected post-hoc analyses of GLOBAL LEADERS trial; Table S2: Prespecified and selected post-hoc analyses of TWILIGHT trial; Table S3: Prespecified and selected post-hoc analyses of TICO trial.
Author Contributions
X.Z.: writing—original draft preparation, L.O.-P. and D.J.A.: writing—review and editing. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
Angiolillo declares that he has received consulting fees or honoraria from Abbott, Amgen, AstraZeneca, Bayer, Biosensors, Boehringer Ingelheim, Bristol-Myers Squibb, Chiesi, Daiichi-Sankyo, Eli Lilly, Haemonetics, Janssen, Merck, Novartis, PhaseBio, PLx Pharma, Pfizer, and Sanofi; D.J.A. also declares that his institution has received research grants from Amgen, AstraZeneca, Bayer, Biosensors, CeloNova, CSL Behring, Daiichi-Sankyo, Eisai, Eli Lilly, Gilead, Idorsia, Janssen, Matsutani Chemical Industry Co., Merck, Novartis, and the Scott R. MacKenzie Foundation. Other authors have nothing to declare.
Abbreviations
| ACC | American College of Cardiology |
| ACS | acute coronary syndrome |
| ADP | adenosine diphosphate |
| AHA | American Heart Association |
| ARC | Academic Research Consortium |
| BARC | bleeding academic research consortium |
| BRS | bioresorbable scaffold |
| CAD | coronary artery disease |
| CCS | chronic coronary syndrome |
| CI | confidence interval |
| COX-1 | cyclooxygenase-1 |
| CV | cardiovascular |
| CYP2C19 | hepatic cytochrome P450 2C19 |
| DAPT | dual antiplatelet therapy |
| DAPT-C | clopidogrel-based dual antiplatelet therapy |
| DAPT-T | ticagrelor-based dual antiplatelet therapy |
| DAPT-T/P | ticagrelor-based or prasugrel-based dual antiplatelet therapy |
| DM | diabetes mellitus |
| ESC | European Society of Cardiology |
| GI | gastrointestinal |
| HBR | high bleeding risk |
| HPR | high platelet reactivity |
| HR | hazard ratio |
| MACCE | major adverse cardiac and cerebrovascular events |
| MI | myocardial infarction |
| NACE | net adverse clinical event |
| NSTE-ACS | non-ST-elevation acute coronary artery syndrome |
| PCI | percutaneous coronary intervention |
| PFT | platelet function test |
| POCE | patient-oriented composite endpoints |
| Pt-EES | platinum-chromium everolimus-eluting stent |
| RCT | randomized controlled trial |
| SCAI | Society for Cardiovascular Angiography and Interventions |
| SIHD | stable ischemic heart disease |
| STEMI | ST elevation myocardial infarction |
| TIMI | Thrombolysis in Myocardial Infarction |
References
- Neumann, F.J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur. Heart J. 2019, 40, 87–165. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lawton, J.S.; Tamis-Holland, J.E.; Bangalore, S.; Bates, E.R.; Beckie, T.M.; Bischoff, J.M.; Bittl, J.A.; Cohen, M.G.; DiMaio, J.M.; Don, C.W.; et al. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2022, 145, e4–e17. [Google Scholar] [CrossRef]
- Alkhouli, M.; Alqahtani, F.; Kalra, A.; Gafoor, S.; Alhajji, M.; Alreshidan, M.; Holmes, D.R.; Holmes, D.R. Trends in Characteristics and Outcomes of Patients Undergoing Coronary Revascularization in the United States, 2003–2016. JAMA Netw. Open 2020, 3, e1921326. [Google Scholar] [CrossRef] [PubMed]
- Mauri, L.; Kereiakes, D.J.; Yeh, R.W.; Driscoll-Shempp, P.; Cutlip, D.E.; Steg, P.G.; Normand, S.-L.T.; Braunwald, E.; Wiviott, S.D.; Cohen, D.J.; et al. Twelve or 30 Months of Dual Antiplatelet Therapy after Drug-Eluting Stents. N. Engl. J. Med. 2014, 371, 2155–2166. [Google Scholar] [CrossRef] [Green Version]
- Brugaletta, S.; Gomez-Lara, J.; Ortega-Paz, L.; Jimenez-Diaz, V.; Jimenez, M.; Jiménez-Quevedo, P.; Diletti, R.; Mainar, V.; Campo, G.; Silvestro, A.; et al. 10-Year Follow-Up of Patients with Everolimus-Eluting Versus Bare-Metal Stents After ST-Segment Elevation Myocardial Infarction. J. Am. Coll. Cardiol. 2021, 77, 1165–1178. [Google Scholar] [CrossRef]
- Coughlan, J.J.; Maeng, M.; Räber, L.; Brugaletta, S.; Aytekin, A.; Jensen, L.O.; Bär, S.; Ortega-Paz, L.; Laugwitz, K.-L.; Madsen, M.; et al. Ten-year patterns of stent thrombosis after percutaneous coronary intervention with new- versus early-generation drug-eluting stents: Insights from the DECADE cooperation. Rev. Esp. Cardiol. 2022. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M.; Bueno, H.; Byrne, R.A.; Collet, J.-P.; Costa, F.; Jeppsson, A.; Jüni, P.; Kastrati, A.; Kolh, P.; Mauri, L.; et al. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur. Heart J. 2018, 39, 213–260. [Google Scholar]
- Knuuti, J.; Revenco, V. 2019 ESC Guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 2020, 41, 407–477. [Google Scholar] [CrossRef] [Green Version]
- Collet, J.-P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef] [PubMed]
- Evidence Review Committee Members; Bittl, J.A.; Baber, U.; Bradley, S.M.; Wijeysundera, D.N. Duration of Dual Antiplatelet Therapy: A Systematic Review for the 2016 ACC/AHA Guideline Focused Update on Duration of Dual Antiplatelet Therapy in Patients with Coronary Artery Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2016, 68, 1116–1139. [Google Scholar]
- Angiolillo, D.J.; Galli, M.; Collet, J.P.; Kastrati, A.; O’Donoghue, M.L. Antiplatelet therapy after percutaneous coronary intervention. EuroIntervention 2022, 17, e1371–e1396. [Google Scholar] [PubMed]
- Angiolillo, D.J.; Fernandez-Ortiz, A.; Bernardo, E.; Alfonso, F.; Macaya, C.; Bass, T.A.; Costa, M.A. Variability in Individual Responsiveness to Clopidogrel: Clinical Implications, Management, and Future Perspectives. J. Am. Coll. Cardiol. 2007, 49, 1505–1516. [Google Scholar] [CrossRef] [PubMed]
- Franchi, F.; Angiolillo, D.J. Novel antiplatelet agents in acute coronary syndrome. Nat. Rev. Cardiol. 2014, 12, 30–47. [Google Scholar] [CrossRef] [PubMed]
- Sibbing, D.; Aradi, D.; Alexopoulos, D.; Berg, J.T.; Bhatt, D.L.; Bonello, L.; Collet, J.-P.; Cuisset, T.; Franchi, F.; Gross, L.; et al. Updated Expert Consensus Statement on Platelet Function and Genetic Testing for Guiding P2Y12 Receptor Inhibitor Treatment in Percutaneous Coronary Intervention. JACC: Cardiovasc. Interv. 2019, 12, 1521–1537. [Google Scholar] [CrossRef]
- Ibanez, B.; James, S.; Agewall, S.; Antunes, M.J.; Bucciarelli-Ducci, C.; Bueno, H.; Caforio, A.L.P.; Crea, F.; Goudevenos, J.A.; Halvorsen, S. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: The Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur. Heart J. 2018, 39, 119–177. [Google Scholar]
- Capodanno, D.; Bhatt, D.L.; Gibson, C.M.; James, S.; Kimura, T.; Mehran, R.; Rao, S.V.; Steg, P.G.; Urban, P.; Valgimigli, M.; et al. Bleeding avoidance strategies in percutaneous coronary intervention. Nat. Rev. Cardiol. 2021, 19, 117–132. [Google Scholar] [CrossRef]
- Cao, D.; Chandiramani, R.; Chiarito, M.; E Claessen, B.; Mehran, R. Evolution of antithrombotic therapy in patients undergoing percutaneous coronary intervention: A 40-year journey. Eur. Heart J. 2020, 42, 339–351. [Google Scholar] [CrossRef]
- Urban, P.; Mehran, R.; Colleran, R.; Angiolillo, D.J.; A Byrne, R.; Capodanno, D.; Cuisset, T.; Cutlip, D.; Eerdmans, P.; Eikelboom, J.; et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention: A consensus document from the Academic Research Consortium for High Bleeding Risk. Eur. Heart J. 2019, 40, 2632–2653. [Google Scholar] [CrossRef] [Green Version]
- Galli, M.; Capodanno, D.; Andreotti, F.; Crea, F.; Angiolillo, D.J. Safety and efficacy of P2Y12 inhibitor monotherapy in patients undergoing percutaneous coronary interventions. Expert Opin. Drug Saf. 2020, 20, 9–21. [Google Scholar] [CrossRef]
- Capodanno, D.; Baber, U.; Bhatt, D.L.; Collet, J.-P.; Dangas, G.; Franchi, F.; Gibson, C.M.; Gwon, H.-C.; Kastrati, A.; Kimura, T.; et al. P2Y12 inhibitor monotherapy in patients undergoing percutaneous coronary intervention. Nat. Rev. Cardiol. 2022, 1–16. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Ueno, M.; Goto, S. Basic Principles of Platelet Biology and Clinical Implications. Circ. J. 2010, 74, 597–607. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Storey, R.F.; Newby, L.J.; Heptinstall, S. Effects of P2Y 1 and P2Y 12 receptor antagonists on platelet aggregation induced by different agonists in human whole blood. Platelets 2001, 12, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Ariotti, S.; van Leeuwen, M.; Brugaletta, S.; Leonardi, S.; Akkerhuis, K.M.; Rimoldi, S.F.; Janssens, G.N.; Ortega-Paz, L.; Gianni, U.; Berge, J.C.V.D.; et al. Effects of Ticagrelor, Prasugrel, or Clopidogrel at Steady State on Endothelial Function. J. Am. Coll. Cardiol. 2018, 71, 1289–1291. [Google Scholar] [CrossRef] [PubMed]
- Ariotti, S.; Ortega-Paz, L.; van Leeuwen, M.; Brugaletta, S.; Leonardi, S.; Akkerhuis, K.M.; Rimoldi, S.F.; Janssens, G.; Gianni, U.; van den Berge, J.C. Effects of Ticagrelor, Prasugrel, or Clopidogrel on Endothelial Function and Other Vascular Biomarkers: A Randomized Crossover Study. JACC Cardiovasc. Interv. 2018, 11, 1576–1586. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Payne, D.; Hayes, P.; Jones, C.; Belham, P.; Naylor, A.; Goodall, A. Combined therapy with clopidogrel and aspirin significantly increases the bleeding time through a synergistic antiplatelet action. J. Vasc. Surg. 2002, 35, 1204–1209. [Google Scholar] [CrossRef] [Green Version]
- Capodanno, D.; Angiolillo, D.J. When Less Becomes More: Insights on the Pharmacodynamic Effects of Aspirin Withdrawal in Patients with Potent Platelet P2Y 12 Inhibition Induced by Ticagrelor. J. Am. Heart Assoc. 2020, 9, e019432. [Google Scholar] [CrossRef]
- Armstrong, P.C.J.; Leadbeater, P.D.; Chan, M.V.; Kirkby, N.S.; Jakubowski, J.A.; Mitchell, J.A.; Warner, T.D. In the presence of strong P2Y12 receptor blockade, aspirin provides little additional inhibition of platelet aggregation. J. Thromb. Haemost. 2010, 9, 552–561. [Google Scholar] [CrossRef] [Green Version]
- Johnson, T.W.; Baos, S.; Collett, L.; Hutchinson, J.L.; Nkau, M.; Molina, M.; Aungraheeta, R.; Reilly-Stitt, C.; Bowles, R.; Reeves, B.C.; et al. Pharmacodynamic Comparison of Ticagrelor Monotherapy Versus Ticagrelor and Aspirin in Patients After Percutaneous Coronary Intervention: The TEMPLATE (Ticagrelor Monotherapy and Platelet Reactivity) Randomized Controlled Trial. J. Am. Heart Assoc. 2020, 9, e016495. [Google Scholar] [CrossRef]
- Baber, U.; Zafar, M.U.; Dangas, G.; Escolar, G.; Angiolillo, D.J.; Sharma, S.K.; Kini, A.S.; Sartori, S.; Joyce, L.; Vogel, B.; et al. Ticagrelor with or Without Aspirin After PCI: The TWILIGHT Platelet Substudy. J. Am. Coll. Cardiol. 2020, 75, 578–586. [Google Scholar] [CrossRef]
- Hennigan, B.W.; Good, R.; Adamson, C.; Parker, W.A.; Martin, L.; Anderson, L.; Campbell, M.; Serruys, P.W.; Storey, R.F.; Oldroyd, K.G. Recovery of platelet reactivity following cessation of either aspirin or ticagrelor in patients treated with dual antiplatelet therapy following percutaneous coronary intervention: A GLOBAL LEADERS substudy. Platelets 2020, 33, 141–146. [Google Scholar] [CrossRef] [PubMed]
- Franchi, F.; Rollini, F.; Faz, G.; Rivas, J.R.; Rivas, A.; Agarwal, M.; Briceno, M.; Wali, M.; Nawaz, A.; Silva, G.; et al. Pharmacodynamic Effects of Vorapaxar in Prior Myocardial Infarction Patients Treated With Potent Oral P2Y 12 Receptor Inhibitors With and Without Aspirin: Results of the VORA-PRATIC Study. J. Am. Heart Assoc. 2020, 9, e015865. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Wang, Z.; Shen, B.; Chen, C.; Ding, X.; Song, H. Effects of aspirin on the gastrointestinal tract: Pros vs. cons. Oncol. Lett. 2020, 20, 2567–2578. [Google Scholar] [CrossRef]
- Lavie, C.J.; Howden, C.W.; Scheiman, J.; Tursi, J. Upper Gastrointestinal Toxicity Associated with Long-Term Aspirin Therapy: Consequences and Prevention. Curr. Probl. Cardiol. 2017, 42, 146–164. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Prats, J.; Deliargyris, E.N.; Schneider, D.J.; Scheiman, J.; Kimmelstiel, C.; Steg, P.G.; Alberts, M.; Rosengart, T.; Mehran, R.; et al. Pharmacokinetic and Pharmacodynamic Profile of a Novel Phospholipid Aspirin Formulation. Clin. Pharmacokinet. 2022, 61, 465–479. [Google Scholar] [CrossRef]
- Moon, J.Y.; Franchi, F.; Rollini, F.; Angiolillo, D.J. Evolution of Coronary Stent Technology and Implications for Duration of Dual Antiplatelet Therapy. Prog. Cardiovasc. Dis. 2018, 60, 478–490. [Google Scholar] [CrossRef] [PubMed]
- Hahn, J.Y.; Song, Y.B.; Oh, J.H.; Chun, W.J.; Park, Y.H.; Jang, W.J.; Im, E.S.; Jeong, J.O.; Koh, Y.Y.; Yun, K.H. Effect of P2Y12 Inhibitor Monotherapy vs Dual Antiplatelet Therapy on Cardiovascular Events in Patients Undergoing Percutaneous Coronary Intervention: The SMART-CHOICE Randomized Clinical Trial. JAMA 2019, 321, 2428–2437. [Google Scholar] [CrossRef] [Green Version]
- Kim, J.; Jang, W.J.; Lee, W.S.; Choi, K.H.; Lee, J.M.; Park, T.K.; Yang, J.H.; Choi, J.-H.; Bin Song, Y.; Choi, S.-H.; et al. P2Y12 inhibitor monotherapy after coronary stenting according to type of P2Y12 inhibitor. Heart 2021, 107, 1077–1083. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.H.; Lee, S.Y.; Chun, W.J.; Song, Y.B.; Choi, S.H.; Jeong, J.O.; Oh, S.K.; Yun, K.H.; Koh, Y.Y.; Koh, Y.Y.; et al. Clopidogrel Monotherapy in Patients with and without On-Treatment High Platelet Reactivity: A SMART-CHOICE sub-study. EuroIntervention 2021. [Google Scholar] [CrossRef] [PubMed]
- Angiolillo, D.J.; Capodanno, D.; Danchin, N.; Simon, T.; Bergmeijer, T.O.; Ten Berg, J.M.; Sibbing, D.; Price, M.J. Derivation, Validation, and Prognostic Utility of a Prediction Rule for Nonresponse to Clopidogrel: The ABCD-GENE Score. JACC Cardiovasc Interv. 2020, 13, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, H.; Domei, T.; Morimoto, T.; Natsuaki, M.; Shiomi, H.; Toyota, T.; Ohya, M.; Suwa, S.; Takagi, K.; Nanasato, M.; et al. Effect of 1-Month Dual Antiplatelet Therapy Followed by Clopidogrel vs 12-Month Dual Antiplatelet Therapy on Cardiovascular and Bleeding Events in Patients Receiving PCI: The STOPDAPT-2 Randomized. Clin. Trial JAMA 2019, 321, 2414–2427. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Watanabe, H.; Morimoto, T.; Natsuaki, M.; Yamamoto, K.; Obayashi, Y.; Ogita, M.; Suwa, S.; Isawa, T.; Domei, T.; Yamaji, K.; et al. Comparison of Clopidogrel Monotherapy After 1 to 2 Months of Dual Antiplatelet Therapy With 12 Months of Dual Antiplatelet Therapy in Patients with Acute Coronary Syndrome: The STOPDAPT-2 ACS Randomized Clinical Trial. JAMA Cardiol. 2022, 7, 407–417. [Google Scholar] [CrossRef] [PubMed]
- Obayashi, Y.; Watanabe, H.; Morimoto, T.; Yamamoto, K.; Natsuaki, M.; Domei, T.; Yamaji, K.; Suwa, S.; Isawa, T.; Watanabe, H.; et al. Clopidogrel Monotherapy After 1-Month Dual Antiplatelet Therapy in Percutaneous Coronary Intervention: From the STOPDAPT-2 Total Cohort. Circ. Cardiovasc. Interv. 2022, 15, e012004. [Google Scholar] [CrossRef]
- Kogame, N.; Guimaraes, P.O.; Modolo, R.; De Martino, F.; Tinoco, J.; Ribeiro, E.E.; Kawashima, H.; Ono, M.; Hara, H.; Wang, R.; et al. Aspirin-Free Prasugrel Monotherapy Following Coronary Artery Stenting in Patients With Stable CAD: The ASET Pilot Study. JACC Cardiovasc. Interv. 2020, 13, 2251–2262. [Google Scholar] [CrossRef] [PubMed]
- Arora, S.; Shemisa, K.; Vaduganathan, M.; Qamar, A.; Gupta, A.; Garg, S.K.; Kumbhani, D.J.; Mayo, H.; Khalili, H.; Pandey, A.; et al. Premature Ticagrelor Discontinuation in Secondary Prevention of Atherosclerotic CVD: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2019, 73, 2454–2464. [Google Scholar] [CrossRef]
- Ortega-Paz, L.; Brugaletta, S.; Ariotti, S.; Akkerhuis, K.M.; Karagiannis, A.; Windecker, S.; Valgimigli, M.; On behalf of the HI-TECH Investigators. Adenosine and Ticagrelor Plasma Levels in Patients with and Without Ticagrelor-Related Dyspnea. Circulation 2018, 138, 646–648. [Google Scholar] [CrossRef]
- GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N. Eng. J. Med. 1993, 329, 673–682. [Google Scholar] [CrossRef] [Green Version]
- Gao, C.; Takahashi, K.; Garg, S.; Hara, H.; Wang, R.; Kawashima, H.; Ono, M.; Montalescot, G.; Haude, M.; Slagboom, T.; et al. Regional variation in patients and outcomes in the GLOBAL LEADERS trial. Int. J. Cardiol. 2020, 324, 30–37. [Google Scholar] [CrossRef]
- Chichareon, P.; Modolo, R.; Kerkmeijer, L.; Tomaniak, M.; Kogame, N.; Takahashi, K.; Chang, C.C.; Komiyama, H.; Moccetti, T.; Talwar, S.; et al. Association of Sex with Outcomes in Patients Undergoing Percutaneous Coronary Intervention: A Subgroup Analysis of the GLOBAL LEADERS Randomized Clinical Trial. JAMA Cardiol. 2020, 5, 21–29. [Google Scholar] [CrossRef] [PubMed]
- Tomaniak, M.; Chichareon, P.; Modolo, R.; Takahashi, K.; Chang, C.C.; Kogame, N.; Spitzer, E.; Buszman, P.E.; van Geuns, R.-J.M.; Valkov, V.; et al. Ticagrelor monotherapy beyond one month after PCI in ACS or stable CAD in elderly patients: A pre-specified analysis of the GLOBAL LEADERS trial. EuroIntervention 2020, 15, e1605–e1614. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, M.; Chichareon, P.; Tomaniak, M.; Kawashima, H.; Takahashi, K.; Kogame, N.; Modolo, R.; Hara, H.; Gao, C.; Wang, R.; et al. The association of body mass index with long-term clinical outcomes after ticagrelor monotherapy following abbreviated dual antiplatelet therapy in patients undergoing percutaneous coronary intervention: A prespecified sub-analysis of the GLOBAL LEADERS Trial. Clin. Res. Cardiol. 2020, 109, 1125–1139. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chichareon, P.; Modolo, R.; Kogame, N.; Takahashi, K.; Chang, C.-C.; Tomaniak, M.; Botelho, R.; Eeckhout, E.; Hofma, S.; Trendafilova-Lazarova, D.; et al. Association of diabetes with outcomes in patients undergoing contemporary percutaneous coronary intervention: Pre-specified subgroup analysis from the randomized GLOBAL LEADERS study. Atherosclerosis 2020, 295, 45–53. [Google Scholar] [CrossRef] [PubMed]
- Tomaniak, M.; Chichareon, P.; Klimczak-Tomaniak, D.; Takahashi, K.; Kogame, N.; Modolo, R.; Wang, R.; Ono, M.; Hara, H.; Gao, C.; et al. Impact of renal function on clinical outcomes after PCI in ACS and stable CAD patients treated with ticagrelor: A prespecified analysis of the GLOBAL LEADERS randomized clinical trial. Clin. Res. Cardiol. 2020, 109, 930–943. [Google Scholar] [CrossRef]
- Kogame, N.; Chichareon, P.; De Wilder, K.; Takahashi, K.; Modolo, R.; Chang, C.C.; Tomaniak, M.; Komiyama, H.; Chieffo, A.; Colombo, A.; et al. Clinical relevance of ticagrelor monotherapy following 1-month dual antiplatelet therapy after bifurcation percutaneous coronary intervention: Insight from GLOBAL LEADERS trial. Catheter. Cardiovasc. Interv. 2019, 96, 100–111. [Google Scholar] [CrossRef] [PubMed]
- Gao, C.; Buszman, P.; Buszman, P.; Chichareon, P.; Modolo, R.; Garg, S.; Takahashi, K.; Kawashima, H.; Wang, R.; Chang, C.C.; et al. Influence of Bleeding Risk on Outcomes of Radial and Femoral Access for Percutaneous Coronary Intervention: An Analysis from the GLOBAL LEADERS Trial. Can. J. Cardiol. 2021, 37, 122–130. [Google Scholar] [CrossRef]
- Franzone, A.; McFadden, E.P.; Leonardi, S.; Piccolo, R.; Vranckx, P.; Serruys, P.W.; Hamm, C.; Steg, P.G.; Heg, D.; Branca, M.; et al. Ticagrelor alone or conventional dual antiplatelet therapy in patients with stable or acute coronary syndromes. EuroIntervention 2020, 16, 627–633. [Google Scholar] [CrossRef]
- Serruys, P.W.; Tomaniak, M.; Chichareon, P.; Modolo, R.; Kogame, N.; Takahashi, K.; Chang, C.C.; Spitzer, E.; Walsh, S.J.; Adlam, D.; et al. Patient-oriented composite endpoints and net adverse clinical events with ticagrelor monotherapy following percutaneous coronary intervention: Insights from the randomised GLOBAL LEADERS trial. EuroIntervention 2019, 15, e1090–e1098. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, K.; Chichareon, P.; Modolo, R.; Kogame, N.; Chang, C.C.; Tomaniak, M.; Moschovitis, A.; Curzen, N.; Haude, M.; Jung, W.; et al. Impact of ticagrelor monotherapy on two-year clinical outcomes in patients with long stenting: A post hoc analysis of the GLOBAL LEADERS trial. EuroIntervention 2020, 16, 634–644. [Google Scholar] [CrossRef]
- Chichareon, P.; Onuma, Y.; van Klaveren, D.; Modolo, R.; Kogame, N.; Takahashi, K.; Chang, C.C.; Tomaniak, M.; Asano, T.; Katagiri, Y.; et al. Validation of the updated logistic clinical SYNTAX score for all-cause mortality in the GLOBAL LEADERS trial. EuroIntervention 2019, 15, e539–e546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Serruys, P.W.; Takahashi, K.; Chichareon, P.; Kogame, N.; Tomaniak, M.; Modolo, R.; Chang, C.C.; Komiyama, H.; Soliman, O.; Wykrzykowska, J.; et al. Impact of long-term ticagrelor monotherapy following 1-month dual antiplatelet therapy in patients who underwent complex percutaneous coronary intervention: Insights from the Global Leaders trial. Eur. Heart J. 2019, 40, 2595–2604. [Google Scholar] [CrossRef] [PubMed]
- Mehran, R.; Baber, U.; Sharma, S.K.; Cohen, D.J.; Angiolillo, D.J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dangas, G.; Dudek, D.; et al. Ticagrelor with or without Aspirin in High-Risk Patients after PCI. N. Engl. J. Med. 2019, 381, 2032–2042. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Cao, D.; Baber, U.; Sartori, S.; Zhang, Z.; Dangas, G.; Mehta, S.; Briguori, C.; Cohen, D.J.; Collier, T.; et al. Impact of Age on the Safety and Efficacy of Ticagrelor Monotherapy in Patients Undergoing PCI. JACC: Cardiovasc. Interv. 2021, 14, 1434–1446. [Google Scholar] [CrossRef] [PubMed]
- Vogel, B.; Baber, U.; Cohen, D.J.; Sartori, S.; Sharma, S.K.; Angiolillo, D.J.; Farhan, S.; Goel, R.; Zhang, Z.; Briguori, C.; et al. Sex Differences Among Patients with High Risk Receiving Ticagrelor with or Without Aspirin After Percutaneous Coronary Intervention: A Subgroup Analysis of the TWILIGHT Randomized Clinical Trial. JAMA Cardiol. 2021, 6, 1032–1041. [Google Scholar] [CrossRef]
- Han, Y.; Claessen, B.E.; Chen, S.L.; Chunguang, Q.; Zhou, Y.; Xu, Y.; Hailong, L.; Chen, J.; Qiang, W.; Zhang, R.; et al. Ticagrelor with or Without Aspirin in Chinese Patients Undergoing Percutaneous Coronary Intervention: A TWILIGHT China Substudy. Circ. Cardiovasc. Interv. 2022, 15, e009495. [Google Scholar] [CrossRef]
- Angiolillo, D.J.; Baber, U.; Sartori, S.; Briguori, C.; Dangas, G.; Cohen, D.J.; Mehta, S.R.; Gibson, C.M.; Chandiramani, R.; Huber, K.; et al. Ticagrelor with or Without Aspirin in High-Risk Patients with Diabetes Mellitus Undergoing Percutaneous Coronary Intervention. J. Am. Coll. Cardiol. 2020, 75, 2403–2413. [Google Scholar] [CrossRef]
- Stefanini, G.G.; Briguori, C.; Cao, D.; Baber, U.; Sartori, S.; Zhang, Z.; Dangas, G.; Angiolillo, D.J.; Mehta, S.; Cohen, D.J.; et al. Ticagrelor monotherapy in patients with chronic kidney disease undergoing percutaneous coronary intervention: TWILIGHT-CKD. Eur. Heart J. 2021, 42, 4683–4693. [Google Scholar] [CrossRef] [PubMed]
- Chiarito, M.; Baber, U.; Cao, D.; Sharma, S.K.; Dangas, G.; Angiolillo, D.J.; Briguori, C.; Cohen, D.J.; Dudek, D.; Džavík, V.; et al. Ticagrelor Monotherapy After PCI in High-Risk Patients With Prior MI: A Prespecified TWILIGHT Substudy. JACC Cardiovasc. Interv. 2022, 15, 282–293. [Google Scholar] [CrossRef] [PubMed]
- Baber, U.; Dangas, G.; Angiolillo, D.J.; Cohen, D.J.; Sharma, S.K.; Nicolas, J.; Briguori, C.; Cha, J.Y.; Collier, T.; Dudek, D.; et al. Ticagrelor alone vs. ticagrelor plus aspirin following percutaneous coronary intervention in patients with non-ST-segment elevation acute coronary syndromes: TWILIGHT-ACS. Eur. Heart J. 2020, 41, 3533–3545. [Google Scholar] [CrossRef]
- Dangas, G.; Baber, U.; Sharma, S.; Giustino, G.; Sartori, S.; Nicolas, J.; Goel, R.; Mehta, S.; Cohen, D.; Angiolillo, D.A.; et al. Safety and efficacy of ticagrelor monotherapy according to drug-eluting stent type: The TWILIGHT-STENT study. EuroIntervention 2022, 17, 1330–1339. [Google Scholar] [CrossRef] [PubMed]
- Escaned, J.; Cao, D.; Baber, U.; Nicolas, J.; Sartori, S.; Zhang, Z.; Dangas, G.; Angiolillo, D.J.; Briguori, C.; Cohen, D.J.; et al. Ticagrelor monotherapy in patients at high bleeding risk undergoing percutaneous coronary intervention: TWILIGHT-HBR. Eur. Heart J. 2021, 42, 4624–4634. [Google Scholar] [CrossRef]
- Kim, B.K.; Hong, S.J.; Cho, Y.H.; Yun, K.H.; Kim, Y.H.; Suh, Y.; Cho, J.Y.; Her, A.Y.; Cho, S.; Jeon, D.W.; et al. Effect of Ticagrelor Monotherapy vs Ticagrelor with Aspirin on Major Bleeding and Cardiovascular Events in Patients With Acute Coronary Syndrome: The TICO Randomized Clinical Trial. JAMA 2020, 323, 2407–2416. [Google Scholar] [CrossRef]
- Yun, K.H.; Cho, J.Y.; Lee, S.Y.; Rhee, S.J.; Kim, B.K.; Hong, M.K.; Jang, Y.; Oh, S.K. The TICO Investigators Ischemic and Bleeding Events of Ticagrelor Monotherapy in Korean Patients with and Without Diabetes Mellitus: Insights From the TICO Trial. Front. Pharmacol. 2021, 11, 620906. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-J.; Lee, Y.-J.; Kim, B.-K.; Hong, S.-J.; Ahn, C.-M.; Kim, J.-S.; Ko, Y.-G.; Choi, D.; Hong, M.-K.; Jang, Y. Ticagrelor Monotherapy Versus Ticagrelor with Aspirin in Acute Coronary Syndrome Patients with a High Risk of Ischemic Events. Circ. Cardiovasc. Interv. 2021, 14, e010812. [Google Scholar] [CrossRef]
- Lee, S.-J.; Cho, J.Y.; Kim, B.-K.; Yun, K.H.; Suh, Y.; Cho, Y.-H.; Kim, Y.H.; Her, A.-Y.; Cho, S.; Jeon, D.W.; et al. Ticagrelor Monotherapy Versus Ticagrelor with Aspirin in Patients With ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2021, 14, 431–440. [Google Scholar] [CrossRef] [PubMed]
- Lee, Y.-J.; Suh, Y.; Kim, J.-S.; Cho, Y.-H.; Yun, K.H.; Kim, Y.H.; Cho, J.Y.; Her, A.-Y.; Cho, S.; Jeon, D.W.; et al. Ticagrelor Monotherapy After 3-Month Dual Antiplatelet Therapy in Acute Coronary Syndrome by High Bleeding Risk: The Subanalysis From the TICO Trial. Korean Circ. J. 2022, 52, 324–337. [Google Scholar] [CrossRef]
- Valgimigli, M.; Gragnano, F.; Branca, M.; Franzone, A.; Baber, U.; Jang, Y.; Kimura, T.; Hahn, J.-Y.; Zhao, Q.; Windecker, S.; et al. P2Y12 inhibitor monotherapy or dual antiplatelet therapy after coronary revascularisation: Individual patient level meta-analysis of randomised controlled trials. BMJ 2021, 373, n1332. [Google Scholar] [CrossRef]
- CAPRIE Steering Committee. A randomised, blinded, trial of clopidogrel versus aspirin in patients at risk of ischaemic events (CAPRIE). CAPRIE Steering Committee. Lancet 1996, 348, 1329–1339. [Google Scholar] [CrossRef]
- Koo, B.-K.; Kang, J.; Park, K.W.; Rhee, T.-M.; Yang, H.-M.; Won, K.-B.; Rha, S.-W.; Bae, J.-W.; Lee, N.H.; Hur, S.-H.; et al. Aspirin versus clopidogrel for chronic maintenance monotherapy after percutaneous coronary intervention (HOST-EXAM): An investigator-initiated, prospective, randomised, open-label, multicentre trial. Lancet 2021, 397, 2487–2496. [Google Scholar] [CrossRef]
- Ono, M.; Hara, H.; Kawashima, H.; Gao, C.; Wang, R.; Wykrzykowska, J.J.; Piek, J.J.; Garg, S.; Hamm, C.; Steg, P.G.; et al. Ticagrelor monotherapy versus aspirin monotherapy at 12 months after percutaneous coronary intervention: A landmark analysis of the GLOBAL LEADERS trial. EuroIntervention 2022, 18, e377–e388. [Google Scholar] [CrossRef] [PubMed]
- Valgimigli, M. Patients with coronary artery disease should receive P2Y12 inhibitor instead of aspirin. Vol ESC Congress 2022, 2022. [Google Scholar]
- Kim, H.K.; Tantry, U.S.; Smith, S.C., Jr.; Jeong, M.H.; Park, S.-J.; Kim, M.H.; Lim, D.-S.; Shin, E.-S.; Park, D.-W.; Huo, Y.; et al. The East Asian Paradox: An Updated Position Statement on the Challenges to the Current Antithrombotic Strategy in Patients with Cardiovascular Disease. Thromb. Haemost. 2020, 121, 422–432. [Google Scholar] [CrossRef] [PubMed]
- Galli, M.; Ortega-Paz, L.; Franchi, F.; Rollini, F.; Angiolillo, D.J. Precision medicine in interventional cardiology: Implications for antiplatelet therapy in patients undergoing percutaneous coronary intervention. Pharmacogenomics 2022, 23, 723–737. [Google Scholar] [CrossRef] [PubMed]
- Laudani, C.; Greco, A.; Occhipinti, G.; Ingala, S.; Calderone, D.; Scalia, L.; Agnello, F.; Legnazzi, M.; Mauro, M.S.; Rochira, C.; et al. Short Duration of DAPT Versus De-Escalation After Percutaneous Coronary Intervention for Acute Coronary Syndromes. JACC Cardiovasc. Interv. 2022, 15, 268–277. [Google Scholar] [CrossRef] [PubMed]
- Otsuka, T.; Ueki, Y.; Kavaliauskaite, R.; Zanchin, T.; Bär, S.; Stortecky, S.; Pilgrim, T.; Valgimigli, M.; Meier, B.; Heg, D.; et al. Single antiplatelet therapy with use of prasugrel in patients undergoing percutaneous coronary intervention. Catheterization and cardiovascular interventions. Off. J. Soc. Card. Angiogr. Interv. 2021, 98, E213–E221. [Google Scholar]
- Ortega-Paz, L.; Angiolillo, D.J. Optimal antiplatelet therapy in patients at high bleeding risk undergoing complex percutaneous coronary intervention. Eur. Heart J. 2022, 43, 3115–3117. [Google Scholar] [CrossRef]
Figure 1.
Selected bleeding avoidance strategies in patients without AF undergoing PCI. AF, atrial fibrillation; ACS, acute coronary syndrome; ASA, aspirin; CAD, coronary artery disease; CCS, chronic coronary syndrome; DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention; PFT, platelet function test; RCT, randomized controlled trial.
Figure 1.
Selected bleeding avoidance strategies in patients without AF undergoing PCI. AF, atrial fibrillation; ACS, acute coronary syndrome; ASA, aspirin; CAD, coronary artery disease; CCS, chronic coronary syndrome; DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention; PFT, platelet function test; RCT, randomized controlled trial.

Figure 2.
Randomized controlled trials of P2Y12 inhibitor monotherapy in patients treated with PCI. ASA, aspirin; DAPT, dual antiplatelet therapy; DAPT-C, clopidogrel-based dual antiplatelet therapy; DAPT-T, ticagrelor-based dual antiplatelet therapy; Invest., investigational group; PCI, percutaneous coronary intervention. * In HOST-EXAM trial, event-free patients who maintained DAPT for 6–18 months after PCI were randomized.
Figure 2.
Randomized controlled trials of P2Y12 inhibitor monotherapy in patients treated with PCI. ASA, aspirin; DAPT, dual antiplatelet therapy; DAPT-C, clopidogrel-based dual antiplatelet therapy; DAPT-T, ticagrelor-based dual antiplatelet therapy; Invest., investigational group; PCI, percutaneous coronary intervention. * In HOST-EXAM trial, event-free patients who maintained DAPT for 6–18 months after PCI were randomized.

Figure 3.
Ongoing randomized controlled trials of P2Y12 inhibitor monotherapy in patients treated with PCI. ASA, aspirin; DAPT, dual antiplatelet therapy; DAPT-C, clopidogrel-based antiplatelet therapy; DAPT-T, ticagrelor-based dual antiplatelet therapy; DAPT-T/P, ticagrelor-based or prasugrel-based dual antiplatelet therapy; Invest., investigational group; PCI, percutaneous coronary intervention. * OPT-BIRISK trial is randomizing patients with high ischemic or bleeding risk who already finished 9–12 months of DAPT.
Figure 3.
Ongoing randomized controlled trials of P2Y12 inhibitor monotherapy in patients treated with PCI. ASA, aspirin; DAPT, dual antiplatelet therapy; DAPT-C, clopidogrel-based antiplatelet therapy; DAPT-T, ticagrelor-based dual antiplatelet therapy; DAPT-T/P, ticagrelor-based or prasugrel-based dual antiplatelet therapy; Invest., investigational group; PCI, percutaneous coronary intervention. * OPT-BIRISK trial is randomizing patients with high ischemic or bleeding risk who already finished 9–12 months of DAPT.


{kind=link}
{kind=link}
{kind=link}
Table 1.
Randomized controlled trials for P2Y12 inhibitor monotherapy in patients treated with PCI.
| Studies | Experimental Group | Control Group * | Primary Outcome | Key Secondary Outcome |
|---|---|---|---|---|
| Immediately after PCI | ||||
| GLOBAL LEADERS 2018 (n = 15,968) | Ticagrelor-based DAPT for 1 month, then Ticagrelor monotherapy | ASA + clopidogrel (53%) ASA + ticagrelor (47%) | At 24 months, all-cause death, new Q-wave MI (RR, 0.87; 95% CI, [0.75–1.01]; p = 0.073) | BARC 3 or 5 bleeding (RR, 0.97; 95%CI, [0.78–1.20]; p = 0.770) |
| TWILIGHT 2019 (n = 7119) | Ticagrelor-based DAPT for 3 months, then Ticagrelor monotherapy | ASA + Ticagrelor | At 12 months, BARC 2–5 bleeding (HR, 0.56; 95% CI, [0.45–0.68]; p < 0.001) | BARC 3 or 5 bleeding (HR, 0.49; 95% CI, [0.33–0.74]; p < 0.001) |
| SMART CHOICE 2019 (n = 2993) | Clopidogrel (76.9%) Prasugrel (4.1%) Ticagrelor (19.0%) DAPT for 3 months, then monotherapy | ASA + clopidogrel (77.6%) ASA + Prasugrel (4.5%) ASA + ticagrelor (17.9%) | At 12 months, all-cause death, MI, stroke (difference, 0.4%; one-sided 95%CI, [−∞–1.3%]; p = 0.007 for non-inferiority) | BARC 2–5 bleeding (HR, 0.58; 95%CI [0.36–0.92]; p = 0.020) |
| STOPDAPT-2 2019 (n = 3045) | Clopidogrel based DAPT, then clopidogrel monotherapy | ASA + clopidogrel | At 12 months, CV death, MI, stroke, stent thrombosis, or TIMI major or minor bleeding (HR, 0.64; 95%CI, [0.42–0.98]; p < 0.001 for noninferiority; p = 0.04 for superiority) | TIMI major or minor bleeding (HR, 0.26; 95%CI, [0.11–0.64]; p = 0.004) -Ischemic endpoints (HR, 0.79; 95%CI, [0.49–1.29]; p = 0.340) |
| TICO (ACS) 2019 (n = 3056) | Ticagrelor-based DAPT, then ticagrelor monotherapy | ASA + ticagrelor | At 12 months, all-cause death, MI, stent thrombosis, stroke, target vessel revascularization and major bleeding (HR, 0.66; 95%CI, [0.48–0.92]; p = 0.01) | -TIMI major bleeding (HR, 0.56; 95%CI, [0.34–0.91]; p = 0.02) MACCE (HR, 0.69; 95%CI, [0.45–1.06]; p = 0.09) |
| STOPDAPT-2 ACS 2022 (n = 4169) | Clopidogrel-based DAPT, then Ticagrelor monotherapy | ASA + clopidogrel | At 12 months, CV death, MI, stroke, stent thrombosis, or TIMI major or minor bleeding (HR, 1.44; 95%CI, [0.80–1.62]; pnoninferiority = 0.06) | TIMI major or minor bleeding (HR, 0.46; 95%CI, [0.23–0.94]; p = 0.03) Significant increased risk of MI (HR, 1.91; 95%CI, [1.06–3.44]; p = 0.03) |
| Long-term 2nd and 3rd prevention | ||||
| HOST–EXAM 2020 (n = 5438) | Clopidogrel monotherapy, for 24 months | ASA monotherapy | At 24 months, all-cause death, non-fatal MI, stroke, readmission due to ACS, BARC 3–5 bleeding (HR, 0.73; 95%CI, [0.59–0.90]; p = 0.003) | BARC 3–5 bleeding (HR, 0.63; 95%CI, [0.41–0.97]; p = 0.035) |
* Complete details about regimen duration are shown in Figure 1. ACS, acute coronary syndrome; ASA, aspirin; CAD, coronary artery disease; CCS, chronic coronary syndrome; CI, confidence interval; CV, cardiovascular; DAPT, dual antiplatelet therapy; HR, hazard ratio; PCI, percutaneous coronary intervention; PFT, platelet function test; RCT, randomized controlled trial; RR, rate ratio; TIMI, Thrombolysis in Myocardial Infarction.
Table 2.
Clinical guidelines recommendations concerning P2Y12 inhibitor monotherapy.
| Cardiology Societies | Clinical Scenario | Recommendations | Level of Evidence * | Class of Recommendation * |
|---|---|---|---|---|
| ESC | NSTE-ACS [10] (2020) | After stent implantation in patients undergoing a strategy of DAPT, stopping aspirin after 3–6 months should be considered, depending on the balance between the ischemic and bleeding risk. | IIa | A |
| Chronic coronary syndrome [9] (2019) | Clopidogrel 75 mg daily is recommended as an alternative to aspirin in patients with aspirin intolerance. | I | B | |
| ACC/AHA/SCAI | Coronary artery revascularization [2] (2021) | In selected patients undergoing PCI, shorter-duration DAPT (1–3 months) is reasonable, with subsequent transition to P2Y12 inhibitor monotherapy to reduce the risk of bleeding events. | A | 2a |
* Details of the specific methodology of level of evidence and class of recommendation are provided in each guideline. ESC, European Society of cardiology; American College of Cardiology, American Heart Association, and Society for Cardiovascular Angiography and Interventions; NSTE-ACS, non-ST elevation acute coronary syndrome; DAPT, dual antiplatelet therapy; PCI, percutaneous coronary intervention.
Table 3.
Ongoing clinical trials for P2Y12 inhibitor monotherapy in patients undergoing PCI.
| Studies | Design | Population | Experimental Group | Control Group | Primary Outcome | Key Secondary Outcomes |
|---|---|---|---|---|---|---|
| RCTs immediately after PCI | ||||||
| NEO–MINDSET (n = 3400) (NCT04360720) | Open-label RCT 12 months follow-up | ACS | Ticagrelor or prasugrel monotherapy | ASA + ticagrelor or prasugrel | Ischemic: all-cause death, cerebrovascular accident, MI or urgent target vessel revascularization Bleeding: BARC type 2, 3 or 5 | Stent thrombosis BARC 1–5 bleeding Cost-effectiveness ratio |
| ULTIMATE–DAPT (n = 3486) (NCT03971500) | Placebo-controlled RCT 12 months follow-up | No MACCE or major bleeding within 30 days | Ticagrelor and placebo for 11 months | ASA + ticagrelor for 11 months | MACCE, clinical-relevant bleeding (BARC ≥ 2), target vessel failure | Net adverse clinical events |
| STOPDAPT-3 (n = 3110) (NCT04609111) | Open-label RCT 12 months follow-up | Patients with HBR or ACS | ASA + prasugrel for 1 month followed by clopidogrel monotherapy 11 months | ASA + prasugrel 1 month, ASA monotherapy 11 months | BARC 3 or 5 bleeding; cardiovascular composite (cardiovascular death, MI, ischemic stroke, definite stent thrombosis) | Target lesion/vessel failure and revascularization |
| BULK–STEMI (n = 1002) (NCT04570345) | Open-label RCT 12 months follow-up | STEMI | Ticagrelor monotherapy after 3 months of DAPT (ASA + ticagrelor) | ASA + P2Y12 inhibitor after 3 months of DAPT (ASA + ticagrelor) | MACCE (all-cause death, MI, cerebrovascular event, stent thrombosis) and bleeding events (BARC 3 or 5) | |
| TARGET FIRST (n = 2246) (NCT04753749) | Open-label RCT 12 months follow-up | NSTEMI or STEMI with complete revascularization | P2Y12 monotherapy after 1 month of DAPT | 12 months of DAPT | All-cause death, non-fatal MI, stent thrombosis, stroke, or bleeding events (BARC 3 or 5) | |
| MATE (n = 2856) (NCT04937699) | Open-label RCT 12 months follow-up | ACS and high bleeding risk | ASA + ticagrelor (60 mg bid) for 1 month → ticagrelor monotherapy (60 mg bid) for 5 months → clopidogrel monotherapy for 6 months | ASA+ ticagrelor | All-cause death, non-fatal MI, stroke, BARC type 2, 3 or 5 bleeding | |
| CAGEFREE II (n = 1908) (NCT04971356) | Open-label RCT 12 months follow-up | ACS treated with drug-coated balloon | ASA + ticagrelor for 1 month → ticagrelor monotherapy for 5 months → ASA monotherapy for 6 months | ASA + ticagrelor | All-cause death, stroke, MI, revascularization, BARC 3 or 5 bleeding | Stent thrombosis rates |
| Non-randomized single-arm study | ||||||
| PIONEER IV CHINA (n = 285) (NCT05015699) | Open-label single arm 12 months follow-up | PCI with HT supreme DES | Ticagrelor monotherapy after 1 month of DAPT | None | All-cause death, stroke, MI, coronary revascularization | |
| ASET–JAPAN (n = 400) (NCT05117866) | Open-label single arm 3 months follow-up for CCS, 12 months for ACS | NSTE–ACS and CCS | Prasugrel (loading: 20 mg; maintenance: 3.75 mg/d) 3 months in CCS and 12 months in NSTE–ACS | None | Ischemic: cardiac death, target-vessel MI, definite stent thrombosis Bleeding: BARC 3 or 5 bleeding | |
| Long-term 2nd and 3rd prevention | ||||||
| OPT–BIRISK (n = 7700) (NCT03431142) | Open-label RCT 9 months follow-up | ACS patients received 9–12 months of DAPT with high ischemic or bleeding risk | Clopidogrel for 9 months | ASA + clopidogrel for 9 months | BARC type 2–5 bleeding | MACCE |
| SMART–CHOICE II (n = 1520) (NCT03119012) | Open-label RCT 36 months follow-up after index procedure | No major MACCE at 12 month after BRS implantation | Clopidogrel or ticagrelor (60 mg bid) monotherapy for 24 months | ASA + clopidogrel or ticagrelor (60 mg bid) | Death, MI, cerebrovascular events | BARC 2, 3, 5 bleeding Revascularization Stent thrombosis |
| SMART–CHOICE III (n = 5000) (NCT04418479) | Open-label RCT 12 months follow-up | Patient finished 12 months of DAPT with high risk of recurrent ischemic events | Clopidogrel monotherapy | ASA monotherapy | MACCE | BARC 3/5 bleeding |
ACS, acute coronary syndrome; ASA, aspirin; BARC, Bleed Academic Research Consortium; BRS, Bioresorbable scaffold; DAPT, dual antiplatelet therapy; HBR, high bleeding risk; MACCE, major adverse cardiac and cerebrovascular events; MI, myocardial infarction; RCT, randomized controlled trial; STEMI, ST elevation myocardial infarction; NSTEMI, non-ST-elevation myocardial infarction. The dosages without specific notes are: aspirin, 81–100 mg daily; ticagrelor, 90 mg twice daily; prasugrel, 10 mg daily.
Table 4.
Current gaps in the evidence and potential research opportunities in the P2Y12 monotherapy.
Table 4.
Current gaps in the evidence and potential research opportunities in the P2Y12 monotherapy.
| Current Gaps | Ongoing Studies and Potential Research Opportunities |
|---|---|
Population:
| |
Clinical presentation:
|
|
Specific conditions:
|
|
Specific medications:
|
|
Comparison with other strategies:
|
|
ACS, acute coronary syndrome; DAPT, dual antiplatelet therapy; HBR, high bleeding risk; HPR, high platelet reactivity; RCT, randomized controlled trial; STEMI, ST elevation myocardial infarction; NSTEMI.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Zhou, X.; Angiolillo, D.J.; Ortega-Paz, L. P2Y12 Inhibitor Monotherapy after Percutaneous Coronary Intervention. J. Cardiovasc. Dev. Dis. 2022, 9, 340. https://doi.org/10.3390/jcdd9100340
AMA Style
Zhou X, Angiolillo DJ, Ortega-Paz L. P2Y12 Inhibitor Monotherapy after Percutaneous Coronary Intervention. Journal of Cardiovascular Development and Disease. 2022; 9(10):340. https://doi.org/10.3390/jcdd9100340
Chicago/Turabian StyleZhou, Xuan, Dominick J. Angiolillo, and Luis Ortega-Paz. 2022. "P2Y12 Inhibitor Monotherapy after Percutaneous Coronary Intervention" Journal of Cardiovascular Development and Disease 9, no. 10: 340. https://doi.org/10.3390/jcdd9100340
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.