
In-Hospital versus Out-of-Hospital Pulmonary Embolism: Clinical Characteristics, Biochemical Markers and Echocardiographic Indices
 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Protocol and Patient Selection
2.2. Biochemical Markers
2.3. Echocardiography
2.4. Follow-Up
2.5. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Symptoms, Signs and Clinical Scores
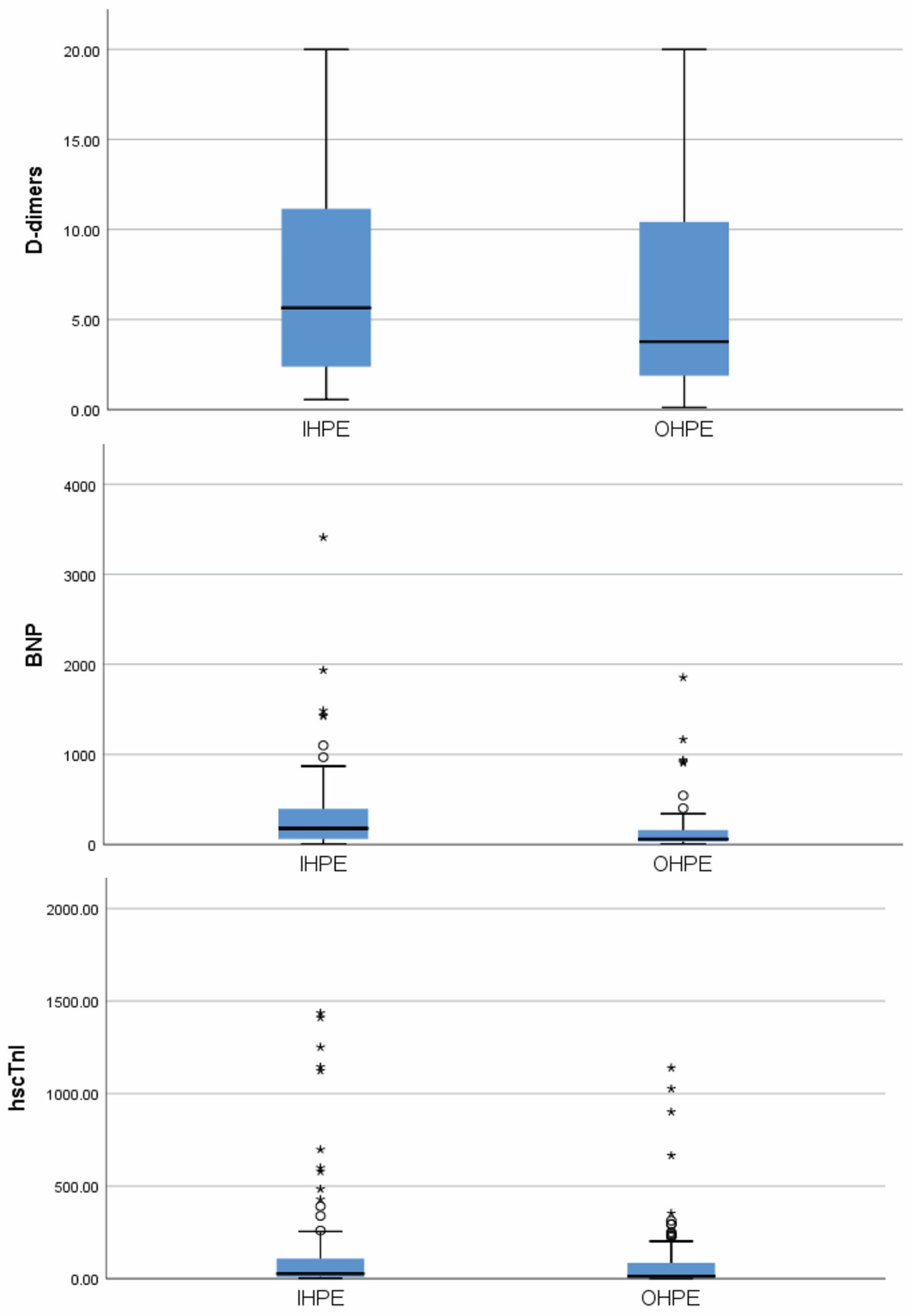
3.3. Biochemical Markers
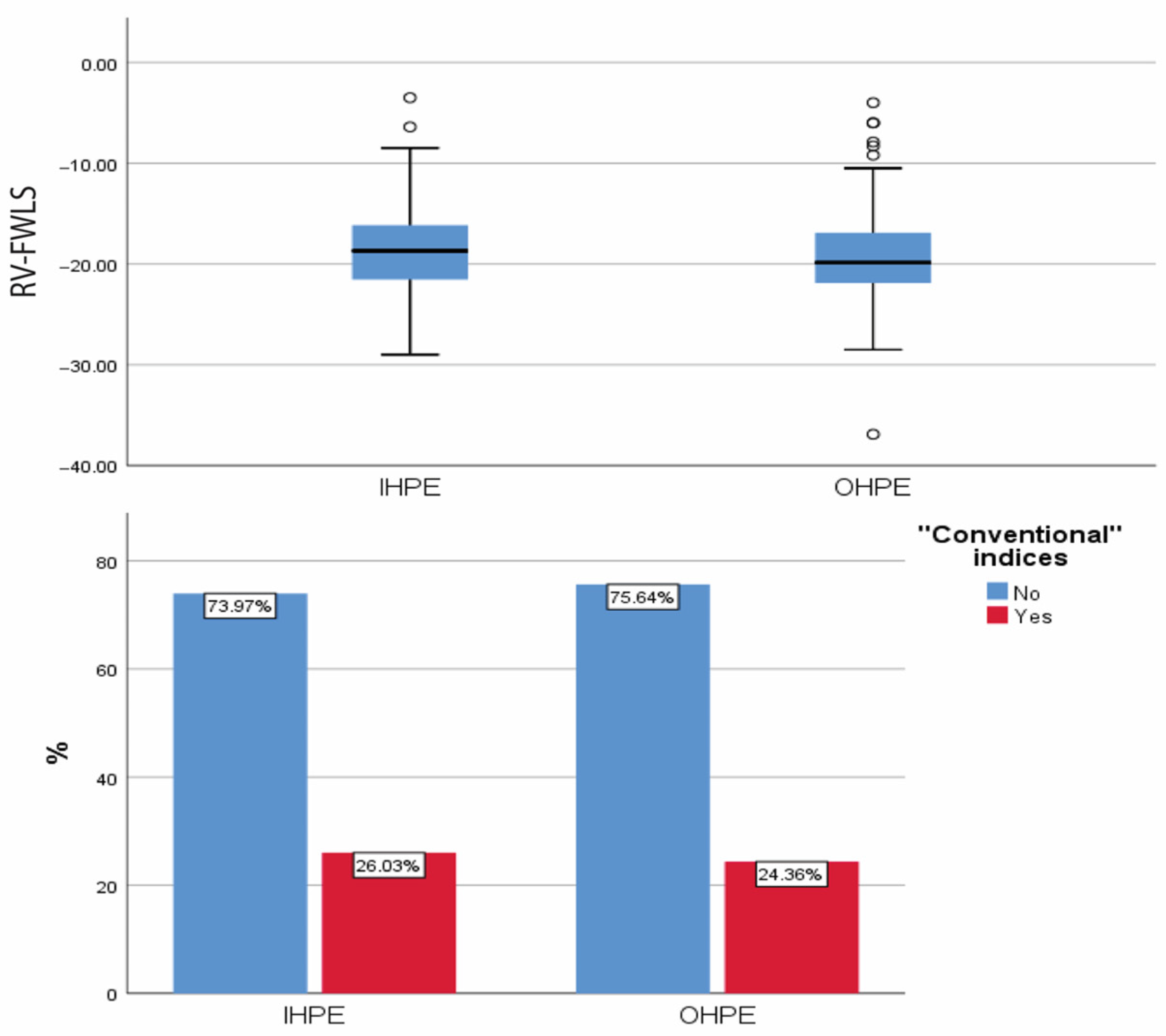
3.4. Echocardiography (Figure 2)

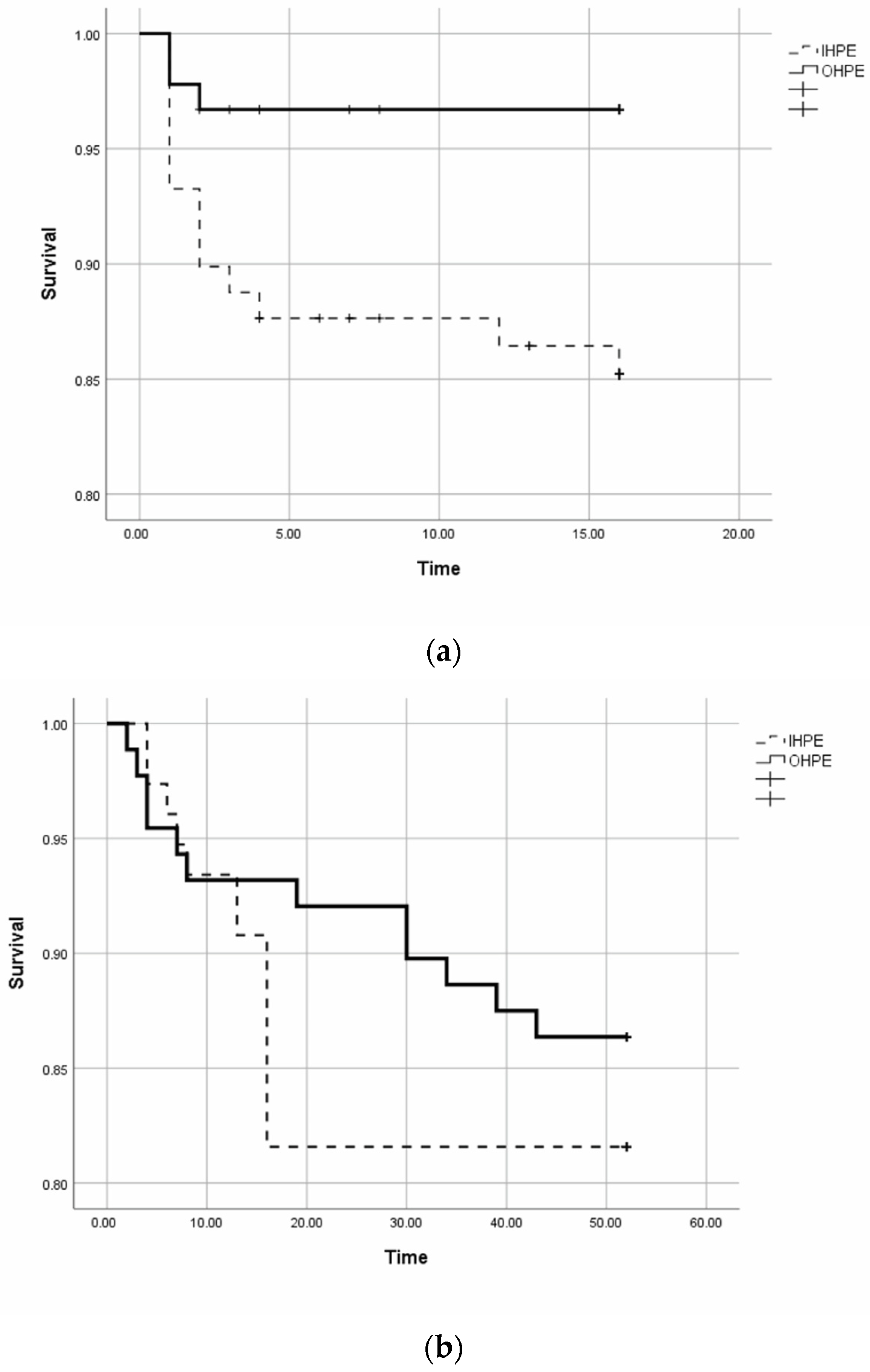
3.5. Prognosis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wendelboe, A.M.; Raskob, G.E. Global burden of thrombosis: Epidemiologic aspects. Circ. Res. 2016, 118, 1340–1347. [Google Scholar] [CrossRef] [PubMed]
- Søgaard, K.K.; Schmidt, M.; Pedersen, L.; Horváth-Puhó, E.; Sørensen, H.T. 30-year mortality after venous thromboembolism: A population-based cohort study. Circulation 2014, 130, 829–836. [Google Scholar] [CrossRef]
- van Maanen, R.; Trinks-Roerdink, E.M.; Rutten, F.H.; Geersing, G.J. A systematic review and meta-analysis of diagnostic delay in pulmonary embolism. Eur. J. Gen. Pract. 2022, 28, 165–172. [Google Scholar] [CrossRef] [PubMed]
- Wells, P.S.; Anderson, D.R.; Rodger, M.; Ginsberg, J.S.; Kearon, C.; Gent, M.; Turpie, A.G.; Bormanis, J.; Weitz, J.; Chamberlain, M.; et al. Derivation of a simple clinical model to categorize patients probability of pulmonary embolism: Increasing the models utility with the SimpliRED D-dimer. Thromb. Haemost. 2000, 83, 416–420. [Google Scholar] [PubMed]
- Gibson, N.S.; Sohne, M.; Kruip, M.J.; Tick, L.W.; Gerdes, V.E.; Bossuyt, P.M.; Wells, P.S.; Buller, H.R. Christopher study investigators. Further validation and simplification of the Wells clinical decision rule in pulmonary embolism. Thromb. Haemost. 2008, 99, 229–234. [Google Scholar] [CrossRef]
- Wolf, S.J.; McCubbin, T.R.; Feldhaus, K.M.; Faragher, J.P.; Adcock, D.M. Prospective validation of Wells Criteria in the evaluation of patients with suspected pulmonary embolism. Ann. Emerg. Med. 2004, 44, 503–510. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.; Goel, A. A study of modified Wells score for pulmonary embolism and age-adjusted D-dimer values in patients at risk for deep venous thrombosis. J. Fam. Med. Prim. Care 2023, 12, 2020–2023. [Google Scholar] [CrossRef]
- Robert-Ebadi, H.; Mostaguir, K.; Hovens, M.M.; Kare, M.; Verschuren, F.; Girard, P.; Huisman, M.V.; Moustafa, F.; Kamphuisen, P.W.; Buller, H.R.; et al. Assessing clinical probability of pulmonary embolism: Prospective validation of the simplified Geneva score. J. Thromb. Haemost. 2017, 15, 1764–1769. [Google Scholar] [CrossRef]
- Aujesky, D.; Obrosky, D.S.; Stone, R.A.; Auble, T.E.; Perrier, A.; Cornuz, J.; Roy, P.M.; Fine, M.J. Derivation and validation of a prognostic model for pulmonary embolism. Am. J. Respir. Crit. Care Med. 2005, 172, 1041–1046. [Google Scholar] [CrossRef]
- Flinterman, L.E.; van Hylckama Vlieg, A.; Cannegieter, S.C.; Rosendaal, F.R. Long-term survival in a large cohort of patients with venous thrombosis: Incidence and predictors. PLoS Med. 2012, 9, e1001155. [Google Scholar] [CrossRef]
- Sanchez, O.; Trinquart, L.; Caille, V.; Couturaud, F.; Pacouret, G.; Meneveau, N.; Verschuren, F.; Roy, P.-M.; Parent, F.; Righini, M.; et al. Prognostic Factors for Pulmonary Embolism. Am. J. Respir. Crit. Care Med. 2010, 181, 168–173. [Google Scholar] [CrossRef] [PubMed]
- Becattini, C.; Vedovati, M.C.; Agnelli, G. Prognostic value of troponins in acute pulmonary embolism: A meta-analysis. Circulation 2007, 116, 427–433. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Mos, I.C.; Huisman, M.V. Brain-type natriuretic peptide levels in the prediction of adverse outcome in patients with pulmonary embolism: A systematic review and meta-analysis. Am. J. Respir. Crit. Care Med. 2008, 178, 425–430. [Google Scholar] [CrossRef] [PubMed]
- Dabbouseh, N.M.; Patel, J.J.; Bergl, P.A. Role of echocardiography in managing acute pulmonary embolism. Heart 2019, 105, 1785–1792. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.K.; Park, J.H. Role of echocardiography in acute pulmonary embolism. Korean J. Intern. Med. 2023, 38, 456–470. [Google Scholar] [CrossRef] [PubMed]
- Lakkas, L.; Katsouras, C.S. Echocardiography in acute pulmonary embolism. Korean J. Intern. Med. 2023, 38, 566–567. [Google Scholar] [CrossRef] [PubMed]
- Allaert, F.A.; Benzenine, E.; Quantin, C. Hospital incidence and annual rates of hospitalization for venous thromboembolic disease in France and the USA. Phlebology 2017, 32, 443–447. [Google Scholar] [CrossRef] [PubMed]
- Heit, J.A.; Melton, L.J., 3rd; Lohse, C.M.; Petterson, T.M.; Silverstein, M.D.; Mohr, D.N.; O’Fallon, W.M. Incidence of venous thromboembolism in hospitalized patients vs community residents. Mayo Clin. Proc. 2001, 76, 1102–1110. [Google Scholar] [CrossRef] [PubMed]
- Oger, E. Incidence of venous thromboembolism: A community-based study in Western France. EPI-GETBP Study Group. Groupe d’Etude de la Thrombose de Bretagne Occidentale. Thromb. Haemost. 2000, 83, 657–660. [Google Scholar]
- Schrecengost, J.E.; LeGallo, R.D.; Boyd, J.C.; Moons, K.G.; Gonias, S.L.; Rose, C.E., Jr.; Bruns, D.E. Comparison of diagnostic accuracies in outpatients and hospitalized patients of D-dimer testing for the evaluation of suspected pulmonary embolism. Clin. Chem. 2003, 49, 1483–1490. [Google Scholar] [CrossRef]
- Jouveshomme, S.; Bohn, I.; Cazaban, A. Diagnosis of pulmonary embolism in hospitalised patients: Retrospective survey of an institutional standard. Eur. Respir. J. 2007, 30, 1117–1123. [Google Scholar] [CrossRef] [PubMed]
- Miron, M.J.; Perrier, A.; Bounameaux, H.; de Moerloose, P.; Slosman, D.O.; Didier, D.; Junod, A. Contribution of noninvasive evaluation to the diagnosis of pulmonary embolism in hospitalized patients. Eur. Respir. J. 1999, 13, 1365–1370. [Google Scholar] [CrossRef]
- Posadas-Martínez, M.L.; Vázquez, F.J.; Giunta, D.H.; Waisman, G.D.; de Quirós, F.G.; Gándara, E. Performance of the Wells score in patients with suspected pulmonary embolism during hospitalization: A delayed-type cross sectional study in a community hospital. Thromb. Res. 2014, 133, 177–181. [Google Scholar] [CrossRef] [PubMed]
- Choffat, D.; Farhoumand, P.D.; Jaccard, E.; de la Harpe, R.; Kraege, V.; Benmachiche, M.; Gerber, C.; Leuzinger, S.; Podmore, C.; Truong, M.K.; et al. Risk stratification for hospital-acquired venous thromboembolism in medical patients (RISE): Protocol for a prospective cohort study. PLoS ONE 2022, 17, e0268833. [Google Scholar] [CrossRef] [PubMed]
- Ballas, C.; Lakkas, L.; Kardakari, O.; Konstantinidis, A.; Exarchos, K.; Tsiara, S.; Kostikas, K.; Naka, K.Κ.; Michalis, L.K.; Katsouras, C.S. What is the real incidence of right ventricular affection in patients with acute pulmonary embolism? Acta Cardiol. 2023, 78, 1089–1098. [Google Scholar] [CrossRef] [PubMed]
- Le Gal, G.; Righini, M.; Roy, P.M.; Sanchez, O.; Aujesky, D.; Bounameaux, H.; Perrier, A. Prediction of pulmonary embolism in the emergency department: The revised Geneva score. Ann. Intern. Med. 2006, 144, 165–171. [Google Scholar] [CrossRef] [PubMed]
- Jiménez, D.; Aujesky, D.; Moores, L.; Gómez, V.; Lobo, J.L.; Uresandi, F.; Otero, R.; Monreal, M.; Muriel, A.; Yusen, R.D.; et al. Simplification of the pulmonary embolism severity index for prognostication in patients with acute symptomatic pulmonary embolism. Arch. Intern. Med. 2010, 170, 1383–1389. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef]
- Dutta, T.; Aronow, W.S. Echocardiographic evaluation of the right ventricle: Clinical implications. Clin. Cardiol. 2017, 40, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Söhne, M.; Kamphuisen, P.W.; van Mierlo, P.J.; Büller, H.R. Diagnostic strategy using a modified clinical decision rule and D-dimer test to rule out pulmonary embolism in elderly in- and outpatients. Thromb. Haemost. 2005, 94, 206–210. [Google Scholar] [CrossRef] [PubMed]
- Trihan, J.E.; Adam, M.; Jidal, S.; Aichoun, I.; Coudray, S.; Laurent, J.; Chaussavoine, L.; Chausserie, S.; Guillaumat, J.; Lanéelle, D.; et al. Performance of the Wells score in predicting deep vein thrombosis in medical and surgical hospitalized patients with or without thromboprophylaxis: The R-WITT study. Vasc. Med. 2021, 26, 288–296. [Google Scholar] [CrossRef] [PubMed]
- Berman, A.R. Pulmonary embolism in the elderly. Clin. Geriatr. Med. 2001, 17, 107–130. [Google Scholar] [CrossRef] [PubMed]
- Poenou, G.; Dumitru Dumitru, T.; Lafaie, L.; Mismetti, V.; Ayoub, E.; Duvillard, C.; Accassat, S.; Mismetti, P.; Heestermans, M.; Bertoletti, L. Pulmonary Embolism in the Cancer Associated Thrombosis Landscape. J. Clin. Med. 2022, 11, 5650. [Google Scholar] [CrossRef] [PubMed]
- Shalaby, K.; Kahn, A.; Silver, E.S.; Kim, M.J.; Balakumaran, K.; Kim, A.S. Outcomes of acute pulmonary embolism in hospitalized patients with cancer. BMC Pulm. Med. 2022, 22, 11. [Google Scholar] [CrossRef] [PubMed]
- Ng, A.C.; Chow, V.; Yong, A.S.; Chung, T.; Kritharides, L. Prognostic impact of the Charlson comorbidity index on mortality following acute pulmonary embolism. Respiration 2013, 85, 408–416. [Google Scholar] [CrossRef] [PubMed]
- de Miguel-Diez, J.; Albaladejo-Vicente, R.; Lopez-de-Andres, A.; Hernández-Barrera, V.; Jiménez, D.; Monreal, M.; Carabantes-Alarcon, D.; Zamorano-Leon, J.J.; Jimenez-Garcia, R. Changing Trends in Hospital Admissions for Pulmonary Embolism in Spain from 2001 to 2018. J. Clin. Med. 2020, 9, 3221. [Google Scholar] [CrossRef] [PubMed]
- Zöller, B.; Pirouzifard, M.; Sundquist, J.; Sundquist, K. Association of Short-Term Mortality of Venous Thromboembolism with Family History of Venous Thromboembolism and Charlson Comorbidity Index. Thromb. Haemost. 2019, 119, 48–55. [Google Scholar] [CrossRef]
- Aujesky, D.; Mor, M.K.; Geng, M.; Stone, R.A.; Fine, M.J.; Ibrahim, S.A. Predictors of early hospital readmission after acute pulmonary embolism. Arch. Intern. Med. 2009, 169, 287–293. [Google Scholar] [CrossRef]
- Keyzer, J.M.; Hoffmann, J.J.; Ringoir, L.; Nabbe, K.C.; Widdershoven, J.W.; Pop, V.J. Age- and gender-specific brain natriuretic peptide (BNP) reference ranges in primary care. Clin. Chem. Lab. Med. 2014, 52, 1341–1346. [Google Scholar] [CrossRef] [PubMed]
- Okamoto, R.; Ali, Y.; Hashizume, R.; Suzuki, N.; Ito, M. BNP as a Major Player in the Heart-Kidney Connection. Int. J. Mol. Sci. 2019, 20, 3581. [Google Scholar] [CrossRef] [PubMed]
- Yoo, B.S. Clinical Significance of B-type Natriuretic Peptide in Heart Failure. J. Lifestyle Med. 2014, 4, 34–38. [Google Scholar] [CrossRef] [PubMed]
- Bando, S.; Soeki, T.; Matsuura, T.; Tobiume, T.; Ise, T.; Kusunose, K.; Yamaguchi, K.; Yagi, S.; Fukuda, D.; Iwase, T.; et al. Plasma brain natriuretic peptide levels are elevated in patients with cancer. PLoS ONE 2017, 12, e0178607. [Google Scholar] [CrossRef] [PubMed]
- Götzinger, F.; Lauder, L.; Sharp, A.S.P.; Lang, I.M.; Rosenkranz, S.; Konstantinides, S.; Edelman, E.R.; Böhm, M.; Jaber, W.; Mahfoud, F. Interventional therapies for pulmonary embolism. Nat. Rev. Cardiol. 2023, 20, 670–684. [Google Scholar] [CrossRef]
- Toma, C.; Jaber, W.A.; Weinberg, M.D.; Bunte, M.C.; Khandhar, S.; Stegman, B.; Gondi, S.; Chambers, J.; Amin, R.; Leung, D.A.; et al. Acute outcomes for the full US cohort of the FLASH mechanical thrombectomy registry in pulmonary embolism. EuroIntervention 2023, 18, 1201–1212. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
| Cause | N, % |
|---|---|
| Infection | 27 (30.3) |
| Mass investigation Final diagnosis: Malignant Nonmalignant | 11 (12.4) 10 (11.3) 1 (1.1) |
| Surgery (includes all the surgical procedures except for surgery for cancer) | 11 (12.4) |
| Surgery for cancer | 5 (5.6) |
| Chemotherapy session | 2 (2.2) |
| Fracture (without surgery) | 8 (9.0) |
| Coronary artery disease (acute or chronic coronary syndrome) | 7 (7.9) |
| Acute heart failure | 3 (3,4) |
| Stroke | 5 (5.6) |
| Chronic obstructive pulmonary disease (exacerbation) | 2 (2.2) |
| Other | 8 (9.0) |
| Total | 89 (100) |
| Clinical Characteristics | IHPE | OHPE | |||||
|---|---|---|---|---|---|---|---|
| N | M (SD) | N | M (SD) | T | p | ||
| Age (years) | 89 | 71.35 (12.65) | 91 | 66.62 (15.75) | 2.222 | 0.028 | |
| BMI (kg/m2) | 89 | 27.94 (6.04) | 91 | 28.43 (5.43) | −0.576 | 0.566 | |
| N | Median (IQR) | N | Median (IQR) | M-W | p | ||
| Time of OSTD (hours) | 89 | 12 (20) | 91 | 72 (216) | 6460 | <0.001 | |
| N | % | N | % | Χ12 | p | ||
| History of smoking | Smoker | 21 | 41.2% | 30 | 58.8% | 2.008 | 0.399 |
| Ex-smoker | 9 | 50.0% | 9 | 50.0% | |||
| Non-smoker | 59 | 53.2% | 52 | 46.8% | |||
| ECG | Normal | 37 | 43.5% | 48 | 56.5% | 2.254 | 0.133 |
| Abnormal | 52 | 54.7% | 43 | 45.3% | |||
| Fever (>37.2 °C) | No | 73 | 49.0% | 76 | 51.0% | 0.070 | 0.791 |
| Yes | 16 | 51.6% | 15 | 48.4% | |||
| Dyspnoea | No | 35 | 47.3% | 39 | 52.7% | 0.232 | 0.630 |
| Yes | 54 | 50.9% | 52 | 49.1% | |||
| Chest pain | No | 78 | 59.1% | 54 | 40.9% | 18.427 | 0.001 |
| Yes | 11 | 22.9% | 37 | 77.1% | |||
| Lower limb pain | No | 87 | 52.1% | 80 | 47.9% | 6.503 | 0.011 |
| Yes | 2 | 15.4% | 11 | 84.6% | |||
| Syncope | No | 84 | 49.4% | 86 | 50.6% | 0.001 | 0.971 |
| Yes | 5 | 50.0% | 5 | 50.0% | |||
| Cough | No | 83 | 51.2% | 79 | 48.8% | 2.077 | 0.150 |
| Yes | 6 | 33.3% | 12 | 66.7% | |||
| Haemoptysis | No | 89 | 52.4% | 81 | 47.6% | 10.356 | 0.001 |
| Yes | 0 | 0% | 10 | 100% | |||
| On anticoagulation treatment | Νο | 56 | 41.2% | 80 | 58.8% | 15.215 | <0.001 |
| Yes | 33 | 75.0% | 11 | 25.0% | |||
| History of congestive heart failure or respiratory failure | No | 66 | 51.8% | 71 | 48.2% | 0.370 | 0.543 |
| Yes | 23 | 53.5% | 20 | 46.5% | |||
| Cancer | No | 61 | 44.9% | 75 | 55.1% | 8.849 | 0.012 |
| Yes | 25 | 71.4% | 10 | 28.6% | |||
| Cured | 3 | 33.3% | 6 | 66.7% | |||
| Major trauma/surgery | Νο | 68 | 44.7% | 84 | 55.3% | 10.012 | 0.002 |
| Yes | 21 | 77.8% | 6 | 22.2% | |||
| Previous VTE | Νο | 82 | 53.6% | 71 | 46.4% | 7.029 | 0.008 |
| Yes | 7 | 25.9% | 20 | 74.1% | |||
| Fracture of lower limb | Νο | 84 | 48.8% | 88 | 51.2% | 0.571 | 0.450 |
| Yes | 5 | 62.5% | 3 | 37.5% | |||
| Strong risk factor * | No | 54 | 48.2% | 58 | 51.8% | 1.423 | 0.491 |
| Yes | 35 | 51.5% | 33 | 48.5% | |||
| Moderate risk factor * | No | 12 | 34.3% | 23 | 65.7% | 3.994 | 0.046 |
| Yes | 77 | 53.1% | 68 | 46.9% | |||
| Weak risk factor * | No | 6 | 37.5% | 10 | 62.5% | 1.002 | 0.317 |
| Yes | 83 | 50.6% | 81 | 49.4% | |||
| Thrombolyis | No | 80 | 49.1% | 83 | 50.9% | 0.092 | 0.762 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ballas, C.; Lakkas, L.; Kardakari, O.; Papaioannou, E.; Siaravas, K.C.; Naka, K.K.; Michalis, L.K.; Katsouras, C.S. In-Hospital versus Out-of-Hospital Pulmonary Embolism: Clinical Characteristics, Biochemical Markers and Echocardiographic Indices. J. Cardiovasc. Dev. Dis. 2024, 11, 103. https://doi.org/10.3390/jcdd11040103
Ballas C, Lakkas L, Kardakari O, Papaioannou E, Siaravas KC, Naka KK, Michalis LK, Katsouras CS. In-Hospital versus Out-of-Hospital Pulmonary Embolism: Clinical Characteristics, Biochemical Markers and Echocardiographic Indices. Journal of Cardiovascular Development and Disease. 2024; 11(4):103. https://doi.org/10.3390/jcdd11040103
Chicago/Turabian StyleBallas, Christos, Lampros Lakkas, Olga Kardakari, Eftychia Papaioannou, Konstantinos C. Siaravas, Katerina K. Naka, Lampros K. Michalis, and Christos S. Katsouras. 2024. "In-Hospital versus Out-of-Hospital Pulmonary Embolism: Clinical Characteristics, Biochemical Markers and Echocardiographic Indices" Journal of Cardiovascular Development and Disease 11, no. 4: 103. https://doi.org/10.3390/jcdd11040103