
Progress in Cardiac Resynchronisation Therapy and Optimisation
 ,
,  ,
,
Abstract
:1. Introduction
2. Cardiac Resynchronisation
2.1. Cardiac Resynchronisation Therapy
2.2. Responders and Non-Responders
2.3. Measuring the Response to Resynchronisation
3. Optimisation
3.1. Echo Optimisation
3.2. Optimising Lead Position
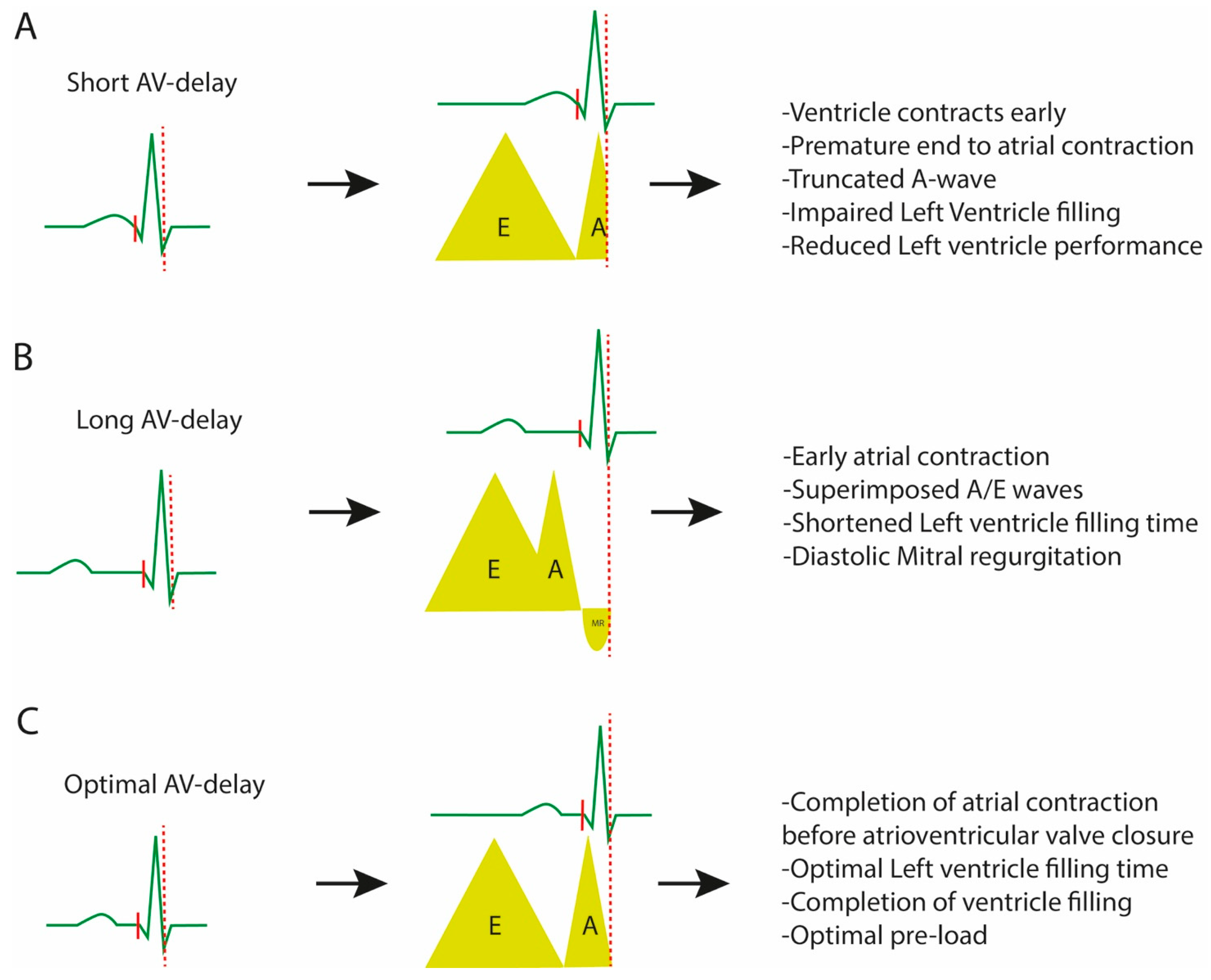
3.3. Optimising the Atrioventricular Interval
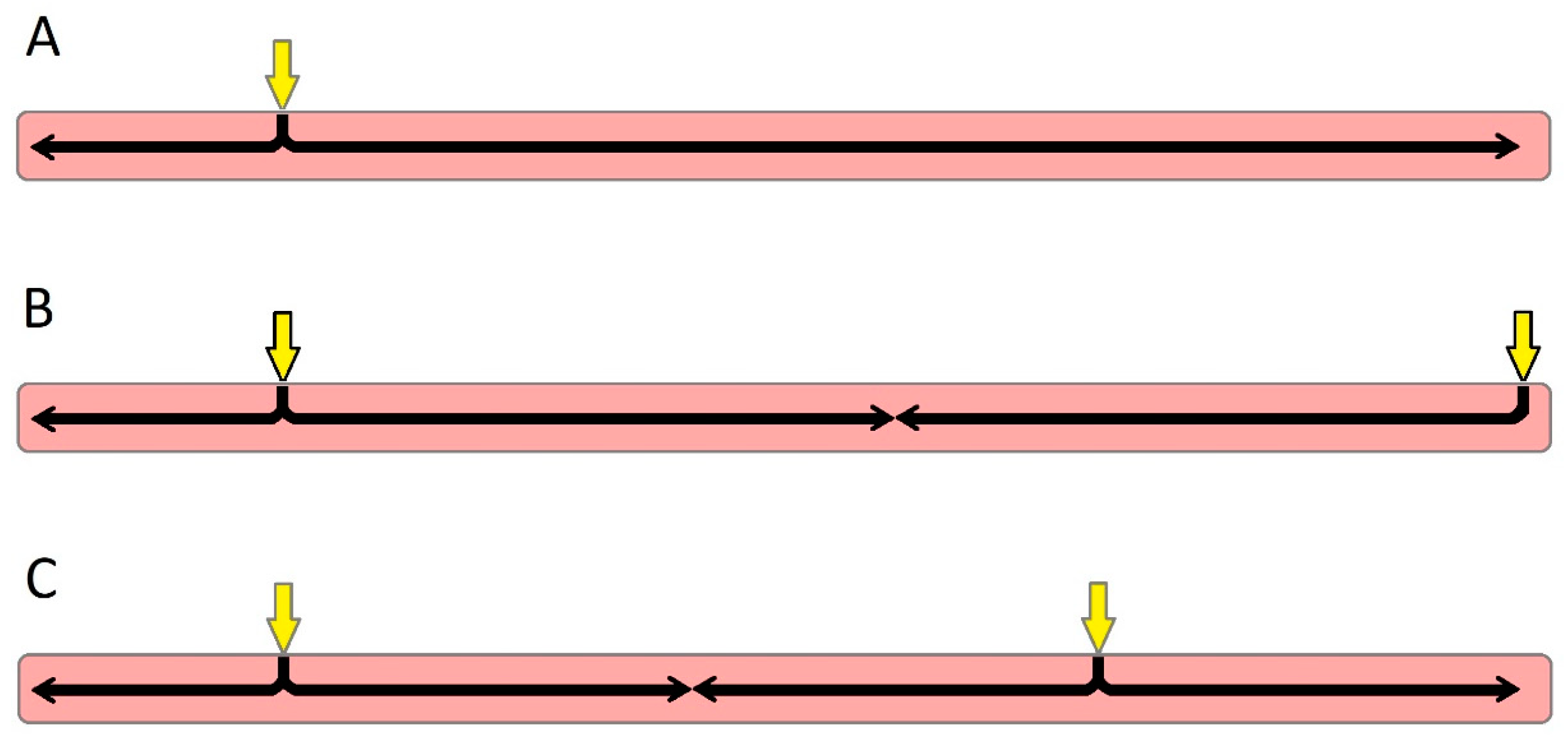
3.4. Optimising the Inter-Ventricular Interval
4. Device Optimisation
4.1. Multipoint Pacing
Optimising MPP
4.2. Adaptive Algorithms
4.2.1. AdaptivCRT

{kind=link}
{kind=link}
{kind=link}
| Method | Description | Comments | Studies |
|---|---|---|---|
| Non-echo guided | |||
| Surface ECG | VV interval: measurement of the narrowest QRS duration on surface ECG. | Simplest and widely available method. Can be combined with LVOT VTI measurements through echo. | Bertini et al. [53]: there was significant accordance with the echo-guided VV optimisation method. |
| Intracardiac Electrograms | AV/VV delay: estimated by the intrinsic interval delays during implantation. | Optimal VV delay= −0.333 × (RV − LV electrical delay) − 20 ms. | DECREASE-HF trial [59]: sequential BiV pacing with programmed LV and RV activation times in this way was similar to simultaneous BiV pacing. |
| Invasive LV dp/dtmax | AV/VV delay: measurement of LV dP/dt max by a 0.014-in sensor-tipped pressure guidewire. | Invasive method. Not applicable for routine clinical follow up. | Van Gelder et al. [54]: significantly increased LV dp/dt max compared with simultaneous BiV pacing. |
| Echo-guided | |||
| LVOT VTI method | AV/VV delay: optimal intervals correspond to the largest LVOT VTI. | Simple method. PW doppler used (in 20 ms steps) to determine optimal interval. | Bertini et al. [53]: Combined with surface ECG for a less-time optimisation approach. |
| Iterative method | AV delay: use of PW transmitral inflow to estimate maximal LV diastolic filling time. | No studies comparing this method to other optimising methods. | CARE-HF trial [18]: beneficial compared to medical treatments in terms of symptoms, quality of life and risk of death. |
| Ritter’s method | AV delay: use of two extreme delays (short and long) to determine the time between QRS onset and A-wave truncation. | Limited use in patients with a high HR or intrinsic AV interval < 150 ms. Validated only in patients with dual-chamber pacemakers and preserved LVEF. | Gold MR et al. [40]: inferior to electrogram-based optimisation. Melzer et al. [41]: good correlation with RNV in patients with an LVEF of <35%. Jansen AHM et al. [42]: no benefits observed in terms of invasive dp/dt max estimation. |
| Device-related | |||
| MPP-AS | MPP optimisation: programming MPP with a wide LV electrode anatomical separation and short timing interval. | Long-term (6 months) clinical outcomes of this optimisation algorithm are debatable. | MPP IDE trial [71]: programming to pace from distal poles (MPP-AS) presents better clinical outcomes and is more likely to convert non-responders to responders. MORE-CRT MPP study [72]: MPP-AS subgroup experienced higher conversion rates to responders compared to MPP-other. |
| AdaptivCRT® | VV delay: synchronises the intrinsic RV conduction with activated LV. AV delay: monitors and optimises the AV delay. | Patients in sinus rhythm, with normal intrinsic AV conduction. Facilitates resynchronisation during exercise. | Adaptive CRT trial [76]: aCRT algorithm is safe and as effective as BiV pacing with comprehensive echo optimisation. Shanmugam et al. [78]: rate-adaptive AV delay during exercise improved exercise times and VO2max. |
| CRT Autoadapt | AV/VV delay: by comparing A-RV and A-LV intervals, BiV pacing configuration is determined. | Optimal AV delay: the shortest of “70% A-RV” or “A-RV–40 ms”. Not for patients with a complete AV block. | Trial (NCT04774523) is in progress, and the estimated completion is 2024. |
| SyncAV® | AV delay: monitors the intrinsic AV interval (every 256 beats) and optimises AV settings accordingly. | Based on the concept that AV delay is dynamic and should constantly be adjusted to stress and exercise. | Varma et al. [79]: in patients with LBBB, the SyncAV algorithm resulted in a significant reduction of the GRS duration regardless of PR, LV-paced intervals or underlying ischemic disease. |
| SmartDelay (SD) | AV delay: electrogram-based algorithm. | Adjust AV delay to changes in hemodynamic conditions. | SMART-AV trial [74]: SD optimisation was not different from echo-determined AV optimisation or a fixed AV delay of 120 ms. |
| Peak Endocardial Acceleration Signals (PEAs) | AV/VV delay: contractility-guided optimisation, using a sensor at the tip of the lead. | Optimisation based on the correlation of these endocardial signals with the cardiac cycle and the LV dp/dt max | RESPOND-CRT trial [80]: AV and VV optimisation was safe and as effective as echo-guided optimisation in increasing the response to CRT. |
4.2.2. SyncAV
4.2.3. SmartDelay
4.2.4. CRT AutoAdapt
4.2.5. Peak Endocardial Acceleration Signals
5. Conduction System Pacing
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Taylor, C.J.; Ordóñez-Mena, J.M.; Roalfe, A.K.; Lay-Flurrie, S.; Jones, N.R.; Marshall, T.; Hobbs, F.D.R. Trends in survival after a diagnosis of heart failure in the United Kingdom 2000-2017: Population based cohort study. BMJ 2019, 364, l223. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Cardiovascular Outcomes Research (NICOR); Institute of Cardiovascular Science; University College London. National Heart Failure Audit Summary Report 2019. Available online: https://www.nicor.org.uk/wp-content/uploads/2019/09/Heart-Failure-2019-Report-final.pdf (accessed on 23 January 2021).
- McMurray, J.J.; Solomon, S.D.; Inzucchi, S.E.; Køber, L.; Kosiborod, M.N.; Martinez, F.A.; Ponikowski, P.; Sabatine, M.S.; Anand, I.S.; Bělohlávek, J.; et al. Dapagliflozin in Patients with Heart Failure and Reduced Ejection Fraction. N. Engl. J. Med. 2019, 381, 1995–2008. [Google Scholar] [CrossRef] [PubMed]
- The Consensus Trial Study Group. Effects of Enalapril on Mortality in Severe Congestive Heart Failure. N. Engl. J. Med. 1987, 316, 1429–1435. [Google Scholar] [CrossRef]
- Packer, M.; Bristow, M.R.; Cohn, J.N.; Colucci, W.S.; Fowler, M.B.; Gilbert, E.M.; Shusterman, N.H. The Effect of Carvedilol on Morbidity and Mortality in Patients with Chronic Heart Failure. N. Engl. J. Med. 1996, 334, 1349–1355. [Google Scholar] [CrossRef] [PubMed]
- Pitt, B.; Zannad, F.; Remme, W.J.; Cody, R.; Castaigne, A.; Perez, A.; Palensky, J.; Wittes, J. The Effect of Spironolactone on Morbidity and Mortality in Patients with Severe Heart Failure. N. Engl. J. Med. 1999, 341, 709–717. [Google Scholar] [CrossRef]
- Mcmurray, J.J.V.; Packer, M.; Desai, A.S.; Gong, J.; Lefkowitz, M.P.; Rizkala, A.R.; Rouleau, J.L.; Shi, V.C.; Solomon, S.D.; Swedberg, K.; et al. Angiotensin–Neprilysin Inhibition versus Enalapril in Heart Failure. PARADIGM-HF Investigators and Committees. N. Engl. J. Med. 2014, 371, 993–1004. [Google Scholar] [CrossRef]
- Smith, K.V.; Dunning, J.R.; Fischer, C.M.; Fera, L.E.; MacLean, T.E.; Bosque-Hamilton, J.W.; Matta, L.; Gaziano, T.A.; MacRae, C.A.; Scirica, B.M.; et al. Reasons for Failure to Optimize Guideline-Directed Medical Therapy for Heart Failure with Reduced Ejection Fraction Patients in Clinical Practice. J. Card. Fail. 2018, 24, S100–S101. [Google Scholar] [CrossRef]
- Nguyên, U.C.; Verzaal, N.J.; van Nieuwenhoven, F.A.; Vernooy, K.; Prinzen, F.W. Pathobiology of cardiac dyssynchrony and resynchronization therapy. Europace 2018, 20, 1898–1909. [Google Scholar] [CrossRef]
- Baldasseroni, S.; Opasich, C.; Gorini, M.; Lucci, D.; Marchionni, N.; Marini, M.; Campana, C.; Perini, G.; Deorsola, A.; Masotti, G.; et al. Left bundle-branch block is associated with increased 1-year sudden and total mortality rate in 5517 outpatients with congestive heart failure: A report from the Italian network on congestive heart failure. Am. Heart J. 2002, 143, 398–405. [Google Scholar] [CrossRef]
- Linde, C.; Ellenbogen, K.; McAlister, F.A. Cardiac resynchronization therapy (CRT): Clinical trials, guidelines, and target populations. Heart Rhythm. 2012, 9, S3–S13. [Google Scholar] [CrossRef]
- Grines, C.L.; Bashore, T.M.; Boudoulas, H.; Olson, S.; Shafer, P.; Wooley, C.F. Functional abnormalities in isolated left bundle branch block. The effect of interventricular asynchrony. Circulation 1989, 79, 845–853. [Google Scholar] [CrossRef]
- Derval, N.; Duchateau, J.; Mahida, S.; Eschalier, R.; Sacher, F.; Lumens, J.; Cochet, H.; Denis, A.; Pillois, X.; Yamashita, S.; et al. Distinctive Left Ventricular Activations Associated With ECG Pattern in Heart Failure Patients. Circ. Arrhythmia Electrophysiol. 2017, 10, e005073. [Google Scholar] [CrossRef] [PubMed]
- Leclercq, C.; Cazeau, S.; Ritter, P.; Alonso, C.; Gras, D.; Mabo, P.; Lazarus, A.; Daubert, J. A pilot experience with permanent biventricular pacing to treat advanced heart failure. Am. Heart J. 2000, 140, 862–870. [Google Scholar] [CrossRef]
- Abraham, W.T.; Fisher, W.G.; Smith, A.L.; Delurgio, D.B.; Leon, A.R.; Loh, E.; Kocovic, D.Z.; Packer, M.; Clavell, A.L.; Hayes, D.L.; et al. Cardiac Resynchronization in Chronic Heart Failure. N. Engl. J. Med. 2002, 346, 1845–1853. [Google Scholar] [CrossRef]
- Moss, A.J.; Hall, W.J.; Cannom, D.S.; Klein, H.; Brown, M.W.; Daubert, J.P.; Estes, N.M., III; Foster, E.; Greenberg, H.; Higgins, S.L.; et al. Cardiac-Resynchronization Therapy for the Prevention of Heart-Failure Events. N. Engl. J. Med. 2009, 361, 1329–1338. [Google Scholar] [CrossRef]
- Bristow, M.R.; Saxon, L.A.; Boehmer, J.; Krueger, S.; Kass, D.A.; De Marco, T.; Carson, P.; DiCarlo, L.; DeMets, D.; White, B.G.; et al. Cardiac-Resynchronization Therapy with or without an Implantable Defibrillator in Advanced Chronic Heart Failure. N. Engl. J. Med. 2004, 350, 2140–2150. [Google Scholar] [CrossRef]
- Cleland, J.G.F.; Daubert, J.C.; Erdmann, E.; Freemantle, N.; Gras, D.; Kappenberger, L.; Tavazzi, L. The Effect of Cardiac Resynchronization on Morbidity and Mortality in Heart Failure. N. Engl. J. Med. 2005, 352, 1539–1549. [Google Scholar] [CrossRef]
- Merkely, B.; Hatala, R.; Wranicz, J.K.; Duray, G.; Földesi, C.; Som, Z.; Németh, M.; Goscinska-Bis, K.; Gellér, L.; Zima, E.; et al. Upgrade of right ventricular pacing to cardiac resynchronisation therapy in heart failure: A randomised trial. Eur. Heart J. 2023; ahead of print. [Google Scholar] [CrossRef]
- Chung, E.S.; Katra, R.P.; Ghio, S.; Bax, J.; Gerritse, B.; Hilpisch, K.; Peterson, B.J.; Feldman, D.S.; Abraham, W.T. Cardiac resynchronization therapy may benefit patients with left ventricular ejection fraction >35%: A PROSPECT trial substudy. Eur. J. Heart Fail. 2010, 12, 581–587. [Google Scholar] [CrossRef] [PubMed]
- Hai, O.Y.; Mentz, R.J.; Zannad, F.; Gasparini, M.; De Ferrari, G.M.; Daubert, J.C.; Holzmeister, J.; Lam, C.S.; Pochet, T.; Vincent, A.; et al. Cardiac resynchronization therapy in heart failure patients with less severe left ventricular dysfunction: CRT in HF patients with less severe LV dysfunction. Eur. J. Heart Fail. 2015, 17, 135–143. [Google Scholar] [CrossRef] [PubMed]
- Bax, J.J.; Gorcsan, J. Echocardiography and Noninvasive Imaging in Cardiac Resynchronization Therapy: Results of the PROSPECT (Predictors of Response to Cardiac Resynchronization Therapy) Study in Perspective. J. Am. Coll. Cardiol. 2009, 53, 1933–1943. [Google Scholar] [CrossRef]
- Van Stipdonk, A.M.; Ter Horst, I.; Kloosterman, M.; Engels, E.B.; Rienstra, M.; Crijns, H.J.; Vos, M.A.; van Gelder, I.C.; Prinzen, F.W.; Meine, M.; et al. QRS Area Is a Strong Determinant of Outcome in Cardiac Resynchronization Therapy. Circ. Arrhythm. Electrophysiol. 2018, 11, e006497. [Google Scholar] [CrossRef]
- Maass, A.H.; Vernooy, K.; Wijers, S.C.; van’t Sant, J.; Cramer, M.J.; Meine, M.; Allaart, C.P.; De Lange, F.J.; Prinzen, F.W.; Gerritse, B.; et al. Refining success of cardiac resynchronization therapy using a simple score predicting the amount of reverse ventricular remodelling: Results from the Markers and Response to CRT (MARC) study. EP Eur. 2018, 20, e1–e10. [Google Scholar] [CrossRef] [PubMed]
- Mullens, W.; Grimm, R.A.; Verga, T.; Dresing, T.; Starling, R.C.; Wilkoff, B.L.; Tang, W.W. Insights From a Cardiac Resynchronization Optimization Clinic as Part of a Heart Failure Disease Management Program. J. Am. Coll. Cardiol. 2009, 53, 765–773. [Google Scholar] [CrossRef] [PubMed]
- van ’t Sant, J.; Mast, T.P.; Bos, M.M.; Ter Horst, I.A.; Van Everdingen, W.M.; Meine, M.; Cramer, M.J. Echo response and clinical outcome in CRT patients. Neth. Heart J. 2016, 24, 47–55. [Google Scholar] [CrossRef]
- Mathias, A.; Moss, A.J.; McNitt, S.; Zareba, W.; Goldenberg, I.; Solomon, S.D.; Kutyifa, V. Clinical Implications of Complete Left-Sided Reverse Remodeling with Cardiac Resynchronization Therapy: A MADIT-CRT Substudy. J. Am. Coll. Cardiol. 2016, 68, 1268–1276. [Google Scholar] [CrossRef] [PubMed]
- Kloosterman, M.; Rienstra, M.; Mulder, B.A.; Van Gelder, I.C.; Maass, A.H. Atrial reverse remodelling is associated with outcome of cardiac resynchronization therapy. Europace 2016, 18, 1211–1219. [Google Scholar] [CrossRef]
- Chung, E.S.; Leon, A.R.; Tavazzi, L.; Sun, J.-P.; Nihoyannopoulos, P.; Merlino, J.; Abraham, W.T.; Ghio, S.; Leclercq, C.; Bax, J.J.; et al. Results of the Predictors of Response to CRT (PROSPECT) Trial. Circulation 2008, 117, 2608–2616. [Google Scholar] [CrossRef]
- Bogaard, M.D.; Houthuizen, P.; Bracke, F.A.; Doevendans, P.A.; Prinzen, F.W.; Meine, M.; van Gelder, B.M. Baseline left ventricular dP/dtmax rather than the acute improvement in dP/dtmax predicts clinical outcome in patients with cardiac resynchronization therapy. Eur. J. Heart Fail. 2011, 13, 1126–1132. [Google Scholar] [CrossRef]
- Boe, E.; Smiseth, O.A.; Storsten, P.; Andersen, O.S.; Aalen, J.; Eriksen, M.; Krogh, M.R.; Kongsgaard, E.; Remme, E.W.; Skulstad, H. Left ventricular end-systolic volume is a more sensitive marker of acute response to cardiac resynchronization therapy than contractility indices: Insights from an experimental study. Europace 2019, 21, 347–355. [Google Scholar] [CrossRef]
- Bittner, V.; Weiner, D.H.; Yusuf, S.; Rogers, W.J.; Mcintyre, K.M.; Bangdiwala, S.I.; Kronenberg, M.W.; Kostis, J.B.; Kohn, R.M.; Guillotte, M.; et al. Prediction of mortality and morbidity with a 6-minute walk test in patients with left ventricular dysfunction. SOLVD Investigators. JAMA 1993, 270, 1702–1707. [Google Scholar] [CrossRef]
- Faggiano, P.; D’Aloia, A.; Gualeni, A.; Brentana, L.; Cas, L.D. The 6 minute walking test in chronic heart failure: Indications, interpretation and limitations from a review of the literature. Eur. J. Heart Fail. 2004, 6, 687–691. [Google Scholar] [CrossRef] [PubMed]
- Lucas, C.; Stevenson, L.W.; Johnson, W.; Hartley, H.; Hamilton, M.A.; Walden, J.; Lem, V.; Eagen-Bengsten, E. The 6-min walk and peak oxygen consumption in advanced heart failure: Aerobic capacity and survival. Am. Heart J. 1999, 138, 618–624. [Google Scholar] [CrossRef] [PubMed]
- Packer, M. Proposal for a new clinical end point to evaluate the efficacy of drugs and devices in the treatment of chronic heart failure. J. Card. Fail. 2001, 7, 176–182. [Google Scholar] [CrossRef]
- Morales, M.-A.; Startari, U.; Panchetti, L.; Rossi, A.; Piacenti, M. Atrioventricular Delay Optimization by Doppler-Derived Left Ventricular dP/dt Improves 6-Month Outcome of Resynchronized Patients. Pacing Clin. Electrophysiol. 2006, 29, 564–568. [Google Scholar] [CrossRef]
- Antonini, L.; Auriti, A.; Pasceri, V.; Meo, A.; Pristipino, C.; Varveri, A.; Greco, S.; Santini, M. Optimization of the atrioventricular delay in sequential and biventricular pacing: Physiological bases, critical review, and new purposes. Europace 2012, 14, 929–938. [Google Scholar] [CrossRef]
- Kedia, N.; Ng, K.; Apperson-Hansen, C.; Wang, C.; Tchou, P.; Wilkoff, B.L.; Grimm, R.A. Usefulness of Atrioventricular Delay Optimization Using Doppler Assessment of Mitral Inflow in Patients Undergoing Cardiac Resynchronization Therapy. Am. J. Cardiol. 2006, 98, 780–785. [Google Scholar] [CrossRef]
- Ritter, P.; Lelieve, T.; Lavergne, T. Quick determination of the optimal AV delay at rest in patients paced in DDD mode for complete AVblock. Eur. J. Card. Pacing Electrophysiol. 1994, 4, P54. [Google Scholar]
- Gold, M.R.; Niazi, I.; Giudici, M.; Leman, R.B.; Sturdivant, J.L.; Kim, M.H.; Yu, Y.; Ding, J.; Waggoner, A.D. A Prospective Comparison of AV Delay Programming Methods for Hemodynamic Optimization during Cardiac Resynchronization Therapy. J. Cardiovasc. Electrophysiol. 2007, 18, 490–496. [Google Scholar] [CrossRef]
- Melzer, C.; Borges, A.; Knebel, F.; Richter, W.; Combs, W.; Baumann, G.; Theres, H. Echocardiographic AV-interval optimization in patients with reduced left ventricular function. Cardiovasc. Ultrasound 2004, 2, 30. [Google Scholar] [CrossRef]
- Jansen, A.H.; Bracke, F.A.; van Dantzig, J.M.; Meijer, A.; van der Voort, P.H.; Aarnoudse, W.; van Gelder, B.M.; Peels, K.H. Correlation of Echo-Doppler Optimization of Atrioventricular Delay in Cardiac Resynchronization Therapy with Invasive Hemodynamics in Patients With Heart Failure Secondary to Ischemic or Idiopathic Dilated Cardiomyopathy. Am. J. Cardiol. 2006, 97, 552–557. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Birgersdotter-Green, U.; Singh, J.P.; Ellenbogen, K.A.; Yu, Y.; Meyer, T.E.; Seth, M.; Tchou, P.J. The relationship between ventricular electrical delay and left ventricular remodelling with cardiac resynchronization therapy. Eur. Heart J. 2011, 32, 2516–2524. [Google Scholar] [CrossRef]
- Khan, F.Z.; Virdee, M.S.; Palmer, C.R.; Pugh, P.J.; O’Halloran, D.; Elsik, M.; Read, P.A.; Begley, D.; Fynn, S.P.; Dutka, D.P. Targeted Left Ventricular Lead Placement to Guide Cardiac Resynchronization Therapy: The TARGET Study: A Randomized, Controlled Trial. J. Am. Coll. Cardiol. 2012, 59, 1509–1518. [Google Scholar] [CrossRef]
- Saba, S.; Marek, J.; Schwartzman, D.; Jain, S.; Adelstein, E.; White, P.; Oyenuga, O.A.; Onishi, T.; Soman, P.; Gorcsan, J., III. Echocardiography-Guided Left Ventricular Lead Placement for Cardiac Resynchronization Therapy: Results of the Speckle Tracking Assisted Resynchronization Therapy for Electrode Region Trial. Circ. Heart Fail. 2013, 6, 427–434. [Google Scholar] [CrossRef]
- de Maat, G.E.; Mulder, B.A.; Van de Lande, M.E.; Rama, R.S.; Rienstra, M.; Mariani, M.A.; Maass, A.H.; Klinkenberg, T.J. Long-Term Performance of Epicardial versus Transvenous Left Ventricular Leads for Cardiac Resynchronization Therapy. J. Clin. Med. 2023, 12, 5766. [Google Scholar] [CrossRef]
- Parreira, L.; Tsyganov, A.; Artyukhina, E.; Vernooy, K.; Tondo, C.; Adragao, P.; Ascione, C.; Carmo, P.; Carvalho, S.; Egger, M.; et al. Non-invasive three-dimensional electrical activation mapping to predict cardiac resynchronization therapy response: Site of latest left ventricular activation relative to pacing site. Europace 2023, 25, 1458–1466. [Google Scholar] [CrossRef]
- Wouters, P.C.; Vernooy, K.; Cramer, M.J.; Prinzen, F.W.; Meine, M. Optimizing lead placement for pacing in dyssynchronous heart failure: The patient in the lead. Heart Rhythm. 2021, 18, 1024–1032. [Google Scholar] [CrossRef]
- Elliott, M.K.; Strocchi, M.; Sieniewicz, B.J.; Mehta, V.; Wijesuriya, N.; Devere, F.; Howell, S.; Thorpe, A.; Martic, D.; Bishop, M.J.; et al. Left bundle branch area pacing reduces epicardial dispersion of repolarization compared with biventricular cardiac resynchronization therapy. Heart Rhythm. 2023, in press. [Google Scholar] [CrossRef]
- Sohal, M.; Shetty, A.; Duckett, S.; Chen, Z.; Sammut, E.; Amraoui, S.; Carr-White, G.; Razavi, R.; Rinaldi, C.A. Noninvasive Assessment of LV Contraction Patterns Using CMR to Identify Responders to CRT. JACC Cardiovasc. Imaging 2013, 6, 864–873. [Google Scholar] [CrossRef]
- Stanton, T.; Hawkins, N.M.; Hogg, K.J.; Goodfield, N.E.R.; Petrie, M.C.; McMurray, J.J.V. How should we optimize cardiac resynchronization therapy? Eur. Heart J. 2008, 29, 2458–2472. [Google Scholar] [CrossRef]
- Brecker, S.; Xiao, H.; Sparrow, J.; Gibson, D. Effects of dual-chamber pacing with short atrioventricular delay in dilated cardiomyopathy. Lancet 1992, 340, 1308–1312. [Google Scholar] [CrossRef]
- Bertini, M.; Delgado, V.; Bax, J.J.; Van de Veire, N.R.L. Why, how and when do we need to optimize the setting of cardiac resynchronization therapy? Europace 2009, 11 (Suppl. S5), v46–v57. [Google Scholar] [CrossRef] [PubMed]
- van Gelder, B.M.; Bracke, F.A.; Meijer, A.; Lakerveld, L.J.M.; Pijls, N.H.J. Effect of optimizing the VV interval on left ventricular contractility in cardiac resynchronization therapy. Am. J. Cardiol. 2004, 93, 1500–1503. [Google Scholar] [CrossRef]
- Houthuizen, P.; Bracke, F.A.; van Gelder, B.M. Atrioventricular and interventricular delay optimization in cardiac resynchronization therapy: Physiological principles and overview of available methods. Heart Fail. Rev. 2011, 16, 263–276. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.; Malik, M.; Dinerman, J.; Lee, J.; Petrutiu, S.; Khoo, M. VV optimization in cardiac resynchronization therapy non-responders: RESPONSE-HF trial results. Heart Rhythm. 2010, 7, S26. [Google Scholar]
- Perego, G.B.; Chianca, R.; Facchini, M.; Frattola, A.; Balla, E.; Zucchi, S.; Cavaglià, S.; Vicini, I.; Negretto, M.; Osculati, G. Simultaneous vs. sequential biventricular pacing in dilated cardiomyopathy: An acute hemodynamic study. Eur. J. Heart Fail. 2003, 5, 305–313. [Google Scholar] [CrossRef]
- Sogaard, P.; Egeblad, H.; Pedersen, A.K.; Kim, W.Y.; Kristensen, B.Ø.; Hansen, P.S.; Mortensen, P.T. Sequential Versus Simultaneous Biventricular Resynchronization for Severe Heart Failure: Evaluation by Tissue Doppler Imaging. Circulation 2002, 106, 2078–2084. [Google Scholar] [CrossRef]
- Rao, R.K.; Kumar, U.N.; Schafer, J.; Viloria, E.; De Lurgio, D.; Foster, E. Reduced ventricular volumes and improved systolic function with cardiac resynchronization therapy: A randomized trial comparing simultaneous biventricular pacing, sequential biventricular pacing, and left ventricular pacing. Circulation 2007, 115, 2136–2144. [Google Scholar] [CrossRef]
- Rinaldi, C.A.; Burri, H.; Thibault, B.; Curnis, A.; Rao, A.; Gras, D.; Sperzel, J.; Singh, J.P.; Biffi, M.; Bordachar, P.; et al. A review of multisite pacing to achieve cardiac resynchronization therapy. Europace 2015, 17, 7–17. [Google Scholar] [CrossRef]
- Auricchio, A.; Fantoni, C.; Regoli, F.; Carbucicchio, C.; Goette, A.; Geller, C.; Kloss, M.; Klein, H. Characterization of Left Ventricular Activation in Patients with Heart Failure and Left Bundle-Branch Block. Circulation 2004, 109, 1133–1139. [Google Scholar] [CrossRef]
- Leclercq, C.; Gadler, F.; Kranig, W.; Ellery, S.; Gras, D.; Lazarus, A.; Clémenty, J.; Boulogne, E.; Daubert, J.-C. A Randomized Comparison of Triple-Site Versus Dual-Site Ventricular Stimulation in Patients with Congestive Heart Failure. J. Am. Coll. Cardiol. 2008, 51, 1455–1462. [Google Scholar] [CrossRef]
- Bordachar, P.; Gras, D.; Clementy, N.; Defaye, P.; Mondoly, P.; Boveda, S.; Anselme, F.; Klug, D.; Piot, O.; Sadoul, N.; et al. Clinical impact of an additional left ventricular lead in cardiac resynchronization therapy nonresponders: The V3 trial. Heart Rhythm. 2018, 15, 870–876. [Google Scholar] [CrossRef]
- Shetty, A.K.; Duckett, S.G.; Bostock, J.; Rosenthal, E.; Rinaldi, C.A. Use of a quadripolar left ventricular lead to achieve successful implantation in patients with previous failed attempts at cardiac resynchronization therapy. Europace 2011, 13, 992–996. [Google Scholar] [CrossRef]
- Sperzel, J.; Dänschel, W.; Gutleben, K.-J.; Kranig, W.; Mortensen, P.; Connelly, D.; Trappe, H.-J.; Seidl, K.; Duray, G.; Pieske, B.; et al. First prospective, multi-centre clinical experience with a novel left ventricular quadripolar lead. Europace 2012, 14, 365–372. [Google Scholar] [CrossRef] [PubMed]
- Ohlow, M.-A.; Lauer, B.; Brunelli, M.; Daralammouri, Y.; Geller, J.C. The Use of a Quadripolar Left Ventricular Lead Increases Successful Implantation Rates in Patients with Phrenic Nerve Stimulation and/or High Pacing Thresholds Undergoing Cardiac Resynchronisation Therapy with Conventional Bipolar Leads. Indian Pacing Electrophysiol. J. 2013, 13, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Thibault, B.; Dubuc, M.; Khairy, P.; Guerra, P.G.; Macle, L.; Rivard, L.; Roy, D.; Talajic, M.; Karst, E.; Ryu, K.; et al. Acute haemodynamic comparison of multisite and biventricular pacing with a quadripolar left ventricular lead. Europace 2013, 15, 984–991. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Ćalović, Ž; Vicedomini, G.; Cuko, A.; McSpadden, L.C.; Ryu, K.; Romano, E.; Saviano, M.; Baldi, M.; Pappone, A.; et al. Multipoint left ventricular pacing improves acute hemodynamic response assessed with pressure-volume loops in cardiac resynchronization therapy patients. Heart Rhythm. 2014, 11, 394–401. [Google Scholar] [CrossRef]
- Forleo, G.B.; Santini, L.; Giammaria, M.; Potenza, D.; Curnis, A.; Calabrese, V.; Ricciardi, D.; D’Agostino, C.; Notarstefano, P.; Ribatti, V.; et al. Multipoint pacing via a quadripolar left-ventricular lead: Preliminary results from the Italian registry on multipoint left-ventricular pacing in cardiac resynchronization therapy (IRON-MPP). Europace 2016, 19, 1170–1177. [Google Scholar] [CrossRef] [PubMed]
- Sohal, M.; Shetty, A.; Niederer, S.; Lee, A.; Chen, Z.; Jackson, T.; Behar, J.M.; Claridge, S.; Bostock, J.; Hyde, E.; et al. Mechanistic insights into the benefits of multisite pacing in cardiac resynchronization therapy: The importance of electrical substrate and rate of left ventricular activation. Heart Rhythm. 2015, 12, 2449–2457. [Google Scholar] [CrossRef]
- Niazi, I.; Baker, J.; Corbisiero, R.; Love, C.; Martin, D.; Sheppard, R.; Worley, S.J.; Varma, N.; Lee, K.; Tomassoni, G.; et al. Safety and Efficacy of Multipoint Pacing in Cardiac Resynchronization Therapy. JACC Clin. Electrophysiol. 2017, 3, 1510–1518. [Google Scholar] [CrossRef]
- Leclercq, C.; Burri, H.; Curnis, A.; Delnoy, P.P.; Rinaldi, C.A.; Sperzel, J.; Lee, K.; Calò, L.; Vicentini, A.; Concha, J.F.; et al. Cardiac resynchronization therapy non-responder to responder conversion rate in the more response to cardiac resynchronization therapy with MultiPoint Pacing (MORE-CRT MPP) study: Results from Phase I. Eur. Heart J. 2019, 40, 2979–2987. [Google Scholar] [CrossRef]
- Delnoy, P.P.; Ritter, P.; Naegele, H.; Orazi, S.; Szwed, H.; Zupan, I.; Goscinska-Bis, K.; Anselme, F.; Martino, M.; Padeletti, L. Association between frequent cardiac resynchronization therapy optimization and long-term clinical response: A post hoc analysis of the Clinical Evaluation on Advanced Resynchronization (CLEAR) pilot study. Europace 2013, 15, 1174–1181. [Google Scholar] [CrossRef]
- Ellenbogen, K.A.; Gold, M.R.; Meyer, T.E.; Lozano, I.F.; Mittal, S.; Waggoner, A.D.; Lemke, B.; Singh, J.P.; Spinale, F.G.; Van Eyk, J.E.; et al. Response to Letter Regarding Article, “Primary Results From the SmartDelay Determined AV Optimization: A Comparison to Other AV Delay Methods Used in Cardiac Resynchronization Therapy (SMART-AV) Trial: A Randomized Trial Comparing Empirical, Echocardiography-Guided and Algorithmic Atrioventricular Delay Programming in Cardiac Resynchronization Therapy”. Circulation 2010, 124, e191–e192. [Google Scholar] [CrossRef]
- Filippatos, G.; Birnie, D.; Gold, M.R.; Gerritse, B.; Hersi, A.; Jacobs, S.; Kusano, K.; Leclercq, C.; Mullens, W.; Wilkoff, B.L.; et al. Rationale and design of the AdaptResponse trial: A prospective randomized study of cardiac resynchronization therapy with preferential adaptive left ventricular-only pacing: Rationale and design of the AdaptResponse trial. Eur. J. Heart Fail. 2017, 19, 950–957. [Google Scholar] [CrossRef]
- Martin, D.O.; Lemke, B.; Birnie, D.; Krum, H.; Lee, K.L.-F.; Aonuma, K.; Gasparini, M.; Starling, R.C.; Milasinovic, G.; Rogers, T.; et al. Investigation of a novel algorithm for synchronized left-ventricular pacing and ambulatory optimization of cardiac resynchronization therapy: Results of the adaptive CRT trial. Heart Rhythm. 2012, 9, 1807–1814.e1. [Google Scholar] [CrossRef] [PubMed]
- Birnie, D.; Lemke, B.; Aonuma, K.; Krum, H.; Lee, K.L.-F.; Gasparini, M.; Starling, R.C.; Milasinovic, G.; Gorcsan, J.; Houmsse, M.; et al. Clinical outcomes with synchronized left ventricular pacing: Analysis of the adaptive CRT trial. Heart Rhythm. 2013, 10, 1368–1374. [Google Scholar] [CrossRef] [PubMed]
- Shanmugam, N.; Prada-Delgado, O.; Campos, A.G.; Grimster, A.; Valencia, O.; Baltabaeva, A.; Jones, S.; Anderson, L. Rate-adaptive AV delay and exercise performance following cardiac resynchronization therapy. Heart Rhythm. 2012, 9, 1815–1821.e1. [Google Scholar] [CrossRef] [PubMed]
- Varma, N.; O’Donnell, D.; Bassiouny, M.; Ritter, P.; Pappone, C.; Mangual, J.; Cantillon, D.; Badie, N.; Thibault, B.; Wisnoskey, B. Programming Cardiac Resynchronization Therapy for Electrical Synchrony: Reaching Beyond Left Bundle Branch Block and Left Ventricular Activation Delay. J. Am. Heart Assoc. 2018, 7, e007489. [Google Scholar] [CrossRef]
- Brugada, J.; Delnoy, P.P.; Brachmann, J.; Reynolds, D.; Padeletti, L.; Noelker, G.; Kantipudi, C.; Lopez, J.M.R.; Dichtl, W.; Borri-Brunetto, A.; et al. Contractility sensor-guided optimization of cardiac resynchronization therapy: Results from the RESPOND-CRT trial. Eur. Heart J. 2016, 38, 730–738. [Google Scholar] [CrossRef]
- Thibault, B.; Ritter, P.; Bode, K.; Calò, L.; Mondésert, B.; Mangual, J.O.; Badie, N.; McSpadden, L.C.; Pappone, C.; Varma, N. Dynamic programming of atrioventricular delay improves electrical synchrony in a multicenter cardiac resynchronization therapy study. Heart Rhythm. 2019, 16, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Gold, M.R.; Ellenbogen, K.; Leclercq, C.; Lowy, J.; Rials, S.; Shoda, M.; Tomassoni, G.; Issa, Z.; Sarrazin, J.-F.; Jennings, J.; et al. Effects of Atrioventricular Optimization on Left Ventricular Reverse Remodeling With Cardiac Resynchronization Therapy: Results of the SMART-CRT Trial. Circ. Arrhythmia Electrophysiol. 2023, 16, 313–324. [Google Scholar] [CrossRef]
- Kloosterman, M.; Daniëls, F.; Roseboom, E.; Rienstra, M.; Maass, A.H. Cardiac Resynchronization Therapy beyond Nominal Settings: An IEGM-Based Approach for Paced and Sensed Atrioventricular Delay Offset Optimization in Daily Clinical Practice. J. Clin. Med. 2023, 12, 4138. [Google Scholar] [CrossRef]
- Rickards, A.F.; Bombardini, T.; Corbucci, G.; Plicchi, G.; Multicenter PEA Study Group. An Implantable Intracardiac Accelerometer for Monitoring Myocardial Contractility. Pacing Clin. Electrophysiol. 1996, 19, 2066–2071. [Google Scholar] [CrossRef]
- Tassin, A.; Kobeissi, A.; Vitali, L.; Rouleau, F.; Ritter, P.; Gaggini, G.; Dupuis, J.-M. Relationship between Amplitude and Timing of Heart Sounds and Endocardial Acceleration. Pacing Clin. Electrophysiol. 2009, 32, S101–S104. [Google Scholar] [CrossRef]
- Sweeney, M.O. Peak Endocardial Acceleration Signals for Atrial Mechanical Activation. J. Cardiovasc. Electrophysiol. 2011, 22, 584–586. [Google Scholar] [CrossRef]
- Deshmukh, P.; Casavant, D.A.; Romanyshyn, M.; Anderson, K. Permanent, Direct His-Bundle Pacing: A Novel Approach to Cardiac Pacing in Patients With Normal His-Purkinje Activation. Circulation 2000, 101, 869–877. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Su, L.; Wu, S.; Xu, L.; Xiao, F.; Zhou, X.; Mao, G.; Vijayaraman, P.; Ellenbogen, K.A. Long-term outcomes of His bundle pacing in patients with heart failure with left bundle branch block. Heart 2019, 105, 137–143. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.; Wu, S.; Vijayaraman, P.; Su, L.; Chen, X.; Cai, B.; Zou, J.; Lan, R.; Fu, G.; Mao, G.; et al. Cardiac Resynchronization Therapy in Patients With Nonischemic Cardiomyopathy Using Left Bundle Branch Pacing. JACC Clin. Electrophysiol. 2020, 6, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhu, H.; Hou, X.; Wang, Z.; Zou, F.; Qian, Z.; Wei, Y.; Wang, X.; Zhang, L.; Li, X.; et al. Randomized Trial of Left Bundle Branch vs Biventricular Pacing for Cardiac Resynchronization Therapy. J. Am. Coll. Cardiol. 2022, 80, 1205–1216. [Google Scholar] [CrossRef]
- Chen, X.; Ye, Y.; Wang, Z.; Jin, Q.; Qiu, Z.; Wang, J.; Qin, S.; Bai, J.; Wang, W.; Liang, Y.; et al. Cardiac resynchronization therapy via left bundle branch pacing vs. optimized biventricular pacing with adaptive algorithm in heart failure with left bundle branch block: A prospective, multi-centre, observational study. Europace 2022, 24, 807–816. [Google Scholar] [CrossRef] [PubMed]



Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Akhtar, Z.; Gallagher, M.M.; Kontogiannis, C.; Leung, L.W.M.; Spartalis, M.; Jouhra, F.; Sohal, M.; Shanmugam, N. Progress in Cardiac Resynchronisation Therapy and Optimisation. J. Cardiovasc. Dev. Dis. 2023, 10, 428. https://doi.org/10.3390/jcdd10100428
Akhtar Z, Gallagher MM, Kontogiannis C, Leung LWM, Spartalis M, Jouhra F, Sohal M, Shanmugam N. Progress in Cardiac Resynchronisation Therapy and Optimisation. Journal of Cardiovascular Development and Disease. 2023; 10(10):428. https://doi.org/10.3390/jcdd10100428
Chicago/Turabian StyleAkhtar, Zaki, Mark M. Gallagher, Christos Kontogiannis, Lisa W. M. Leung, Michael Spartalis, Fadi Jouhra, Manav Sohal, and Nesan Shanmugam. 2023. "Progress in Cardiac Resynchronisation Therapy and Optimisation" Journal of Cardiovascular Development and Disease 10, no. 10: 428. https://doi.org/10.3390/jcdd10100428