
Postoperative Weight Gain within Enhanced Recovery after Cardiac Surgery
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Pre-and Intraoperative Management
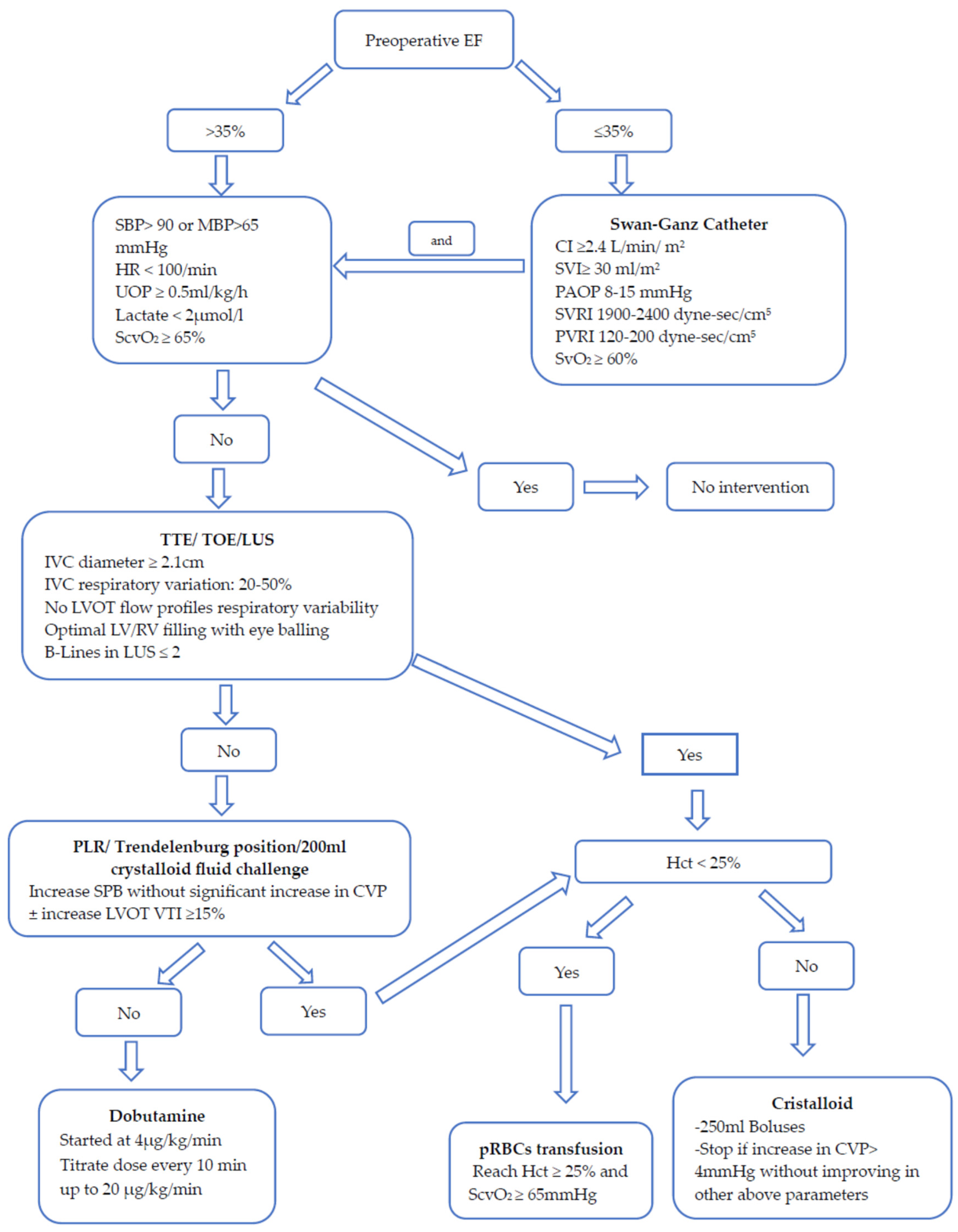
2.2. Perioperative Fluid Management
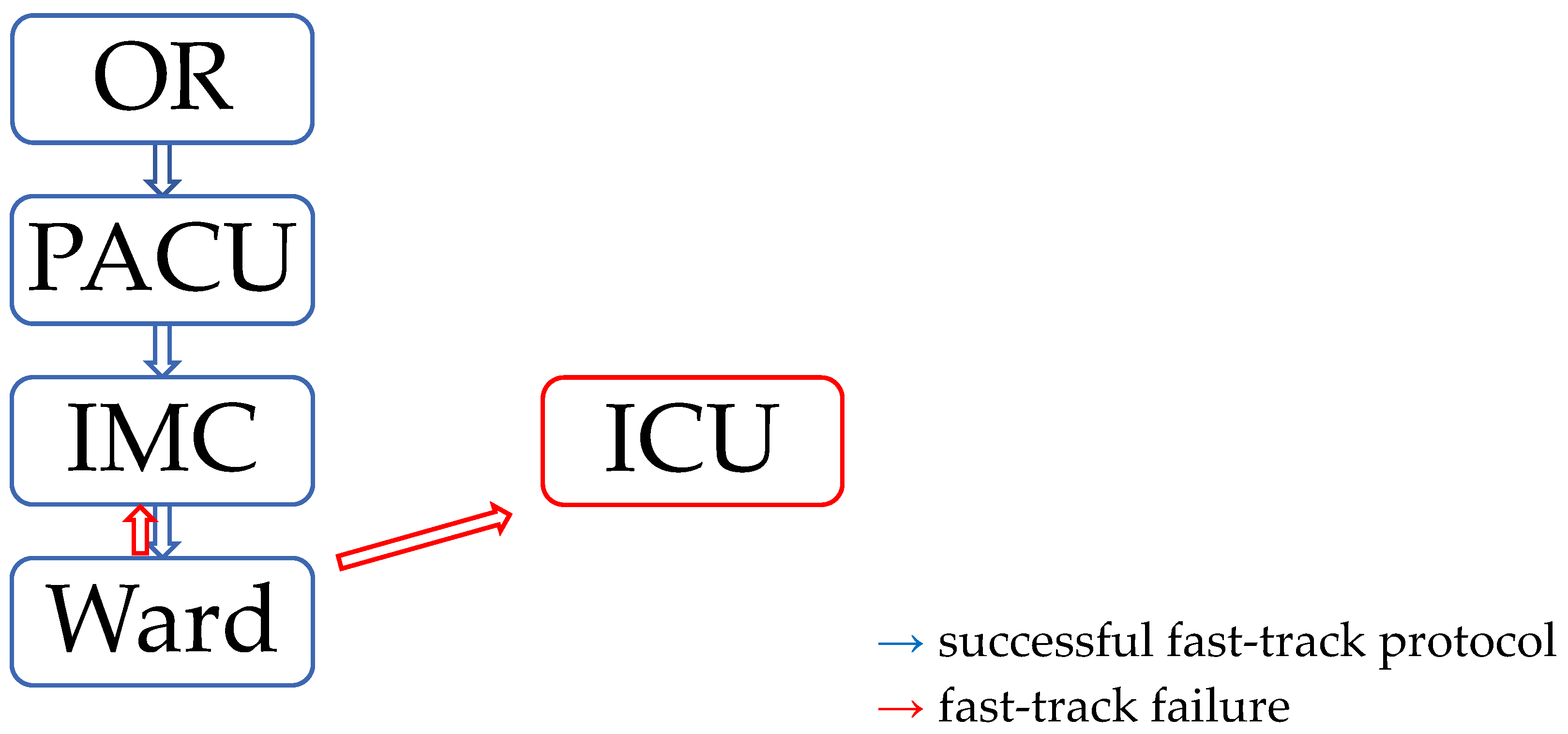
2.3. Postanesthetic Care Unit (PACU) and Intermediate Care Unit (IMC) Management
2.4. ERACS Protocol
2.5. Variables
2.6. Statistical Analysis
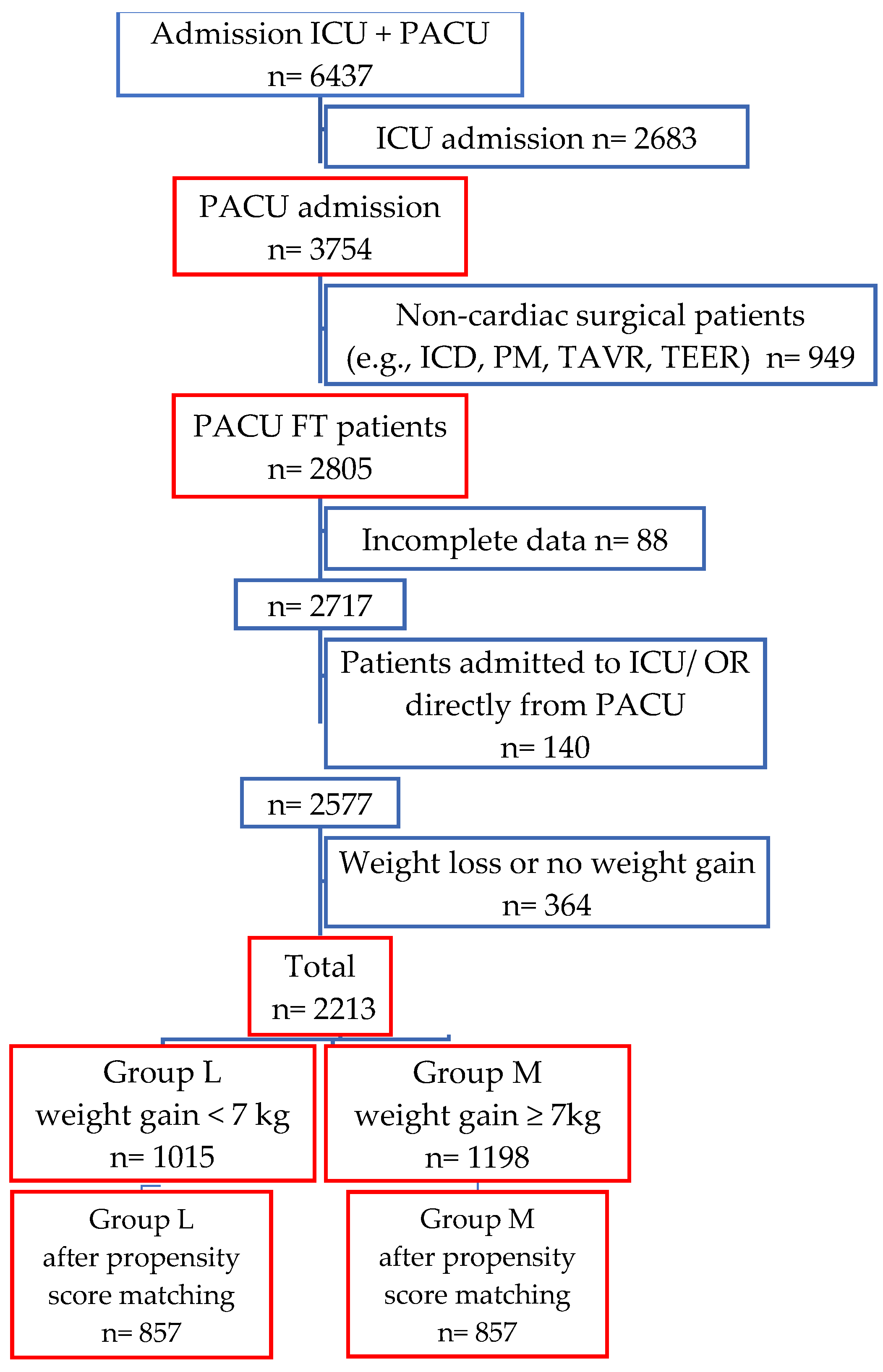
3. Results
3.1. Weight Gain vs. Fluid Balance
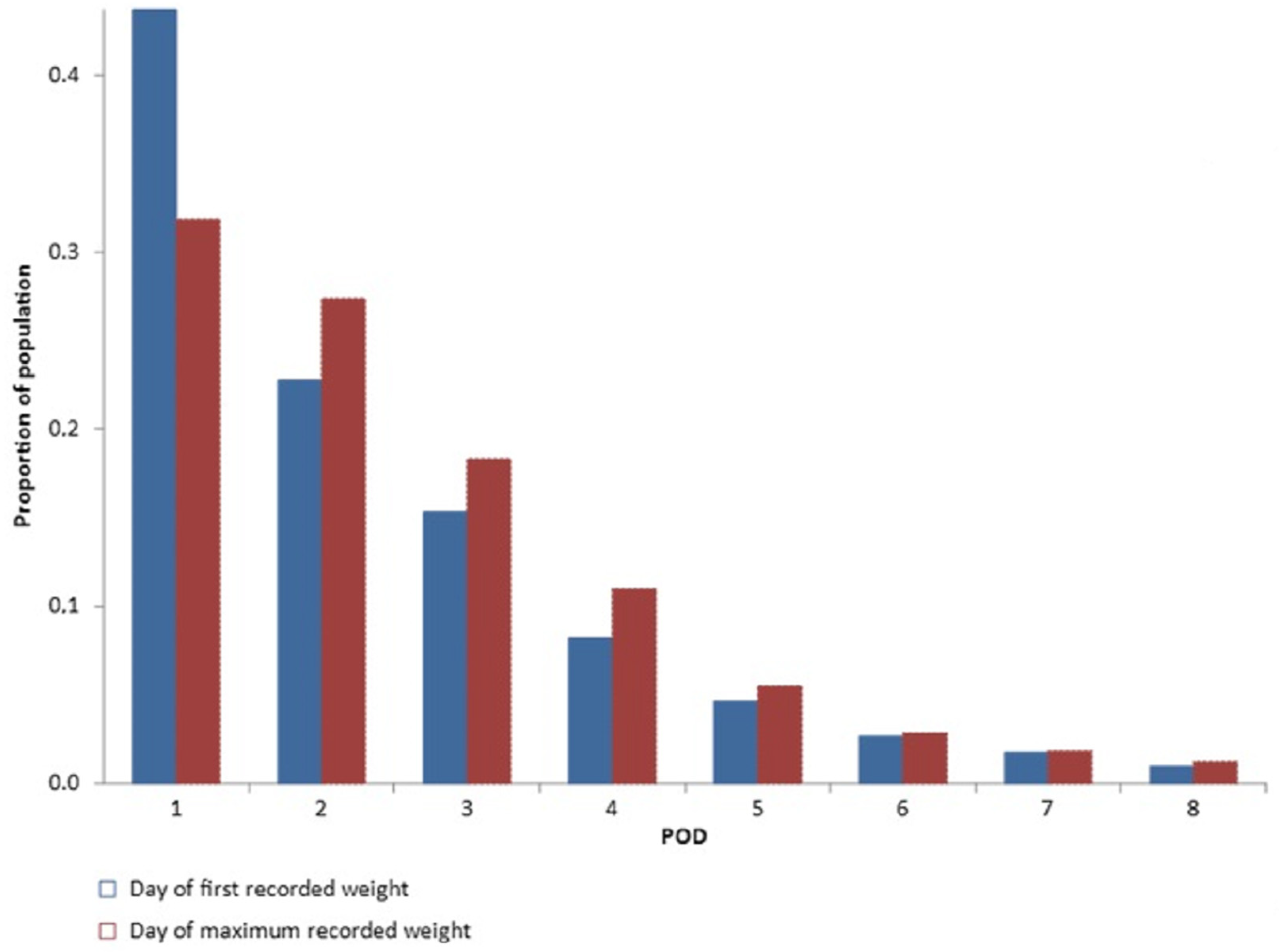
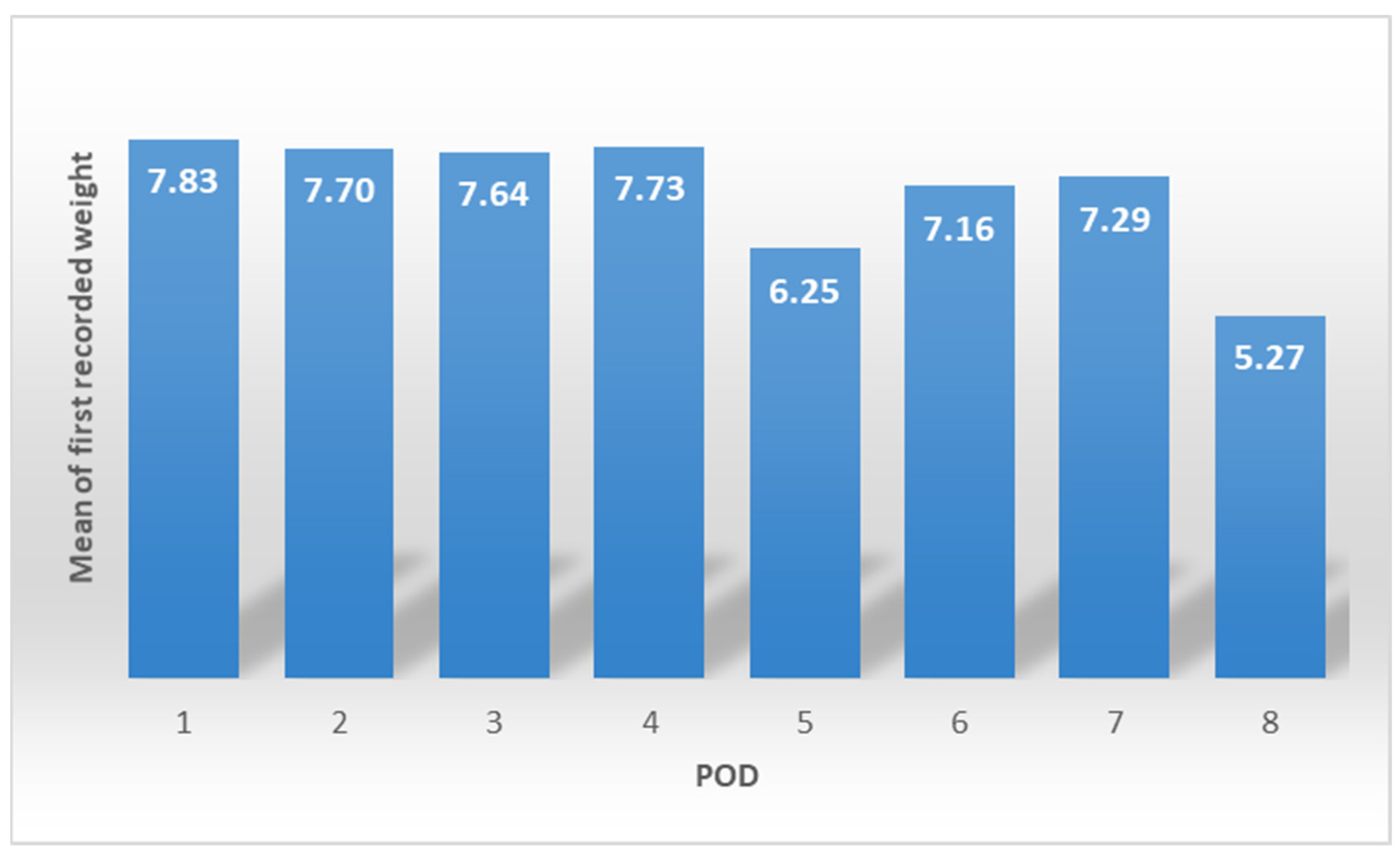
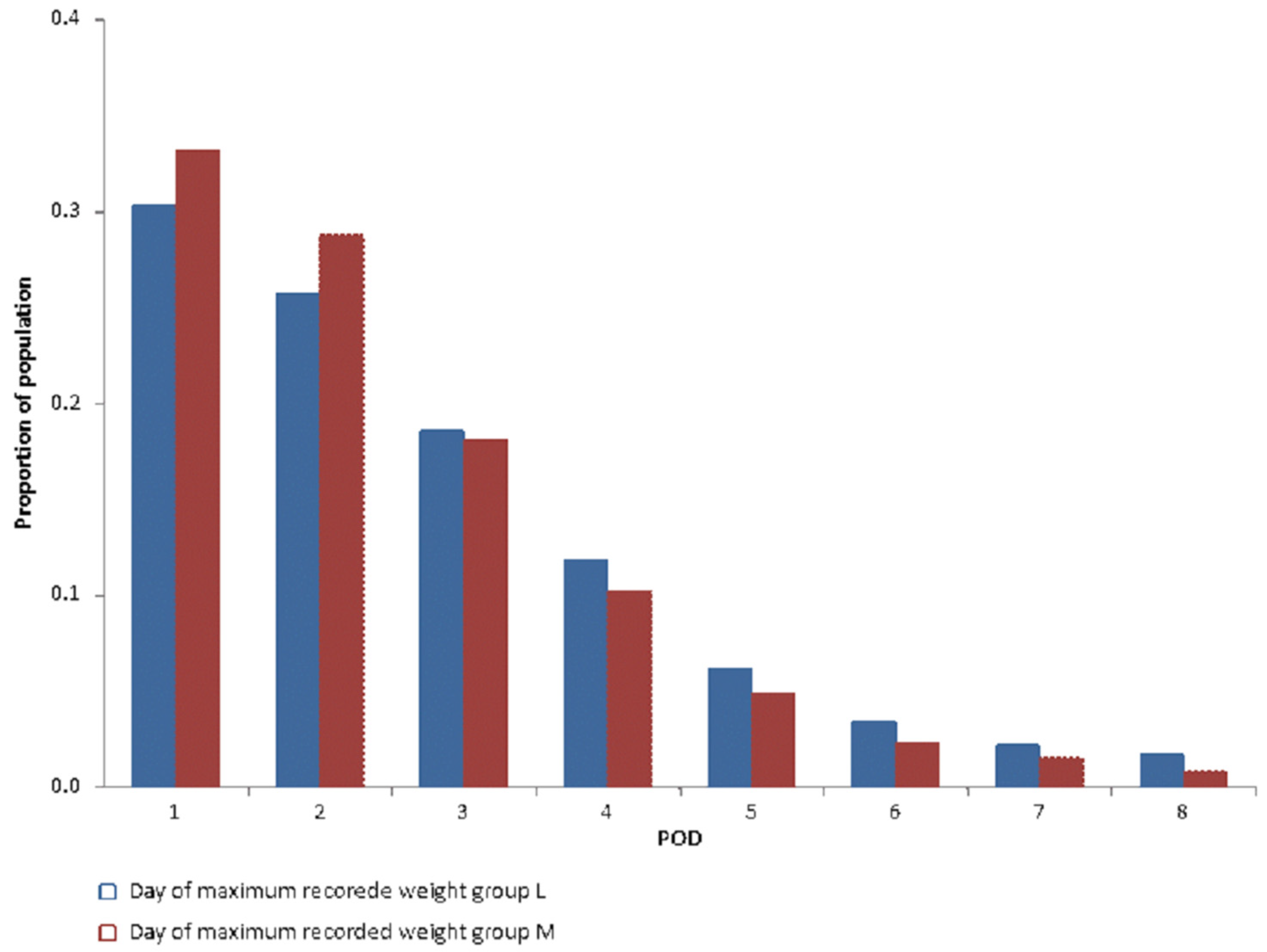
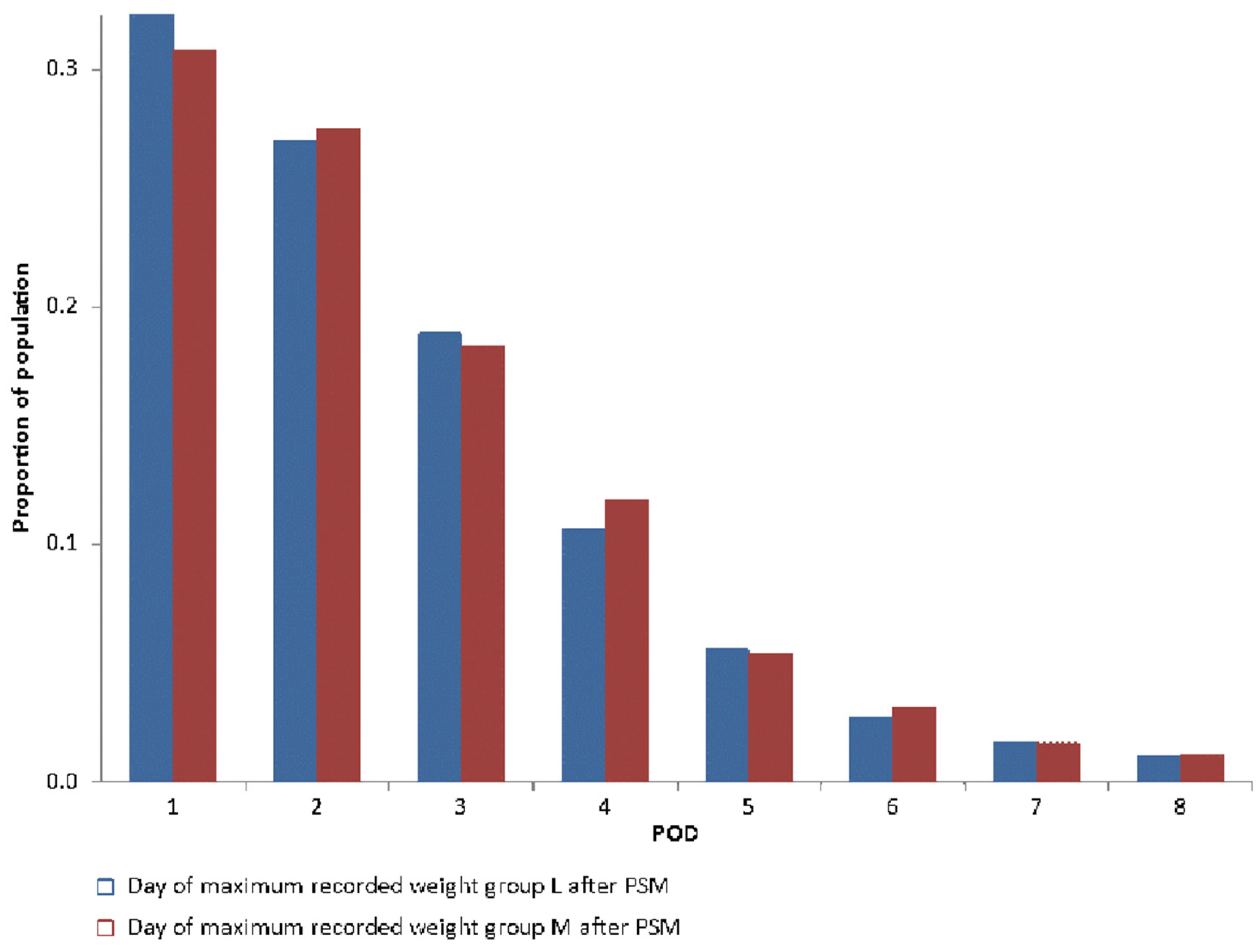
3.2. Day of Maximum Collected Weight
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

References
- Morin, J.-F.; Mistry, B.; Langlois, Y.; Ma, F.; Chamoun, P.; Holcroft, C. Fluid Overload after Coronary Artery Bypass Grafting Surgery Increases the Incidence of Post-Operative Complications. WJCS 2011, 1, 18–23. [Google Scholar] [CrossRef] [Green Version]
- Engelman, D.T.; Ben Ali, W.; Williams, J.B.; Perrault, L.P.; Reddy, V.S.; Arora, R.C.; Roselli, E.E.; Khoynezhad, A.; Gerdisch, M.; Levy, J.H.; et al. Guidelines for Perioperative Care in Cardiac Surgery: Enhanced Recovery After Surgery Society Recommendations. JAMA Surg. 2019, 154, 755–766. [Google Scholar] [CrossRef] [PubMed]
- Osawa, E.A.; Rhodes, A.; Landoni, G.; Galas, F.R.B.G.; Fukushima, J.T.; Park, C.H.L.; Almeida, J.P.; Nakamura, R.E.; Strabelli, T.M.V.; Pileggi, B.; et al. Effect of Perioperative Goal-Directed Hemodynamic Resuscitation Therapy on Outcomes Following Cardiac Surgery: A Randomized Clinical Trial and Systematic Review. Crit. Care Med. 2016, 44, 724–733. [Google Scholar] [CrossRef]
- Parke, R.L.; Gilder, E.; Gillham, M.J.; Walker, L.J.C.; Bailey, M.J.; McGuinness, S.P. A Multicenter, Open-Label, Randomized Controlled Trial of a Conservative Fluid Management Strategy Compared With Usual Care in Participants After Cardiac Surgery: The Fluids After Bypass Study. Crit. Care Med. 2021, 49, 449–461. [Google Scholar] [CrossRef]
- Aya, H.D.; Cecconi, M.; Hamilton, M.; Rhodes, A. Goal-directed therapy in cardiac surgery: A systematic review and meta-analysis. Br. J. Anaesth. 2013, 110, 510–517. [Google Scholar] [CrossRef] [Green Version]
- Messina, A.; Robba, C.; Calabrò, L.; Zambelli, D.; Iannuzzi, F.; Molinari, E.; Scarano, S.; Battaglini, D.; Baggiani, M.; de Mattei, G.; et al. Perioperative liberal versus restrictive fluid strategies and postoperative outcomes: A systematic review and metanalysis on randomised-controlled trials in major abdominal elective surgery. Crit. Care 2021, 25, 205. [Google Scholar] [CrossRef]
- Myles, P.S.; Bellomo, R.; Corcoran, T.; Forbes, A.; Peyton, P.; Story, D.; Christophi, C.; Leslie, K.; McGuinness, S.; Parke, R.; et al. Restrictive versus Liberal Fluid Therapy for Major Abdominal Surgery. N. Engl. J. Med. 2018, 378, 2263–2274. [Google Scholar] [CrossRef]
- Eastwood, G.M. Evaluating the reliability of recorded fluid balance to approximate body weight change in patients undergoing cardiac surgery. Heart Lung 2006, 35, 27–33. [Google Scholar] [CrossRef]
- Butti, F.; Pache, B.; Winiker, M.; Grass, F.; Demartines, N.; Hübner, M. Correlation of postoperative fluid balance and weight and their impact on outcomes. Langenbecks. Arch. Surg. 2020, 405, 1191–1200. [Google Scholar] [CrossRef]
- Grützner, H.; Flo Forner, A.; Meineri, M.; Janai, A.; Ender, J.; Zakhary, W.Z.A. A Comparison of Patients Undergoing On- vs. Off-Pump Coronary Artery Bypass Surgery Managed with a Fast-Track Protocol. J. Clin. Med. 2021, 10, 4470. [Google Scholar] [CrossRef]
- Zakhary, W.Z.A.; Turton, E.W.; Flo Forner, A.; von Aspern, K.; Borger, M.A.; Ender, J.K. A comparison of sufentanil vs. remifentanil in fast-track cardiac surgery patients. Anaesthesia 2019, 74, 602–608. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zakhary, W.; Lindner, J.; Sgouropoulou, S.; Eibel, S.; Probst, S.; Scholz, M.; Ender, J. Independent Risk Factors for Fast-Track Failure Using a Predefined Fast-Track Protocol in Preselected Cardiac Surgery Patients. J. Cardiothorac. Vasc. Anesth. 2015, 29, 1461–1465. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ender, J.; Borger, M.A.; Scholz, M.; Funkat, A.-K.; Anwar, N.; Sommer, M.; Mohr, F.W.; Fassl, J. Cardiac surgery fast-track treatment in a postanesthetic care unit: Six-month results of the Leipzig fast-track concept. Anesthesiology 2008, 109, 61–66. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hasheminejad, E.; Forner, A.F.; Meineri, M.; Ender, J.; Zakhary, W.Z.A. Postoperative Nausea and Vomiting Prophylaxis in Fast-Track Cardiac Anesthesia: A Patient Matched Retrospective before and after Study. Int. J. Anesthesiol. Pain Med. 2022, 8, 78–85. [Google Scholar]
- Korsik, E.; Meineri, M.; Zakhary, W.Z.A.; Balga, I.; Jawad, K.; Ender, J.; Flo Forner, A. Persistent and acute postoperative pain after cardiac surgery with anterolateral thoracotomy or median sternotomy: A prospective observational study. J. Clin. Anesth. 2022, 77, 110577. [Google Scholar] [CrossRef] [PubMed]
- Probst, S.; Cech, C.; Haentschel, D.; Scholz, M.; Ender, J. A specialized post anaesthetic care unit improves fast-track management in cardiac surgery: A prospective randomized trial. Crit. Care 2014, 18, 468. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- GRAß, C.; Stretti, F.; Zakhary, W.; Turton, E.; Sgouoropoulou, S.; Mende, M.; Ender, J. Impact of the post-anesthetic care unit opening hours on fast-track success in cardiac surgery. Minerva Anestesiol. 2017, 83, 155–164. [Google Scholar] [CrossRef]
- Zaouter, C.; Damphousse, R.; Moore, A.; Stevens, L.-M.; Gauthier, A.; Carrier, F.M. Elements not Graded in the Cardiac Enhanced Recovery After Surgery Guidelines Might Improve Postoperative Outcome: A Comprehensive Narrative Review. J. Cardiothorac. Vasc. Anesth. 2022, 36, 746–765. [Google Scholar] [CrossRef]
- Kellum, J.A. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1. [Google Scholar] [CrossRef] [Green Version]
- Köster, M.; Dennhardt, S.; Jüttner, F.; Hopf, H.-B. Cumulative changes in weight but not fluid volume balances reflect fluid accumulation in ICU patients. Acta Anaesthesiol. Scand. 2017, 61, 205–215. [Google Scholar] [CrossRef]
- Cagini, L.; Capozzi, R.; Tassi, V.; Savignani, C.; Quintaliani, G.; Reboldi, G.; Puma, F. Fluid and electrolyte balance after major thoracic surgery by bioimpedance and endocrine evaluation. Eur. J. Cardiothorac. Surg. 2011, 40, e71–e76. [Google Scholar] [CrossRef]
- Shiao, C.-C.; Huang, Y.-T.; Lai, T.-S.; Huang, T.-M.; Wang, J.-J.; Huang, C.-T.; Wu, P.-C.; Wu, C.-H.; Tsai, I.-J.; Tseng, L.-J.; et al. Perioperative body weight change is associated with in-hospital mortality in cardiac surgical patients with postoperative acute kidney injury. PLoS ONE 2017, 12, e0187280. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hübner, M.; Pache, B.; Solà, J.; Blanc, C.; Hahnloser, D.; Demartines, N.; Grass, F. Thresholds for optimal fluid administration and weight gain after laparoscopic colorectal surgery. BJS Open 2019, 3, 532–538. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perko, M.J.; Jarnvig, I.L.; Højgaard-Rasmussen, N.; Eliasen, K.; Arendrup, H. Electric impedance for evaluation of body fluid balance in cardiac surgical patients. J. Cardiothorac. Vasc. Anesth. 2001, 15, 44–48. [Google Scholar] [CrossRef]
- Chen, X.; Xu, J.; Li, Y.; Shen, B.; Jiang, W.; Luo, Z.; Wang, C.; Teng, J.; Ding, X.; Lv, W. The Effect of Postoperative Fluid Balance on the Occurrence and Progression of Acute Kidney Injury After Cardiac Surgery. J. Cardiothorac. Vasc. Anesth. 2021, 35, 2700–2706. [Google Scholar] [CrossRef] [PubMed]
- Shen, Y.; Zhang, W.; Cheng, X.; Ying, M. Association between postoperative fluid balance and acute kidney injury in patients after cardiac surgery: A retrospective cohort study. J. Crit. Care 2018, 44, 273–277. [Google Scholar] [CrossRef]
- Palomba, H.; Treml, R.E.; Caldonazo, T.; Katayama, H.T.; Gomes, B.C.; Malbouisson, L.M.S.; Silva Junior, J.M. Intraoperative fluid balance and cardiac surgery-associated acute kidney injury: A multicenter prospective study. Braz. J. Anesthesiol. 2022, 72, 688–694. [Google Scholar] [CrossRef]
- Brown, J.K.; Shaw, A.D.; Mythen, M.G.; Guzzi, L.; Reddy, V.S.; Crisafi, C.; Engelman, D.T.; Gan, T.J.; Miller, T.; Guinn, N.R.; et al. Adult Cardiac Surgery Associated Acute Kidney Injury: Joint Consensus Report of the PeriOperative Quality Initiative (POQI) and the Enhanced Recovery After Surgery (ERAS®) Cardiac Society. J. Cardiothorac. Vasc. Anesth. 2023; in press. [Google Scholar] [CrossRef]
- Hu, J.; Chen, R.; Liu, S.; Yu, X.; Zou, J.; Ding, X. Global Incidence and Outcomes of Adult Patients With Acute Kidney Injury After Cardiac Surgery: A Systematic Review and Meta-Analysis. J. Cardiothorac. Vasc. Anesth. 2016, 30, 82–89. [Google Scholar] [CrossRef]
- Doenst, T.; Diab, M.; Sponholz, C.; Bauer, M.; Färber, G. The Opportunities and Limitations of Minimally Invasive Cardiac Surgery. Dtsch. Arztebl. Int. 2017, 114, 777–784. [Google Scholar] [CrossRef] [Green Version]
- Olsthoorn, J.R.; Heuts, S.; Houterman, S.; Maessen, J.G.; Sardari Nia, P. Minimally invasive approach compared to resternotomy for mitral valve surgery in patients with prior cardiac surgery: Retrospective multicentre study based on the Netherlands Heart Registration. Eur. J. Cardiothorac. Surg. 2022, 62, 1–48. [Google Scholar] [CrossRef] [PubMed]
- Murphy, G.J.; Pike, K.; Rogers, C.A.; Wordsworth, S.; Stokes, E.A.; Angelini, G.D.; Reeves, B.C. Liberal or restrictive transfusion after cardiac surgery. N. Engl. J. Med. 2015, 372, 997–1008. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mazer, C.D.; Whitlock, R.P.; Fergusson, D.A.; Hall, J.; Belley-Cote, E.; Connolly, K.; Khanykin, B.; Gregory, A.J.; de Médicis, É.; McGuinness, S.; et al. Restrictive or Liberal Red-Cell Transfusion for Cardiac Surgery. N. Engl. J. Med. 2017, 377, 2133–2144. [Google Scholar] [CrossRef]
- Ziemann, S.; Coburn, M.; Rossaint, R.; van Waesberghe, J.; Bürkle, H.; Fries, M.; Henrich, M.; Henzler, D.; Iber, T.; Karst, J.; et al. Implementierung anästhesiologischer Qualitätsindikatoren in Deutschland: Eine prospektive, nationale, multizentrische Qualitätssteigerungsstudie. Anaesthesist 2021, 70, 38–47. [Google Scholar] [CrossRef]
- Statistisches Bundesamt. Zahl der Herzoperationen 2018: 23% Mehr Eingriffe Als Zehn Jahre Zuvor. Available online: https://www.destatis.de/DE/Presse/Pressemitteilungen/2019/09/PD19_380_231.html#:~:text=Die%20durchschnittliche%20Verweildauer%20lag%20bei,37b%20f%C3%BCr%202008%20und%202018) (accessed on 30 April 2023).
- InEK GmbH, Fallpauschalen-Katalog 2021, InEK GmbH. Available online: https://www.g-drg.de/ag-drg-system-2021/fallpauschalen-katalog/fallpauschalen-katalog-2021 (accessed on 29 April 2023).








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| L n = 1015 {after PSM n = 857} | M n = 1198 {after PSM n = 857} | p Value | |
|---|---|---|---|
| Age (y) | 62.7 ± 11.6 {63 ± 11.5} | 64.3 ± 11.8 {64 ± 11.6} | 0.02 {0.129} |
| Female gender | 238 (23) {207 (24)} | 331 (27) {234 (27)} | 0.02 {0.15} |
| NYHA III and IV | 353 (34) {311 (36)} | 453 (37) {315 (37)} | 0.1 {0.92} |
| Preoperative weight (kg) | 85 ± 17 {85.3 ± 16.9} | 84 ± 17 {84.3 ± 17.1} | 0.137 {0.255} |
| BMI (kg/m2) | 28.2 ± 4.7 {28 ± 4.7} | 28 ± 5 {28.1 ± 5.1} | 0.249 {0.486} |
| EuroSCORE II | 1.82 ± 2.0 {1.6 ± 2.1} | 2.0 ± 2.1 {1.6 ± 2} | 0.547 {0.949} |
| Complex surgeries (CABG + Valve/s or 2 or more x Valve) | 149 (14.6) {143 (16.6)} | 283 (23.6) {153 (17.8)} | <0.0001 {0.565} |
| On-pump CABG | 271 (26.6) {226 (26)} | 221 (18.4) {165 (19.2)} | <0.0001 {0.0006} |
| OPCAB/MIDCAB | 237 (23.3) {167 (19.5)} | 155 (13) {149 (17.3)} | <0.0001 {0.289} |
| Isolated AVR | 170 (16.7) {150 (17.5)} | 314 (26) {210 (24.5)} | <0.0001 {0.005} |
| Isolated MVR | 106 (10.4) {100 (11.6)} | 147 (12) {98 (11.4)} | 0.20 {0.939} |
| Minimal invasive approaches (Thoracotomy or partial sternotomy) | 255 (25) {237 (27.5)} | 317 (26.3) {227 (26.4)} | 0.504 {0.624} |
| Thoracotomy approach | 170 (16.7) {156 (18.2)} | 169 (14) {129 (15)} | 0.096 {0.091} |
| Partial sternotomy (superior) | 85 (8.3) {81 (9.4)} | 148 (12.3) {98 (11.4)} | 0.003 {0.20} |
| Emergency surgery | 127 (12.6) {101 (12)} | 153 (12.9) {106 (12.5)} | 0.905 {0.76} |
| Re-do operations | 60 (6.2) {53 (6)} | 83 (7.2) {56 (6.5)} | 0.375 {0.781} |
| Preoperative ejection fraction (%) | 56 ± 10.5 {56 ± 10.5} | 57 ± 10.4 {57 ± 10.5} | 0.082 {0.148} |
| Hypertension | 761 (78.3) {643 (77.5)} | 852 (75) {625 (73)} | 0.47 {0.349} |
| DM | 244 (24) {205 (24)} | 276 (23) {196 (23)} | 0.614 {0.648} |
| Preoperative hematocrit (%) | 40.8 ± 5.4 {38.9 ± 4.9} | 40.1 ± 5.8 {38.3 ± 4.9} | 0.161 {0.001} |
| Preoperative hemoglobin (g/dl) | 12.5 ± 2 {12.5 ± 1.6} | 12.2 ± 2 {12.3 ± 1.6} | 0.09 {0.001} |
| Minimal intraoperative hemoglobin (g/dl) | 10.7 ± 4.8 {10.7 ± 5} | 10.1 ± 3.2 {10.1 ± 2} | <0.0001 {<0.001} |
| Preoperative creatinine (mg/dl) | 0.96 ± 0.02 {0.97 ± 0.69} | 0.91 ± 0.01 {0.92 ± 0.3} | 0.642 {0.02} |
| CPB duration (min) | 71 ± 56 {76 ± 51} | 87 ± 51 {78 ± 49} | <0.0001 {0.322} |
| x-clamp time (min) | 40 ± 41 {46 ± 41} | 55 ± 40 {47 ± 40} | <0.0001 {0.574} |
| Length of surgery (min) | 183 ± 61 {184 ± 60} | 192 ± 55 {188 ± 53} | 0.002 {0.06} |
| Postoperative ventilation time (min) | 106 ± 54 {106 ± 55} | 115 ± 60 {115 ± 60} | 0.015 {0.004} |
| PACU LOS (min) | 240 [90] {235 [95]} | 245 [90] {255 [85]} | 0.006 {<0.001} |
| IMC LOS (h) | 27.5 [47] {25 [46]} | 23.1 [45] {24 [47]} | 0.008 {0.625} |
| Weight gain (kg) | 4.1 ± 1.8 {4.2 ± 1.8} | 10.6 ± 3.1 {10.4 ± 3} | <0.0001 {<0.0001} |
| L n = 857 | M n = 857 | p Value | 95% CI | RR | |
|---|---|---|---|---|---|
| Hospital LOS | 8 [3] | 9 [6] | <0.0001 | 0.58 to 0.64 | |
| In-hospital mortality | 1 (0.1) | 5 (0.5) | 0.12 | 0.19 | |
| FTF | 81 (9.5) | 103 (12) | 0.103 | 0.86 | |
| Postoperative acute kidney injury (AKI) total | 84 (9.8) | 165 (19.2) | <0.0001 | 0.63 | |
| AKI stage I | 62 (8.4) | 136 (15.8) | <0.0001 | 0.66 | |
| AKI stage II | 9 (1) | 24 (2.8) | 0.013 | 0.54 | |
| AKI stage III | 3 (0.3) | 5 (0.6) | 0.506 | 0.75 | |
| Postop chronic renal impairment | 91 (11) | 117 (14.5) | 0.06 | 0.86 | |
| Any postoperative pulmonary complications | 17 (2) | 16 (1.8) | 0.999 | 1.0 | |
| Number of patients who received 1 or more pRBCs | 311 (36) | 429 (50) | <0.0001 | 0.75 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Krüger, A.; Flo Forner, A.; Ender, J.; Janai, A.; Roufail, Y.; Otto, W.; Meineri, M.; Zakhary, W.Z.A. Postoperative Weight Gain within Enhanced Recovery after Cardiac Surgery. J. Cardiovasc. Dev. Dis. 2023, 10, 263. https://doi.org/10.3390/jcdd10060263
Krüger A, Flo Forner A, Ender J, Janai A, Roufail Y, Otto W, Meineri M, Zakhary WZA. Postoperative Weight Gain within Enhanced Recovery after Cardiac Surgery. Journal of Cardiovascular Development and Disease. 2023; 10(6):263. https://doi.org/10.3390/jcdd10060263
Chicago/Turabian StyleKrüger, Alexandra, Anna Flo Forner, Jörg Ender, Aniruddha Janai, Youssef Roufail, Wolfgang Otto, Massimiliano Meineri, and Waseem Z. A. Zakhary. 2023. "Postoperative Weight Gain within Enhanced Recovery after Cardiac Surgery" Journal of Cardiovascular Development and Disease 10, no. 6: 263. https://doi.org/10.3390/jcdd10060263