
Diagnostic Performance of Cardiac Computed Tomography for Detecting Patent Foramen Ovale: Evaluation Using Transesophageal Echocardiography and Catheterization as Reference Standards
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
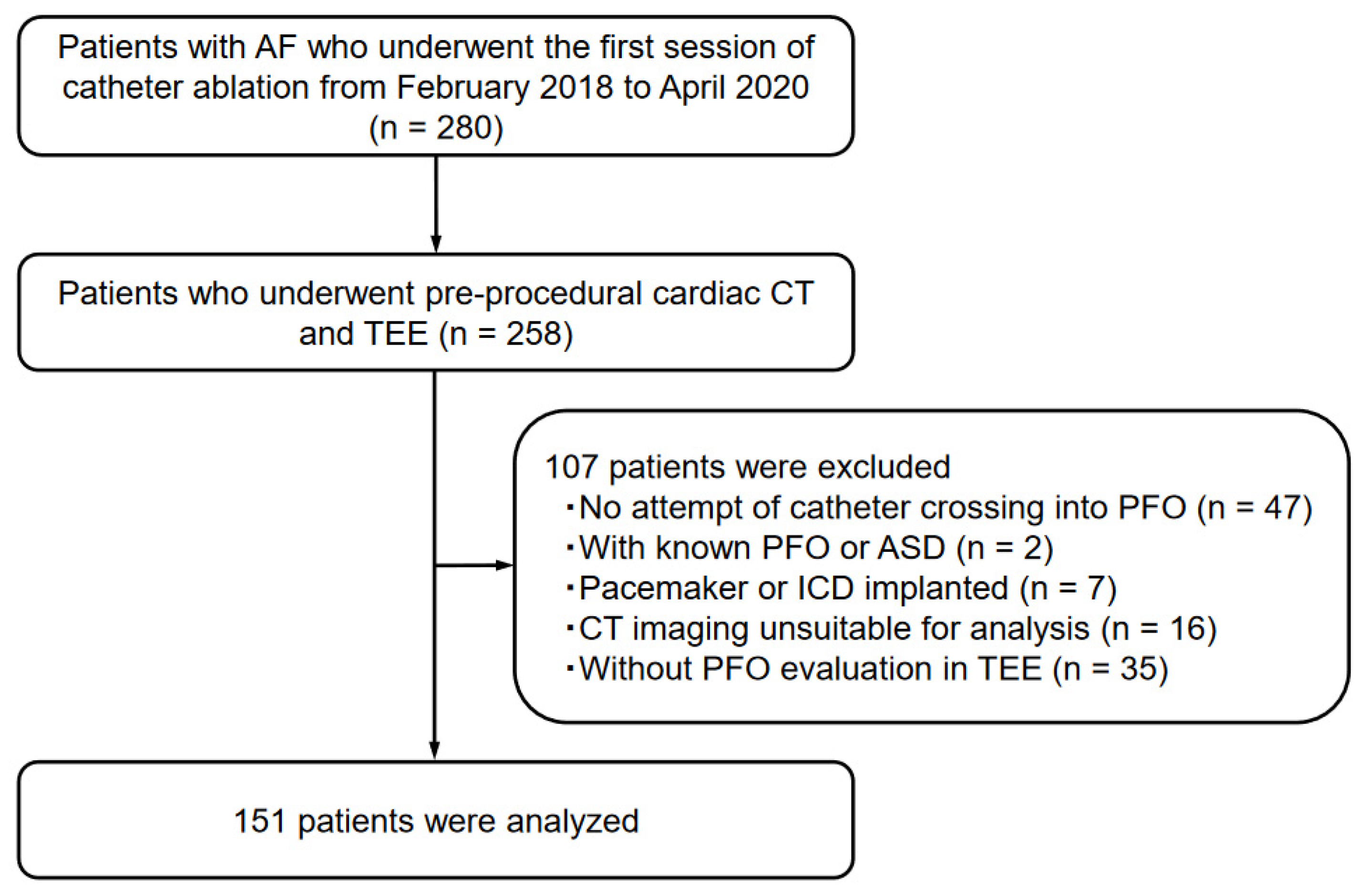
2.1. Study Population
2.2. CT Image Acquisition
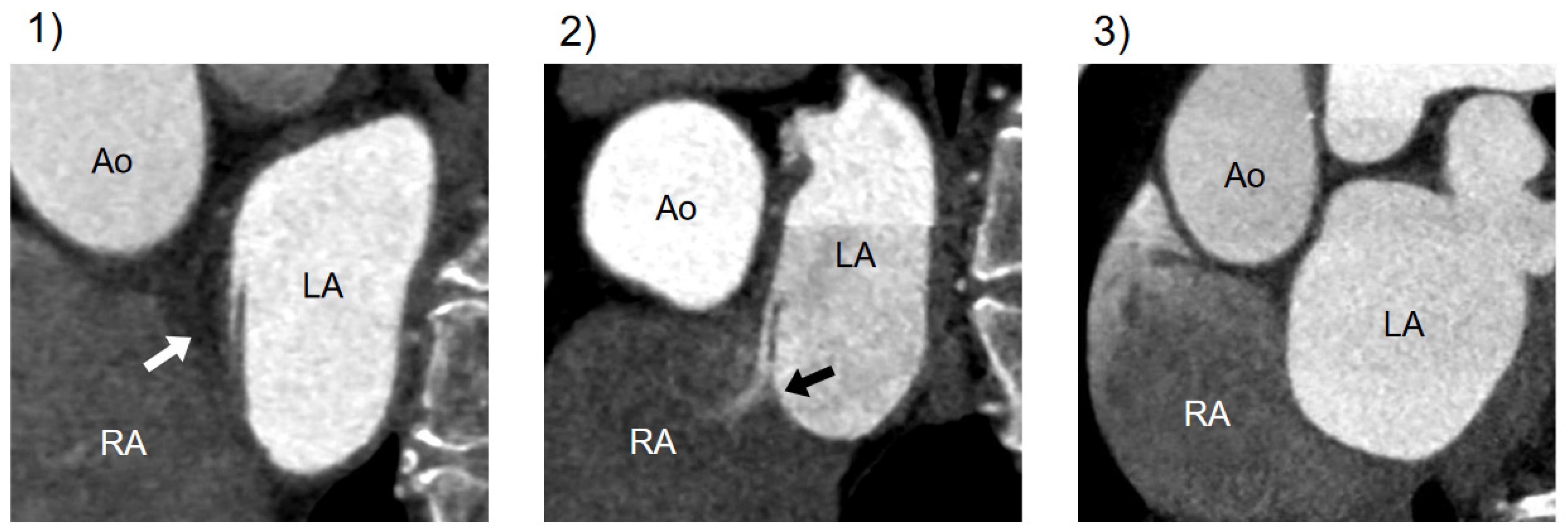
2.3. Assessment of PFO at Cardiac CT
2.4. PFO Confirmation
2.5. Risk Factors for Cardiovascular Disease, Laboratory Analyses, and TTE Data
2.6. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. PFO Diagnosis with TEE and Catheterization
3.3. PFO Detection and Diagnostic Performance at CT Imaging
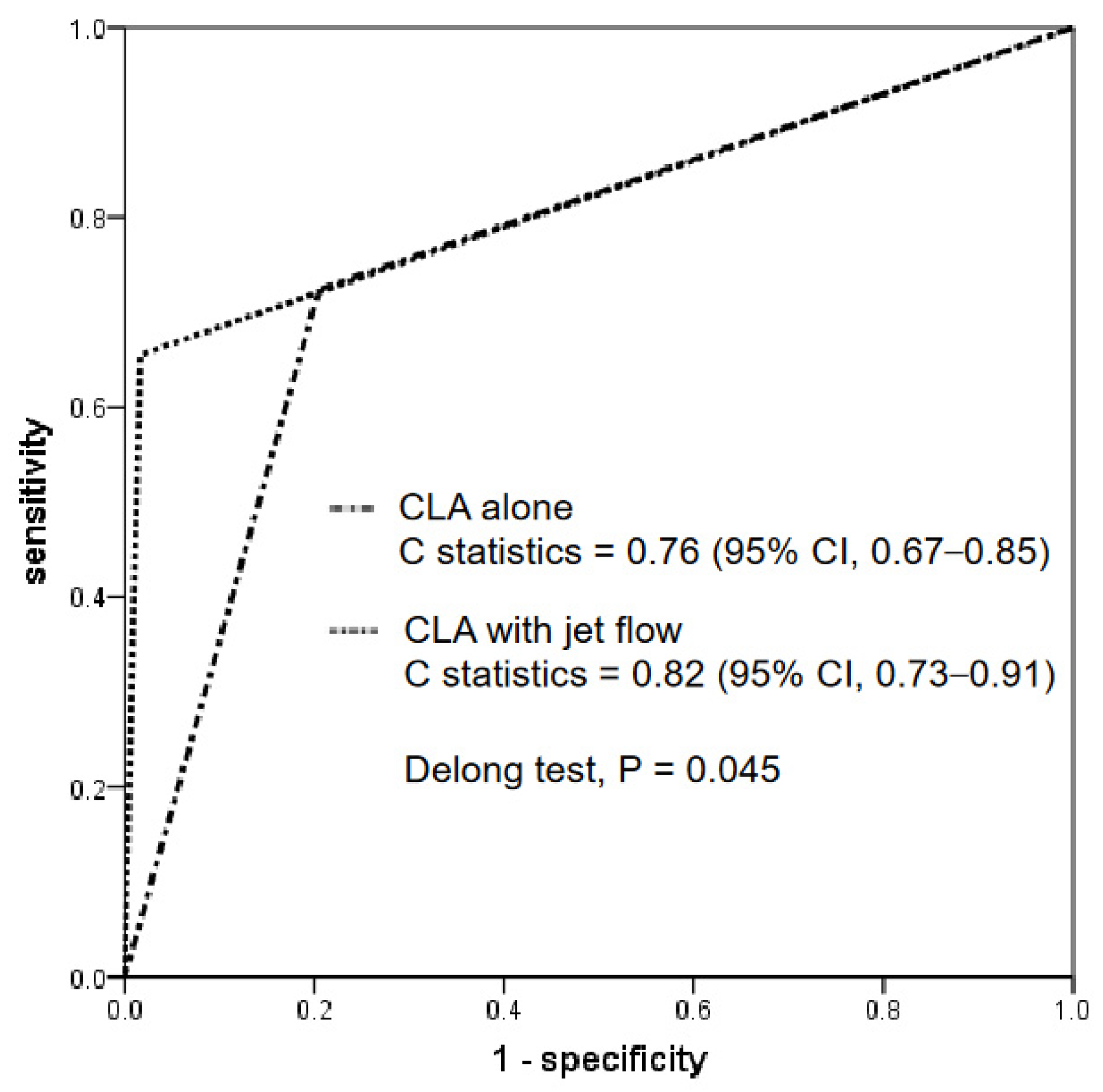
3.4. Comparison of Diagnostic Performance of CT Findings: CLA Alone versus CLA with Jet Flow
3.5. Effect of AF during CT Acquisition for PFO Diagnosis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
List of Abbreviations
| PFO | patent foramen ovale |
| TEE | transesophageal echocardiography |
| IAS | interatrial septum |
| AF | atrial fibrillation |
| CLA | channel-like appearance |
References
- Hagen, P.T.; Scholz, D.G.; Edwards, W.D. Incidence and Size of Patent Foramen Ovale During the First 10 Decades of Life: An Autopsy Study of 965 Normal Hearts. Mayo Clin. Proc. 1984, 59, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Miranda, B.; Fonseca, A.C.; Ferro, J.M. Patent foramen ovale and stroke. J. Neurol. 2018, 265, 1943–1949. [Google Scholar] [CrossRef] [PubMed]
- Lip, P.Z.Y.; Lip, G.Y.H. Patent Foramen Ovale and Migraine Attacks: A Systematic Review. Am. J. Med. 2014, 127, 411–420. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Palkar, A.; Talwar, A. The multiple dimensions of Platypnea-Orthodeoxia syndrome: A review. Respir. Med. 2017, 129, 31–38. [Google Scholar] [CrossRef] [PubMed]
- Torti, S.R.; Billinger, M.; Schwerzmann, M.; Vogel, R.; Zbinden, R.; Windecker, S.; Seiler, C. Risk of decompression illness among 230 divers in relation to the presence and size of patent foramen ovale. Eur. Heart J. 2004, 25, 1014–1020. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Carroll, J.D.; Thaler, D.E.; Smalling, R.W.; MacDonald, L.A.; Marks, D.S.; Tirschwell, D.L.; Investigators, R. Long-Term Outcomes of Patent Foramen Ovale Closure or Medical Therapy after Stroke. N. Engl. J. Med. 2017, 377, 1022–1032. [Google Scholar] [CrossRef]
- Sondergaard, L.; Kasner, S.E.; Rhodes, J.F.; Andersen, G.; Iversen, H.K.; Nielsen-Kudsk, J.E.; Settergren, M.; Sjostrand, C.; Roine, R.O.; Hildick-Smith, D.; et al. Patent Foramen Ovale Closure or Antiplatelet Therapy for Cryptogenic Stroke. N. Engl. J. Med. 2017, 377, 1033–1042. [Google Scholar] [CrossRef]
- Mas, J.L.; Derumeaux, G.; Guillon, B.; Massardier, E.; Hosseini, H.; Mechtouff, L.; Arquizan, C.; Bejot, Y.; Vuillier, F.; Detante, O.; et al. Patent Foramen Ovale Closure or Anticoagulation vs. Antiplatelets after Stroke. N. Engl. J. Med. 2017, 377, 1011–1021. [Google Scholar] [CrossRef]
- De Cuyper, C.; Pauwels, T.; Derom, E.; De Pauw, M.; De Wolf, D.; Vermeersch, P.; Van Berendoncks, A.; Paelinck, B.; Vermeersch, G. Percutaneous Closure of PFO in Patients with Reduced Oxygen Saturation at Rest and during Exercise: Short- and Long-Term Results. J. Interv. Cardiol. 2020, 2020, 9813038. [Google Scholar] [CrossRef]
- Pearson, A.C.; Labovitz, A.J.; Tatineni, S.; Gomez, C.R. Superiority of transesophageal echocardiography in detecting cardiac source of embolism in patients with cerebral ischemia of uncertain etiology. J. Am. Coll. Cardiol. 1991, 17, 66–72. [Google Scholar] [CrossRef]
- Pinto, F.J. When and how to diagnose patent foramen ovale. Heart 2005, 91, 438–440. [Google Scholar] [CrossRef] [PubMed]
- Hilberath, J.N.; Oakes, D.A.; Shernan, S.K.; Bulwer, B.E.; D’Ambra, M.N.; Eltzschig, H.K. Safety of transesophageal echocardiography. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2010, 23, 1115–1127; quiz 1220–1221. [Google Scholar] [CrossRef] [PubMed]
- Sainathan, S.; Andaz, S. A systematic review of transesophageal echocardiography-induced esophageal perforation. Echocardiography 2013, 30, 977–983. [Google Scholar] [CrossRef] [PubMed]
- Kosehan, D.; Akin, K.; Koktener, A.; Cakir, B.; Aktas, A.; Teksam, M. Interatrial shunt: Diagnosis of patent foramen ovale and atrial septal defect with 64-row coronary computed tomography angiography. Jpn. J. Radiol. 2011, 29, 576–582. [Google Scholar] [CrossRef]
- Kim, Y.J.; Hur, J.; Shim, C.Y.; Lee, H.J.; Ha, J.W.; Choe, K.O.; Heo, J.H.; Choi, E.Y.; Choi, B.W. Patent foramen ovale: Diagnosis with multidetector CT--comparison with transesophageal echocardiography. Radiology 2009, 250, 61–67. [Google Scholar] [CrossRef]
- Lee, S.; Kim, I.C.; Kim, Y.D.; Nam, H.S.; Kim, S.Y.; Choi, S.M.; Chang, H.J. The role of cardiac CT throughout the full cardiac cycle in diagnosing patent foramen ovale in patients with acute stroke. Eur. Radiol. 2021, 31, 8983–8990. [Google Scholar] [CrossRef]
- Mojadidi, M.K.; Bogush, N.; Caceres, J.D.; Msaouel, P.; Tobis, J.M. Diagnostic accuracy of transesophageal echocardiogram for the detection of patent foramen ovale: A meta-analysis. Echocardiogram 2014, 31, 752–758. [Google Scholar] [CrossRef]
- Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020, 43, S14–S31. [CrossRef]
- Silvestry, F.E.; Cohen, M.S.; Armsby, L.B.; Burkule, N.J.; Fleishman, C.E.; Hijazi, Z.M.; Lang, R.M.; Rome, J.J.; Wang, Y. Guidelines for the Echocardiographic Assessment of Atrial Septal Defect and Patent Foramen Ovale: From the American Society of Echocardiography and Society for Cardiac Angiography and Interventions. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2015, 28, 910–958. [Google Scholar] [CrossRef]
- Schneider, B.; Zienkiewicz, T.; Jansen, V.; Hofmann, T.; Noltenius, H.; Meinertz, T. Diagnosis of patent foramen ovale by transesophageal echocardiography and correlation with autopsy findings. Am. J. Cardiol. 1996, 77, 1202–1209. [Google Scholar] [CrossRef]
- Knecht, S.; Wright, M.; Lellouche, N.; Nault, I.; Matsuo, S.; O’Neill, M.D.; Lomas, O.; Deplagne, A.; Bordachar, P.; Sacher, F.; et al. Impact of a patent foramen ovale on paroxysmal atrial fibrillation ablation. J. Cardiovasc. Electrophysiol. 2008, 19, 1236–1241. [Google Scholar] [CrossRef]
- Saremi, F.; Channual, S.; Raney, A.; Gurudevan, S.V.; Narula, J.; Fowler, S.; Abolhoda, A.; Milliken, J.C. Imaging of patent foramen ovale with 64-section multidetector CT. Radiology 2008, 249, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Krishnan, S.C.; Salazar, M. Septal pouch in the left atrium: A new anatomical entity with potential for embolic complications. JACC Cardiovasc. Interv. 2010, 3, 98–104. [Google Scholar] [CrossRef] [PubMed]
- Luotolahti, M.; Saraste, M.; Hartiala, J. Saline contrast and colour Doppler transoesophageal echocardiography in detecting a patent foramen ovale and right-to-left shunts in stroke patients. Clin. Physiol. 1995, 15, 265–273. [Google Scholar] [CrossRef]
- Sun, J.P.; Stewart, W.J.; Hanna, J.; Thomas, J.D. Diagnosis of patent foramen ovale by contrast versus color Doppler by transesophageal echocardiography: Relation to atrial size. Am. Heart J. 1996, 131, 239–244. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| All (n = 151) | PFO Present (n = 29) | PFO Absent (n = 122) | p-Value * | |
|---|---|---|---|---|
| Age, years | 68 ± 9 | 70 ± 6 | 68 ± 10 | 0.298 |
| Male sex | 94 (62) | 19 (66) | 75 (62) | 0.687 |
| Hypertension | 93 (62) | 17 (59) | 76 (62) | 0.715 |
| Dyslipidemia | 48 (32) | 10 (35) | 38 (31) | 0.729 |
| Diabetes mellitus | 27 (18) | 7 (24) | 20 (16) | 0.328 |
| Smoking | 14 (9) | 2 (7) | 12 (10) | 0.624 |
| Paroxysmal AF | 94 (62) | 14 (48) | 80 (66) | 0.084 |
| AF at CT acquisition | 60 (40) | 14 (48) | 46 (38) | 0.296 |
| History of ischemic stroke | 12 (8) | 3 (10) | 9 (7) | 0.595 |
| Obesity | 62 (41) | 8 (28) | 54 (44) | 0.101 |
| CHADS2 score | 1.4 ± 1.0 | 1.6 ± 1.1 | 1.3 ± 1.0 | 0.241 |
| BNP, pg/mL | 113 [57–229] | 156 [50–361] | 105 [57–213] | 0.289 |
| LVEF, % | 62.2 ± 7.8 | 59.5 ± 9.2 | 62.9 ± 7.3 | 0.074 |
| LA volume index, mL/m2 | 44.7 ± 13.8 | 45.4 ± 11.5 | 44.5 ± 14.3 | 0.743 |
| E/e′ | 13.0 ± 7.3 | 12.9 ± 5.2 | 13.0 ± 7.7 | 0.954 |
| Sensitivity, % | Specificity, % | PPV, % | NPV, % | Accuracy, % | |
|---|---|---|---|---|---|
| CLA alone | 72.4 | 79.5 | 45.7 | 92.4 | 78.1 |
| CLA with jet flow | 65.5 | 98.4 | 90.5 | 92.3 | 92.1 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Miki, T.; Nakagawa, K.; Ichikawa, K.; Mizuno, T.; Nakayama, R.; Ejiri, K.; Kawada, S.; Takaya, Y.; Miyamoto, M.; Miyoshi, T.; et al. Diagnostic Performance of Cardiac Computed Tomography for Detecting Patent Foramen Ovale: Evaluation Using Transesophageal Echocardiography and Catheterization as Reference Standards. J. Cardiovasc. Dev. Dis. 2023, 10, 193. https://doi.org/10.3390/jcdd10050193
Miki T, Nakagawa K, Ichikawa K, Mizuno T, Nakayama R, Ejiri K, Kawada S, Takaya Y, Miyamoto M, Miyoshi T, et al. Diagnostic Performance of Cardiac Computed Tomography for Detecting Patent Foramen Ovale: Evaluation Using Transesophageal Echocardiography and Catheterization as Reference Standards. Journal of Cardiovascular Development and Disease. 2023; 10(5):193. https://doi.org/10.3390/jcdd10050193
Chicago/Turabian StyleMiki, Takashi, Koji Nakagawa, Keishi Ichikawa, Tomofumi Mizuno, Rie Nakayama, Kentaro Ejiri, Satoshi Kawada, Yoichi Takaya, Masakazu Miyamoto, Toru Miyoshi, and et al. 2023. "Diagnostic Performance of Cardiac Computed Tomography for Detecting Patent Foramen Ovale: Evaluation Using Transesophageal Echocardiography and Catheterization as Reference Standards" Journal of Cardiovascular Development and Disease 10, no. 5: 193. https://doi.org/10.3390/jcdd10050193