

History of Neonatal Screening of Congenital Hypothyroidism in Portugal
 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
3. Results
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guthrie, R. Blood Screening for Phenylketonuria. JAMA 1961, 178, 863. [Google Scholar] [CrossRef]
- Dussault, J.H. The Anecdotal History of Screening for Congenital Hypothyroidism. J. Clin. Endocrinol. Metab. 1999, 84, 4332–4334. [Google Scholar] [CrossRef] [PubMed]
- Gaudino, R.; Garel, C.; Czernichow, P.; Leger, J. Proportion of various types of thyroid disorders among newborns with congenital hypothyroidism and normally located gland: A regional cohort study. Clin. Endocrinol. 2005, 62, 444–448. [Google Scholar] [CrossRef]
- McGrath, N.; Hawkes, C.P.; McDonnell, C.M.; Cody, D.; O’Connell, S.M.; Mayne, P.D.; Murphy, N.P. Incidence of Congenital Hypothyroidism over 37 Years in Ireland. Pediatrics 2018, 142, e20181199. [Google Scholar] [CrossRef] [PubMed]
- Nagasaki, K.; Minamitani, K.; Nakamura, A.; Kobayashi, H.; Numakura, C.; Itoh, M.; Mushimoto, Y.; Fujikura, K.; Fukushi, M.; Tajima, T. Guidelines for Newborn Screening of Congenital Hypothyroidism (2021 Revision). Clin. Pediatr. Endocrinol. Case Rep. Clin. Investig. Off. J. Jpn. Soc. Pediatr. Endocrinol. 2023, 32, 26–51. [Google Scholar] [CrossRef] [PubMed]
- Rose, S.R.; Wassner, A.J.; Wintergerst, K.A.; Yayah-Jones, N.-H.; Hopkin, R.J.; Chuang, J.; Smith, J.R.; Abell, K.; LaFranchi, S.H.; Bethin, K.E.; et al. Congenital Hypothyroidism: Screening and Management. Pediatrics 2022, 151, e2022060420. [Google Scholar] [CrossRef] [PubMed]
- Van Trotsenburg, P.; Stoupa, A.; Léger, J.; Rohrer, T.; Peters, C.; Fugazzola, L.; Cassio, A.; Heinrichs, C.; Beauloye, V.; Pohlenz, J.; et al. Congenital Hypothyroidism: A 2020–2021 Consensus Guidelines Update—An ENDO-European Reference Network Initiative Endorsed by the European Society for Pediatric Endocrinology and the European Society for Endocrinology. Thyroid® 2021, 31, 387–419. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatrics; Rose, S.R.; Section on Endocrinology and Committee on Genetics; American Thyroid Association; Brown, R.S.; Public Health Committee; Lawson Wilkins Pediatric Endocrine Society; Foley, T.; Kaplowitz, P.B.; Kaye, C.I.; et al. Update of Newborn Screening and Therapy for Congenital Hypothyroidism. Pediatrics 2006, 117, 2290–2303. [Google Scholar] [PubMed]
- Liu, L.; He, W.; Zhu, J.; Deng, K.; Tan, H.; Xiang, L.; Yuan, X.; Li, Q.; Huang, M.; Guo, Y.; et al. Global prevalence of congenital hypothyroidism among neonates from 1969 to 2020: A systematic review and meta-analysis. Eur. J. Pediatr. 2023, 182, 2957–2965. [Google Scholar] [CrossRef]
- LaFranchi, S.H. Thyroid Function in Preterm/Low Birth Weight Infants: Impact on Diagnosis and Management of Thyroid Dysfunction. Front. Endocrinol. 2021, 12, 666207. [Google Scholar] [CrossRef]
- Sack, J. Thyroid function in pregnancy—Maternal-fetal relationship in health and disease. Pediatr. Endocrinol. Rev. 2003, 1 (Suppl. 2), 176. [Google Scholar]
- Thorpe-Beeston, J.; Nicolaides, K.; McGregor, A. Fetal Thyroid Function. Thyroid® 1992, 2, 207–217. [Google Scholar] [CrossRef]
- Ford, G.; LaFranchi, S.H. Screening for congenital hypothyroidism: A worldwide view of strategies. Best Pract. Res. Clin. Endocrinol. Metab. 2014, 28, 175–187. [Google Scholar] [CrossRef]
- Diário da República. Despacho Nº 752/2010—Portuguese National Program of Neonatal Screening; Diário da República: Lisbon, Portugal, 2010. [Google Scholar]
- Wilson, J.; Glover, M.; Jungner, G.; World Health Organization. Principles and Practice of Screening for Disease; World Health Organization: Geneva, Switzerland, 1968. [Google Scholar]
- Léger, J.; Olivieri, A.; Donaldson, M.; Torresani, T.; Krude, H.; van Vliet, G.; Polak, M.; Butler, G.; on behalf of ESPE-PES-SLEP-JSPE-APEG-APPES-ISPAE, and the Congenital Hypothyroidism Consensus Conference Group. European Society for Paediatric Endocrinology Consensus Guidelines on Screening, Diagnosis, and Management of Congenital Hypothyroidism. J. Clin. Endocrinol. Metab. 2014, 99, 363–384. [Google Scholar] [CrossRef]
- LaFranchi, S.H. Newborn screening strategies for congenital hypothyroidism: An update. J. Inherit. Metab. Dis. 2010, 33 (Suppl. 2), 225–233. [Google Scholar] [CrossRef] [PubMed]
- McGrath, N.; Hawkes, C.P.; Mayne, P.; Murphy, N.P. Optimal Timing of Repeat Newborn Screening for Congenital Hypothyroidism in Preterm Infants to Detect Delayed Thyroid-Stimulating Hormone Elevation. J. Pediatr. 2019, 205, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Scavone, M.; Giancotti, L.; Anastasio, E.; Pensabene, L.; Sestito, S.; Concolino, D. Evolution of congenital hypothyroidism in a cohort of preterm born children. Pediatr. Neonatol. 2020, 61, 629–636. [Google Scholar] [CrossRef] [PubMed]
- Jo, H.Y.; Yang, E.H.; Kim, Y.M.; Choi, S.-H.; Park, K.H.; Yoo, H.W.; Park, S.J.; Kwak, M.J. Incidence of congenital hypothyroidism by gestational age: A retrospective observational study. Yeungnam Univ. J. Med. 2023, 40, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Klosinska, M.; Kaczynska, A.; Ben-Skowronek, I. Congenital Hypothyroidism in Preterm Newborns—The Challenges of Diagnostics and Treatment: A Review. Front. Endocrinol. 2022, 13, 860862. [Google Scholar] [CrossRef]
- Medda, E.; Vigone, M.C.; Cassio, A.; Calaciura, F.; Costa, P.; Weber, G.; de Filippis, T.; Gelmini, G.; Di Frenna, M.; Caiulo, S.; et al. Neonatal Screening for Congenital Hypothyroidism: What Can We Learn from Discordant Twins? J. Clin. Endocrinol. Metab. 2019, 104, 5765–5779. [Google Scholar] [CrossRef] [PubMed]
- Simonetti, S.; D’amato, G.; Esposito, B.; Chiarito, M.; Dentico, D.; Lorè, T.; Cardinali, R.; Russo, S.; Laforgia, N.; Faienza, M.F. Congenital hypothyroidism after newborn screening program reorganization in the Apulia region. Ital. J. Pediatr. 2022, 48, 131. [Google Scholar] [CrossRef]
- Delange, F.; Dalhem, A.; Bourdoux, P.; Lagasse, R.; Glinoer, D.; Fisher, D.A.; Walfish, P.G.; Ermans, A.-M. Increased risk of primary hypothyroidism in preterm infants. J. Pediatr. 1984, 105, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Danner, E.; Niuro, L.; Huopio, H.; Niinikoski, H.; Viikari, L.; Kero, J.; Jääskeläinen, J. Incidence of primary congenital hypothyroidism over 24 years in Finland. Pediatr. Res. 2022, 93, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Olivieri, A.; Corbetta, C.; Weber, G.; Vigone, M.C.; Fazzini, C.; Medda, E.; The Italian Study Group for Congenital Hypothyroidism. Congenital Hypothyroidism due to Defects of Thyroid Development and Mild Increase of TSH at Screening: Data From the Italian National Registry of Infants With Congenital Hypothyroidism. J. Clin. Endocrinol. Metab. 2013, 98, 1403–1408. [Google Scholar] [CrossRef] [PubMed]
- Silvfromin, S.M.; Leone, C.; Leone, C.R. Detecting Congenital Hypothyroidism with Newborn Screening: The Relevance of Thyroid-Stimulating Hormone Cutoff Values. J. Pediatr. 2017, 93, 274–280. [Google Scholar]
- Langham, S.; Hindmarsh, P.; Krywawych, S.; Peters, C. Screening for Congenital Hypothyroidism: Comparison of Borderline Screening Cut-Off Points and the Effect on the Number of Children Treated with Levothyroxine. Eur. Thyroid. J. 2013, 2, 180–186. [Google Scholar] [CrossRef] [PubMed]
- Maggio, M.C.; Ragusa, S.S.; Aronica, T.S.; Granata, O.M.; Gucciardino, E.; Corsello, G. Neonatal screening for congenital hypothyroidism in an Italian Centre: A 5-years real-life retrospective study. Ital. J. Pediatr. 2021, 47, 108. [Google Scholar] [CrossRef] [PubMed]
- Peters, C.; Schoenmakers, N. Mechanisms in Endocrinology: The pathophysiology of transient congenital hypothyroidism. Eur. J. Endocrinol. 2022, 187, R1–R16. [Google Scholar] [CrossRef] [PubMed]
- Gmür, S.; Konrad, D.; Fingerhut, R. Prevalence of Transient Hypothyroidism in Children Diagnosed with Congenital Hypothyroidism between 2000 and 2016. Int. J. Mol. Sci. 2023, 24, 2817. [Google Scholar] [CrossRef]
- Hinton, C.F.; Harris, K.B.; Borgfeld, L.; Drummond-Borg, M.; Eaton, R.; Lorey, F.; Therrell, B.L.; Wallace, J.; Pass, K.A. Trends in Incidence Rates of Congenital Hypothyroidism Related to Select Demographic Factors: Data from the United States, California, Massachusetts, New York, and Texas. Pediatrics 2010, 125 (Suppl. 2), S37–S47. [Google Scholar] [CrossRef]
- Rezaeian, S.; Khazaei, S.; Hooshmand, E.; Esmailnasab, N. Gender and Risk of Congenital Hypothyroidism: A Systematic Review and Meta-Analysis. Int. J. Pediatr. 2017, 5, 6703–6712. [Google Scholar]
- Waller, D.K.; Anderson, J.L.; Lorey, F.; Cunningham, G.C. Risk Factors for Congenital Hypothyroidism: An Investigation of Infant’s Birth Weight, Ethnicity, and Gender in California, 1990–1998. Teratology 2000, 62, 36–41. [Google Scholar] [CrossRef] [PubMed]
- Clapin, H.; Lewis, B.D.; Greed, L.; Dawkins, H.; O’leary, P. Factors influencing neonatal thyroid-stimulating hormone concentrations as a measure of population iodine status. J. Pediatr. Endocrinol. Metab. 2014, 27, 101–106. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Castell, E.; Juste, M.; Palazón-Bru, A.; Goicoechea, M.; Gil-Guillén, V.F.; Rizo-Baeza, M.M. Factors associated with moderate neonatal hyperthyrotropinemia. PLoS ONE 2019, 14, e0220040. [Google Scholar] [CrossRef]
- The Iodine Global Network. Global Scorecard of Iodine Nutrition in 2020 in the General Population Based on School-Age Children (Sac); The Iodine Global Network: Paris, France, 2021. [Google Scholar]
- World Health Organization; UNICEF; ICCIDD; Nutrition and Food Safety (NFS). Assessment of Iodine Deficiency Disorders and Monitoring Their Elimination. A Guide for Programme Managers, 3rd ed.; Updated 1 September 2008; World Health Organization: Geneva, Switzerland, 2007. [Google Scholar]
- Costeira, M.J.; Oliveira, P.; Ares, S.; Roque, S.; de Escobar, G.M.; Palha, J.A. Parameters of Thyroid Function Throughout and After Pregnancy in an Iodine-Deficient Population. Thyroid® 2010, 20, 995–1001. [Google Scholar] [CrossRef]
- Limbert, E.; Prazeres, S.; Pedro, M.S.; Madureira, D.; Miranda, A.; Ribeiro, M.; de Castro, J.J.; Carrilho, F.; Oliveira, M.J.; Reguengo, H.; et al. Iodine intake in Portuguese pregnant women: Results of a countrywide study. Eur. J. Endocrinol. 2010, 163, 631–635. [Google Scholar] [CrossRef]
- Direção-Geral da Saúde. Aporte de Iodo em Mulheres na Pré-Conceção, Gravidez e Amamentação: Orientação Nº 011/2013, De 26/08/2013; Direção-Geral da Saúde: Lisbon, Portugal, 2013.




{kind=link}
{kind=link}
{kind=link}
| Year | ||||||
|---|---|---|---|---|---|---|
| Program indicator | 1981 # | 1990 | 2000 | 2010 | 2020 | 2021 ## |
| Number of births | 152,102 | 116,383 | 120,071 | 101,381 | 84,426 | 79,582 |
| Number of screened newborns | 29,323 | 110,607 | 118,554 | 101,773 | 85,456 | 79,217 |
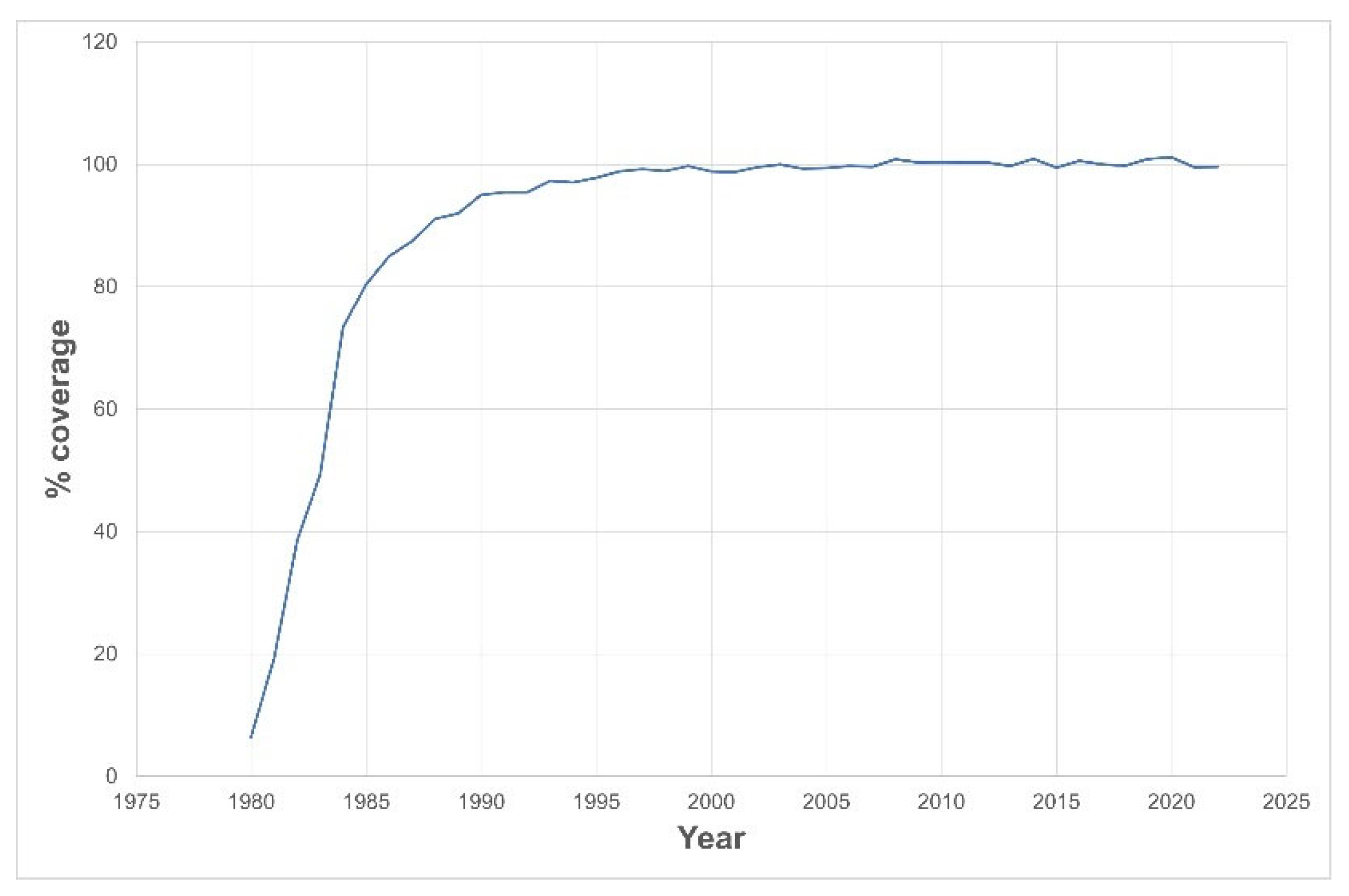
| Coverage rate (%) & | 19.3 | 95 | 98.8 | 100.4 | 101.1 | 99.5 |
| Cumulative incidence | 1/4300 * | 1/3900 | 1/3367 | 1/3045 | 1/2841 | 1/2827 |
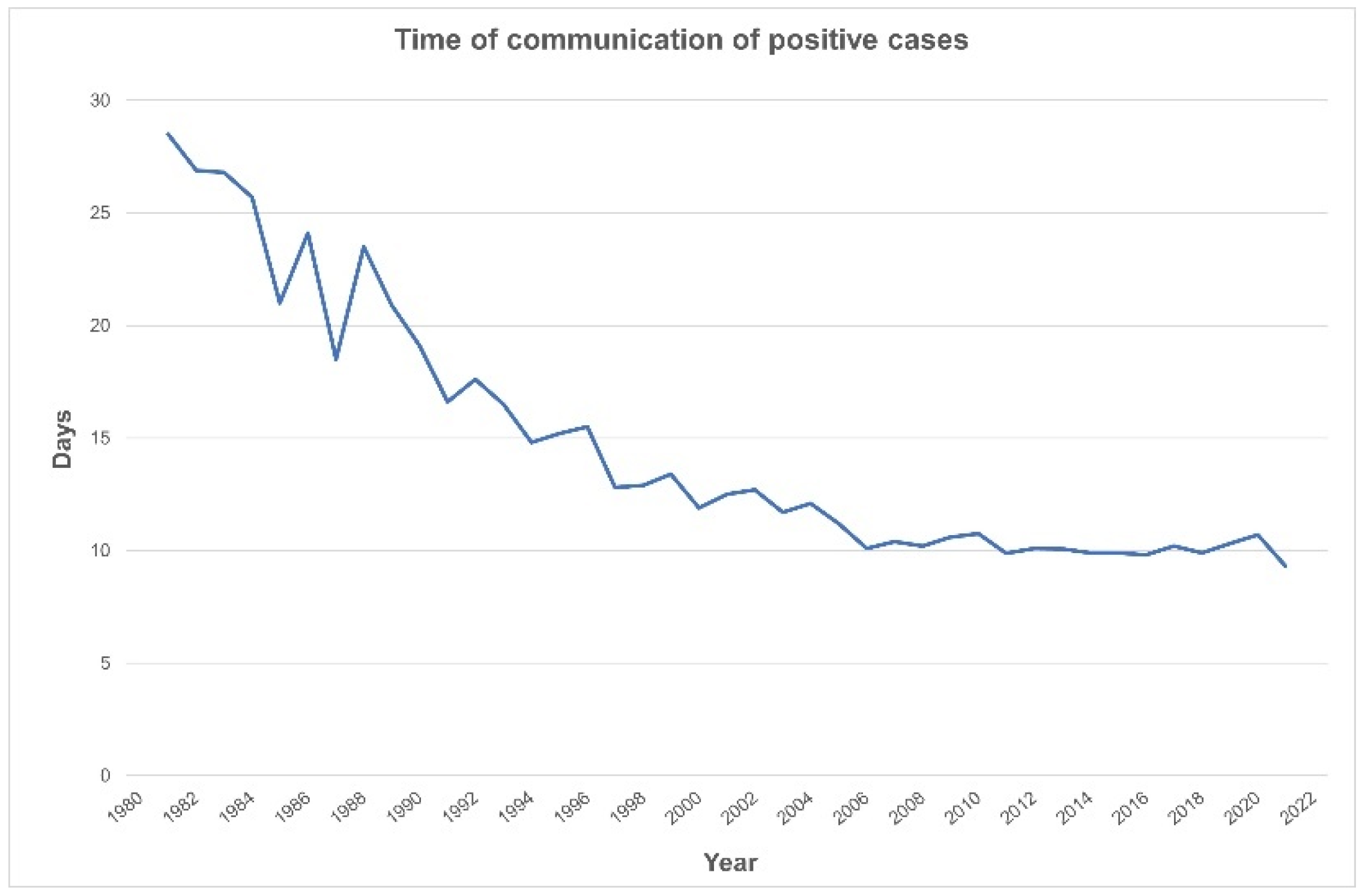
| Beginning of treatment (days) | 30 * | 19.1 | 11.9 | 10.4 | 10.9 | 9.3 |
| % Recall CH | 0.09 | 0.27 | 0.33 | 0.07 | 0.08 | |
| % Recall preterms | 0.0029 ** | 0.1828 | 1.326 | NA | ||
| Year | Sample Collection (Day) | Decision Tree | Retesting Preterm Babies | ||
|---|---|---|---|---|---|
| TSH Cutoff (mIU/L) | Procedure | Criteria | Procedure | ||
| 1981–1988 | 5–10 | <90–80–50 # | normal | NA | NA |
| >90–80–50 # | referral | ||||
| 1989–1996 | 4–7 | <30 | normal | ||
| >30 | referral; use of TT4 as 2nd tier | ||||
| 1997–2002 | 4–7 | <20 | normal | ||
| 20–40 | 2nd sample | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2003–2005 | 3–6 | <20 | normal | ||
| 20–40 | 2nd sample | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2006–2008 | 3–6 | <10 | normal | ||
| 10–20 | 2nd tier- if TT4 < 6.5 µg/dL: 2nd sample | ||||
| >20 | referral; use of TT4 as 2nd tier | ||||
| 2009–2014 | 3–6 | <10 | normal | PT < 30 wGA and/or BW < 1500 g | Retesting: 14–15 days |
| 10–20 | 2nd tier- if TT4 < 6.5 µg/dL: 2nd sample | ||||
| 20–40 | 2nd sample | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2015 | 3–6 | <10 | normal | PT < 30 wGA and/or BW < 1500 g | Retesting: 14–15 and 28–30 days |
| 10–20 | 2nd tier if TT4 < 6.5 µg/dL: 2nd sample | ||||
| 20–40 | 2nd sample | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2016–2017 | 3–6 | <10 | normal | ||
| 10–20 | 2nd tier if TT4 < 8.5 µg/dL: 2nd sample | ||||
| 20–40 | 2nd sample | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2018–2020 | 3–6 | <10 | normal | ||
| 10–20 | 2nd tier if TT4 < 9.5 µg/dL: 2nd sample if TSH >10 mIU/L: refer | ||||
| 20–40 | 2nd sample if TSH > 10 mIU/L: refer | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2021–2022 | 3–6 | <10 | normal | PT < 27 wGA | Retesting: 14–15, 28–30 days, 32 and 36 weeks |
| 10–20 | 2nd tier if TT4 < 9.5 µg/dL: 2nd sampleif TSH >10 mIU/L: refer | PT 27–30 wGA PT 30–32 wGA | Retesting: 14–15, 28–30 days and 36 weeks | ||
| 20–40 | 2nd sample if TSH >10 mIU/L: refer | ||||
| >40 | referral; use of TT4 as 2nd tier | ||||
| 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | |
|---|---|---|---|---|---|---|---|---|
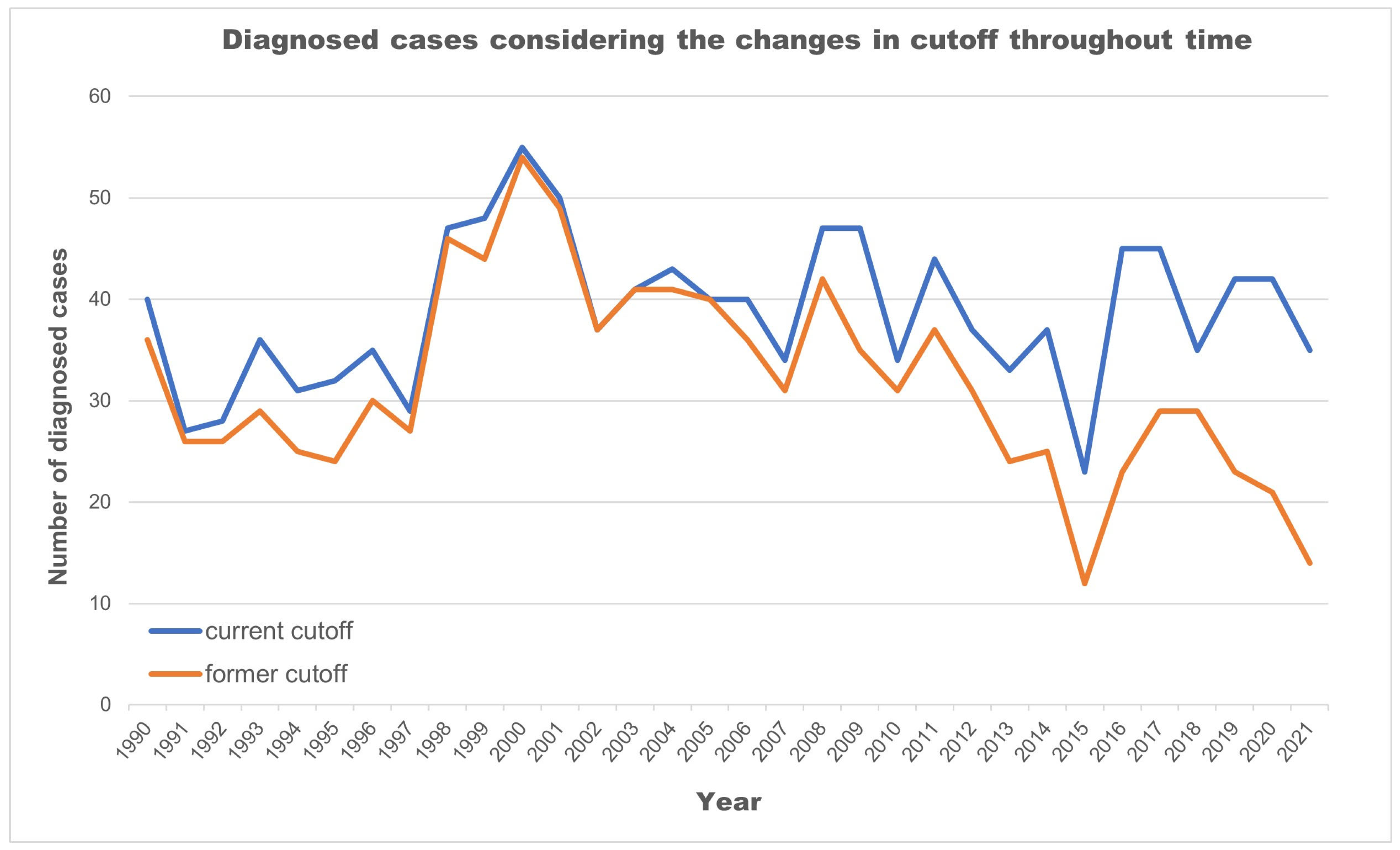
| Number of CH cases | 37 | 23 | 45 | 45 | 35 | 42 | 42 | 35 |
| Number (and %) of CH cases who required 2–3 measurements for diagnosis | 12 (32%) | 6 (26%) | 22 (49%) | 24 (53%) | 24 (69%) | 17 (40%) | 22 (52%) | 22 (63%) |
| Number of PTs of the ones (with CH) who had 2–3 samples | NA | NA | 2 | 5 | 6 | 4 | 8 | 9 |
| Number of PTs with TSH < 10 mU/L in 1st sample | NA | NA | 2 | 5 | 0 | 3 | 7 | 8 |
| Number of PTs with TSH < 10 mU/L in 2nd–3rd samples | NA | NA | 2 | 2 | 0 | 2 | 5 | 6 |
| Number of PTs with normal TT4 at all times | NA | NA | 2 | 1 | 0 | 1 | 3 | 2 |
| Year | Screened Babies with TSH > 5 mIU/L (%) |
|---|---|
| 2013 | 2.5 |
| 2014 | 2.9 |
| 2015 | 2.7 |
| 2016 | 3.0 |
| 2017 | 3.6 |
| 2018 | 3.0 |
| 2019 | 2.9 |
| 2020 | 2.9 |
| 2021 | 3.4 |
| 2022 | 3.3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Costeira, M.J.; Costa, P.; Roque, S.; Carvalho, I.; Vilarinho, L.; Palha, J.A. History of Neonatal Screening of Congenital Hypothyroidism in Portugal. Int. J. Neonatal Screen. 2024, 10, 16. https://doi.org/10.3390/ijns10010016
Costeira MJ, Costa P, Roque S, Carvalho I, Vilarinho L, Palha JA. History of Neonatal Screening of Congenital Hypothyroidism in Portugal. International Journal of Neonatal Screening. 2024; 10(1):16. https://doi.org/10.3390/ijns10010016
Chicago/Turabian StyleCosteira, Maria José, Patrício Costa, Susana Roque, Ivone Carvalho, Laura Vilarinho, and Joana Almeida Palha. 2024. "History of Neonatal Screening of Congenital Hypothyroidism in Portugal" International Journal of Neonatal Screening 10, no. 1: 16. https://doi.org/10.3390/ijns10010016