
Navigating the Nexus: HIV and Breast Cancer—A Critical Review
 , , , , ,
, , , , , {kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
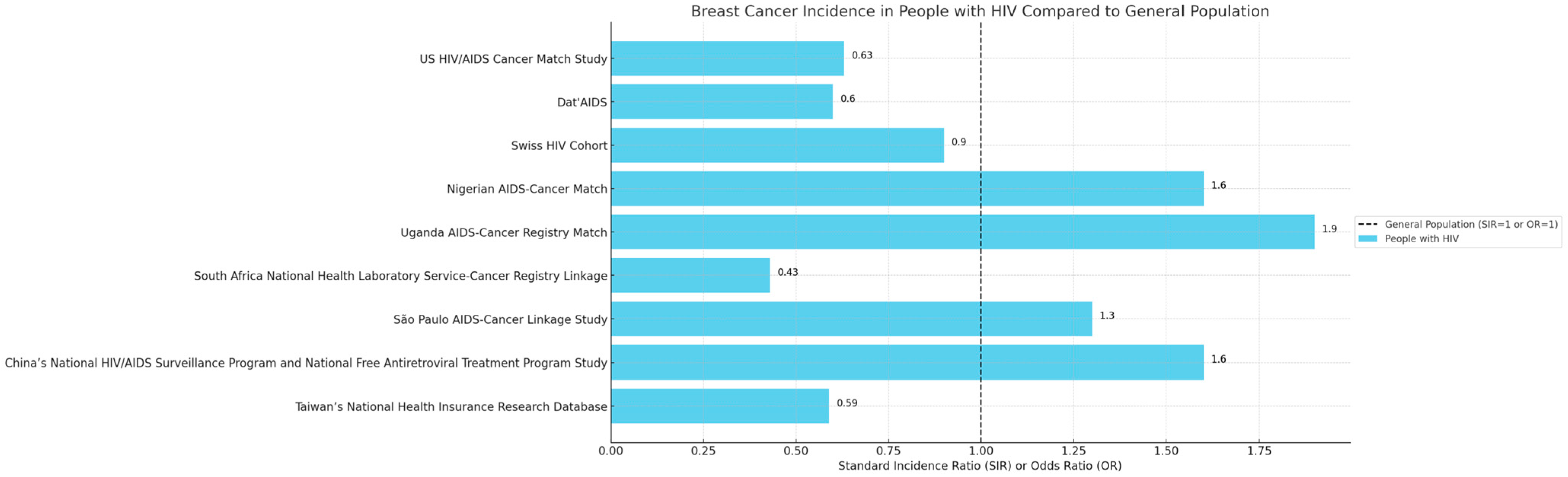
2. Epidemiological and Demographic Considerations
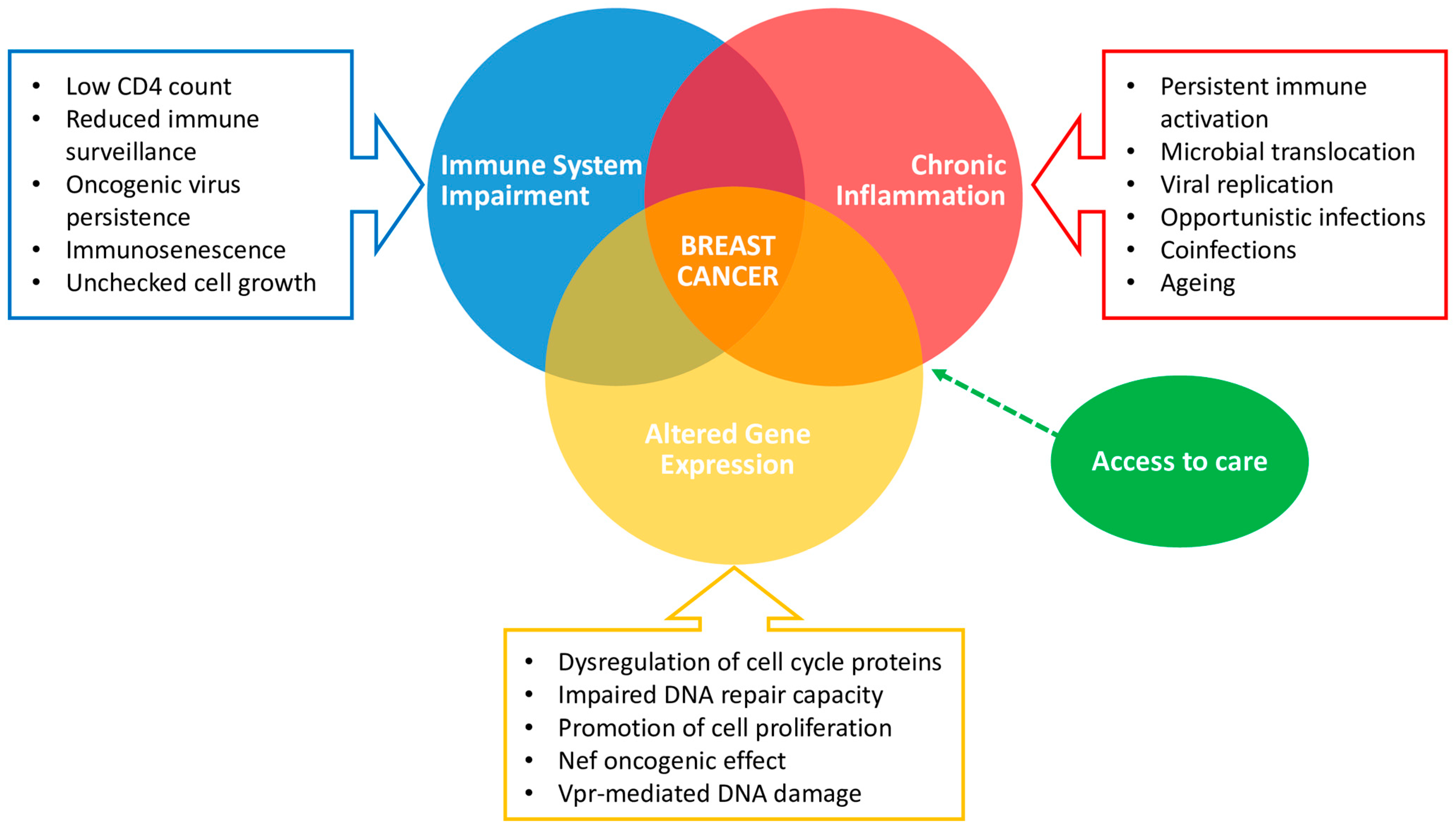
3. Biological Interplay between HIV Infection and Breast Cancer
3.1. Immune System Impairment and Cancer Risk
3.2. HIV, Chronic Inflammation, and Cancer
3.3. Gene Expression Alteration and Breast Cancer in HIV Infection
3.4. Debating Considerations
4. Breast Cancer Clinical Characteristics in PLWH
5. Clinical Outcomes of HIV+ve Breast Cancer Patients
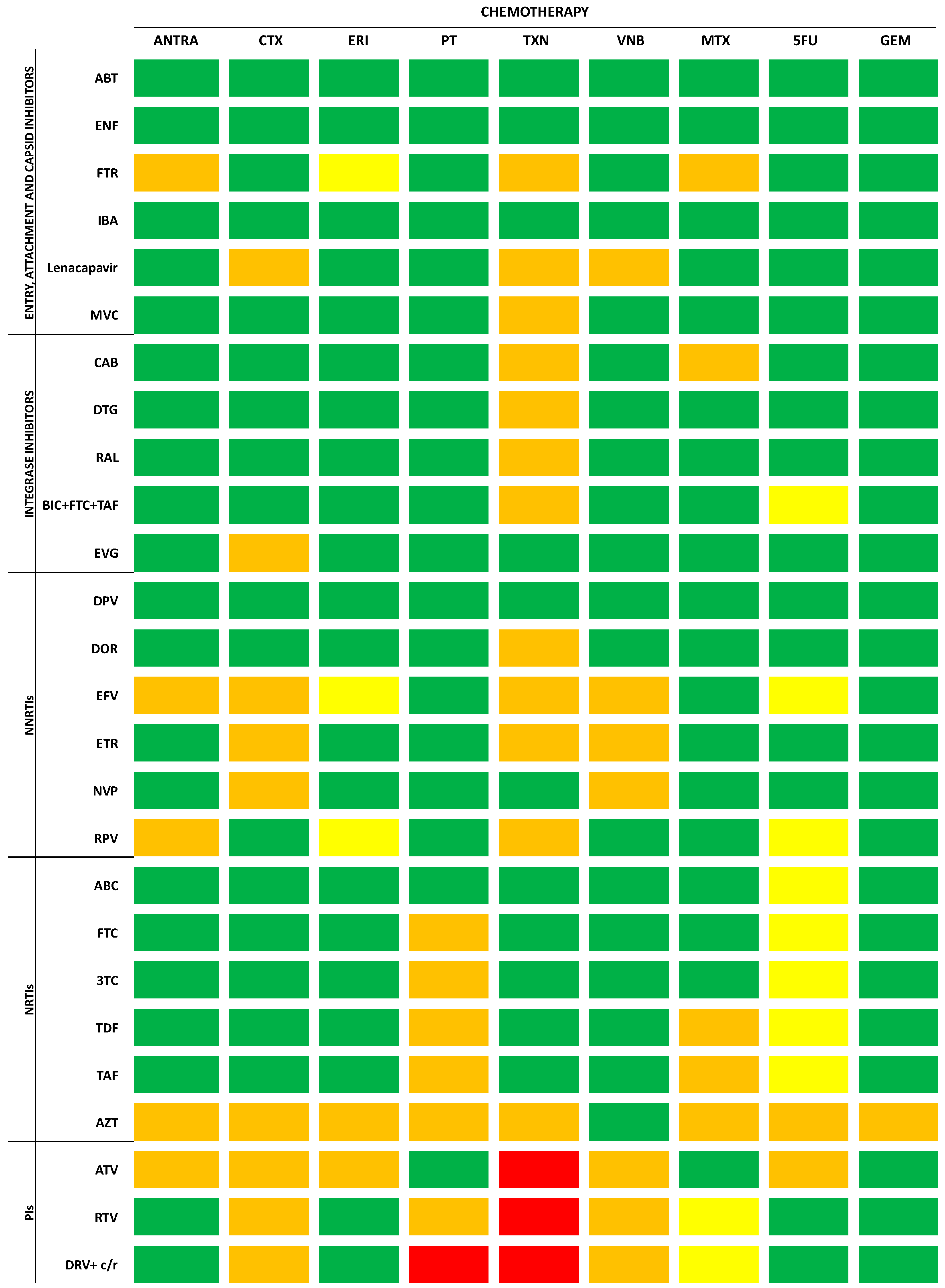
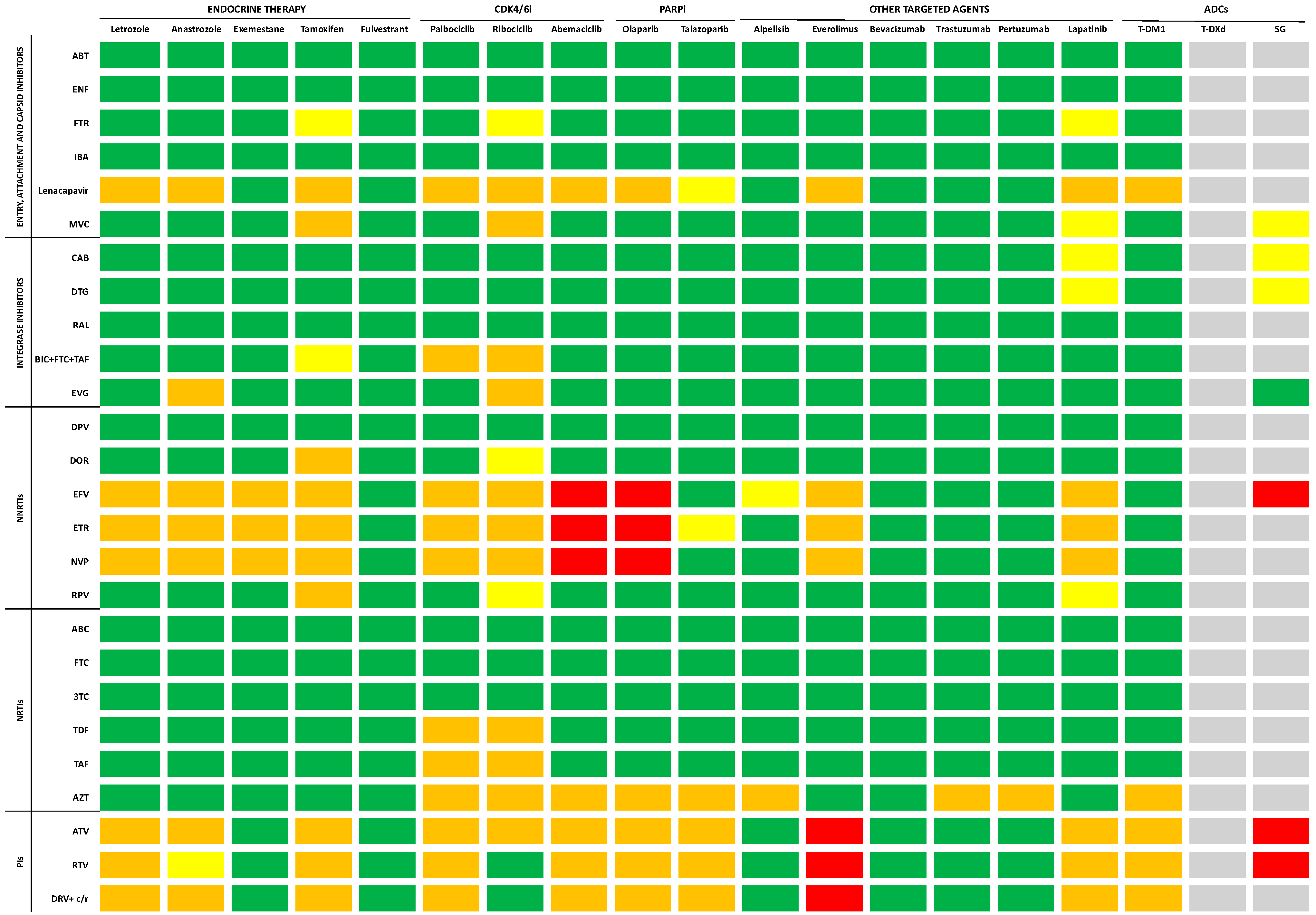
6. Antiretroviral Therapy and Anticancer Agents: Cross-Toxicities and Drug–Drug Interactions
- Entry, Attachment, and Capsid Inhibitors
- Integrase inhibitors
- Non-nucleoside reverse transcriptase inhibitors (NNRTIs)
- Nucleoside reverse transcriptase inhibitors (NRTIs)
- Protease inhibitors (Pis)
7. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- WHO. 2022. Available online: https://www.who.int/news-room/fact-sheets/detail/breast-cancer (accessed on 10 February 2024).
- UNAIDS. 2022. Available online: https://www.unaids.org/en/resources/documents/2023/2022_unaids_data (accessed on 10 February 2024).
- Marino, A.; Caltabiano, E.; Zagami, A.; Onorante, A.; Zappalà, C.; Locatelli, M.E.; Pampaloni, A.; Scuderi, D.; Bruno, R.; Cacopardo, B. Rapid emergence of cryptococcal fungemia, Mycobacterium chelonae vertebral osteomyelitis and gastro intestinal stromal tumor in a young HIV late presenter: A case report. BMC Infect. Dis. 2018, 18, 693. [Google Scholar] [CrossRef]
- McCormack, V.A.; Febvey-Combes, O.; Ginsburg, O.; dos-Santos-Silva, I. Breast cancer in women living with HIV: A first global estimate. Int. J. Cancer 2018, 143, 2732–2740. [Google Scholar] [CrossRef]
- Deeks, S.G.; Overbaugh, J.; Phillips, A.; Buchbinder, S. HIV infection. Nat. Rev. Dis. Primers 2015, 1, 15035. [Google Scholar] [CrossRef]
- Lurain, K. Treating Cancer in People with HIV. J. Clin. Oncol. 2023, 41, 3682–3688. [Google Scholar] [CrossRef]
- Yarchoan, R.; Uldrick, T.S. HIV-Associated Cancers and Related Diseases. N. Engl. J. Med. 2018, 378, 1029–1041. [Google Scholar] [CrossRef] [PubMed]
- Park, B.; Ahn, K.H.; Choi, Y.; Kim, J.H.; Seong, H.; Kim, Y.J.; Choi, J.Y.; Song, J.Y.; Lee, E.; Jun, Y.H.; et al. Cancer Incidence Among Adults with HIV in a Population-Based Cohort in Korea. JAMA Netw. Open 2022, 5, e2224897. [Google Scholar] [CrossRef] [PubMed]
- Chiao, E.Y.; Coghill, A.; Kizub, D.; Fink, V.; Ndlovu, N.; Mazul, A.; Sigel, K. The effect of non-AIDS-defining cancers on people living with HIV. Lancet Oncol. 2021, 22, e240–e253. [Google Scholar] [CrossRef] [PubMed]
- Yuan, T.; Hu, Y.; Zhou, X.; Yang, L.; Wang, H.; Li, L.; Wang, J.; Qian, H.Z.; Clifford, G.M.; Zou, H. Incidence and mortality of non-AIDS-defining cancers among people living with HIV: A systematic review and meta-analysis. EClinicalMedicine 2022, 52, 101613. [Google Scholar] [CrossRef] [PubMed]
- Horner, M.J.; Shiels, M.S.; McNeel, T.S.; Monterosso, A.; Miller, P.; Pfeiffer, R.M.; Engels, E.A. Real-world use of antiretroviral therapy and risk of cancer among people with HIV in Texas. Aids 2024, 38, 379–386. [Google Scholar] [CrossRef]
- Knettel, B.; Corrigan, K.; Cherenack, E.; Ho, N.; Carr, S.; Cahill, J.; Chino, J.; Ubel, P.; Watt, M.; Suneja, G. HIV, cancer, and coping: The cumulative burden of a cancer diagnosis among people living with HIV. J. Psychosoc. Oncol. 2021, 39, 734–748. [Google Scholar] [CrossRef]
- Lasagna, A.; Zuccaro, V.; Sacchi, P.; Pagnucco, L.; Ferraris, E.; Armani, G.; Rizzo, G.; Tancredi, R.J.; Pedrazzoli, P. Breast Cancer and HIV: State of the Art and Practical Implications. SN Compr. Clin. Med. 2021, 3, 1727–1739. [Google Scholar] [CrossRef]
- Casper, C.; Crane, H.; Menon, M.; Money, D. HIV/AIDS Comorbidities: Impact on Cancer, Noncommunicable Diseases, and Reproductive Health. In Major Infectious Diseases; Holmes, K.K., Bertozzi, S., Bloom, B.R., Jha, P., Eds.; The International Bank for Reconstruction and Development/The World Bank. © 2017 International Bank for Reconstruction and Development; The World Bank: Washington, DC, USA, 2017. [Google Scholar]
- Robbins, H.A.; Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Epidemiologic contributions to recent cancer trends among HIV-infected people in the United States. Aids 2014, 28, 881–890. [Google Scholar] [CrossRef]
- Coghill, A.E.; Shiels, M.S.; Suneja, G.; Engels, E.A. Elevated Cancer-Specific Mortality Among HIV-Infected Patients in the United States. J. Clin. Oncol. 2015, 33, 2376–2383. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Engels, E.A. Age at cancer diagnosis among persons with AIDS in the United States. Ann. Intern. Med. 2010, 153, 452–460. [Google Scholar] [CrossRef]
- Stella, S.; Vitale, S.R.; Martorana, F.; Massimino, M.; Pavone, G.; Lanzafame, K.; Bianca, S.; Barone, C.; Gorgone, C.; Fichera, M.; et al. Mutational Analysis of BRCA1 and BRCA2 Genes in Breast Cancer Patients from Eastern Sicily. Cancer Manag. Res. 2022, 14, 1341–1352. [Google Scholar] [CrossRef]
- Sun, Y.S.; Zhao, Z.; Yang, Z.N.; Xu, F.; Lu, H.J.; Zhu, Z.Y.; Shi, W.; Jiang, J.; Yao, P.P.; Zhu, H.P. Risk Factors and Preventions of Breast Cancer. Int. J. Biol. Sci. 2017, 13, 1387–1397. [Google Scholar] [CrossRef] [PubMed]
- D’Andrea, F.; Ceccarelli, M.; Facciolà, A.; Nunnari, G.; Pellicanò, G.F.; Venanzi Rullo, E. Breast cancer in women living with HIV. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 1158–1164. [Google Scholar] [CrossRef]
- Cubasch, H.; Ruff, P.; Joffe, M.; Norris, S.; Chirwa, T.; Nietz, S.; Sharma, V.; Duarte, R.; Buccimazza, I.; Čačala, S.; et al. South African Breast Cancer and HIV Outcomes Study: Methods and Baseline Assessment. J. Glob. Oncol. 2017, 3, 114–124. [Google Scholar] [CrossRef]
- Santucci, C.; Carioli, G.; Bertuccio, P.; Malvezzi, M.; Pastorino, U.; Boffetta, P.; Negri, E.; Bosetti, C.; La Vecchia, C. Progress in cancer mortality, incidence, and survival: A global overview. Eur. J. Cancer Prev. 2020, 29, 367–381. [Google Scholar] [CrossRef]
- Ruffieux, Y.; Dhokotera, T.; Muchengeti, M.; Bartels, L.; Olago, V.; Bohlius, J.; Singh, E.; Egger, M.; Rohner, E. Cancer risk in adolescents and young adults living with HIV in South Africa: A nationwide cohort study. Lancet HIV 2021, 8, e614–e622. [Google Scholar] [CrossRef]
- Sung, H.; Rosenberg, P.S.; Chen, W.Q.; Hartman, M.; Lim, W.Y.; Chia, K.S.; Wai-Kong Mang, O.; Chiang, C.J.; Kang, D.; Ngan, R.K.; et al. Female breast cancer incidence among Asian and Western populations: More similar than expected. J. Natl. Cancer Inst. 2015, 107, djv107. [Google Scholar] [CrossRef]
- Chasimpha, S.; McCormack, V.; Cubasch, H.; Joffe, M.; Zietsman, A.; Galukande, M.; Parham, G.; Pinder, L.F.; Anele, A.; Adisa, C.A.; et al. Disparities in breast cancer survival between women with and without HIV across sub-Saharan Africa (ABC-DO): A prospective, cohort study. Lancet HIV 2022, 9, e160–e171. [Google Scholar] [CrossRef]
- Caccuri, F.; Giordano, F.; Barone, I.; Mazzuca, P.; Giagulli, C.; Andò, S.; Caruso, A.; Marsico, S. HIV-1 matrix protein p17 and its variants promote human triple negative breast cancer cell aggressiveness. Infect. Agents Cancer 2017, 12, 49. [Google Scholar] [CrossRef]
- Micali, C.; Russotto, Y.; Facciolà, A.; Marino, A.; Celesia, B.M.; Pistarà, E.; Caci, G.; Nunnari, G.; Pellicanò, G.F.; Venanzi Rullo, E. Pulmonary Kaposi Sarcoma without Respiratory Symptoms and Skin Lesions in an HIV-Naïve Patient: A Case Report and Literature Review. Infect. Dis. Rep. 2022, 14, 228–242. [Google Scholar] [CrossRef]
- Celesia, B.M.; Marino, A.; Del Vecchio, R.F.; Bruno, R.; Palermo, F.; Gussio, M.; Nunnari, G.; Cacopardo, B. Is it Safe and Cost Saving to Defer the CD4+ Cell Count Monitoring in Stable Patients on Art with More than 350 or 500 cells/μL? Mediterr. J. Hematol. Infect. Dis. 2019, 11, e2019063. [Google Scholar] [CrossRef] [PubMed]
- Hiam-Galvez, K.J.; Allen, B.M.; Spitzer, M.H. Systemic immunity in cancer. Nat. Rev. Cancer 2021, 21, 345–359. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; van Leeuwen, M.T.; Falster, M.O.; Vajdic, C.M. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: A meta-analysis. Lancet 2007, 370, 59–67. [Google Scholar] [CrossRef] [PubMed]
- Franceschi, S.; Lise, M.; Clifford, G.M.; Rickenbach, M.; Levi, F.; Maspoli, M.; Bouchardy, C.; Dehler, S.; Jundt, G.; Ess, S.; et al. Changing patterns of cancer incidence in the early- and late-HAART periods: The Swiss HIV Cohort Study. Br. J. Cancer 2010, 103, 416–422. [Google Scholar] [CrossRef]
- Wu, Q.; Deng, L.; Cao, Y.; Lian, S. Preoperative Biomarkers and Survival in Chinese Breast Cancer Patients with HIV: A Propensity-Score-Matched-Cohort Study. Viruses 2023, 15, 1490. [Google Scholar] [CrossRef] [PubMed]
- Spano, J.P.; Lanoy, E.; Mounier, N.; Katlama, C.; Costagliola, D.; Heard, I. Breast cancer among HIV infected individuals from the ONCOVIH study, in France: Therapeutic implications. Eur. J. Cancer 2012, 48, 3335–3341. [Google Scholar] [CrossRef]
- Ayeni, O.A.; O’Neil, D.S.; Pumpalova, Y.S.; Chen, W.C.; Nietz, S.; Phakathi, B.; Buccimazza, I.; Čačala, S.; Stopforth, L.W.; Farrow, H.A.; et al. Impact of HIV infection on survival among women with stage I-III breast cancer: Results from the South African breast cancer and HIV outcomes study. Int. J. Cancer 2022, 151, 209–221. [Google Scholar] [CrossRef] [PubMed]
- Celesia, B.M.; Marino, A.; Borracino, S.; Arcadipane, A.F.; Pantò, G.; Gussio, M.; Coniglio, S.; Pennisi, A.; Cacopardo, B.; Panarello, G. Successful Extracorporeal Membrane Oxygenation Treatment in an Acquired Immune Deficiency Syndrome (AIDS) Patient with Acute Respiratory Distress Syndrome (ARDS) Complicating Pneumocystis jirovecii Pneumonia: A Challenging Case. Am. J. Case Rep. 2020, 21, e919570. [Google Scholar] [CrossRef] [PubMed]
- Quiros-Roldan, E.; Properzi, M.; Paghera, S.; Raffetti, E.; Castelli, F.; Imberti, L. Factors associated with immunosenescence during early adulthood in HIV-infected patients after durable efficient combination antiretroviral therapy. Sci. Rep. 2020, 10, 10057. [Google Scholar] [CrossRef]
- Lv, T.; Cao, W.; Li, T. HIV-Related Immune Activation and Inflammation: Current Understanding and Strategies. J. Immunol. Res. 2021, 2021, 7316456. [Google Scholar] [CrossRef]
- Belzile, J.P.; Duisit, G.; Rougeau, N.; Mercier, J.; Finzi, A.; Cohen, E.A. HIV-1 Vpr-mediated G2 arrest involves the DDB1-CUL4AVPRBP E3 ubiquitin ligase. PLoS Pathog. 2007, 3, e85. [Google Scholar] [CrossRef]
- Foster, J.L.; Garcia, J.V. HIV-1 Nef: At the crossroads. Retrovirology 2008, 5, 84. [Google Scholar] [CrossRef]
- Mavigner, M.; Delobel, P.; Cazabat, M.; Dubois, M.; L’Faqihi-Olive, F.E.; Raymond, S.; Pasquier, C.; Marchou, B.; Massip, P.; Izopet, J. HIV-1 residual viremia correlates with persistent T-cell activation in poor immunological responders to combination antiretroviral therapy. PLoS ONE 2009, 4, e7658. [Google Scholar] [CrossRef]
- Cummins, N.W.; Badley, A.D. Mechanisms of HIV-associated lymphocyte apoptosis: 2010. Cell Death Dis. 2010, 1, e99. [Google Scholar] [CrossRef] [PubMed]
- Deeks, S.G.; Tracy, R.; Douek, D.C. Systemic effects of inflammation on health during chronic HIV infection. Immunity 2013, 39, 633–645. [Google Scholar] [CrossRef]
- Zicari, S.; Sessa, L.; Cotugno, N.; Ruggiero, A.; Morrocchi, E.; Concato, C.; Rocca, S.; Zangari, P.; Manno, E.C.; Palma, P. Immune Activation, Inflammation, and Non-AIDS Co-Morbidities in HIV-Infected Patients under Long-Term ART. Viruses 2019, 11, 200. [Google Scholar] [CrossRef] [PubMed]
- Isaguliants, M.; Bayurova, E.; Avdoshina, D.; Kondrashova, A.; Chiodi, F.; Palefsky, J.M. Oncogenic Effects of HIV-1 Proteins, Mechanisms Behind. Cancers 2021, 13, 305. [Google Scholar] [CrossRef] [PubMed]
- Clifford, G.M.; Franceschi, S. Cancer risk in HIV-infected persons: Influence of CD4+ count. Future Oncol. 2009, 5, 669–678. [Google Scholar] [CrossRef] [PubMed]
- Brandão, M.; Bruzzone, M.; Franzoi, M.A.; De Angelis, C.; Eiger, D.; Caparica, R.; Piccart-Gebhart, M.; Buisseret, L.; Ceppi, M.; Dauby, N.; et al. Impact of HIV infection on baseline characteristics and survival of women with breast cancer. Aids 2021, 35, 605–618. [Google Scholar] [CrossRef] [PubMed]
- Hessol, N.A.; Pipkin, S.; Schwarcz, S.; Cress, R.D.; Bacchetti, P.; Scheer, S. The impact of highly active antiretroviral therapy on non-AIDS-defining cancers among adults with AIDS. Am. J. Epidemiol. 2007, 165, 1143–1153. [Google Scholar] [CrossRef] [PubMed]
- Goedert, J.J.; Schairer, C.; McNeel, T.S.; Hessol, N.A.; Rabkin, C.S.; Engels, E.A. for the HIV/AIDS Cancer Match Study. Risk of breast, ovary, and uterine corpus cancers among 85 268 women with AIDS. Br. J. Cancer 2006, 95, 642–648. [Google Scholar] [CrossRef] [PubMed]
- Ruiz, M.; Davis, H. Breast Cancer in HIV-Infected Patients: A Retrospective Single-Institution Study. J. Int. Assoc. Physicians AIDS Care 2011, 10, 30–34. [Google Scholar] [CrossRef] [PubMed]
- Hessol, N.A.; Napolitano, L.A.; Smith, D.; Lie, Y.; Levine, A.; Young, M.; Cohen, M.; Minkoff, H.; Anastos, K.; D’Souza, G.; et al. HIV tropism and decreased risk of breast cancer. PLoS ONE 2010, 5, e14349. [Google Scholar] [CrossRef]
- Spano, J.P.; Costagliola, D.; Katlama, C.; Mounier, N.; Oksenhendler, E.; Khayat, D. AIDS-related malignancies: State of the art and therapeutic challenges. J. Clin. Oncol. 2008, 26, 4834–4842. [Google Scholar] [CrossRef]
- Grover, S.; Martei, Y.M.; Puri, P.; Prabhakar, P.; Mutebi, M.; Balogun, O.D.; Price, A.J.; Freeman, A.H.; Narasimhamurthy, M.; Rodin, D.; et al. Breast Cancer and HIV in Sub-Saharan Africa: A Complex Relationship. J. Glob. Oncol. 2018, 4, 1–11. [Google Scholar] [CrossRef]
- Pogo, B.G.; Holland, J.F. Possibilities of a viral etiology for human breast cancer. A review. Biol. Trace Elem. Res. 1997, 56, 131–142. [Google Scholar] [CrossRef]
- Rakowicz-Szulczynska, E.M.; Jackson, B.; Szulczynska, A.M.; Smith, M. Human immunodeficiency virus type 1-like DNA sequences and immunoreactive viral particles with unique association with breast cancer. Clin. Diagn. Lab. Immunol. 1998, 5, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Liu, B.; Wang, Y.; Melana, S.M.; Pelisson, I.; Najfeld, V.; Holland, J.F.; Pogo, B.G. Identification of a proviral structure in human breast cancer. Cancer Res. 2001, 61, 1754–1759. [Google Scholar] [PubMed]
- Global, regional, and national incidence, prevalence, and mortality of HIV, 1980-2017, and forecasts to 2030, for 195 countries and territories: A systematic analysis for the Global Burden of Diseases, Injuries, and Risk Factors Study 2017. Lancet HIV 2019, 6, e831–e859. [CrossRef] [PubMed]
- Cubasch, H.; Joffe, M.; Hanisch, R.; Schuz, J.; Neugut, A.I.; Karstaedt, A.; Broeze, N.; van den Berg, E.; McCormack, V.; Jacobson, J.S. Breast cancer characteristics and HIV among 1,092 women in Soweto, South Africa. Breast Cancer Res. Treat. 2013, 140, 177–186. [Google Scholar] [CrossRef] [PubMed]
- Phakathi, B.; Cubasch, H.; Nietz, S.; Dickens, C.; Dix-Peek, T.; Joffe, M.; Neugut, A.I.; Jacobson, J.; Duarte, R.; Ruff, P. Clinico-pathological characteristics among South African women with breast cancer receiving anti-retroviral therapy for HIV. Breast 2019, 43, 123–129. [Google Scholar] [CrossRef] [PubMed]
- van Zyl, N.; Minné, C.; Mokone, D.H. Human immunodeficiency virus infection in breast cancer patients: The prevalence thereof and its effect on breast cancer characteristics at Dr. George Mukhari Academic Hospital Breast Clinic, Ga-Rankuwa, South Africa. SA J. Radiol. 2018, 22, 1361. [Google Scholar] [CrossRef]
- Pumpalova, Y.S.; Ayeni, O.A.; Chen, W.C.; O’Neil, D.S.; Nietz, S.; Phakathi, B.; Buccimazza, I.; Čačala, S.; Stopforth, L.W.; Farrow, H.A.; et al. Impact of HIV infection on overall survival among women with stage IV breast cancer in South Africa. Breast Cancer Res. Treat. 2021, 189, 285–296. [Google Scholar] [CrossRef]
- Bhatia, R.K.; Narasimhamurthy, M.; Martei, Y.M.; Prabhakar, P.; Hutson, J.; Chiyapo, S.; Makozhombwe, I.; Feldman, M.; Kayembe, M.K.A.; Cooper, K.; et al. Report of clinico-pathological features of breast cancer in HIV-infected and uninfected women in Botswana. Infect. Agents Cancer 2019, 14, 28. [Google Scholar] [CrossRef]
- Phakathi, B.; Nietz, S.; Cubasch, H.; Dickens, C.; Dix-Peek, T.; Joffe, M.; Neugut, A.I.; Jacobson, J.; Duarte, R.; Ruff, P. Survival of south african women with breast cancer receiving anti-retroviral therapy for HIV. Breast 2021, 59, 27–36. [Google Scholar] [CrossRef]
- Phakathi, B.; Dix-Peek, T.; Van Den Berg, E.; Dickens, C.; Nietz, S.; Cubasch, H.; Joffe, M.; Neugut, A.I.; Jacobson, J.S.; Ruff, P.; et al. PAM50 intrinsic subtypes, risk of recurrence score and breast cancer survival in HIV-positive and HIV-negative patients-a South African cohort study. Breast Cancer Res. Treat. 2023, 200, 337–346. [Google Scholar] [CrossRef]
- Coghill, A.E.; Han, X.; Suneja, G.; Lin, C.C.; Jemal, A.; Shiels, M.S. Advanced stage at diagnosis and elevated mortality among US patients with cancer infected with HIV in the National Cancer Data Base. Cancer 2019, 125, 2868–2876. [Google Scholar] [CrossRef]
- McKenzie, F.; Zietsman, A.; Galukande, M.; Anele, A.; Adisa, C.; Parham, G.; Pinder, L.; Cubasch, H.; Joffe, M.; Kidaaga, F.; et al. Drivers of advanced stage at breast cancer diagnosis in the multicountry African breast cancer—Disparities in outcomes (ABC-DO) study. Int. J. Cancer 2018, 142, 1568–1579. [Google Scholar] [CrossRef]
- Brandão, M.; Guisseve, A.; Bata, G.; Alberto, M.; Ferro, J.; Garcia, C.; Zaqueu, C.; Lorenzoni, C.; Leitão, D.; Come, J.; et al. Breast cancer subtypes: Implications for the treatment and survival of patients in Africa-a prospective cohort study from Mozambique. ESMO Open 2020, 5, e000829. [Google Scholar] [CrossRef]
- Howlader, N.; Altekruse, S.F.; Li, C.I.; Chen, V.W.; Clarke, C.A.; Ries, L.A.; Cronin, K.A. US incidence of breast cancer subtypes defined by joint hormone receptor and HER2 status. J. Natl. Cancer Inst. 2014, 106, dju055. [Google Scholar] [CrossRef]
- Caro-Vegas, C.; Ramirez, C.; Landis, J.; Adimora, A.A.; Strickler, H.; French, A.L.; Ofotokun, I.; Fischl, M.; Seaberg, E.C.; Wang, C.J.; et al. Molecular profiling of breast and lung cancer in women with HIV reveals high tumor mutational burden. Aids 2022, 36, 567–571. [Google Scholar] [CrossRef]
- Chasimpha, S.; Silva, I.d.S.; Martei, Y.M.; Grover, S.; Cubasch, H.; McCormack, V. Survival Disparities Between Patients with Breast Cancer With and Without HIV: A Research Framework. JCO Glob. Oncol. 2023, 9, e2200330. [Google Scholar] [CrossRef]
- Nietz, S.; O’Neil, D.S.; Ayeni, O.; Chen, W.C.; Joffe, M.; Jacobson, J.S.; Neugut, A.I.; Ruff, P.; Mapanga, W.; Buccimazza, I.; et al. A comparison of complete pathologic response rates following neoadjuvant chemotherapy among South African breast cancer patients with and without concurrent HIV infection. Breast Cancer Res. Treat. 2020, 184, 861–872. [Google Scholar] [CrossRef] [PubMed]
- Martei, Y.M.; Narasimhamurthy, M.; Setlhako, D.I.; Ayane, G.; Ralefala, T.; Chiyapo, S.; Gross, R.; Shulman, L.N.; Grover, S.; DeMichele, A. Relative Dose Intensity and Pathologic Response Rates in Patients With Breast Cancer and With and Without HIV Who Received Neoadjuvant Chemotherapy. JCO Glob. Oncol. 2022, 8, e2200016. [Google Scholar] [CrossRef] [PubMed]
- Strazzanti, A.; Martorana, F.; Intagliata, E.; Lanzafame, K.; Pavone, G.; Mauro, S.; Santi, G.; Manzella, L.; Basile, F.; Trovato, C. Implications of Antidepressants Use in Breast Cancer: A Brief Review. Surg. Gastroenterol. Oncol. 2020, 25, 229–235. [Google Scholar] [CrossRef]
- Strope, J.D.; Lochrin, S.E.; Sissung, T.M.; Kem, R.; Chandrasekaran, P.; Sharon, E.; Price, D.K.; Uldrick, T.S.; Yarchoan, R.; Figg, W.D. Drug-drug Interactions in Patients with HIV and Cancer in Sub-Saharan Africa. AIDS Rev. 2020, 23, 13–27. [Google Scholar] [CrossRef] [PubMed]
- Suneja, G.; Boyer, M.; Yehia, B.R.; Shiels, M.S.; Engels, E.A.; Bekelman, J.E.; Long, J.A. Cancer Treatment in Patients With HIV Infection and Non–AIDS-Defining Cancers: A Survey of US Oncologists. J. Oncol. Pract. 2015, 11, e380–e387. [Google Scholar] [CrossRef]
- Coghill, A.E.; Suneja, G.; Rositch, A.F.; Shiels, M.S.; Engels, E.A. HIV Infection, Cancer Treatment Regimens, and Cancer Outcomes Among Elderly Adults in the United States. JAMA Oncol. 2019, 5, e191742. [Google Scholar] [CrossRef] [PubMed]
- Reid, E.; Suneja, G.; Ambinder, R.F.; Ard, K.; Baiocchi, R.; Barta, S.K.; Carchman, E.; Cohen, A.; Gupta, N.; Johung, K.L.; et al. Cancer in People Living With HIV, Version 1.2018, NCCN Clinical Practice Guidelines in Oncology. J. Natl. Compr. Canc Netw. 2018, 16, 986–1017. [Google Scholar] [CrossRef]
- Medscape Drug Interaction Checker. Available online: https://reference.medscape.com/drug-interactionchecker (accessed on 22 January 2024).
- Interaction Report, University of Liverpool. Available online: https://www.hiv-druginteractions.org/checker (accessed on 24 January 2024).
- Drug Interactions Checker, PEPID, LLC. Evanston, IL. Available online: https://pepid.com (accessed on 24 January 2024).
- Berretta, M.; Di Francia, R.; Stanzione, B.; Facchini, G.; Lleshi, A.; De Paoli, P.; Spina, M.; Tirelli, U. New treatment strategies for HIV-positive cancer patients undergoing antiblastic chemotherapy. Expert. Opin. Pharmacother. 2016, 17, 2391–2403. [Google Scholar] [CrossRef] [PubMed]
- Rudek, M.A.; Flexner, C.; Ambinder, R.F. Use of antineoplastic agents in patients with cancer who have HIV/AIDS. Lancet Oncol. 2011, 12, 905–912. [Google Scholar] [CrossRef] [PubMed]
- Beumer, J.H.; Venkataramanan, R.; Rudek, M.A. Pharmacotherapy in cancer patients with HIV/AIDS. Clin. Pharmacol. Ther. 2014, 95, 370–372. [Google Scholar] [CrossRef] [PubMed]
- Dubrow, R.; Silverberg, M.J.; Park, L.S.; Crothers, K.; Justice, A.C. HIV infection, aging, and immune function: Implications for cancer risk and prevention. Curr. Opin. Oncol. 2012, 24, 506–516. [Google Scholar] [CrossRef] [PubMed]
- Bertholee, D.; Maring, J.G.; van Kuilenburg, A.B.P. Genotypes Affecting the Pharmacokinetics of Anticancer Drugs. Clin. Pharmacokinet. 2017, 56, 317–337. [Google Scholar] [CrossRef] [PubMed]
- Kozal, M.; Aberg, J.; Pialoux, G.; Cahn, P.; Thompson, M.; Molina, J.M.; Grinsztejn, B.; Diaz, R.; Castagna, A.; Kumar, P.; et al. Fostemsavir in Adults with Multidrug-Resistant HIV-1 Infection. N. Engl. J. Med. 2020, 382, 1232–1243. [Google Scholar] [CrossRef]
- Berretta, M.; Facchini, B.A.; Colpani, A.; Di Francia, R.; Montopoli, M.; Pellicanò, G.; Tirelli, U.; Fiorica, F.; Ottaiano, A.; Madeddu, G.; et al. New treatment strategies for HIV-positive cancer patients undergoing anticancer medical treatment: Update of the literature. Eur. Rev. Med. Pharmacol. Sci. 2023, 27, 4185–4201. [Google Scholar] [CrossRef]
- Emu, B.; Fessel, J.; Schrader, S.; Kumar, P.; Richmond, G.; Win, S.; Weinheimer, S.; Marsolais, C.; Lewis, S. Phase 3 Study of Ibalizumab for Multidrug-Resistant HIV-1. N. Engl. J. Med. 2018, 379, 645–654. [Google Scholar] [CrossRef] [PubMed]
- Beccari, M.V.; Mogle, B.T.; Sidman, E.F.; Mastro, K.A.; Asiago-Reddy, E.; Kufel, W.D. Ibalizumab, a Novel Monoclonal Antibody for the Management of Multidrug-Resistant HIV-1 Infection. Antimicrob. Agents Chemother. 2019, 63, 10–1128. [Google Scholar] [CrossRef] [PubMed]
- Makinson, A.; Pujol, J.L.; Le Moing, V.; Peyriere, H.; Reynes, J. Interactions between cytotoxic chemotherapy and antiretroviral treatment in human immunodeficiency virus-infected patients with lung cancer. J. Thorac. Oncol. 2010, 5, 562–571. [Google Scholar] [CrossRef] [PubMed]
- LiverTox: Clinical and Research Information on Drug-Induced Liver Injury [Internet]; National Institute of Diabetes and Digestive and Kidney Diseases: Bethesda, MD, USA, 2012.
- Nachega, J.B.; Scarsi, K.K.; Gandhi, M.; Scott, R.K.; Mofenson, L.M.; Archary, M.; Nachman, S.; Decloedt, E.; Geng, E.H.; Wilson, L.; et al. Long-acting antiretrovirals and HIV treatment adherence. Lancet HIV 2023, 10, e332–e342. [Google Scholar] [CrossRef]
- Mounier, N.; Katlama, C.; Costagliola, D.; Chichmanian, R.M.; Spano, J.P. Drug interactions between antineoplastic and antiretroviral therapies: Implications and management for clinical practice. Crit. Rev. Oncol. Hematol. 2009, 72, 10–20. [Google Scholar] [CrossRef]




Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marino, A.; Pavone, G.; Martorana, F.; Fisicaro, V.; Motta, L.; Spampinato, S.; Celesia, B.M.; Cacopardo, B.; Vigneri, P.; Nunnari, G. Navigating the Nexus: HIV and Breast Cancer—A Critical Review. Int. J. Mol. Sci. 2024, 25, 3222. https://doi.org/10.3390/ijms25063222
Marino A, Pavone G, Martorana F, Fisicaro V, Motta L, Spampinato S, Celesia BM, Cacopardo B, Vigneri P, Nunnari G. Navigating the Nexus: HIV and Breast Cancer—A Critical Review. International Journal of Molecular Sciences. 2024; 25(6):3222. https://doi.org/10.3390/ijms25063222
Chicago/Turabian StyleMarino, Andrea, Giuliana Pavone, Federica Martorana, Viviana Fisicaro, Lucia Motta, Serena Spampinato, Benedetto Maurizio Celesia, Bruno Cacopardo, Paolo Vigneri, and Giuseppe Nunnari. 2024. "Navigating the Nexus: HIV and Breast Cancer—A Critical Review" International Journal of Molecular Sciences 25, no. 6: 3222. https://doi.org/10.3390/ijms25063222