
Impact of Immunopathy and Coagulopathy on Multi-Organ Failure and Mortality in a Lethal Porcine Model of Controlled and Uncontrolled Hemorrhage

Abstract
:1. Introduction
2. Results
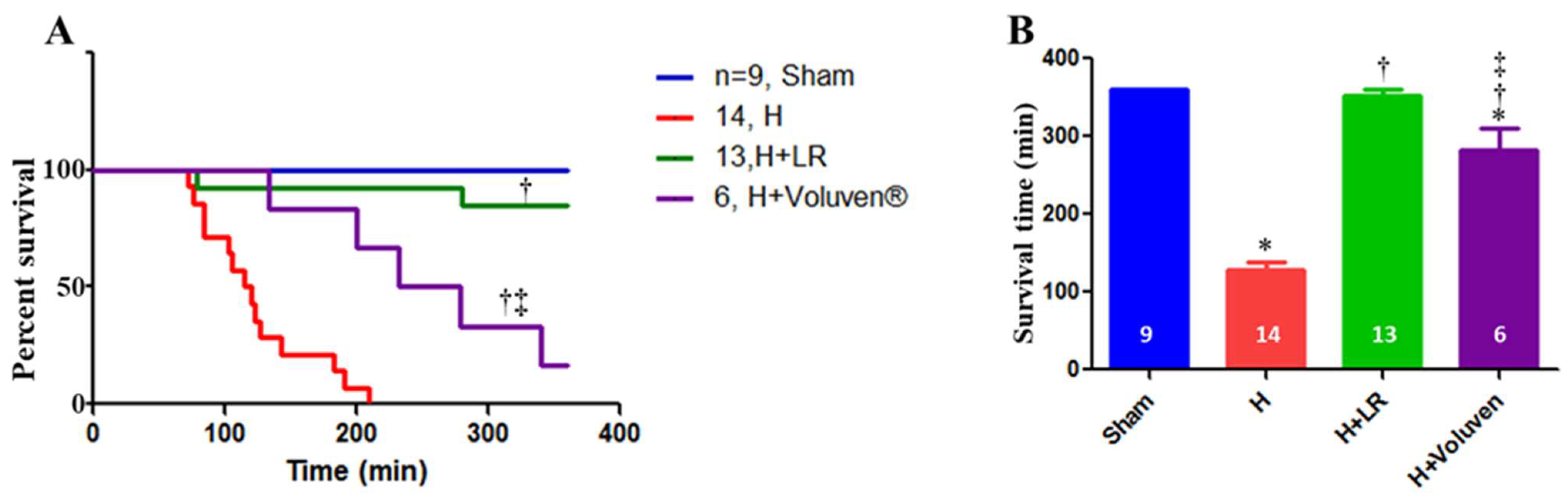
2.1. Effect of Hemorrhage and Fluid Resuscitation on Survival
2.2. Baseline Characterization and Mortality
2.3. Physiological Responses to Hemorrhage
2.4. Effects of Fluid Resuscitation on Hemodynamic and Metabolic Parameters
2.5. Effects of Fluid Resuscitation on Hemodilution and Coagulation Parameters
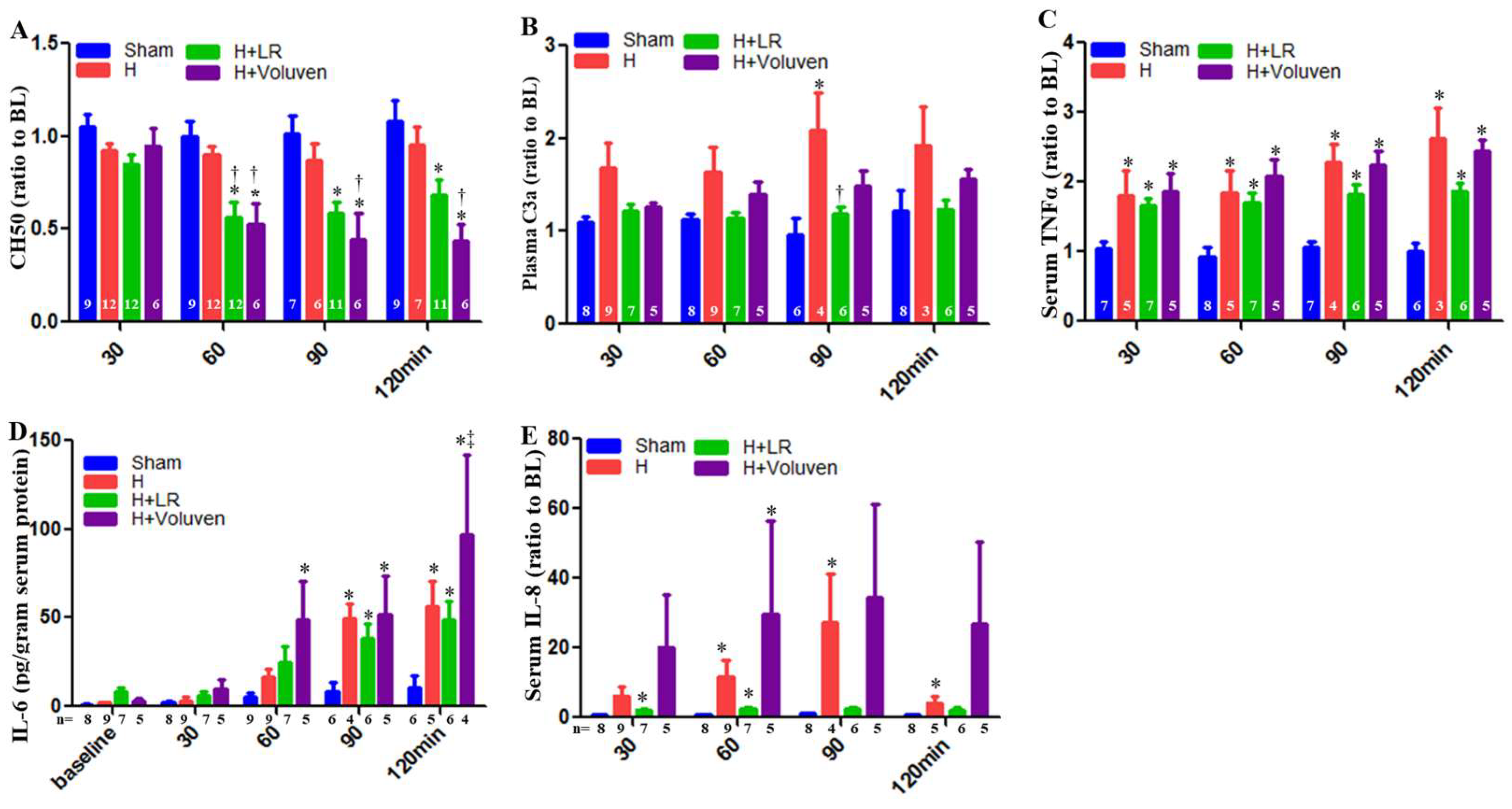
2.6. Circulating Complement Activation and Cytokine Release
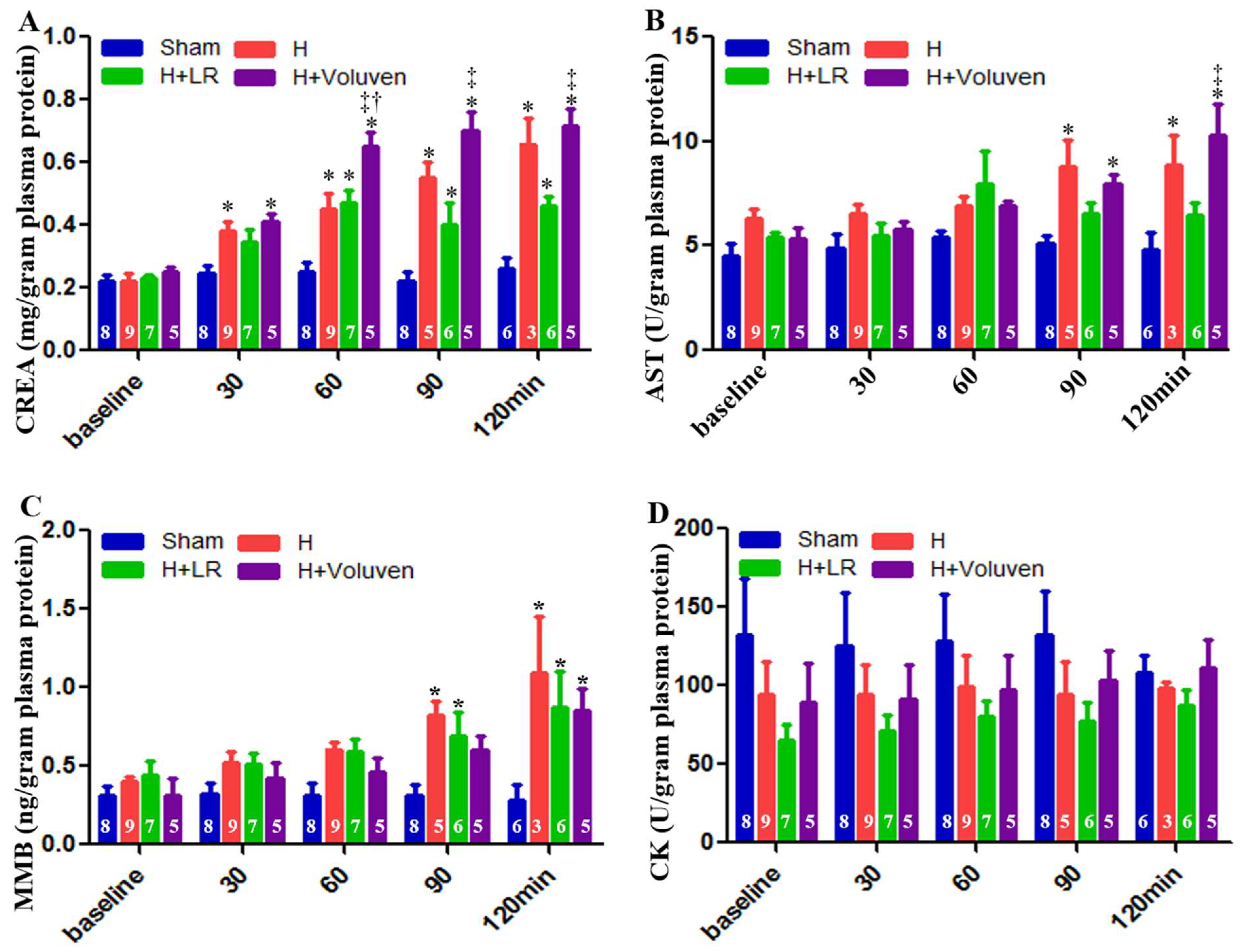
2.7. End Organ Function
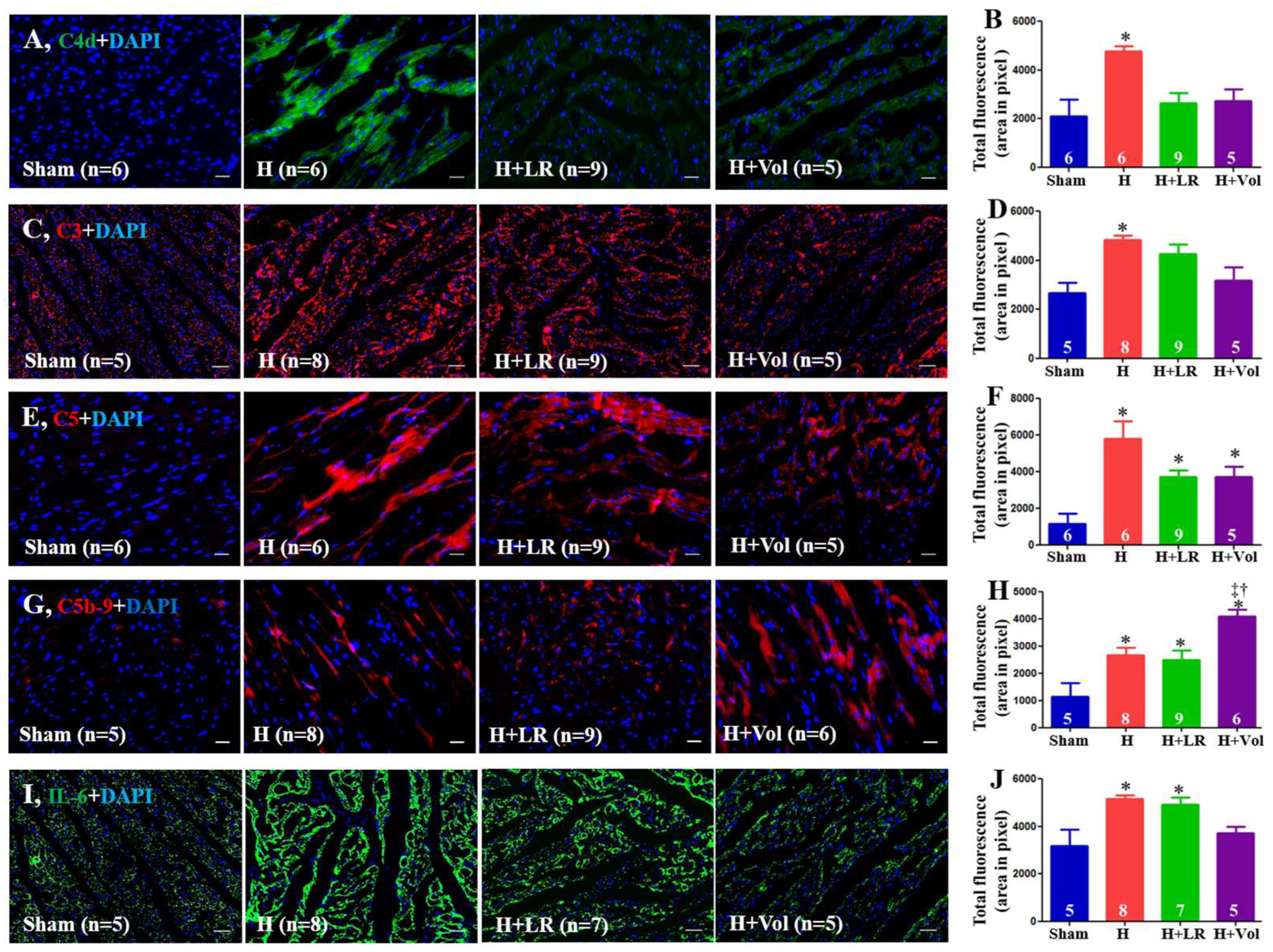
2.8. Myocardial Inflammatory Responses to Hemorrhagic Shock and Fluid Resuscitation
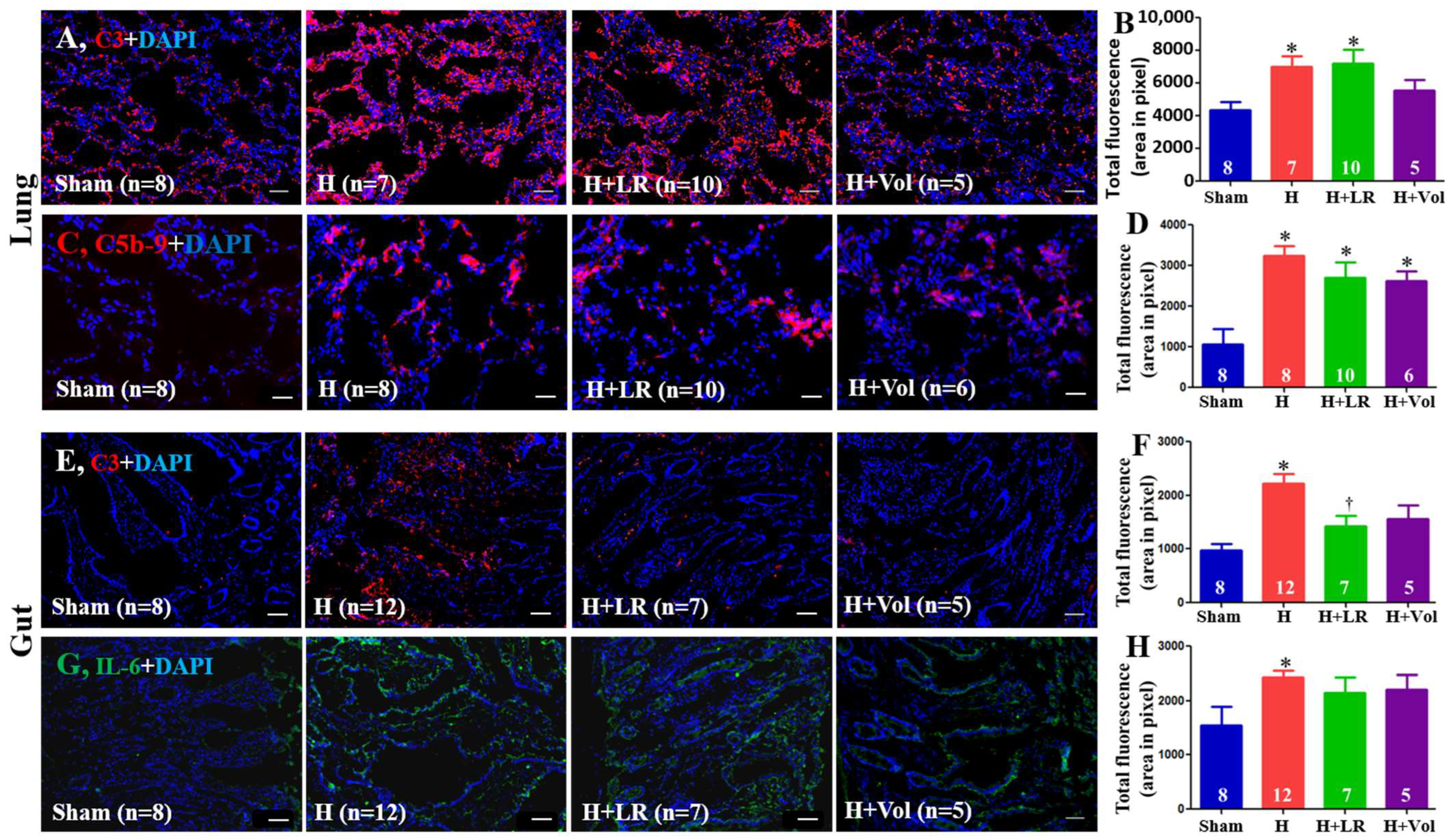
2.9. Pulmonary and Intestinal Inflammatory Responses to Hemorrhagic Shock and Fluid Resuscitation
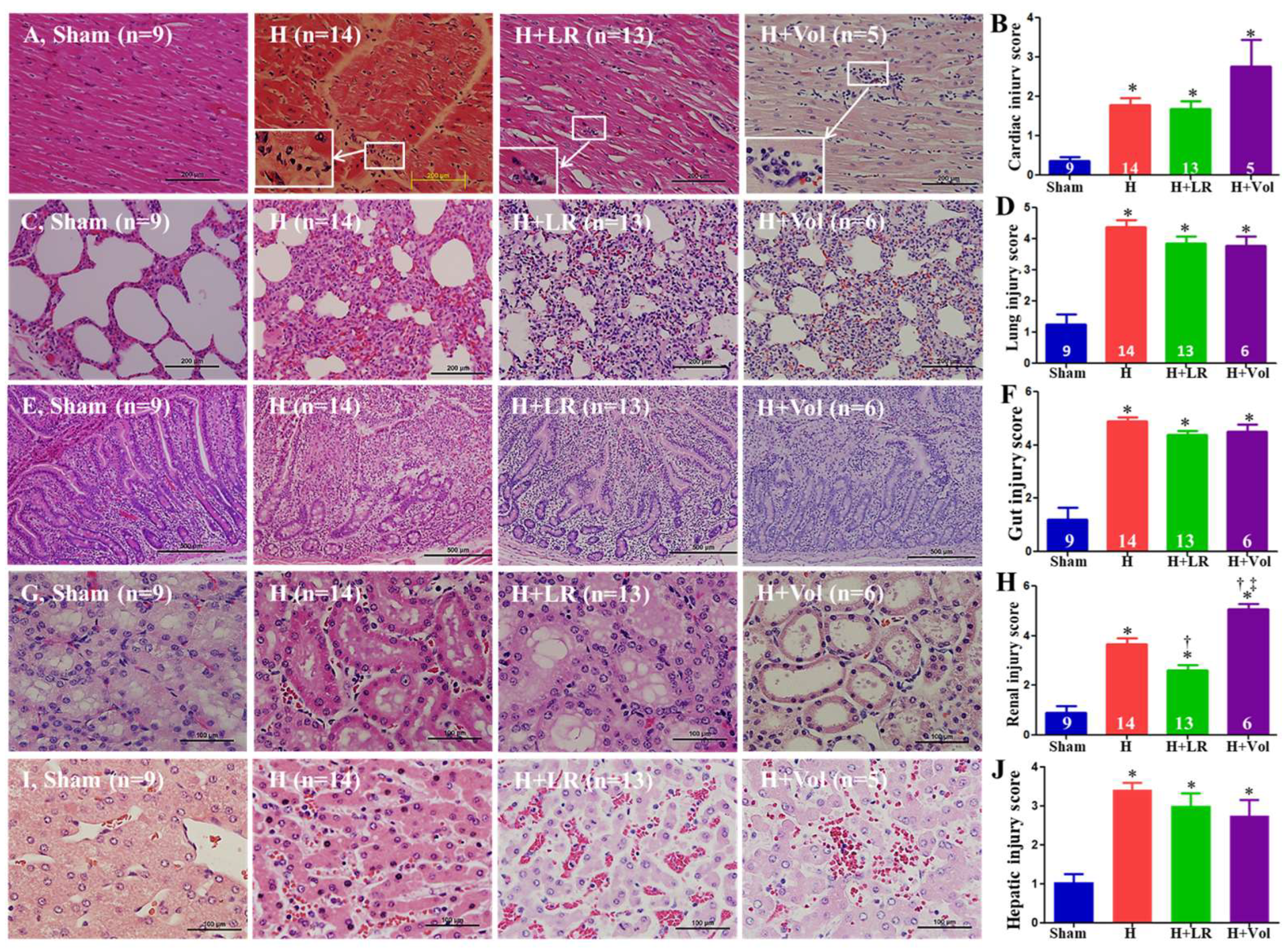
2.10. Effect of Hemorrhage and Fluid Resuscitation on Organ Histopathological Alterations
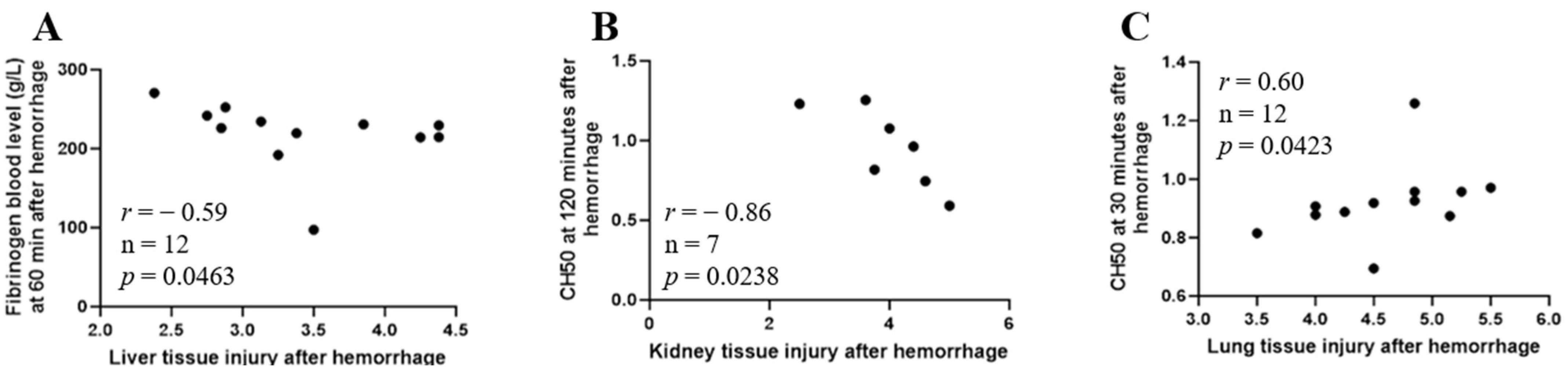
2.11. Correlation between Early Immunopathy and Coagulopathy and Organ Injury
3. Discussion
4. Conclusions
5. Materials and Methods
5.1. Animal Study
5.1.1. General Procedures
5.1.2. Surgical Preparation
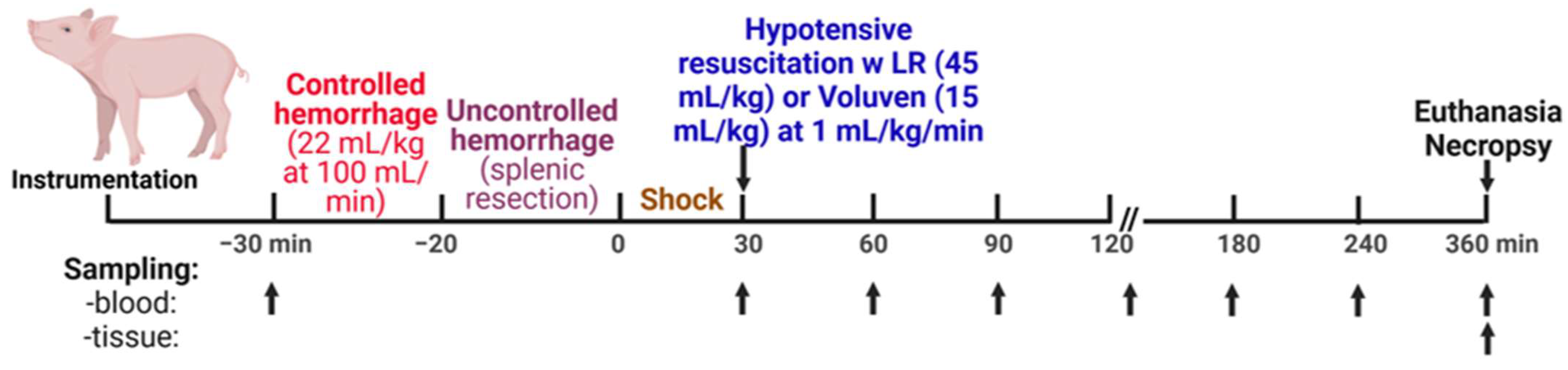
5.1.3. Experimental Design
5.1.4. Biosampling
5.2. Assays
5.2.1. Reagents and Antibodies
5.2.2. Histological Examination
5.2.3. Immunohistochemical Staining
5.2.4. Cytokine Assays
5.2.5. Quantitative Assessment of End Tissue Function
5.2.6. Measurement of Coagulation Parameters
5.2.7. Analysis of Complement Functional Activity
5.2.8. Analysis of Plasma C3a
5.2.9. Serum Protein Assay
5.3. Statistical Analysis
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Hooper, T.J.; De Pasquale, M.; Strandenes, G.; Sunde, G.; Ward, K.R. Challenges and Possibilities in Forward Resuscitation. Shock 2014, 41 (Suppl. S1), 13–20. [Google Scholar] [CrossRef]
- Gruen, R.L.; Brohi, K.; Schreiber, M.; Balogh, Z.J.; Pitt, V.; Narayan, M.; Maier, R.V. Haemorrhage Control in Severely Injured Patients. Lancet 2012, 380, 1099–1108. [Google Scholar] [CrossRef]
- Satyam, A.; Graef, E.R.; Lapchak, P.H.; Tsokos, M.G.; Dalle Lucca, J.J.; Tsokos, G.C. Complement and Coagulation Cascades in Trauma. Acute Med. Surg. 2019, 6, 329–335. [Google Scholar] [CrossRef]
- Barea-Mendoza, J.A.; Chico-Fernández, M.; Molina-Díaz, I.; Moreno-Muñoz, G.; Toboso-Casado, J.M.; Viña-Soria, L.; Matachana-Martínez, M.; Freire-Aragón, M.D.; Pérez-Bárcena, J.; Llompart-Pou, J.A. Risk Factors Associated with Early and Late Posttraumatic Multiorgan Failure: An Analysis From RETRAUCI. Shock 2021, 55, 326–331. [Google Scholar] [CrossRef] [PubMed]
- Cole, E.; Gillespie, S.; Vulliamy, P.; Brohi, K.; Organ Dysfunction in Trauma (ORDIT) Study Collaborators. Multiple Organ Dysfunction after Trauma. Br. J. Surg. 2020, 107, 402–412. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, J.; Nelson, D.; Holst, A.; Hellgren, E.; Friman, O.; Oldner, A. Temporal Patterns of Organ Dysfunction after Severe Trauma. Crit. Care 2021, 25, 165. [Google Scholar] [CrossRef]
- Hutchings, L.; Watkinson, P.; Young, J.D.; Willett, K. Defining Multiple Organ Failure after Major Trauma: A Comparison of the Denver, Sequential Organ Failure Assessment, and Marshall Scoring Systems. J. Trauma Acute Care Surg. 2017, 82, 534–541. [Google Scholar] [CrossRef]
- Ramesh, G.H.; Uma, J.C.; Farhath, S. Fluid resuscitation in trauma: What are the best strategies and fluids? Int. J. Emerg. Med. 2019, 12, 38. [Google Scholar] [CrossRef]
- Roger, C.; Muller, L.; Deras, P.; Louart, G.; Nouvellon, E.; Molinari, N.; Goret, L.; Gris, J.C.; Ripart, J.; De La Coussaye, J.E.; et al. Does the Type of Fluid Affect Rapidity of Shock Reversal in an Anaesthetized-Piglet Model of near-Fatal Controlled Haemorrhage? A Randomized Study. Br. J. Anaesth. 2014, 112, 1015–1023. [Google Scholar] [CrossRef]
- Curry, N.; Hopewell, S.; Dorée, C.; Hyde, C.; Brohi, K.; Stanworth, S. The Acute Management of Trauma Hemorrhage: A Systematic Review of Randomized Controlled Trials. Crit. Care 2011, 15, R92. [Google Scholar] [CrossRef] [PubMed]
- Bowley, D.; Barker, P.; Boffard, K. Damage Control Surgery—Concepts and Practice. J. R. Army Med. Corps 2000, 146, 176–182. [Google Scholar] [CrossRef]
- Chang, R.; Holcomb, J.B. Optimal Fluid Therapy for Traumatic Hemorrhagic Shock. Crit. Care Clin. 2017, 33, 15–36. [Google Scholar] [CrossRef]
- Samuels, J.M.; Moore, H.B.; Moore, E.E. Damage Control Resuscitation. Chirurgia 2017, 112, 514. [Google Scholar] [CrossRef] [PubMed]
- Leibner, E.; Andreae, M.; Galvagno, S.M.; Scalea, T. Damage Control Resuscitation. Clin. Exp. Emerg. Med. 2020, 7, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; Del Junco, D.J.; Fox, E.E.; Wade, C.E.; Cohen, M.J.; Schreiber, M.A.; Alarcon, L.H.; Bai, Y.; Brasel, K.J.; Bulger, E.M.; et al. The Prospective, Observational, Multicenter, Major Trauma Transfusion (PROMMTT) Study: Comparative Effectiveness of a Time-Varying Treatment with Competing Risks. JAMA Surg. 2013, 148, 127. [Google Scholar] [CrossRef] [PubMed]
- Parr, M.J.; Bouillon, B.; Brohi, K.; Dutton, R.P.; Hauser, C.J.; Hess, J.R.; Holcomb, J.B.; Kluger, Y.; Mackway-Jones, K.; Rizoli, S.B.; et al. Traumatic Coagulopathy: Where Are the Good Experimental Models? J. Trauma Inj. Infect. Crit. Care 2008, 65, 766–771. [Google Scholar] [CrossRef] [PubMed]
- Curry, N.; Davis, P.W. What’s New in Resuscitation Strategies for the Patient with Multiple Trauma? Injury 2012, 43, 1021–1028. [Google Scholar] [CrossRef] [PubMed]
- Moore, E.E.; Moore, H.B.; Kornblith, L.Z.; Neal, M.D.; Hoffman, M.; Mutch, N.J.; Schöchl, H.; Hunt, B.J.; Sauaia, A. Trauma-Induced Coagulopathy. Nat. Rev. Dis. Primers 2021, 7, 30. [Google Scholar] [CrossRef] [PubMed]
- Snyder, C.W.; Weinberg, J.A.; McGwin, G.; Melton, S.M.; George, R.L.; Reiff, D.A.; Cross, J.M.; Hubbard-Brown, J.; Rue, L.W.; Kerby, J.D. The Relationship of Blood Product Ratio to Mortality: Survival Benefit or Survival Bias? J. Trauma Inj. Infect. Crit. Care 2009, 66, 358–364. [Google Scholar] [CrossRef] [PubMed]
- MacLeod, J.B.A.; Lynn, M.; McKenney, M.G.; Cohn, S.M.; Murtha, M. Early Coagulopathy Predicts Mortality in Trauma. J. Trauma. 2003, 55, 39–44. [Google Scholar] [CrossRef]
- Maegele, M.; Lefering, R.; Yucel, N.; Tjardes, T.; Rixen, D.; Paffrath, T.; Simanski, C.; Neugebauer, E.; Bouillon, B. Early Coagulopathy in Multiple Injury: An Analysis from the German Trauma Registry on 8724 Patients. Injury 2007, 38, 298–304. [Google Scholar] [CrossRef] [PubMed]
- Karmaniolou, I.I.; Theodoraki, K.A.; Orfanos, N.F.; Kostopanagiotou, G.G.; Smyrniotis, V.E.; Mylonas, A.I.; Arkadopoulos, N.F. Resuscitation after Hemorrhagic Shock: The Effect on the Liver—A Review of Experimental Data. J. Anesth. 2013, 27, 447–460. [Google Scholar] [CrossRef]
- Waxman, K. Shock: Ischemia, Reperfusion, and Inflammation. New Horiz. 1996, 4, 153–160. [Google Scholar] [PubMed]
- Chakraborty, R.K.; Burns, B. Systemic Inflammatory Response Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Maiden, M.J.; Chapman, M.J. Multiple Organ Dysfunction Syndrome. In Oh’s Intensive Care Manual; Elsevier: Amsterdam, The Netherlands, 2014; pp. 138–145.e2. [Google Scholar] [CrossRef]
- Huber-Lang, M.; Lambris, J.D.; Ward, P.A. Innate Immune Responses to Trauma. Nat. Immunol. 2018, 19, 327–341. [Google Scholar] [CrossRef]
- Huber-Lang, M.; Sarma, J.V.; Zetoune, F.S.; Rittirsch, D.; Neff, T.A.; McGuire, S.R.; Lambris, J.D.; Warner, R.L.; Flierl, M.A.; Hoesel, L.M.; et al. Generation of C5a in the Absence of C3: A New Complement Activation Pathway. Nat. Med. 2006, 12, 682–687. [Google Scholar] [CrossRef]
- Amara, U.; Flierl, M.A.; Rittirsch, D.; Klos, A.; Chen, H.; Acker, B.; Brückner, U.B.; Nilsson, B.; Gebhard, F.; Lambris, J.D.; et al. Molecular Intercommunication between the Complement and Coagulation Systems. J. Immunol. 2010, 185, 5628–5636. [Google Scholar] [CrossRef] [PubMed]
- Gulla, K.C.; Gupta, K.; Krarup, A.; Gal, P.; Schwaeble, W.J.; Sim, R.B.; O’Connor, C.D.; Hajela, K. Activation of Mannan-binding Lectin-associated Serine Proteases Leads to Generation of a Fibrin Clot. Immunology 2010, 129, 482–495. [Google Scholar] [CrossRef]
- Simovic, M.O.; Yang, Z.; Jordan, B.S.; Fraker, T.L.; Cancio, T.S.; Lucas, M.L.; Cancio, L.C.; Li, Y. Immunopathological Alterations after Blast Injury and Hemorrhage in a Swine Model of Prolonged Damage Control Resuscitation. Int. J. Mol. Sci. 2023, 24, 7494. [Google Scholar] [CrossRef]
- Yang, Z.; Aderemi, O.A.; Zhao, Q.; Edsall, P.R.; Simovic, M.O.; Lund, B.J.; Espinoza, M.D.; Woodson, A.M.; Li, Y.; Cancio, L.C. Early Complement and Fibrinolytic Activation in a Rat Model of Blast-Induced Multi-Organ Damage. Mil. Med. 2019, 184 (Suppl. S1), 282–290. [Google Scholar] [CrossRef]
- Yang, Z.; Simovic, M.O.; Liu, B.; Burgess, M.B.; Cap, A.P.; Dalle Lucca, J.J.; Li, Y. Indices of Complement Activation and Coagulation Changes in Trauma Patients. Trauma. Surg. Acute Care Open 2022, 7, e000927. [Google Scholar] [CrossRef]
- Yang, Z.; Le, T.D.; Simovic, M.O.; Liu, B.; Fraker, T.L.; Cancio, T.S.; Cap, A.P.; Wade, C.E.; Dalle Lucca, J.J.; Li, Y. Traumatized Triad of Complementopathy, Endotheliopathy, and Coagulopathy—Impact on Clinical Outcomes in Severe Polytrauma Patients. Front. Immunol. 2022, 13, 991048. [Google Scholar] [CrossRef]
- Dutton, R.P. Current Concepts in Hemorrhagic Shock. Anesthesiol. Clin. 2007, 25, 23–34. [Google Scholar] [CrossRef]
- Niles, S.E.; McLaughlin, D.F.; Perkins, J.G.; Wade, C.E.; Li, Y.; Spinella, P.C.; Holcomb, J.B. Increased Mortality Associated with the Early Coagulopathy of Trauma in Combat Casualties. J. Trauma: Inj. Infect. Crit. Care 2008, 64, 1459–1465. [Google Scholar] [CrossRef]
- Bermudez, T.; Sammani, S.; Song, J.H.; Hernon, V.R.; Kempf, C.L.; Garcia, A.N.; Burt, J.; Hufford, M.; Camp, S.M.; Cress, A.E.; et al. eNAMPT Neutralization Reduces Preclinical ARDS Severity via Rectified NFkB and Akt/mTORC2 Signaling. Sci. Rep. 2022, 12, 696. [Google Scholar] [CrossRef]
- Campbell, J.C.; Li, Y.; van Amersfoort, E.; Relan, A.; Dubick, M.; Sheppard, F.; Pusateri, A.; Niemeyer, D.; Tsokos, G.C.; Dalle Lucca, J.J. C1 Inhibitor Limits Organ Injury and Prolongs Survival in Swine Subjected to Battlefield Simulated Injury. Shock 2016, 46 (Suppl. S1), 177–188. [Google Scholar] [CrossRef]
- Carey, M.E. Analysis of Wounds Incurred by U.S. Army Seventh Corps Personnel Treated in Corps Hospitals during Operation Desert Storm, February 20 to March 10, 1991. J. Trauma: Inj. Infect. Crit. Care 1996, 40, 165S–169S. [Google Scholar] [CrossRef] [PubMed]
- Dalle Lucca, J.J.; Li, Y.; Simovic, M.O.; Slack, J.L.; Cap, A.; Falabella, M.J.; Dubick, M.; Lebeda, F.; Tsokos, G.C. Decay-Accelerating Factor Limits Hemorrhage-Instigated Tissue Injury and Improves Resuscitation Clinical Parameters. J. Surg. Res. 2013, 179, 153–167. [Google Scholar] [CrossRef]
- Huber-Lang, M.; Gebhard, F.; Schmidt, C.Q.; Palmer, A.; Denk, S.; Wiegner, R. Complement Therapeutic Strategies in Trauma, Hemorrhagic Shock and Systemic Inflammation—Closing Pandora’s Box? Semin. Immunol. 2016, 28, 278–284. [Google Scholar] [CrossRef] [PubMed]
- Karasu, E.; Nilsson, B.; Köhl, J.; Lambris, J.D.; Huber-Lang, M. Targeting Complement Pathways in Polytrauma- and Sepsis-Induced Multiple-Organ Dysfunction. Front. Immunol. 2019, 10, 543. [Google Scholar] [CrossRef] [PubMed]
- Lupu, L.; Horst, K.; Greven, J.; Mert, Ü.; Ludviksen, J.A.K.; Pettersen, K.; Lau, C.; Li, Y.; Palmer, A.; Qin, K.; et al. Simultaneous C5 and CD14 Inhibition Limits Inflammation and Organ Dysfunction in Pig Polytrauma. Front. Immunol. 2022, 13, 952267. [Google Scholar] [CrossRef] [PubMed]
- Simovic, M.O.; Falabella, M.J.; Le, T.D.; Dalle Lucca, J.J.; Li, Y. Decay-Accelerating Factor Creates an Organ-Protective Phenotype after Hemorrhage in Conscious Rats. Int. J. Mol. Sci. 2022, 23, 13563. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Nicholson, S.E.; Cancio, T.S.; Cancio, L.C.; Li, Y. Complement as a Vital Nexus of the Pathobiological Connectome for Acute Respiratory Distress Syndrome: An Emerging Therapeutic Target. Front. Immunol. 2023, 14, 1100461. [Google Scholar] [CrossRef]
- Yang, Z.; Nunn, M.A.; Le, T.D.; Simovic, M.O.; Edsall, P.R.; Liu, B.; Barr, J.L.; Lund, B.J.; Hill-Pryor, C.D.; Pusateri, A.E.; et al. Immunopathology of Terminal Complement Activation and Complement C5 Blockade Creating a Pro-Survival and Organ-Protective Phenotype in Trauma. Br. J. Pharmacol. 2023, 180, 422–440. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z.; Simovic, M.O.; Edsall, P.R.; Liu, B.; Cancio, T.S.; Batchinsky, A.I.; Cancio, L.C.; Li, Y. HMGB1 Inhibition to Ameliorate Organ Failure and Increase Survival in Trauma. Biomolecules 2022, 12, 101. [Google Scholar] [CrossRef] [PubMed]
- Holcomb, J.B.; McMullin, N.R.; Pearse, L.; Caruso, J.; Wade, C.E.; Oetjen-Gerdes, L.; Champion, H.R.; Lawnick, M.; Farr, W.; Rodriguez, S.; et al. Causes of Death in U.S. Special Operations Forces in the Global War on Terrorism: 2001–2004. Ann. Surg. 2007, 245, 986–991. [Google Scholar] [CrossRef]
- Maughon, J.S. An Inquiry into the Nature of Wounds Resulting in Killed in Action in Vietnam. Mil. Med. 1970, 135, 8–13. [Google Scholar] [CrossRef]
- Sauaia, A.; Moore, F.A.; Moore, E.E.; Moser, K.S.; Brennan, R.; Read, R.A.; Pons, P.T. Epidemiology of Trauma Deaths: A Reassessment. J. Trauma. 1995, 38, 185–193. [Google Scholar] [CrossRef]
- Holcomb, J.B. Transport Time and Preoperating Room Hemostatic Interventions Are Important: Improving Outcomes After Severe Truncal Injury. Crit. Care Med. 2018, 46, 447–453. [Google Scholar] [CrossRef]
- Szebeni, J.; Baranyi, L.; Savay, S.; Götze, O.; Alving, C.R.; Bünger, R.; Mongan, P.D. Complement Activation during Hemorrhagic Shock and Resuscitation in Swine. Shock 2003, 20, 347–355. [Google Scholar] [CrossRef]
- Foucher, C.D.; Tubben, R.E. Lactic Acidosis. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2024. [Google Scholar]
- Treml, B.; Kleinsasser, A.; Knotzer, J.; Breitkopf, R.; Velik-Salchner, C.; Rajsic, S. Hemorrhagic Shock: Blood Marker Sequencing and Pulmonary Gas Exchange. Diagnostics 2023, 13, 639. [Google Scholar] [CrossRef]
- Bellamy, R.F.; Maningas, P.A.; Wenger, B.A. Current Shock Models and Clinical Correlations. Ann. Emerg. Med. 1986, 15, 1392–1395. [Google Scholar] [CrossRef]
- Fülöp, A.; Turóczi, Z.; Garbaisz, D.; Harsányi, L.; Szijártó, A. Experimental Models of Hemorrhagic Shock: A Review. Eur. Surg. Res. 2013, 50, 57–70. [Google Scholar] [CrossRef]
- Pfeifer, R.; Lichte, P.; Schreiber, H.; Sellei, R.M.; Dienstknecht, T.; Sadeghi, C.; Pape, H.-C.; Kobbe, P. Models of Hemorrhagic Shock: Differences in the Physiological and Inflammatory Response. Cytokine 2013, 61, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Hannon, J.P.; Bossone, C.A.; Rodkey, W.G. Splenic Red Cell Sequestration and Blood Volume Measurements in Conscious Pigs. Am. J. Physiol. 1985, 248 Pt 2, R293–R301. [Google Scholar] [CrossRef] [PubMed]
- Bebarta, V.S.; Daheshia, M.; Ross, J.D. The Significance of Splenectomy in Experimental Swine Models of Controlled Hemorrhagic Shock. J. Trauma. Acute Care Surg. 2013, 75, 920. [Google Scholar] [CrossRef] [PubMed]
- Boysen, S.R.; Caulkett, N.A.; Brookfield, C.E.; Warren, A.; Pang, J.M. Splenectomy Versus Sham Splenectomy in a Swine Model of Controlled Hemorrhagic Shock. Shock 2016, 46, 439–446. [Google Scholar] [CrossRef]
- Kheirabadi, B.S.; Sandeen, J.L.; Dubick, M.A. Re: The Significance of Splenectomy in Experimental Swine Models of Hemorrhagic Shock. J. Trauma. Acute Care Surg. 2013, 75, 920–921. [Google Scholar] [CrossRef]
- Vnuk, D.; Lemo, N.; Nesek-Adam, V.; Maticić, D.; Radisić, B.; Kos, J.; Rumenjak, V.; Dohan Ehrenfest, D.M. Cardiopulmonary Effects of Hemorrhagic Shock in Splenic Autotransplanted Pigs: A New Surgical Model. Coll. Antropol. 2010, 34, 923–930. [Google Scholar]
- Pottecher, J.; Chemla, D.; Xavier, L.; Liu, N.; Chazot, T.; Marescaux, J.; Fischler, M.; Diemunsch, P.; Duranteau, J. Re: The Significance of Splenectomy in Experimental Swine Models of Hemorrhagic Shock. J. Trauma. Acute Care Surg. 2013, 75, 921–922. [Google Scholar] [CrossRef]
- Barry, M.; Trivedi, A.; Vivona, L.R.; Chui, J.; Pathipati, P.; Miyazawa, B.; Pati, S. Recovery of Endotheliopathy at 24 Hours in an Established Mouse Model of Hemorrhagic Shock and Trauma. Shock 2022, 58, 313–320. [Google Scholar] [CrossRef]
- Bunch, C.M.; Chang, E.; Moore, E.E.; Moore, H.B.; Kwaan, H.C.; Miller, J.B.; Al-Fadhl, M.D.; Thomas, A.V.; Zackariya, N.; Patel, S.S.; et al. SHock-INduced Endotheliopathy (SHINE): A Mechanistic Justification for Viscoelastography-Guided Resuscitation of Traumatic and Non-Traumatic Shock. Front. Physiol. 2023, 14, 1094845. [Google Scholar] [CrossRef] [PubMed]
- Burk, A.-M.; Martin, M.; Flierl, M.A.; Rittirsch, D.; Helm, M.; Lampl, L.; Bruckner, U.; Stahl, G.L.; Blom, A.M.; Perl, M.; et al. Early Complementopathy after Multiple Injuries in Humans. Shock 2012, 37, 348–354. [Google Scholar] [CrossRef] [PubMed]
- Ganter, M.T.; Brohi, K.; Cohen, M.J.; Shaffer, L.A.; Walsh, M.C.; Stahl, G.L.; Pittet, J.-F. Role of the Alternative Pathway in the Early Complement Activation Following Major Trauma. Shock 2007, 28, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Zhao, Q.; Liu, B.; Dixon, A.; Cancio, L.; Dubick, M.; Dalle Lucca, J. Early Complementopathy Predicts the Outcomes of Patients with Trauma. Trauma. Surg. Acute Care Open 2019, 4, e000217. [Google Scholar] [CrossRef] [PubMed]
- Lord, J.M.; Midwinter, M.J.; Chen, Y.-F.; Belli, A.; Brohi, K.; Kovacs, E.J.; Koenderman, L.; Kubes, P.; Lilford, R.J. The Systemic Immune Response to Trauma: An Overview of Pathophysiology and Treatment. Lancet 2014, 384, 1455–1465. [Google Scholar] [CrossRef] [PubMed]
- Huber-Lang, M.S.; Ignatius, A.; Köhl, J.; Mannes, M.; Braun, C.K. Complement in Trauma-Traumatised Complement? Br. J. Pharmacol. 2021, 178, 2863–2879. [Google Scholar] [CrossRef] [PubMed]
- Dobson, G.P.; Morris, J.L.; Letson, H.L. Why Are Bleeding Trauma Patients Still Dying? Towards a Systems Hypothesis of Trauma. Front. Physiol. 2022, 13, 990903. [Google Scholar] [CrossRef]
- Medby, C. Is There a Place for Crystalloids and Colloids in Remote Damage Control Resuscitation? Shock 2014, 41, 47–50. [Google Scholar] [CrossRef]
- Cazzolli, D.; Prittie, J. The Crystalloid-colloid Debate: Consequences of Resuscitation Fluid Selection in Veterinary Critical Care. J. Vet. Emergen Crit. Care 2015, 25, 6–19. [Google Scholar] [CrossRef]
- Fleming, S.D.; Phillips, L.M.; Lambris, J.D.; Tsokos, G.C. Complement Component C5a Mediates Hemorrhage-Induced Intestinal Damage. J. Surg. Res. 2008, 150, 196–203. [Google Scholar] [CrossRef] [PubMed]
- Horstick, G.; Kempf, T.; Lauterbach, M.; Bhakdi, S.; Kopacz, L.; Heimann, A.; Malzahn, M.; Horstick, M.; Meyer, J.; Kempski, O. C1-Esterase-Inhibitor Treatment at Early Reperfusion of Hemorrhagic Shock Reduces Mesentry Leukocyte Adhesion and Rolling. Microcirculation 2001, 8, 427–433. [Google Scholar] [CrossRef]
- Hoth, J.J.; Wells, J.D.; Jones, S.E.; Yoza, B.K.; McCall, C.E. Complement Mediates a Primed Inflammatory Response after Traumatic Lung Injury. J. Trauma Acute Care Surg. 2014, 76, 601–609. [Google Scholar] [CrossRef]
- Peckham, R.M.; Handrigan, M.T.; Bentley, T.B.; Falabella, M.J.; Chrovian, A.D.; Stahl, G.L.; Tsokos, G.C. C5-Blocking Antibody Reduces Fluid Requirements and Improves Responsiveness to Fluid Infusion in Hemorrhagic Shock Managed with Hypotensive Resuscitation. J. Appl. Physiol. 2007, 102, 673–680. [Google Scholar] [CrossRef]
- Wang, P.; Ba, Z.F.; Reich, S.S.; Zhou, M.; Holme, K.R.; Chaudry, I.H. Effects of Nonanticoagulant Heparin on Cardiovascular and Hepatocellular Function after Hemorrhagic Shock. Am. J. Physiol. Heart Circ. Physiol. 1996, 270, H1294–H1302. [Google Scholar] [CrossRef] [PubMed]
- Relja, B.; Wagner, N.; Franz, N.; Dieteren, S.; Mörs, K.; Schmidt, J.; Marzi, I.; Perl, M. Ethyl Pyruvate Reduces Acute Lung Damage Following Trauma and Hemorrhagic Shock via Inhibition of NF-κB and HMGB1. Immunobiology 2018, 223, 310–318. [Google Scholar] [CrossRef]
- Wagner, N.; Dieteren, S.; Franz, N.; Köhler, K.; Mörs, K.; Nicin, L.; Schmidt, J.; Perl, M.; Marzi, I.; Relja, B. Ethyl Pyruvate Ameliorates Hepatic Injury Following Blunt Chest Trauma and Hemorrhagic Shock by Reducing Local Inflammation, NF-kappaB Activation and HMGB1 Release. PLoS ONE 2018, 13, e0192171. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Harada, T.; Mollen, K.P.; Prince, J.M.; Levy, R.M.; Englert, J.A.; Gallowitsch-Puerta, M.; Yang, L.; Yang, H.; Tracey, K.J.; et al. Anti-HMGB1 Neutralizing Antibody Ameliorates Gut Barrier Dysfunction and Improves Survival after Hemorrhagic Shock. Mol. Med. 2006, 12, 105–114. [Google Scholar] [CrossRef] [PubMed]
- Keshari, R.S.; Silasi, R.; Popescu, N.I.; Patel, M.M.; Chaaban, H.; Lupu, C.; Coggeshall, K.M.; Mollnes, T.E.; DeMarco, S.J.; Lupu, F. Inhibition of Complement C5 Protects against Organ Failure and Reduces Mortality in a Baboon Model of Escherichia Coli Sepsis. Proc. Natl. Acad. Sci. USA 2017, 114, E6390–E6399. [Google Scholar] [CrossRef] [PubMed]
- Morrison, A.M.; Wang, P.; Chaudry, I.H. A Novel Nonanticoagulant Heparin Prevents Vascular Endothelial Cell Dysfunction During Hyperdynamic Sepsis. Shock 1996, 6, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Dalle Lucca, J.J.; Simovic, M.; Li, Y.; Moratz, C.; Falabella, M.; Tsokos, G.C. Decay-Accelerating Factor Mitigates Controlled Hemorrhage-Instigated Intestinal and Lung Tissue Damage and Hyperkalemia in Swine. J. Trauma 2011, 71 (Suppl. S1), S151–S160. [Google Scholar] [CrossRef]
- Dalle Lucca, J.J.; Li, Y.; Simovic, M.; Pusateri, A.E.; Falabella, M.; Dubick, M.A.; Tsokos, G.C. Effects of C1 Inhibitor on Tissue Damage in a Porcine Model of Controlled Hemorrhage. Shock 2012, 38, 82–91. [Google Scholar] [CrossRef]
- CRASH-2 Trial Collaborators; Shakur, H.; Roberts, I.; Bautista, R.; Caballero, J.; Coats, T.; Dewan, Y.; El-Sayed, H.; Gogichaishvili, T.; Gupta, S.; et al. Effects of Tranexamic Acid on Death, Vascular Occlusive Events, and Blood Transfusion in Trauma Patients with Significant Haemorrhage (CRASH-2): A Randomised, Placebo-Controlled Trial. Lancet 2010, 376, 23–32. [Google Scholar] [CrossRef]
- Draxler, D.F.; Yep, K.; Hanafi, G.; Winton, A.; Daglas, M.; Ho, H.; Sashindranath, M.; Wutzlhofer, L.M.; Forbes, A.; Goncalves, I.; et al. Tranexamic Acid Modulates the Immune Response and Reduces Postsurgical Infection Rates. Blood Adv. 2019, 3, 1598–1609. [Google Scholar] [CrossRef] [PubMed]
- Relke, N.; Chornenki, N.L.J.; Sholzberg, M. Tranexamic Acid Evidence and Controversies: An Illustrated Review. Res. Pract. Thromb. Haemost. 2021, 5, e12546. [Google Scholar] [CrossRef] [PubMed]
- Okholm, S.; Krog, J.; Hvas, A.-M. Tranexamic Acid and Its Potential Anti-Inflammatory Effect: A Systematic Review. Semin. Thromb. Hemost. 2022, 48, 568–595. [Google Scholar] [CrossRef] [PubMed]
- Guyette, F.X.; Brown, J.B.; Zenati, M.S.; Early-Young, B.J.; Adams, P.W.; Eastridge, B.J.; Nirula, R.; Vercruysse, G.A.; O’Keeffe, T.; Joseph, B.; et al. Tranexamic Acid during Prehospital Transport in Patients at Risk for Hemorrhage After Injury: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial. JAMA Surg. 2020, 156, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Rowell, S.E.; Meier, E.N.; McKnight, B.; Kannas, D.; May, S.; Sheehan, K.; Bulger, E.M.; Idris, A.H.; Christenson, J.; Morrison, L.J.; et al. Effect of Out-of-Hospital Tranexamic Acid vs. Placebo on 6-Month Functional Neurologic Outcomes in Patients with Moderate or Severe Traumatic Brain Injury. JAMA 2020, 324, 961. [Google Scholar] [CrossRef] [PubMed]
- Li, S.R.; Guyette, F.; Brown, J.; Zenati, M.; Reitz, K.M.; Eastridge, B.; Nirula, R.; Vercruysse, G.A.; O’Keeffe, T.; Joseph, B.; et al. Early Prehospital Tranexamic Acid following Injury Is Associated with a 30-Day Survival Benefit: A Secondary Analysis of a Randomized Clinical Trial. Ann. Surg. 2021, 274, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Bösch, F.; Angele, M.K.; Chaudry, I.H. Gender Differences in Trauma, Shock and Sepsis. Mil. Med. Res. 2018, 5, 35. [Google Scholar] [CrossRef] [PubMed]
- Brännström, A.; Von Oelreich, E.; Degerstedt, L.E.; Dahlquist, A.; Hånell, A.; Gustavsson, J.; Günther, M. The Swine as a Vehicle for Research in Trauma-Induced Coagulopathy: Introducing Principal Component Analysis for Viscoelastic Coagulation Tests. J. Trauma Acute Care Surg. 2021, 90, 360–368. [Google Scholar] [CrossRef]
- Stettler, G.R.; Moore, E.E.; Moore, H.B.; Lawson, P.J.; Fragoso, M.; Nunns, G.R.; Silliman, C.C.; Banerjee, A. Thrombelastography Indicates Limitations of Animal Models of Trauma-Induced Coagulopathy. J. Surg. Res. 2017, 217, 207–212. [Google Scholar] [CrossRef] [PubMed]
- Van Poucke, S.; Stevens, K.; Marcus, A.E.; Lancé, M. Hypothermia: Effects on Platelet Function and Hemostasis. Thromb. J. 2014, 12, 31. [Google Scholar] [CrossRef] [PubMed]
- Gallos, I.; Devall, A.; Martin, J.; Middleton, L.; Beeson, L.; Galadanci, H.; Alwy Al-Beity, F.; Qureshi, Z.; Hofmeyr, G.J.; Moran, N.; et al. Randomized Trial of Early Detection and Treatment of Postpartum Hemorrhage. N. Engl. J. Med. 2023, 389, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Sondeen, J.L.; Dubick, M.A.; Holcomb, J.B.; Wade, C.E. Uncontrolled Hemorrhage Differs from Volume- or Pressure-Matched Controlled Hemorrhage in Swine. Shock 2007, 28, 426–433. [Google Scholar] [CrossRef]
- Sondeen, J.L.; Prince, M.D.; Kheirabadi, B.S.; Wade, C.E.; Polykratis, I.A.; de Guzman, R.; Dubick, M.A. Initial Resuscitation with Plasma and Other Blood Components Reduced Bleeding Compared to Hetastarch in Anesthetized Swine with Uncontrolled Splenic Hemorrhage. Transfusion 2011, 51, 779–792. [Google Scholar] [CrossRef]
- Weeks, C.; Moratz, C.; Zacharia, A.; Stracener, C.; Egan, R.; Peckham, R.; Moore, F.D.; Tsokos, G.C. Decay-Accelerating Factor Attenuates Remote Ischemia-Reperfusion-Initiated Organ Damage. Clin. Immunol. 2007, 124, 311–327. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | ||||
|---|---|---|---|---|
| Sham | H | H + LR | H+Voluven® | |
| n | 9 | 13 | 12 | 6 |
| Body weight (kg) | 39.4 ± 1.1 | 38.2 ± 0.6 | 39.1 ± 0.8 | 40.8 ± 1.7 |
| Controlled SBV (mL/kg) | 22 | 22 | 22 | 22 |
| Uncontrolled SBV (mL/kg) at 30 | N/A | 11.1 ± 1.0 | 7.8 ± 0.9 | 10.1 ± 1.5 |
| 60 | N/A | 12.7 ± 1.1 | 10.7 ± 2.4 | 13.9 ± 1.8 |
| 90 | N/A | 12.7 ± 1.1 | 8.6 ± 1.0 | 16.1 ± 2.3 ‡ |
| 120 | N/A | 12.5 ± 1.6 | 8.6 ± 1.0 | 17.5 ± 2.7 ‡ |
| 360 min | N/A | 13.7 ± 1.0 | 11.0 ± 2.3 | 18.3 ± 2.8 ‡ |
| Fluid resuscitation (mL) at 60 | N/A | N/A | 733.2 ± 183.1 | 391.2 ± 94.3 |
| 90 | N/A | N/A | 1057.1 ± 218.0 | 481.7 ± 106.8 |
| 120 | N/A | N/A | 757.2 ± 237.4 | 544.1 ± 107.5 |
| 240 | N/A | N/A | 1385.8 ± 241.0 | 636.8 ± 90.7 |
| 360 min | N/A | N/A | 1757.3 ± 75.3 | 785.4 ± 16.4 |
| PP (mmHg) | ||||
| Baseline | 26.7 ± 2.1 | 28.7 ± 3.2 | 29.1 ± 2.8 | 28.8 ± 1.8 |
| At 30 | 28.5 ± 1.7 | 20.1 ± 2.9 | 17.7 ± 2.7 * | 19.7 ± 4.0 * |
| 60 | 29.1 ± 1.3 | 21.5 ± 3.1 | 22.0 ± 2.6 | 27.8 ± 3.1 |
| 90 | 27.2 ± 1.5 | 14.3 ± 1.5 | 22.0 ± 3.3 | 28.0 ± 2.6 † |
| 120 min | 26.0 ± 1.5 | 16.3 ± 3.8 | 21.3 ± 3 | 24.6 ± 3.9 |
| MAP (mmHg) | ||||
| Baseline | 63.4 ± 2.5 | 62.6 ± 3.2 | 63.4 ± 3.1 | 60.8 ± 1.6 |
| At 30 | 65.1 ± 1.3 | 38.7 ± 2.3 * | 39.5 ± 3.8 * | 32.2 ± 4.1 * |
| 60 | 63.3 ± 1.4 | 37.9 ± 2.2 * | 44.6 ± 2.8 * | 44.3 ± 1.5 * |
| 90 | 62.4 ± 1.9 | 29.6 ± 1.9 * | 44.1 ± 1.9 *† | 43.0 ± 1.3 * |
| 120 min | 63.4 ± 1.8 | 26.9 ± 2.2 * | 43.0 ± 1.6 *† | 38.1 ± 3.7 * |
| Shock index (bpm/mmHg) | ||||
| Baseline | 1.3 ± 0.1 | 1.4 ± 0.2 | 1.3 ± 0.1 | 1.3 ± 0.1 |
| At 30 | 1.4 ± 0.1 | 4.5 ± 0.3 * | 5.2 ± 1.2 * | 4.8 ± 0.7 * |
| 60 | 1.5 ± 0.1 | 4.5 ± 0.2 * | 3.5 ± 0.4 * | 3.2 ± 0.1 *† |
| 90 | 1.5 ± 0.1 | 5.4 ± 0.5 * | 3.2 ± 0.2 *† | 3.1 ± 0.1 *† |
| 120 min | 1.6 ± 0.1 | 5.3 ± 0.2 * | 3.4 ± 0.2 *† | 3.3 ± 0.1 *† |
| Group | ||||
|---|---|---|---|---|
| Sham | H | H + LR | H+Voluven® | |
| n | 9 | 14 | 12 | 6 |
| pH: Baseline | 7.44 ± 0.02 | 7.43 ± 0.01 | 7.43 ± 0.01 | 7.45 ± 0.01 |
| At time 30 | 7.43 ± 0.02 | 7.40 ± 0.01 | 7.40 ± 0.02 | 7.42 ± 0.03 |
| 60 | 7.44 ± 0.02 | 7.38 ± 0.01 | 7.38 ± 0.01 | 7.36 ± 0.02 |
| 90 | 7.45 ± 0.02 | 7.38 ± 0.03 | 7.39 ± 0.01 | 7.39 ± 0.03 |
| 120 min | 7.45 ± 0.02 | 7.40 ± 0.03 | 7.41 ± 0.02 | 7.45 ± 0.07 |
| Base excess (mmol/L): Baseline | 5.3 ± 0.8 | 6.2 ± 0.6 | 5.2 ± 1.0 | 6.7 ± 0.8 |
| At time 30 | 6.3 ± 0.9 | 2.5 ± 0.6 * | 2.8 ± 0.7 | 0.4 ± 1 * |
| 60 | 5.9 ± 0.8 | −0.7 ± 1.0 * | 1.8 ± 1.0 * | 1.6 ± 0.9 * |
| 90 | 6.1 ± 1.0 | −3.4 ± 2.2 * | 3.5 ± 1.0 † | 3.2 ± 1.2 † |
| 120 min | 7.1 ± 0.9 | −3.7 ± 1.7 * | 4.0 ± 1.1 † | 4.0 ± 1.4 † |
| Lactate (mmol/L): Baseline | 2.2 ± 0.2 | 2.0 ± 0.1 | 2.2 ± 0.2 | 2.0 ± 0.2 |
| At time 30 | 1.9 ± 0.1 | 4.1 ± 0.2 * | 3.3 ± 0.2 | 5.3 ± 0.6 * |
| 60 | 1.7 ± 0.1 | 6.6 ± 0.6 * | 5.1 ± 0.8 * | 5.5 ± 0.4 * |
| 90 | 1.7 ± 0.2 | 8.9 ± 1.9 * | 4.3 ± 0.7 *† | 4.9 ± 0.4 *† |
| 120 min | 1.5 ± 0.2 | 9.3 ± 1.5 * | 3.8 ± 0.6 *† | 5.2 ± 0.8 *† |
| SvO2 (%): Baseline | 79.0 ± 3.3 | 73.4 ± 2.4 | 76.0 ± 1.2 | 79.4 ± 2.2 |
| At time 30 | 79.4 ± 2.2 | 54.3 ± 6.5 * | 52.2 ± 6.5 * | 66.5 ± 6.4 |
| 60 | 78.2 ± 2.5 | 62.1 ± 6.5 | 59.1 ± 3.7 * | 71.7 ± 4.2 |
| 90 | 74.4 ± 1.4 | 71.3 ± 7.4 | 54.2 ± 5.6 * | 71.8 ± 4.3 |
| 120 min | 77.1 ± 2.6 | 49.4 ± 10.4 * | 56.5 ± 4.8 * | 67.3 ± 6.1 |
| Hemoglobin (g/dL): Baseline | 8.3 ± 0.3 | 8.4 ± 0.17 | 8.6 ± 0.2 | 8.1 ± 0.2 |
| At time 30 | 8.1 ± 0.4 | 8.31 ± 0.23 | 8.6 ± 0.4 | 7.8 ± 0.4 |
| 60 | 8 ± 0.4 | 8.25 ± 0.27 | 6.9 ± 0.6 * | 4.5 ± 0.4 * |
| 90 | 7.9 ± 0.3 | 6.6 ± 1.0 | 6.3 ± 0.6 | 4.6 ± 0.5 ‡† |
| 120 min | 8.3 ± 0.3 | 7.1 ± 0.7 | 6.7 ± 0.37 † | 4.4 ± 0.4 †* |
| Hct (%): Baseline | 24.5 ± 1.06 | 24.7 ± 0.5 | 25.4 ± 0.6 | 23.8 ± 0.8 |
| At time 30 | 25.2 ± 1.2 | 24.5 ± 0.7 | 25.3 ± 1.2 | 23.0 ± 1.2 |
| 60 | 24.2 ± 1.4 | 23.2 ± 1.3 | 19.4 ± 1.8 | 13.2 ± 1.0 *†‡ |
| 90 | 23.5 ± 1.2 | 19.4 ± 2.8 | 18.4 ± 1.6 | 12.8 ± 1.4 *†‡ |
| 120 min | 25.2 ± 1.2 | 21.0 ± 2.1 | 19.7 ± 1.1 * | 12.4 ± 1.1 *†‡ |
| Potassium (mmol/L): Baseline | 4.1 ± 0.0 | 4.0 ± 0.1 | 3.9 ± 0.1 | 3.9 ± 0.1 |
| At time 30 | 4.2 ± 0.1 | 4.7 ± 0.1 | 4.6 ± 0.3 | 5.1 ± 0.3 * |
| 60 | 4.2 ± 0.1 | 5.1 ± 0.2 * | 4.4 ± 0.3† | 3.8 ± 0.1 † |
| 90 | 4.4 ± 0.1 | 5.2 ± 0.4 | 4.4 ± 0.1 | 4.3 ± 0.1 |
| 120 min | 4.5 ± 0.1 | 6.2 ± 0.7 * | 4.6 ± 0.1 † | 4.8 ± 0.1 † |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simovic, M.O.; Bynum, J.; Liu, B.; Dalle Lucca, J.J.; Li, Y. Impact of Immunopathy and Coagulopathy on Multi-Organ Failure and Mortality in a Lethal Porcine Model of Controlled and Uncontrolled Hemorrhage. Int. J. Mol. Sci. 2024, 25, 2500. https://doi.org/10.3390/ijms25052500
Simovic MO, Bynum J, Liu B, Dalle Lucca JJ, Li Y. Impact of Immunopathy and Coagulopathy on Multi-Organ Failure and Mortality in a Lethal Porcine Model of Controlled and Uncontrolled Hemorrhage. International Journal of Molecular Sciences. 2024; 25(5):2500. https://doi.org/10.3390/ijms25052500
Chicago/Turabian StyleSimovic, Milomir O., James Bynum, Bin Liu, Jurandir J. Dalle Lucca, and Yansong Li. 2024. "Impact of Immunopathy and Coagulopathy on Multi-Organ Failure and Mortality in a Lethal Porcine Model of Controlled and Uncontrolled Hemorrhage" International Journal of Molecular Sciences 25, no. 5: 2500. https://doi.org/10.3390/ijms25052500