
Synovial Fluid from Patients with Osteoarthritis Shows Different Inflammatory Features Depending on the Presence of Calcium Pyrophosphate Crystals

 , , and
, , and
Abstract
:1. Introduction
2. Results
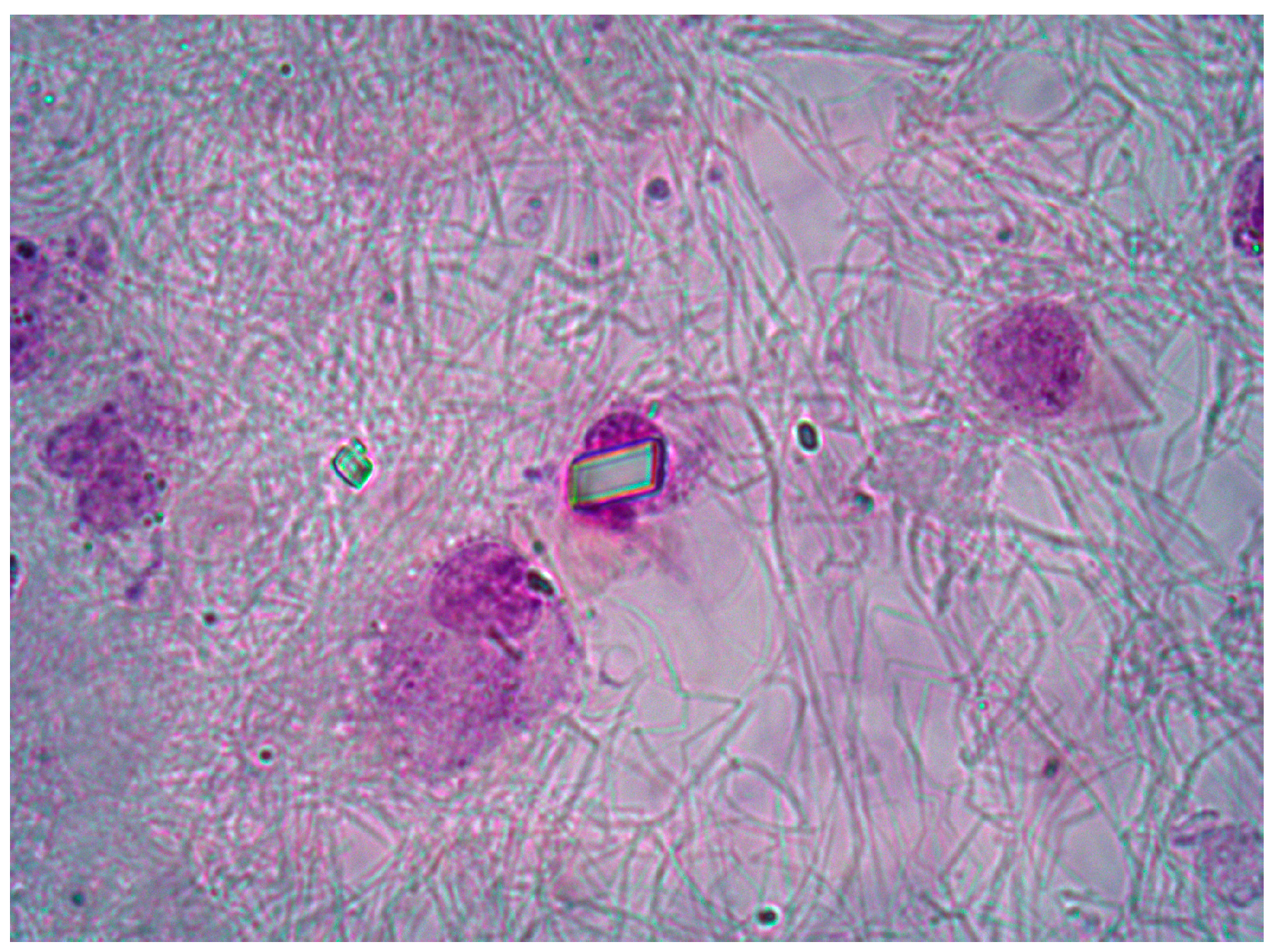
2.1. Synovial Fluid Characteristics
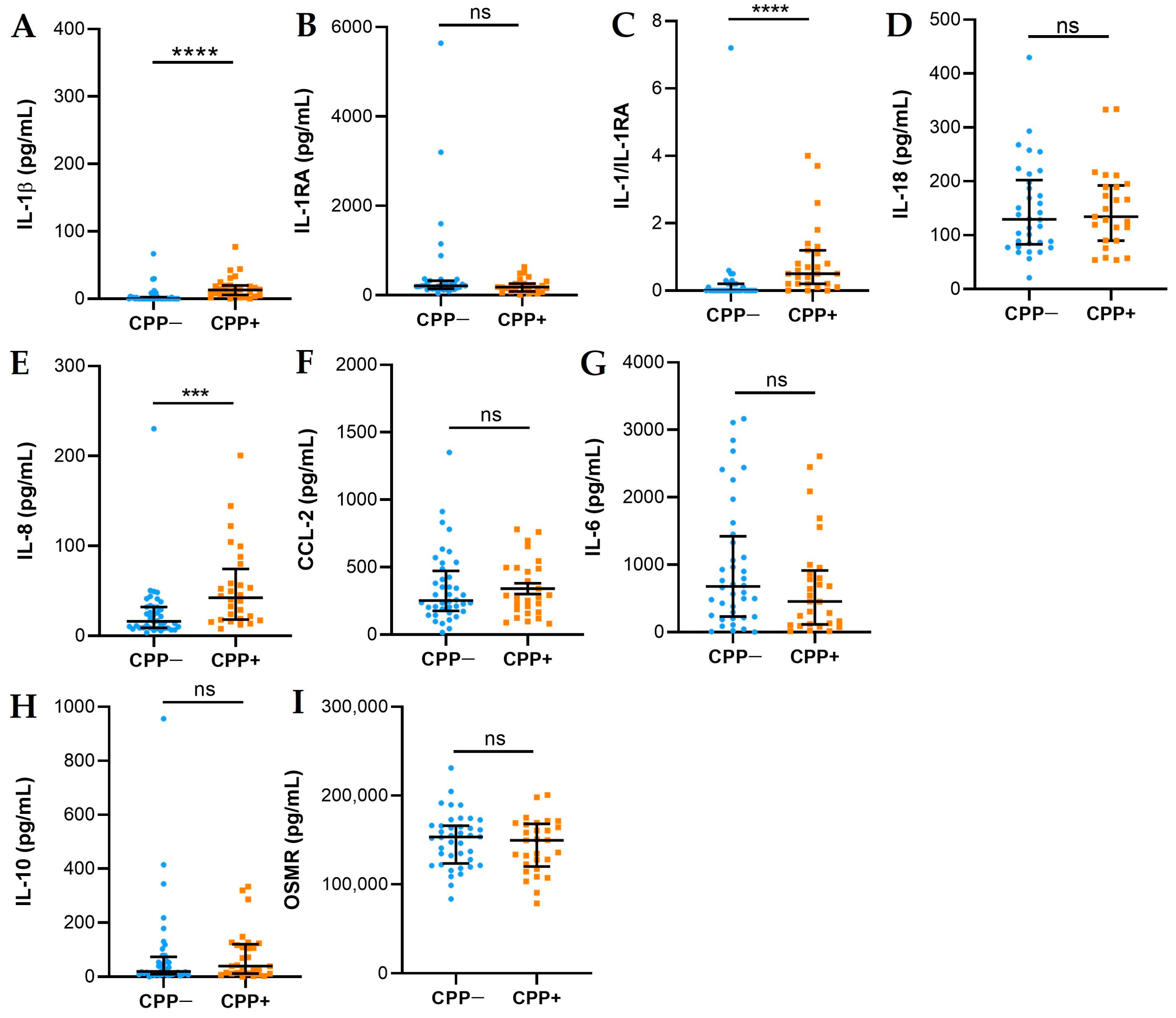
2.2. Cytokines and Chemokines
Inflammasome Activation
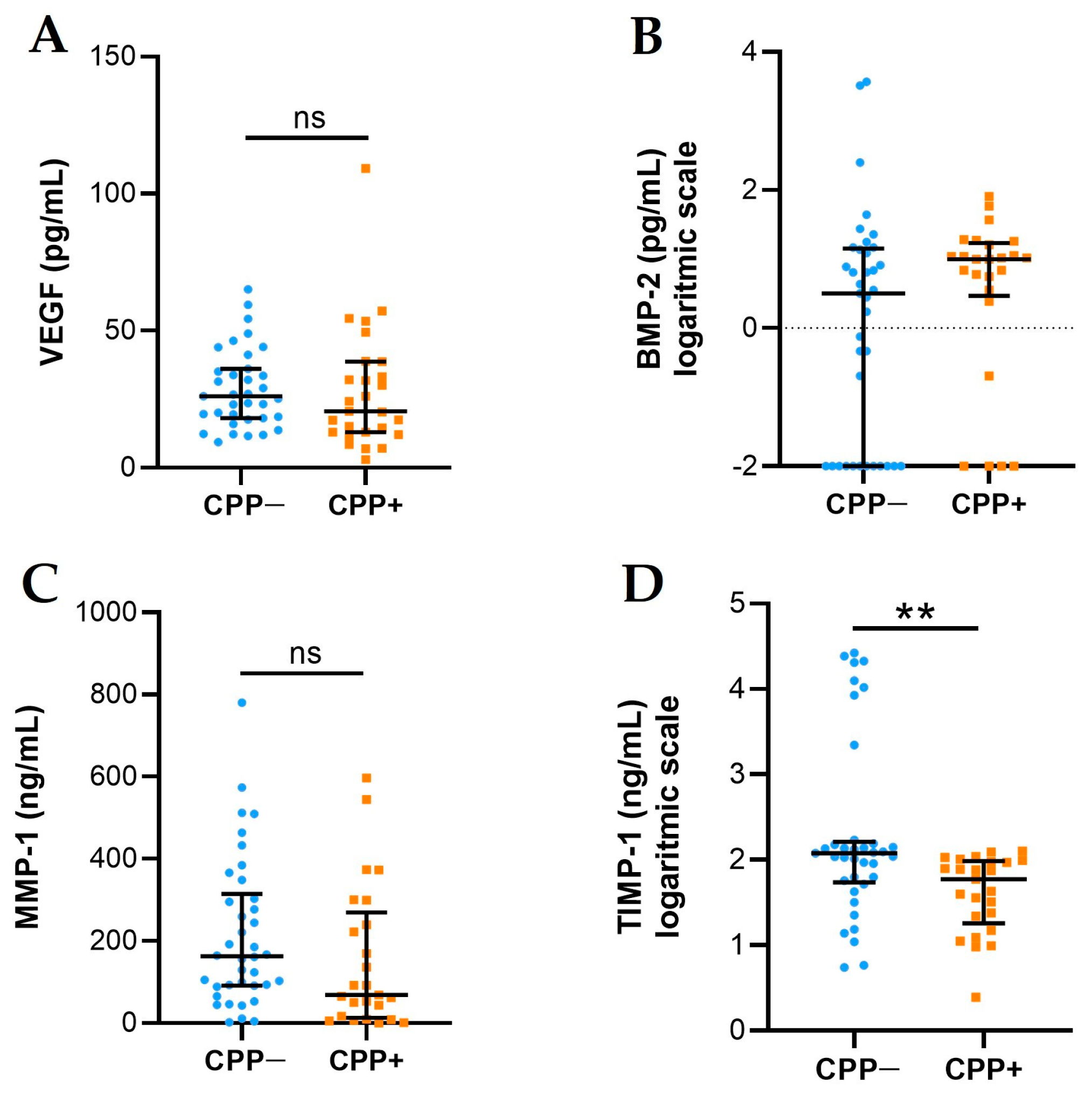
2.3. VEGF, BMP-2, MMP-1, and TIMP-1 Levels
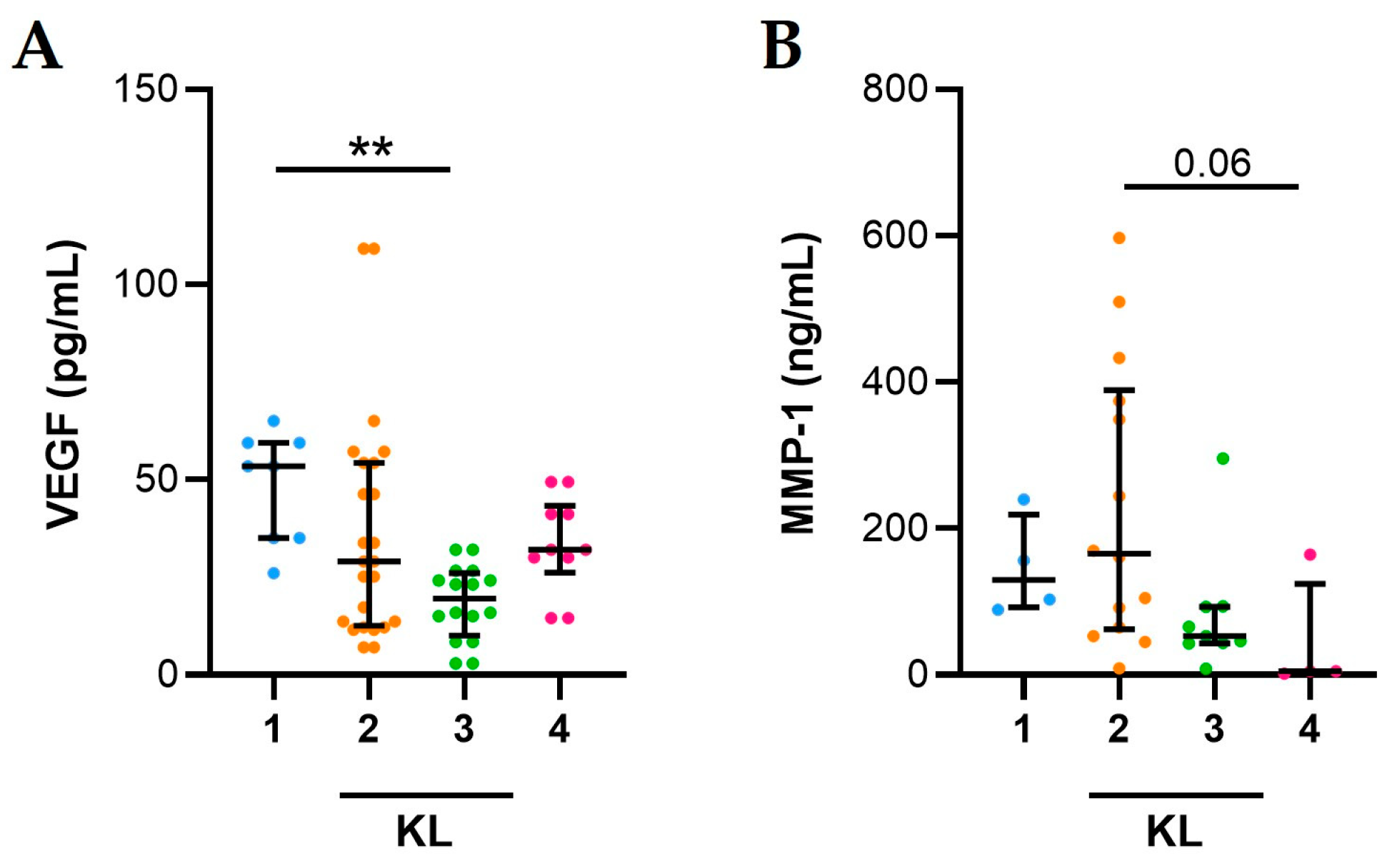
2.4. Association between Inflammation and Synovial Fluid Factors
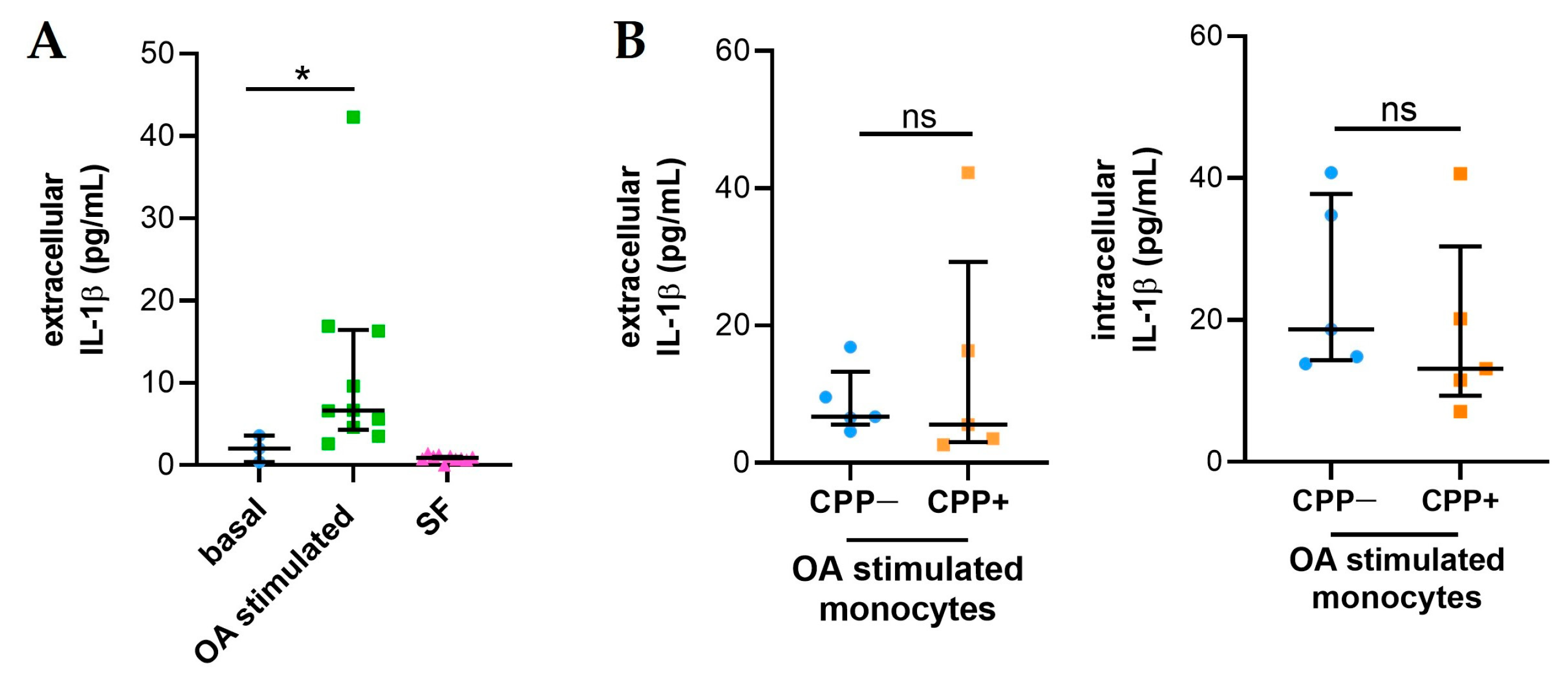
2.5. Synovial Fluids from Patients with OA Stimulate the Release of IL-1β in Monocytes
3. Discussion
4. Materials and Methods
4.1. Reagents
4.2. Study Design and Patient’s Characteristics
4.3. Synovial Fluid Examination
4.4. Cytokine, Chemokine, Growth Factor, Metalloproteases, BMP-2, and TIMP-1 Measurement
4.5. RNA Extraction and Real-Time qPCR
4.6. Cell Culture and Treatment with Synovial Fluids
4.7. Statistical Analysis
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- GBD 2021 Osteoarthritis Collaborators. Global, regional, and national burden of osteoarthritis, 1990–2020 and projections to 2050: A systematic analysis for the Global Burden of Disease Study 2021. Lancet Rheumatol. 2023, 5, e508–e522. [Google Scholar] [CrossRef] [PubMed]
- Roos, E.M.; Arden, N.K. Strategies for the prevention of knee osteoarthritis. Nat. Rev. Rheumatol. 2016, 12, 92–101. [Google Scholar] [CrossRef] [PubMed]
- Snoeker, B.; Turkiewicz, A.; Magnusson, K.; Frobell, R.; Yu, D.; Peat, G.; Englund, M. Risk of knee osteoarthritis after different types of knee injuries in young adults: A population-based cohort study. Br. J. Sports Med. 2020, 54, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Sahin, N.; Yesil, H. Regenerative methods in osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2023, 37, 101824. [Google Scholar] [CrossRef] [PubMed]
- Krakowski, P.; Karpiński, R.; Maciejewski, R.; Jonak, J.; Jurkiewicz, A. Short-Term Effects of Arthroscopic Microfracturation of Knee Chondral Defects in Osteoarthritis. Appl. Sci. 2020, 10, 8312. [Google Scholar] [CrossRef]
- Lioté, F.; Ea, H.K. Clinical implications of pathogenic calcium crystals. Curr. Opin. Rheumatol. 2014, 26, 192–196. [Google Scholar] [CrossRef]
- Conway, R.; McCarthy, G.M. Calcium-Containing Crystals and Osteoarthritis: An Un-healthy Alliance. Curr. Rheumatol. Rep. 2018, 20, 13. [Google Scholar] [CrossRef]
- Rosenthal, A.K. Crystals, inflammation, and osteoarthritis. Curr. Opin. Rheumatol. 2011, 23, 170–173. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Bardin, T.; Barskova, V.; Guerne, P.A.; Jansen, T.L.; Leeb, B.F.; Perez-Ruiz, F.; Pimentao, J.; Punzi, L.; et al. European League against Rheumatism recommendations for calcium pyrophosphate deposition. Part I: Terminology and diagnosis. Ann. Rheum. Dis. 2011, 70, 563–570. [Google Scholar] [CrossRef]
- Campillo-Gimenez, L.; Renaudin, F.; Jalabert, M.; Gras, P.; Gosset, M.; Rey, C.; Sarda, S.; Collet, C.; Cohen-Solal, M.; Combes, C.; et al. Inflammatory Potential of Four Different Phases of Calcium Pyrophosphate Relies on NF-κB Activation and MAPK Pathways. Front. Immunol. 2018, 9, 2248. [Google Scholar] [CrossRef]
- Nasi, S.; So, A.; Combes, C.; Daudon, M.; Busso, N. Interleukin-6 and chondrocyte mineralisation act in tandem to promote experimental osteoarthritis. Ann. Rheum. Dis. 2016, 75, 1372–1379. [Google Scholar] [CrossRef]
- Frallonardo, P.; Ramonda, R.; Peruzzo, L.; Scanu, A.; Galozzi, P.; Tauro, L.; Punzi, L.; Oliviero, F. Basic calcium phosphate and pyrophosphate crystals in early and late osteoarthritis: Relationship with clinical indices and inflammation. Clin. Rheumatol. 2018, 37, 2847–2853. [Google Scholar] [CrossRef]
- Oliviero, F.; Scanu, A.; Galozzi, P.; Gava, A.; Frallonardo, P.; Ramonda, R.; Punzi, L. Prevalence of calcium pyrophosphate and monosodium urate crystals in synovial fluid of patients with previously diagnosed joint diseases. Jt. Bone Spine 2013, 80, 287–290. [Google Scholar] [CrossRef]
- Mandell, B.F. (Ed.) Synovial Fluid Analysis and the Evaluation of Patients with Arthritis; Springer: Cham, Switzerland, 2022. [Google Scholar]
- Martínez Sanchis, A.; Pascual, E. Intracellular and extracellular CPPD crystals are a regular feature in synovial fluid from uninflamed joints of patients with CPPD related arthropathy. Ann. Rheum. Dis. 2005, 64, 1769–1772. [Google Scholar] [CrossRef]
- Onai, N.; Ogasawara, C. Calcium Pyrophosphate Dihydrate Crystals Increase the Granulocyte/Monocyte Progenitor (GMP) and Enhance Granulocyte and Monocyte Differentiation In Vivo. Int. J. Mol. Sci. 2020, 22, 262. [Google Scholar] [CrossRef]
- Ea, H.K.; Chobaz, V.; Nguyen, C.; Nasi, S.; Van Lent, P.; Daudon, M.; Dessombz, A.; Bazin, D.; McCarthy, G.; Jolles-Haeberli, B.; et al. Pathogenic role of basic calcium phosphate crystals in destructive arthropathies. PLoS ONE 2013, 8, e57352. [Google Scholar] [CrossRef]
- So, A.K.; Martinon, F. Inflammation in gout: Mechanisms and therapeutic targets. Nat. Rev. Rheumatol. 2017, 13, 639–647. [Google Scholar] [CrossRef]
- Ma, Z.; Wei, Y.; Liao, T.; Jie, L.; Yang, N.; Yu, L.; Wang, P. Activation of vascular endothelial cells by synovial fibrosis promotes Ne-trin-1-induced sensory nerve sprouting and exacerbates pain sensitivity. J. Cell. Mol. Med. 2023, 27, 3773–3785. [Google Scholar] [CrossRef]
- Li, J.; Zhang, W.; Liu, X.; Li, G.; Gu, Y.; Zhang, K.; Shen, F.; Wu, X.; Jiang, Y.; Zhang, Q.; et al. Endothelial Stat3 activation promotes osteoarthritis development. Cell Prolif. 2023, 13, e13518. [Google Scholar] [CrossRef]
- Quintero-Fabián, S.; Arreola, R.; Becerril-Villanueva, E.; Torres-Romero, J.C.; Arana-Argáez, V.; Lara-Riegos, J.; Ramírez-Camacho, M.A.; Alvarez-Sánchez, M.E. Role of Matrix Metalloproteinases in Angiogenesis and Cancer. Front. Oncol. 2019, 9, 1370. [Google Scholar] [CrossRef]
- Zhang, W.; Doherty, M.; Peat, G.; Bierma-Zeinstra, M.A.; Arden, N.K.; Bresnihan, B.; Herrero-Beaumont, G.; Kirschner, S.; Leeb, B.F.; Lohmander, L.S.; et al. EULAR evidence-based recommendations for the diagnosis of knee osteoarthritis. Ann. Rheum. Dis. 2010, 69, 483–489. [Google Scholar] [CrossRef] [PubMed]
- Kellgren, J.H.; Lawrence, J.S. Radiological assessment of osteoarthrosis. Ann. Rheum. Dis. 1957, 16, 494–502. [Google Scholar] [CrossRef] [PubMed]
- Bernal, J.A.; Andrés, M.; López-Salguero, S.; Jovaní, V.; Vela-Casasempere, P.; Pascual, E. Agreement Among Multiple Observers on Crystal Identification by Synovial Fluid Microscopy. Arthritis Care Res. 2023, 75, 682–688. [Google Scholar] [CrossRef] [PubMed]
- Scanu, A.; Oliviero, F.; Gruaz, L.; Galozzi, P.; Luisetto, R.; Ramonda, R.; Burger, D.; Punzi, L. Synovial fluid proteins are required for the induction of interleukin-1β production by monosodium urate crystals. Scand. J. Rheumatol. 2016, 45, 384–393. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| OA | CPP− | CPP+ | p |
|---|---|---|---|
| Patients, n | 39 | 29 | |
| Age, years (IQR) | 66 (52–76) | 74 (68–79) | 0.0235 |
| Sex, n | F, 27; M, 12 | F, 19; M, 10 | ns |
| WBC, n/mm3 (IQR) | 100 (100–200) | 200 (100–300) | 0.0028 |
| PMN, % (IQR) | 0 (0) | 2 (0–9.5) | <0.0001 |
| M, % (IQR) | 98 (98) | 96 (90–98) | <0.0001 |
| Score, n | CPP− (n = 20) | CPP+ (n = 15) |
|---|---|---|
| 1–2 | 13 (65%) | 7 (46.6%) |
| 3–4 | 7 (35%) | 8 (53.4%) |
| CPP− | CPP+ | p | |
|---|---|---|---|
| Caspase-1, 2-∆Ct (IQR) | 0.1366 (0.02409–0.2733) | 0.2292 (0.1568–0.5294) | ns |
| NLRP3, 2-∆Ct (IQR) | 0.1240 (0.1136–0.1414) | 0.1130 (0.01196–0.1167) | ns |
| WBC | PMN | M | |
|---|---|---|---|
| IL-1β | ns | p = 0.001 (r = 0.419) | p = 0.049 (r = −0.253) |
| IL-8 | p = 0.001 (r = 0.387) | p < 0.0001 (r = 0.556) | p < 0.0001 (r = −0.504) |
| IL-10 | p = 0.014 (r = 0.299) | ns | ns |
| OSMR | ns | ns | p = 0.015 (r = 0.309) |
| VEGF | p = 0.039 (r = −0.267) | p = 0.007 (r = −0.362) | p = 0.031 (r = 0.291) |
| Gene | Forward Primer | Reverse Primer |
|---|---|---|
| IL-1β IL-18 NLRP3 CASPASE-1 GAPDH | CAGCCAATCTTCATTGCTCA TGTCGCAGGAATAAAGATGGCT TGAAGAAAGATTACCGTAAGAAGTACAGA GCTGAGGTTGACATCACAGGCA TGCACCACCAACTGCTTAGC | TCGGAGATTCGTAGGTGGAT CCTTGGTCAATGAAGAGAACTTGGT GCGTTTGTTGAGGCTCACACT TGCTGTCAGAGGTCTTGTGCTC GGCATGGACTGTGGTCATGAG |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oliviero, F.; Baggio, C.; Favero, M.; Damasco, A.C.; Boscaro, C.; Tietto, D.; Albiero, M.; Doria, A.; Ramonda, R. Synovial Fluid from Patients with Osteoarthritis Shows Different Inflammatory Features Depending on the Presence of Calcium Pyrophosphate Crystals. Int. J. Mol. Sci. 2024, 25, 393. https://doi.org/10.3390/ijms25010393
Oliviero F, Baggio C, Favero M, Damasco AC, Boscaro C, Tietto D, Albiero M, Doria A, Ramonda R. Synovial Fluid from Patients with Osteoarthritis Shows Different Inflammatory Features Depending on the Presence of Calcium Pyrophosphate Crystals. International Journal of Molecular Sciences. 2024; 25(1):393. https://doi.org/10.3390/ijms25010393
Chicago/Turabian StyleOliviero, Francesca, Chiara Baggio, Marta Favero, Amelia Carmela Damasco, Carlotta Boscaro, Davide Tietto, Mattia Albiero, Andrea Doria, and Roberta Ramonda. 2024. "Synovial Fluid from Patients with Osteoarthritis Shows Different Inflammatory Features Depending on the Presence of Calcium Pyrophosphate Crystals" International Journal of Molecular Sciences 25, no. 1: 393. https://doi.org/10.3390/ijms25010393